
Tumor Necrosis Factor-a! Downregulates Protein S
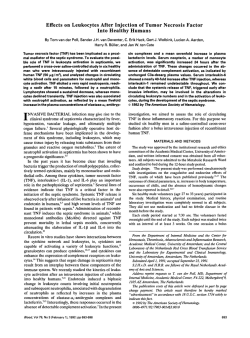
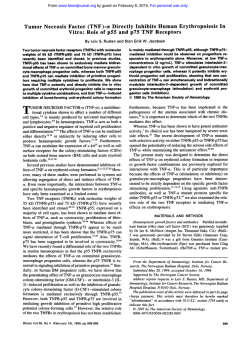
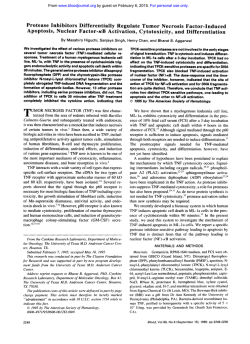
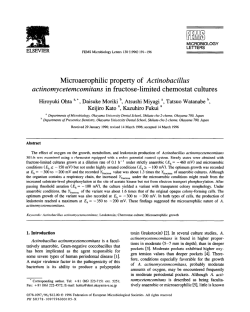
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Tumor Necrosis Factor-a! Downregulates Protein S Secretion in Human Microvascular and Umbilical Vein Endothelial Cells But Not in the HepG-2 Hepatoma Cell Line By W. Craig Hooper, Donald J. Phillips, Maria J.A. Ribeiro, Jane M. Benson, Velma and Bruce L. Evatt G. George, Edwin W. Ades, Protein S deficiency, which is associated with thrombosis, can either be inherited or acquired. Recently, we reported that a decrease in free protein S was observed in 19 of 25 persons with HIV/AIDS. The proinflammatory cytokine, tumor necrosis factor-a (TNF-a), has been reported t o be elevated in human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) patientsand has been shown t o induce a procoagulant state on thesurface of endothelial cells. We report here that recombinant TNF-a (rTNF-a) downregulated protein S synthesis in the SV-4OT transfected human microvascular endothelial cell line (HMEC-1) model system by approximately 70% and in primary human umbilical vein and dermal microvascular endothelial cell cultures by approximately 50%. Using the HMEC1 model, Northernblot analysis showed adecrease in protein S RNA at 24 hours that was corroborated by Western blot analysis and enzyme-linked immunosorbent assay (ELISA) quantification. Evidence supporting the specificity of the TNF-a effect included the following: (1) TNF-adownregulation of protein S was completelyblocked by TNF neutralizing antibody; (2)the effect was transient, and protein S was restoredt o near normal levels after TNF was removed to the TNF RI (55from cell cultures; (3)an antibody directed kD receptor) was shown t o mimic the action of TNF-a on HMEC-1 cells; and (4) other proinflammatory cytokines, interleukin (lL)-l, IL-6, and TGF-p, had no effect on protein S secretion. However, TNF-a showed no regulatory control over protein S synthesis in the human hepatocellular carcinoma cellline HepG-2. Wesuggest that TNF-a downregulaS may bea mechanism for localized procoagtion of protein ulant activity and thrombosis recently reported in some AIDS patients with associated protein S deficiency. This is a US government work. There are no restrictions on its use. H associated with decreased levels of protein S such as HIV infectiodacquired immunodeficiency syndrome Cytokines are soluble effector proteins that are functionally involved in hematopoiesis, inflammation, hemostasis and the immune The effector function of cytokines are tightly controlled, and any dysfunction in their regulation could lead to inappropriate cytokine expression and contribute to disease pathogenesis. Because it has been suggested that cytokine production may be responsible for many of the symptoms associated with HIV?' and it has been reported that some endothelial cell-derived proteins associated with coagulation and fibrinolysis could be modulated in vitro by TNF and IL- l our laboratory has begun to investigate the role of these cytokines in the regulation of protein S. UMAN PROTEIN S is a 75-kDvitamin K-dependent plasma glycoprotein that acts as a cofactor for activated protein C (APC) in the anticoagulation cascade.',' Approximately 40% of the circulating protein S is physiologically active and is found free in the plasma, while the remainder is bound to the C4b binding protein. Even though hepatocytes are thought to be the major source of protein S prod~ction,~ vascular endothelial cells$5 megakaryocytes,6 osteoblast^,^ and neural-derived tissue' synthesize significant amounts of protein S. The physiologic relevance of protein S has been illustrated by many reports that have documented an association between recurrent thrombosis and inherited protein S defi~ i e n c y . ~Genetic "~ analysis of families with the inherited deficiency has shown that large DNA deletions of the protein S gene were present in some, but not all fa mi lie^.'^,'^ Other molecular studies have found point mutations in the protein S gene that have resulted in amino acid substitutions. These results suggest that any one of several DNA alterations may be responsible for an inherited functional or physical free protein S deficiency. Protein S deficiency can also be acquired.I6-" It is common in persons undergoing oral anticoagulant therapy with vitamin K antagonists,16." and has been reported to be associated with liver d i ~ e a s e , ' ~pregnan~y,".'~ .~' oral contraceptive intake," infection-associated disseminated intravascular coagdation2' (DIC), and systemic lupus erythematosus.22Although the association of acquired protein S deficiency with thrombosis is not as well documented as that of familial protein S deficiency, an increase in clinical evidence has made this association more apparent.'9,23,24 More recently, two reports have documented decreased protein S levels in some persons infected with the human immunodeficiency virus (HIV) and associated t h r o m b o s i ~ . ~Although ~ , ~ ~ the mechanism(s) responsible for the decrease in protein S are currently not known, elevated plasma levels of some cytokines, eg, tumor necrosis factor (W), interleukin (IL)-l, and IL-6, are known to occur in some of the conditions Blood, Vol 84, No 2 (July 15), 1994: pp 483-489 MATERIALS AND METHODS Cell culture. The HepG-2 hepatocellular carcinoma cell line was obtained from the American Type Culture Collection (Rockville, MD). The establishment of an SV-40T transfected human microvascular endothelial cell line, HMEC-1, has been previously described." Both cell lines were maintained by the Biological Products Branch, Scientific Resources Program of The Centers for Disease Control and Prevention. Human umbilical vein endothelial cells (HUVEC, Clonetics, San Diego, CA) and human dermal microvascular endo- From the Hematologic Diseases and Biological Products Branches, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA. Submitted August 19, 1993; accepted March 15, 1994. Address reprint requests to W. Craig Hooper, PhD, Hematologic Diseases Branch, MS-DO2, Centers for Disease Control and Prevention, I600 Clifton Rd, Atlanta, GA 30333. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. This is a US g o v e m n t work. There are m resrzicrions on its me. 0006-4971/94/8402-0$0.00/0 483 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 484 thelia1 cells (HDMEC, Cell Systems Corp, Kirkland, WA) were obtained commercially and propagated using the manufacturer’s medium and accompanying instructions. Experiments performed with HepG-2 and HMEC-l used cells at passage levels 18 to 28 and 8 to 16, respectively, while HUVEC and HDMEC were used at passage levels 3 to 7. Cells, propagated as monolayer cultures, were initially plated at a density of 0.5 to 1 X lo5 cells/cm2 in 2.0-cm2 24-well plates (Costar, Cambridge, MA) or for RNA harvest, a 75cmz culture flask. Once confluence was established, culture fluids were removed by aspiration and fresh media with or without added cytokine was dispensed over the cell monolayers (zero time). Cells and culture fluids were harvested at scheduled intervals for protein S RNA analysis by Northern blot and for antigen quantification by enzyme-linked immunosorbent assay (ELISA) and Western blot. Cell viability and proliferation was determined by neutral red4”and naphthol blue black assays4’as described previously. Data presented here represent measurement averages (mean 2 1 SD) from four to six replicate culture well fluids from at least two separate experimental determinations. Cytokines. Recombinant human TNF-a, TNF-B, IL-la, and IL6, and highly purified TGF-P were purchased from R & D Systems, Inc (Minneapolis, MN). The manufacturer had determined endotoxin levels to be less than 0.1 ng per 1 pg of cytokine. Unless stated otherwise, TNF and TGF-P additions to cell cultures were at 10 ng1 mL of culture media. IL-la and IL-6 were usedat 5 ng1mLof culture media. ELISA. The ELISA used to quantify protein S in cell culture fluids has been previously described.* Briefly, goat antiprotein S antiserum (American Diagnostica, Greenwich, CT) fractionated on DEAE-Sephadex A50 (fall through after equilibration in 0.1 m o m Tris-HC1 pH 8.3, 0.05 molL NaCI) was used as capture antibody. Rabbit antihuman protein S second antibody (Sigma, St Louis, MO) was used at 1:2,000 in phosphate-buffered saline, 5% normal goat serum, and detected with horseradish peroxidase (HRP)-conjugated donkey antirabbit IgG (Amersham, Arlington Heights, IL) diluted 111,500 in the same buffer. HRP activity was measured against ophenylenediamine (Sigma) dissolved at 0.4 mg1mLin0.05 moll L citrate-phosphate buffer, pH 5.0 containing H2O2 (0.00133%). Absorbance at 490 nm was determined with an EL312e Microplate Reader (Biotek, Winooski, VT). Data reduction used the KinetiCalc software package (Biotek). Purified protein S used for calibration and as a positive control was obtained from American Diagnostica and has been previously ~haracterized.’~ Western blot. A nonreducing 8% gel was charged with 30 pL of media from cell cultures that had been incubated without and with TNF for the time periods indicated. Following electrophoresis, the gel was transblotted onto ECL nitrocellulose paper (Amersham) by using BioRad (Richmond, CA) gel and transblot apparatus, and incubated with goat antiprotein S antiserum (1: 1,OOO; American Diagnostics). Bound antibody was detected with HRP-conjugated rabbit antigoat IgG (Cappel, West Chester, PA) and a chemiluminescent detection system (Amersham). Northern blot. Total cellular RNA was isolated using the TRI Reagent Kit (Molecular Research Center, Inc, Cincinnati, OH) according to the manufacturer’s protocol. Following electrophoresis in 1% agarose gel containing 0.67 molL formaldehyde, RNA was transferred and cross-linked to nylon membranes (MSI, Westbord, MA). An 810-bp polymerase chain reaction generated protein S fragment was SzP-labeledby random priming (Pharmacia, Piscataway, NJ). The labeled probe was subsequently purified by being passed through a Sephadex G-50 column. Hybridization and posthybridization washes were performed as previously de~cribed.~’ TNF-a antibody neutralization. A goat anti-TNF-a neutralizing antibody No. AB-210-NA (R & D Systems, Inc) was used to demonstrate specificity of the TNF-a monokine. The manufacturer’s specifications were total IgG, purified by protein G affinity chromatogra- HOOPER ET AL phy, and with an endotoxin level (determined by the limulus amebocyte lysate method) of less than 10 ng per 1 mgof protein. In this experiment, rTNF-a (10 ng1mL) was preincubated with 0, 2, 5 , and 50 pg1mL of IgG overnight at 4°C in culture medium. Similarly, media containing IgG but without TNF-a were prepared for control experiments. Following this preincubation period, 1 mLof the antibody-antigen mixture was added to confluent cultures of HMEC-I cells and culture fluids were then harvested as indicated. TNF agonist determination on HMEC-I/HepG-2 cultures. A goat anti-TNF RI antibody (AB225-PB) against the 55-kD human TNF RI receptor, which reportedly does not cross-react with human recombinant TNF BPI1 (75-kD TNF receptor) and exhibits TNF agonist activity on the human cell line A549, was purchased from R & D Systems, Inc. To determine if this antibody demonstrated agonist activity on the HMEC- 1 and HepG-2 cell lines, the antibody (10 pg1mL of culture fluid) was substituted for TNF-a in some experiments, and protein S levels in culture fluids were measured by ELISA and compared with those in untreated and TNF-a treated cultures. Effects of TNF-a wash-out and vitamin K on proteinS production. To determine if the TNF effect on HMEC-I cells was transitory, cultures were treated for 12 to 72 hours with TNF-a. The culture fluids were then removed and monolayers were washed with a balanced salts solution and replaced with fresh medium. Protein S levels in culture fluids harvested from these pretreated cells were then measured over time with the ELISA. The influence of vitamin K on protein S production was determined by adding 10 pg1mL vitamin K (Sigma) to culture fluids of TNF-treated and untreated HMEC-l cell cultures. RESULTS Protein S was constitutively synthesized and released by the three different endothelial cell cultures, and the increase was almost linear with time. Figure 1 shows typical relative I l l I l I 1 2 3 4 5 6 DAY S Fig 1. Constitutiveexpression of protein S by the HMEC-1 (01, HDMEC (0) and . HUVEC (A) cell cultures and subsequant accumulation in the culture fluids over a h i a y period. Error bars represent 1 SD about the mean proteinS value. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 485 DOWNREGULATION OF PROTEIN S BY TNF + Fig 2. Specificity of TNF-a downregulation effect on endothelial cell (HMEC-1) protein S production. (A) TNF-a downregulated protein S in a dosedependentmanner (0 nglmL 0; 0.1, 0; 1.0. A; 5.0, V; 10, 0; 50, V 1, and was not cytotoxic to the HMEC-1 cell line ( + l , and TNF downregulation was (B) abrogated with the addition of antiTNFa neutralizingantibody (untreated, 0; TNF, 0; 2 p g antibody + TNF, A; 50 p g antibody + TNF, V). (C1 The TNFa effect on protein S Ievds in HMEC-1 culture fluids was not observed with other inflammatory cytokinea. IL-l, V; 11-6. A; TGF-p, U. TNF-8 ( V ) was ObMWed t o downregulate protein S, but not to the same extent as TNF-a (0). n U 351 30 20 A 10 P 9 c ' 5 ' 20 -10 15 -20 2 C E 0 8 E W -30 5 -40 0 -50 M v 244872 .-> Z W 96 Hours Hours 1 .o 24 4872 96 24 4872 96 Hours concentration of TNF-a used. Antibody neutralization experiments (Fig 2B) demonstrated the specificity of TNF-a in the downregulation of protein S. The anti-TNF neutralizing antibody preparation at 2 pg/mL abolished the inhibitory effects of TNF-a and had no adverse effects on the cell culture when used alone at 50 pg/mL. Functionally related cytokines, IL-1a and IL-6, had no effect on protein S production in the Hh4EC-1 cell line (Fig 2C). Another multifunctional cytokine, TGF-P, had no effect on protein S secretion. Although TNF-p or lymphotoxin did exhibit an inhibitory effect on protein S production, this inhibition was about 50% of that experienced with TNF-a (Fig 2C). The combination of TNF-cu and TNF-@ did not result in either additive or synergistic inhibition (data not shown), and the inhibition observed was the same as that with TNF-a alone. TNF-p downregulation of protein S was also dose-dependent; the effect was seen maximally at 5 to 10 ng/mL. B E 0.8 0 b 4 in Q] m 3 0.6 0 c C e - E Q 10 W .-a c r = E C t + a 25 amounts of antigen accumulation in culture fluids in nanograms per lo5 cells. In the majority of experiments, data were collected over a 96-hour incubation period and protein S concentration expressed as nanograms per milliliter of culture fluid. The extent of TNF-a-induced downregulation of protein S in HMEC-1 is illustrated in Fig 2. Dose-response experiments (Fig 2A) demonstrated that a TNF-a concentration as low as 0.1 ng/mL, could reduce protein S levels. However, at the concentration of 0.1 ng/mL, the reduction in protein S antigen was 20% less than control cultures at 72 and 96 hours, whereas at higher concentrations marked reductions were present by 48 hours. Maximal downregulation of protein S (-70%) was at 72 hours when the TNF-a concentration was between 5 and 10 ng/mL. A TNF-a concentration of 50 ng/mL had no further effect. Cell viability (Fig 2A) and proliferation (data not shown) were not affected by any 6 5W O e 2 0.4 0 L) cn n a1 0 Fig 3. (A) Dose-dependentTNF downregulation 0.2 J 24 48 I I 72 Hours 96 I I # 1 Hours l of protein S in HUVEC cultures (0 nalmL0; 0.1.0; 1.0, A; 5, V; lo,.; 50, 0).(B) Neutral red uptake of TNF-treated and untreated HUVEC monolayera a h o w that TNF haa some mitogenic effect In HWEC culturea (symbols represent the same TNF douge as in Flg 3A). From www.bloodjournal.org by guest on February 6, 2015. For personal use only. HOOPER ET AL 486 r - n L W .f 70 T 4 t I 30 Q) 1 I L lo U t 4824 72 96 Hours lated, while RNA for the low-density lipoprotein receptor was upregulated (Fig 5). Similar observations have previously been reported.4’.44 Western blot analysis of HMEC-l protein S synthesis demonstrated a successive decrease in the 75-kD protein S antigen as a function of TNF-a treatment over time (Fig 6). The decrease in protein S relative to that in the control was striking at 48 hours and persistent at 72 and 96 hours. The decrease in protein S antigen seen in Westernblot and ELISA was corroborated by the decrease of protein S RNA in Northern blot analysis (Fig 7). Analysis ofRNA levels showed a biphasic pattern of expression in whichTNF-(r treatment induced an increase in transcript levels at 30 minutes and at 6 hours as compared with those in the control. This increase was followed by a marked decrease of protein S message at 24 and 72 hours (Fig 7A). This biphasic increase was not due to unequal RNA loading because ethidium bromide staining demonstrated equal amounts in each lane (Fig 7B). Wash-out experiments documented that the continuous presence of TNF-a was required to suppress production of protein S . Protein S levels rebounded after TNF-a was washed out after 24 hours and fresh mediumwas added (Fig 8). Similar results were seen when TNF-a was washed out after 12, 48, and 72 hours (data not shown). An antibody (AB225-PB) against the 55-kD TNF receptor, described by the manufacturer to have agonist activity on the human A549 cell line, was found to act as a TNF agonist on HMEC-I (Fig 9). The antibody-mediated down- Fig 4. Protein S downregulation was not observed in the HepG2 liver cell line followingthe addition of TNFa to cell culture fluids (V).Untreated HepG-2, A; untreated, 0;treated HMEG1.0. Hours We tested HUVEC cells and HDMEC cells to determine if TNF-a induced a similar protein S downregulation in these nontransfected, low-passage endothelial cells. Significantly, as shown inFig 3A, TNF-a-activated H W E C cultures produced approximately 50% lcss protein S than companion untreated cultures. The response was dose-dependent, and, as with HMEC-l, TNF exerted maximal effect at 5 to 10 ng/mL of culture fluid. This experiment was conducted with third-passage HUVEC cells and repeated with fifth- andseventh-passage cells. The outcome was the same each time as illustrated by Fig 3A. Figure 3B shows that the decrease in culture fluid protein S levels was not due to TNFcytotoxicity for HUVEC cells. The absorbance of neutral red at 570 nm following uptake and release from the lysosomes of viable cells from the same cultures used for protein S measurement is shown in Fig 3A. Similar culture monolayers stained with naphthol blue black supported the neutral red viability data. Human dermal microvascular endothelial cell culture fluids showed similarly reduced protein S levels when these cells were propagated in the presence of TNF (not shown). In contrast to that seen in the endothelial cell cultures, protein S production in the HepG-2 cell line was not affected by 10 ng/mL of TNF-a (Fig 4). Concentrations of TNF-a ranging from 0.1 ng to 1 0 0 ng/mL also had no inhibitory effect on this cell line (data not shown). However, HepG-2 cells were responsive to TNF-a. Following stimulation with TNF-a, RNA for the 55-kD TNF receptor was downregu- C 3 6 24 A B * ” * Fig 5. Northern blot showing that HepG-2cellsareresponsive to TNF. (A) TNF downregulation of its 55-kD receptor RNA, and (B) upregulation of the low-density lipoprotein receptor RNA. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. DOWNREGULATION OF PROTEIN S BY TNF 487 Hours 24 72 48 96 Fig 6. TNFa downregulation of protein S production in the HMEC-1 cell line as illustrated by a chemiluminescent Western blot. A purified protein S preparation (1 ng/mLl was included for reference. regulation of protein S was nearly identical to the cytokineinduced inhibition. No additive or synergistic effects were observed when TNF-a and the antibody agonist were combined (data not shown). The TNF agonist had no effect on the HepG-2 cell line. Addition of vitamin K, alone or in combination with TNF, did not alter the levels of protein S production from that measured in untreated or TNF-treated HMEC-I cells. factor, protein S , in the SV-40T-transfected human microvascular endothelial cell line, HMEC-l. This downregulation was seen at the transcriptional and posttranscriptional levels. The negative regulation of protein S appeared to be TNFspecific; other functionally related cytokines, IL-la and IL6, had no effect. Another multifunctional cytokine, TGF-0, also had no effect on protein S production in the HMEC1 cellline. Furthermore, neutralizing anti-TNF antibodies DISCUSSION This study has demonstrated that the proinflammatory cytokine TNF-a can negatively regulate the anticoagulant co- Hours A C' 25 c S W v> .-ac, -W B 15 10 0 L m 5 0 24 40 72 Hours Fig 7. (A) Northern blot analysis of the TNFa effect on HMEC-1 cell line RNA transcripts showing protein S RNA expression during a 0.5- t o 72-hour period. The lane labeledc contains RNA from untreated confluent monolayer cells. (B) Equal amounts of RNA were present in each lane as documented by ethidium bromide staining. Fig 8. Recovery of protein S synthesis and release after the removal of TNF containing media from the HMEC-1 cell cultures (A). Cultures werepretreated with TNF for 24 hours bafore replacement of media with fresh TNF free culture media. IO) Untreated, (0)TNFtreated cultures. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 4aa HOOPER ET AL 35 downregulating protein S. This observation is of potential significance because it provides another TNF-related mechanism for the downregulation of protein S in the absence of TNF. Furthermore, this antibody-mediated event may have a more prolonged physiologic effect, since its half-life and stability may be greater than those of TNF. Serum levels of TNF and IL-l have beenfound to be elevated in patients with either bacterial or viral infections,2S26,47 Current evidence suggests that these cytokines n 30 E \ 25 ol c W m .S Q) W 20 15 10 0 I B 5 0 I I I l 24 48 72 96 Hours Fig 9. The agonist effect of a goat-anti TNF RI antibody on the HMEC-1 cells (V), TNF alone (01,the combination of antibody and TNF (A), and control (01.A combination of the agonist and TNF (A) was not synergistic, ie, the downregulating effect was the same as with either compound alone. abolished the inhibitory effect of TNF-a. That TNF-P or lymphotoxin also inhibited protein S secretion was not surprising, because TNF-a and TNF-P are known to share the same receptors (TNF-R55 and TNF-R75) and tohave similar affinit~.~’ This decrease was approximately 50% of that seen with TNF-a and the difference in inhibition can perhaps be explained by postreceptor signaling pathways that are unique to each receptor and cytokine/receptor interaction. The TNFa effect was not permanent; by removing TNF-a, protein S secretion returned to near-normal levels. When expanded from the HMEC-1 model, TNF was shown to significantly downregulate protein S synthesis in low-passage, nontransfected HUVEC and HDMEC cultures, indicating that this observation of TNF dysregulation of protein S synthesis may represent a more general phenomenon with implications for in vivo vascular procoagulant activity. In contrast to its effect in the HMEC-l cell line and primary endothelial cell cultures, TNF-a hadno measurable effect on protein S production in the HepG-2 hepatoma cell line. However, the HepG-2 cells were responsive to TNFa, as demonstrated by its effect on the LDL-receptor and its own TNF-R55-kD receptor. Earlier studies have shown that antibodies against the TNF-a receptors (55 kD and 75 kD) can mimic the actions of TNF-cY!~Our results have demonstrated that an antibody against the 55-kD TNF-receptor was similar to TNF-a in are notonly a consequence of infection, but also play a role in disease progression.’6,28-”1 Not surprisingly, increased serum levels of TNF25-27 and IL- l 2627 have been documented in many patients infected with HIV. Two recent studies have shown that plasmalevels of total protein S are also decreased in a number of individuals with HIV/AIDS.22.24 One study found that out of 25 HIV-positive patients 19 had decreased protein S levels and three of these 19 had a history of thrombosis following the onset of HIV positivity.*‘ This coagulation abnormality was reportedly associated with an overall decrease in free and total protein S rather than to changes inthe normal physiologic distribution of free andbound protein S, which may occur in response to elevated levels of the acute-phase reactant C4b binding protein. A known source of protein S, the endothelium is responsive to TNF and IL- 1 exposure and investigators have shown that these cytokines can modulate endothelial cell derived proteins of the coagulation cascades in nearly identical fashion.” However, we did not see a similar effect on protein S production with IL- 1 in the HMEC- 1 cell line. The lack of an IL-1 response was not due to the absence of functional IL-l receptors, since we have determined in other studies that PAI- 1, leukemia inhibitory factor, and IL-6 RNA were induced by IL-l in the HMEC-I cells (unpublished data), as is the case with primary endothelial cell cultures.7’.33.35.38 Our studies are the first, that we are aware of, to show a direct correlation betweenTNF and the downregulationof the anticoagulant cofactor proteinS in an endothelial cell line and primary HUVEC and HDMEC cultures. These results may indicate a possible mechanism for thedecreasedprotein S levels and associated thrombosis seen in some AIDS patients. Furthermore, the HMEC-1 cells may serve as a convenient model for the study of regulatory mechanisms for protein S and other endothelial cell-derived proteins. REFERENCES I . Walker FJ: Regulation of activated protein C by a new protein: A role for bovine protein S. J Biol Chem 255:5521, 1980 2. Esmond C: The regulation of naturalanticoagulant pathway. Science 235:1384, 1987 3. Fair DS, Marlar RA: Biosynthesis and secretion of factor VII, protein C, protein S and the protein C inhibitor from a human hepatoma cell line. Blood 6754, 1986 4. Fair DS, Marlar R A , Levin EG: Human endothelial cells synthesize protein S. Blood 67:1168, 1986 5. Stem D, Brett J, Harris K, Nawroth PJ: Participation of endothelial cells in the protein C-protein S anticoagulant pathway: The synthesis and release of protein S. Cell Biol 102:1971, 1986 6. Schwartz HP, Heeb MJ, Wencel-Drake JS, Griffin JH: Identification and quantification of protein S inhuman platelets. Blood 66: 1452, 1985 7. Maillard C, Berruyer M, Serre CM, Dechavanne M, Delmas From www.bloodjournal.org by guest on February 6, 2015. For personal use only. DOWNREGULATION OFPROTEIN S BY TNF PD: Protein S, a vitamin K-dependent protein, is a bone matrix component synthesized and secreted by osteoblasts. Endocrinology 130:1599, 1992 8. Phillips DJ, Greengard JS, Femandez JA, Ribeiro M, Evatt BL, Griffin JH, Hooper W C Protein S, an antithmmbotic factor,is synthesized and released by neural tumor cells. J Neurochem 61:344, 1993 9. Comp Pc, Nixon RR, Cooper MR, Esmon CT: Familial protein S deficiency is associated with recurrent thrombosis. J Clin Invest 74:2082, 1984 10. Comp PC, Esmon CT: Recurrent venous thromboembolism in patients with a partial deficiency of protein S. N Engl J Med 311:1525, 1984 1 1. Schwartz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH: Plasma protein S deficiency in familial thrombotic disease. Blood 64:1297, 1984 12. Bertina RM: Hereditary protein S deficiency. Haemostasis 15:241, 1985 13. Engesser L, Broekmans AW, Briet E, Brommer ET, Bertina RM: Hereditary protein S deficiency: Clinical manifestations. Ann Int Med 106:677, 1987 14.van Ploos AJK, Huisman MV, Reitsma PH, ten Cate J W , Bertina RM: Partial protein S gene deletion in a family with hereditary thrombophilia. Blood 73:479, 1989 15. Schmidel DK, Nelson RM, Broxson EH Jr, Comp PC, Marlar RA, Long CL: A 5.3-Kb deletion including exon XI11 of the protein S a gene occurs in two protein S-deficient families. Blood 77:551, 1991 16. Fair DS, Revak DJ: Quantitation of human protein S in the plasma of normal and warfarin-treated individuals by radioimmunoassay. Thromb Res 36:527, 1984 17. Bertina RM, van Wijngaarden A, Reinalda-Poot J, Poort SR. Bom VJJ: Determination of plasma protein S-The protein cofactor of activated protein C. Thromb Haemostasis 53:268, 1985 18. Comp PC, Thumau GR, Welsh J, Esmon CT: Functional and immunologic protein S levels are decreased during pregnancy. Blood 68:881, 1986 19. Rose PG, Essig GF, Vaccaro PS, Brandt JT: Protein S deficiency in pregnancy. Am J Obstet Gynecol 155:140, 1986 20. Boerger LM, Moms PC, Thumau GR, Esmon C T , Comp TC: Oral contraceptives and gender affect protein S status. Blood 69:692, 1987 21. D’Angelo A, Vigano-D’Angelo S, Esmon CT, Comp PC: Acquired deficiencies of protein S: Protein S activity during oral anticoagulation, in liver disease and in disseminated intravascular coagulation. J Clin Invest 81:1445, 1988 22. Keeling DM, Cambell SJ, Mackie U, Machin SJ, Isenberg DA: Total and free protein S in systemic lupus erythematosus. Thromb Res 60:237, 1990 23. Lafeuillade A, Alessi MC, Poizot-Martin I, Dhiver C, Quilichini R, Aubert L, Gastaut JA, Juhan-Vague I: Protein S deficiency and HIV infection. N Engl J Med 324:1220, 1991 24. Stahl CP, Wideman CS, Spira TJ, Haff EC, Hixon GJ, Evatt BL: Protein S deficiency in men with long-term human immunodeficiency virus infection. Blood 81:1801, 1993 25. Lahdevirta J, Maury CPJ, Teppo A-M, Rep0 H: Elevated levels of circulating cachectidtumor necrosis factor in patients with acquired immunodeficiency syndrome. Am J Med 85:289, 1988 26. Scott-Algara D, Vuillier F, Marasescu M, de Saint Martin J, Dighiero G: Serum levels of L-2, L - l a , TNF-a, and soluble receptor of IL-2 in HIV-l infected patients. AIDS Res Human Retroviruses 7:381, 1991 27. Berman MA, Sanborg CI: Cytokines and AIDS, in Kunkel SL, Remick DC (eds): Cytokines in Health and Disease. New York, NY, Marcel Dekker, 1992, p 537 28. Beutler B, Cerami A: The biology of cachectinlTNF: A primary mediator of host response. Ann Rev Immunol 7:625, 1989 489 29. Vassalli P: The pathophysiology of tumor necrosis factors. Ann Rev Immunol 10411, 1992 30. Matsuyama T, Kobayashi N, Yamamoto N: Cytokines and HIV infection: Is AIDS a tumor necrosis factor disease? AIDS 5:1405, 1991 31. Bevilacqua MP, Pober JS, Majeau GR, Fiers W, Cotran RS, Gimbrone MA: Recombinant tumor necrosis factor induces procoagulant activity in cultured human vascular endothelium: Characterization and comparison with the actions of interleukin 1. h o c Natl Acad Sci USA 83:4533, 1986 32. Libby P, Ordovas JM, Auger KR, Robbins AH, Birinyi LK, Dinarello CA: Endotoxin and tumor necrosis factor induce interleukin-l gene expression on adult human vascular endothelial cells. Am J Pathol 124179, 1986 33. Nachman R L , Hajjar KA, Silverstein RL, Dinarello CA: Interleukin 1 induces endothelial cell synthesis of plasminogen activator inhibitor. J Exp Med 163:1597, 1986 34. Nawroth P, Bank I, Handley D, Cassimeris J, Chess L, Stem D: Tumor necrosis factorkachectin interacts with endothelial cell receptors to induce releaseof interleukin 1. J Exp Med 163:1363, 1986 35. Nawroth PP, Handley DA, Esmon CT, Stem DM: Interleukin 1 induces endothelial cell procoagulant while suppressing cell-surface anticoagulant activity. Proc Natl Acad Sci USA 83:3460, 1986 36. Nawroth PP, Stem DM: Modulation of endothelial cell hemostatic properties by tumor necrosis factor. J Exp Med i63:740, 1986 37. Conway EM, Rosenberg RD: Tumor necrosis factor suppresses transcription ofthe thrombomodulin gene in endothelial cells. Mol Cell Biol 8:5588, 1988 38. May LT, Torcia G, Cozzolino F, Ray A, Tatter SB, Santhanam U, Sehgal PB, Stem D: Interleukin-6 gene expression in human endothelial cells: RNA start sites, multiple IL-6 proteins and inhibition of proliferation. Biochem Biophys Res Commun 159:991, 1989 39. Ades A, Candal FJ, Swerlick RA, George VG, Summers S, Bosse DC, Lawley TJ: HMEC-1: Establishment of an immortalized human microvascular endothelial cell line. J Invest Dennatol99:683, 1992 40. Louis CB, Obrig TG: Shiga toxin-associated hemolytic uremic syndrome: Combined cytotoxic effects of shiga toxin and lipopolysaccharide (endotoxin) on human vascular endothelial cells in vitro. Infect Immun 6 0 : 1536, 1992 41. Kohase M, Henriksen-DeStefano D, May LT, Vilcek J, Sehgal PB: Induction of &interferon by tumor necrosis factor: A homeostatic mechanism in the control of cell proliferation. Cell 45:659, 1986 42. La1 RB, Rudolph D, Buckner C, Pardi D, Hooper WC: Infection with humanT-lymphotropic viruses leads to constitutive expression of leukemia inhibitory factor and interleukin-6. Blood 8 1 :1827, 1993 43. Stopeck AT, Nicholson AC, Mancini FP, Hajjar DP: Cytokine regulation of low density lipoprotein receptor gene transcription in HepG2 cells. J Biol Chem 268:17489, 1993 44. Winzen R, Wallach D, Kemper 0, Resch K, Holtman H: Selective up-regulation of 75-kDa tumor necrosis factor (TNF) receptor and its mRNA by TNF and IL-1. J Immunol 1504346, 1993 45. Loetscher H, Gentz R, Zalauf M, Lustig A, Tabachi H, Schlaeger EJ, Brockhaus M, Gallanti H, Manneberg M, Leeslauer W: Recombinant 55 kDa tumor necrosis factor (TNF) receptor. J Biol Chem 266:18324, 1991 46. Engelmann H, Holtmann H, Brakebusch C, Avni YS, Sarov I, Nophar Y, Hadas E, Leitner 0, Wallach D: Antibodies to a soluble form of a tumor necrosis factor (TNF) receptor have TNF-like activity. J Biol Chem 265:14497, 1990 47. Waage A, Halstensen A, Esenik T: Association between tumor necrosis factor in serum and fatal outcome in patients with meningococcal disease. Lancet 1:355, 1987 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1994 84: 483-489 Tumor necrosis factor-alpha downregulates protein S secretion in human microvascular and umbilical vein endothelial cells but not in the HepG- 2 hepatoma cell line WC Hooper, DJ Phillips, MJ Ribeiro, JM Benson, VG George, EW Ades and BL Evatt Updated information and services can be found at: http://www.bloodjournal.org/content/84/2/483.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.






© Copyright 2026