
1-s2.0-S1529943014000552-main
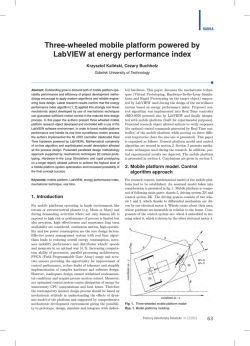
The Spine Journal 14 (2014) 1070–1071 Cervical osteoid osteoma progression to osteoblastoma A 16-year-old boy presented with 6 months of moderate neck pain, more severe at night, and temporarily relief by nonsteroidal anti-inflammatory drugs. Radiographs were normal. Magnetic resonance imaging showed edema in C6 vertebral body and surrounding C5–C6 posterior element (Fig. 1). Computed tomography (CT) scan findings were consistent with osteoid osteoma located on the right pedicle of C6 (Fig. 2). Intralesional excision was proposed to the patient and parents who did not accept. One year later, the patient reported a worsening cervical pain no longer responsive to analgesics with root irritation in the right arm. A new CT scan showed considerable expansion of the lesion involving C6 right pedicle and articular process surrounding the C6 nerve root and vertebral artery, highly Fig. 2. Computed tomography scan showed the typical feature of osteoid osteoma (axial view). suspicious for osteoblastoma (Fig 3, Left and Right). An intralesional excision and posterior C4–C7 fusion provided immediate pain relief. Histologic examination of the specimens confirmed the diagnosis of osteoblastoma. Five years after surgical treatment, the patient was asymptomatic; CT scan (Fig. 4) and radiographs (Fig. 5) showed no local recurrence and complete fusion from C4 to C7 at the left side. This case demonstrates that although rare, spinal osteoid osteoma can progress to osteoblastoma [1]. Reference [1] Bruneau M, Polivka M, Cornelius JF, George B. Progression of an osteoid osteoma to an osteoblastoma. Case report. J Neurosurg Spine 2005;3:238–41. Fig. 1. Sagittal magnetic resonance imaging demonstrated bone and soft tissue edema. 1529-9430/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.spinee.2013.12.021 Michele Cappuccio, MDa Federico De Iure, MDa Luca Amendola, MDa Alessandro Corghi, MDa Alessandro Gasbarrini, MDb a Department of Orthopaedics and TraumatologydSpine Surgery Maggiore Hospital ‘‘C.A. Pizzardi’’ M. Cappuccio et al. / The Spine Journal 14 (2014) 1070–1071 1071 Fig. 3. Computed tomography scan showed progression of the lesion: (Left) axial view and (Right) sagittal view. Largo Nigrisoli 2 40100 Bologna, Italy b Department of Oncologic and Degenerative Spine Surgery Rizzoli Orthopedics Institute Via G.C. Pupilli 1 40100 Bologna, Italy Fig. 4. Computed tomography scan 5 years after the surgery. FDA device/drug status: Not applicable. Author disclosures: MC: Nothing to disclose. FDI: Nothing to disclose. LA: Nothing to disclose. AC: Nothing to disclose. AG: Nothing to disclose. Fig. 5. Radiograph 5 years after the surgery.











© Copyright 2026