
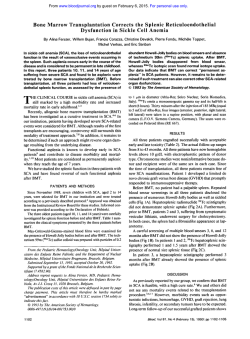
Clonal dysregulation of the antibody response to t
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Clonal Dysregulation of the Antibody Response to Tetanus-Toxoid After Bone Marrow Transplantation By E.J.A. Gerritsen, M.J.D. Van Tol, M.B. Van ’t Veer, J.M.A. Wels, I.M.S.L. Khouw, CR. Touw, CM. Jol-Van Der Zijde, J. Hermans, H.C. Rumke, J. Radl, and J.M. Vossen After bone marrow transplantation (BMT), a prolonged dysregulation of humoral immunity can be observed. In the present study, we investigated whether this is reflected in an abnormal production of specific antibodies (Ab)t o the Tcell-dependent recall antigen tetanus-toxoid (TT). The study group consisted of children receiving transplants of an unmodified allogeneic graft and of adults receiving eithera Tcell-depleted allogeneic or an unmodified autologous BM graft. Findings were compared with those in healthy controls. In pediatric graft recipients, who were routinely revaccinated early after BMT, the Abresponse was quantitatively superior to thatin adult graftrecipients who did not receive early revaccination. In the majority of graft recipients, the time periodafter vaccination required t o reach the peak level of antibodieswas prolongedand the number of responding TT-specific B-cell clones was markedly decreased in comparison withcontrols. In controls, a low frequency of dominant B-cell clones may produce low quantities of homogeneous Ab components (H-Ab) against a heterogeneous background. However, in BM graftrecipients, “overshooting“ of Ab production by separate B-cell clones was observed, resulting in the development of H-Ab at a relatively high concentration. These abnormalities were present up t o 10 years after BMT, irrespective of eitherthe age of the recipient, the modulation of the graft, or the vaccination schedule used. It is hypothesized that thedysregulated Ab production is the consequence of activation of a restricted number of resting memory B cells, present in germinal centers, repopulating gradually after BMT. Our data show that routinerevaccination early after BMT improves the humoral immune response. However, because of a clonally dysregulatedAb production, long-lastingqualitative defects maybe present even after normalization of Ab titers. 0 1994 by The American Societyof Hematology. B ONE MARROW transplant (BMT) recipients may sufanti-TT response, as assessed by the electrophoretic heterofer froman immunologic deficiency up to several years geneity of TT-specific IgG antibodies in sera from children after transplant.’ In the absence of chronic graft-versus-host and adults vaccinated after BMT. The findings were comdisease (GVHD), normalization of B-cell function is considpared with those found in routinely vaccinated healthy in1 to 2 years.’ Although B-cell eredto takeplacewithin fants, children, and adults. Although normal Ab titers were numbers become normal at 4 to 8 months posttransplant, already reached at 4 months after BMT in the majority of their phenotype is immature and their function is inadequate recipients, the number of B-cell clones involved in the rein a way similar to that found during ~ntogeny.’.~ Transient sponse wasmarkedly reduced for a prolonged periodof time. Ig (sub)class deficiencies may be observed after BMT.’” In Sometimes the response was largely dominated by a single clone and seemingly monoclonal. These abnormalities could addition, Ig synthesis is clonally dysregulated for some time be found as long as 10 years after BMT. after transplantation, resulting in monoclonal gammopathies (MG) and restricted heterogeneity of Ig.7.xAn abnormal huMATERIALS AND METHODS moral immune response may thus persist despite a normalization of serum Ig (sub)class levels. Specific antibody (Ab) Controls and Patients production can be detected from 3 months after BMT onThis study was approved by the Institutional Review Boards on wards, depending on the vaccines used”” and on whether Medical Ethics at the University Hospital (BMT center for children), the donorsorthe recipientshad been vaccinatedbefore Leiden, The Netherlands and the Dr. Daniel den Hoed Cancer Center BMT.I4-IXHowever, detailed information on qualitative as(BMT center for adults), Rotterdam, The Netherlands. pects of the Ab response in BMT recipients is still lacking. In thepresentstudy, we investigated more extensively Controls than hitherto the humoral immune response to the T-cellSera from 20 healthy infants and children, observed from birth dependent (TD) recall antigen tetanus-toxoid (TT). This inup to the age of 4 years, and from 20 healthy adult volunteers with vestigation was performednotonly by quantification of amedianage of 35years(range,25to 45 years)wereused as specific antibodies, but also by qualitative evaluation of the controls. Pediutric Patients From the Departments of Pediatrics and Medical Statistics, University Hospital, Leiden; the Department of Hematology, Dr. Daniel den Hoed Cancer Center,Rotterdam; the National Institute of Public Health and Environmental Protection, Bilthoven; and the TNO Institute of Ageing and Vascular Research, Leiden. The Netherlands. Submitted April 6, 1994; accepted August 23, 1994. Address reprint requests to E.J.A. Gerritsen, MD, Department oj Pediatrics, Leiden University Hospital, PO Box 9600.2300 RC Leiden, The Netherlands. The publication costsof this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicute this fact. 0 1994 by The Americun Society of Hematology. 0006-4971/94/8412-0018$3.00/0 4374 ChildrenreceivinggraftsofBMcellsfromanHLA-identical sibling between 1982 and 1989, who were cured of their original disease and who are alive and well, were included in the study (n = 38). The characteristics of these patients are given in Table 1. All receivedanunmodified BM graftwhilestayingintheprotective environment of a laminar flow isolator and after antimicrobial suppression of theirintestinal micro-flora.” By January I , 1993,the 7.5 years (range, 1.0 to1 1.0 years). median follow-up after BMT was As we previously reported, complete chimerism was present in the majority of patients.20 Adult Patients = Recipients treated with either an HLA-identical sibling graft (n 26) or an autologous graft (n = 9) between 1980 and 1992 who Blood, Vol 84, No 12 (December 151, 1994: pp 4374-4382 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. CLONALDYSREGULATION 4375 OF THE ANTIBODYRESPONSE Table 1. Characteristics of the Patients Children (n = 381 Age (yr) Median Range 16-60 Diagnosis AML ALL NHL CML Others Conditioning regimen CTX 120 TB1 12 CTX 120 TB1 10 6CTX 120 TB1 7-8 2 BU 16 CTX 120-200 Other Graft 26 Allogeneic Autologous GVHD prophylaxis TCD MTX CSA 2MTX + CSA Acute GVHD 24 Absent Grade I 32 Grade II Chronic GVHD 33 Absent Limited Extended 9 Adults (n = 35) 39 0.5-18 16 14 15 5 1 2 5 4 0 0 33 3 11 14 2 2 38 0 9 0 14 8 16 5 6 26* 2 18 30 2 8 ria toxoid (D)-pertussis (P)-tetanus toxoid (T)-inactivated polio virus type I, 11, and 111 (IPV) at 3, 4, 5 , and 11 (n = 16) or at 14 (n = 4) months (DPT-IPV I to IV) and with DT-IPV at 4 and 9 years of age (DT-IPV V and VI; Table 2). In addition, 20 healthy adult volunteers received a DT-IPV booster (B) vaccination. Pediatric patients. The patients and their BM donors had been vaccinated during infancy and early childhood with D(P)T-IPV vaccine, according to the Dutch National Vaccination Program. Twentyseven of 38 patients were immunized with DT-IPV within l month before BMT (DT-IPV 0; Table 2). In the light of other studies,"." 5 BM donors also received a DT-IPV vaccination within 2 weeks before graft donation. In the first 4 months after BMT, the recipients received 3 DTIPV booster injections (I to 111) with an interval of 1 month, starting from 6 weeks after BMT. A limited number of children received an additional injection (IV) between 6 and 24 months after BMT. In 1992, 21 children with a follow-up period of at least 3 years (range, 3 to 10 years) after BMT again received a DT-IPV injection (DTIPV V). Adult patients. As far as could be evaluated, all adult BM graft recipients and their donors had received routine D(P)T-IPV vaccinations in infancy and childhood. In addition, most male patients had received a DT-IPV injection at the start of their military service. None of the adult patients was vaccinated shortly before BMT and none received revaccination after BMT until the occurrence of an outbreak of poliomyelitis in The Netherlands (November 1992). At that time, all patients received three DT-IPV vaccinations at monthly intervals and one vaccination 6 months later. The response to the second vaccination (DT-IPV 11) was investigated. 6 30 4 4 Serum Samples 1 1 Abbreviations: AML, acute myeloblastic leukemia in first ( n = 30) or second (n = 1) remission; ALL, acute lymphoblastic leukemia in first ( n = 6 ) or second ( n = 13) remission; NHL, non-Hodgkin's lymphoma; CML, adult (Ph') chronic myeloblastic leukemia; Others, for children, severe aplastic anaemia (n = 2).@-thalassemiamaior (n = 2),and combined immunodeficiency(n = l ) ,for adults, M. Hodgkin (n = 2), multiple myeloma (n = 2), paroxysmal nocturnal hemoglobinuria (PNH; n = l ) , and mamma carcinoma (n = 1); CTX 120-200, cyclophosphamide 2 x 60 or 4 x 50 mg/kg; TB1 7-12,total body irradiation in grays (Gy), dose depending on age of recipient administered in one ( 5 8 Gy) or 2 ( 2 1 0 Gy) fractions with a dose rate of 24 to 48 cGy/min; 61.116,busulphan for 4 days at 4 mg/kg; GVHD, graft-versushost disease; TCD, r2 log T-cell depletion; MTX, methotrexate <50 mg/m2 in only first 2 weeks (n = 20). >l00 mg/m2 until day +l00 (n = 14; children with MTX only); CSA, cyclosporin A 2 mg/kg intravenously or 6 mg/kg orally for at least 3 months after BMT. In 13 patients, MTX and/or cyclosporin A was administered in addition to TCD. were alive and well were included. The characteristics of these patients are givenin Table l . In case of an allogeneic BMT, the graft was more than 2 log T-cell-depleted by albumin gradient centrifugation and E rosette sedimentation?' By January 1, 1993, the median follow-up of these patients was 2.5 years (range, 0.5 to 13.0 years). Methods Vaccination Controls. Twenty healthy infants and children were vaccinated according to the Dutch National Vaccination Program with diphthe- Serum samples were obtained after informed consent before and at a median of 3 weeks (range, 2 to 4 weeks) after vaccination, with the following exceptions. From children of the control group receiving DPT-IPV IV at 14 months of age (n = 4), the postvaccination serum sample was taken 4 weeks later; from those immunized at 11 months of age (n = 16), serum was taken at 4 months after vaccination. Cord blood samples were available from all healthy infants included in the study. Sera from healthy adults were obtained at 2 and 4 weeks and at 3, 6, and 12 months after the booster. From pediatric graft recipients, serum samples were also obtained at 3 and 6 months after DT-IPV IV. From adult graft recipients, only one serum sample, taken 4 weeks after the second DT-IPV vaccination, was available. All sera were kept frozen at -20°C until analysis. Serum Analysis Quantification of IgG anti-7T antibodies. The concentration of IgG anti-TT antibodies was measured by enzyme-linked immunosorbent assay (ELISA), as has previously been described.**The concentration was expressed in arbitrary units (AU) per milliliter using a reference serum for standardization. The Ab response in healthy children after DT-IPV VI at 9 years of age was not investigated in this study. Data on IgG anti-'M levels after vaccination of 8 pediatric graft recipients early after BMT werenot included, because the children were being treated at that time for acute or chronic GVHD with immunosuppressive therapy. Dejinition of response to TT. In healthy infants (controls), a primary Ab response to 'M was scored as positive if the postimmunization IgG titer was at least twice the preimmunization titer and reached 20.2 AU/mL. In pediatric and adult controls andinthe pediatric patients a secondary Ab response was considered positive in case of an increase of the post-immunization IgG titer to 125% of the pre-immunization titer, reaching at least 1.0 AU/mL. In two cases, newly arising TT-specific homogeneous Ab components (HAb) were detected in the absence of an increase of the Ab titer. This From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 4376 GERRITSENET AL Table 2. Vaccination Protocols in BMT Patients and Controls 19 Controls Vaccination no. No. of 20 individuals Age* Median Range Pediatric patients Vaccination no. No. of patients Period post-BMT Median Range Adult patients Vaccination no. No. of evaluable cases Period post-BMT Median Range II 111 IV V B 20 4 m0 5 m0 12 mo 11-14 mo 4 yr 35 yr 25-45 yr 111 IV V 9 mo 6-24 wk 7 yr 3.5-10.5 yr I 19 20 3 m0 0 27 I 21 -3 wk 11 -(1-4) wk 38 I1 2338 7 wk 6-10 10-14 wk 24 wk wk 15 wk wk 14-20 II 35 2.5 yr 0.5-13 yr Abbreviation: -, before BMT. The Dutch National Vaccination Program also provides vaccination at 9 years of age. The response to this immunization was not investigated. 0-v, D(P)T-IPVvaccination number in healthy infants and children, and in BMT recipients. B, DT-IpV booster vaccination in adult controls. finding was interpreted as an indication for a positive TT response. I n the adult patients. a preimmunization sample was not available. In thesepatients,an A b responsewas defined as positive if the postimmunization titer was 2 1.0 AUlmL. 7T-sprcific itnrnunohlotfing. To investigate the heterogeneity of IgG anti-TT and the occurrence o f H-Ab, we applied agar gel-elec'T trophoresis o f serum samples according to Wieme, followed by I antigen-specific immunoblotting (WABL) onto nitrocellulose membranes coated with 10 pglmL (3 pg/cmZ) o f I T . The patterns were developed using Ig isotype-specific monoclonal antibodies (MoAbs: Nordic Immunological Laboratories, Tilburg, The Netherlands), as described earlier.2'.2' The serum samples (diluted 1:2SO) were investigated for TT-specific IgG patterns together with a positive and a negative control25 (Fig IA; these human MoAbs were kindly provided by Dr W.P. Zeijlemaker, CLB, Amsterdam, The Netherlands). In 7 selected patients with H-Ab at a relatively high concentration (0.2 to 2 pglmL) in the first year after BMT, we investigated whether the H-Ab present at 3 to IO years after B M T were still produced by thesame B-cell clones. T h i s investigation was performed by 'ITspecific W A B L and by isoelectric focusing (IEF) followed by IT antigen-specific immunoblotting (FABL)"." for the characterization o f the IgG subclass and light chain type o f the H-Ab. A.sse.s.srnenf of WABL patfems. Overall patterns and presence o f H-Ab were analyzed independently by two investigators (E.J.A.G. and M.J.D.v.T.). The patterns were scored as either heterogeneous or o f restricted heterogeneity (Fig 2). Besides the number of H-Ab, the concentration o f H - A h was assessed semiquantitatively as high (>O.S pg/mL), medium, or low ( 4 . 1 pglmL), using the positive control sample diluted inphosphate-buffered saline (PRS) as a reference (Fig IB). The limit o f sensitivityfor the detection o f ITspecific H-Ab by WABLranges from S to SO nglmL, depending on the intensity of the pattern of the heterogeneous antibodies." Sfatistical evaluation. Responsepercentages and frequencies o f tests on 2 X 2 tables, and 9S% confiH-Ab were compared with dence intervals for the difference of the percentages were calculated. The titer values were analysed using the Student's f-test. x' RESULTS Quantification of IgG Anti-TT Antibodies Controls. After thefirst vaccination, 45% of the infants responded to TT (Table 3). The infants who responded had a lower preimmunization Ab titer in the cord blood andin the prevaccination sample than did the nonresponders ( P < .OOl and P < . O l , respectively; data not shown). This finding indicates that, in the presence of passively acquired maternal IgG anti-TT antibodies, the actual Ab production by the infant is delayed. After further vaccinations, the cumulative response rate reached 95%. Infants at 12 months ofage, children at 4 years of age, and adults all mounted an Ab A kl H-Ab a TT H-Ab a HB l TT BSA 1 -- l -I" B pgm 1.0 0.5 0.2 High Medium 0.1 0.05 Low J-j 0.02 Fig l. lT-specific immunoblotting. (AI Specificity of TT-specific immunoblotting (WABL). Abbreviations: H-Ab a TT, human lgGl MoAb against tetanus toxoid (concentration, 0.2 p g / ~ n L ) ~ H-Ab ~; a HB, human lgGl MoAb against hepatitis B surface antigen (concentration, 20.0 pglmL1; lg, blotting on noncoated membrane (signal intensity is related t o protein concentrationl; TT, blotting on TTcoated membrane (only signal ofTT-specific MoAb is obtained with increased intensity); BSA, blotting onBSA-coated membrane (no signal isobtained). (B) Sensitivity of WABL and semiquantitative determination ofhomogeneous antibodies (H-Ab) at low (01.medium (@), and high ( W ) concentration. The values from 0.02 t o 1.0 indicate the concentration rangeof MoAb against TT in micrograms per milliliter. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 4377 CLONAL DYSREGULATION OF THE ANTIBODY RESPONSE CONTROLS AUImL A 0.8 IV D Hetsrogenrour 31.7 Hetaogeneour 1250 with H-Ab < 0.1 p i m L A A BMT PATIENTS Rentrioted heterogenelty (RH) wfth H-Ab 0.1-0.5 D ,WmL 4.7 ID 5.8 II D 16.0 Restrloted lllb heterogenelty (RH) wlth H-Ab 420 10.5 pimL k250 Fig 2. Examples of representativeWABL patterns. (A) WABL pattern of sera from a 4-year-old healthy child (control) before and after DT-IPV booster vaccination (IVD):electrophoretic heterogeneity of lgG a n t i - l l after vaccination. (B) WABL pattern of serum from a 4year-old healthy child (control)before and after DT-IPV booster vaccination (IVD):electrophoretic heterogeneity of IgG anti-TT and presence of H-Abat a low concentration(<0.1 pg/mL). IC)WABL pattern of serum from a 2-year-old boy (after an uncomplicatedBMT for acute myeloblastic leukemia in first remission) after DT-IPV 111 vaccination post-BMT IIIID): restricted electrophoretic heterogeneity (RH) and presence of 7 H-Abof medium concentration (0.1 to 0.5 pg/mL). WABL for IgG subclasses showed H-Ab in all subclasses (data not shown). (D) WABL pattern of sera from a 4-year-old girl (after an uncomplicated BMT for acute lymphoblastic leukemia in second remission) before the first (ID) and after the first, second (113).and third (IIID)post-BMT vaccinations: restricted electrophoreticheterogeneity (RH) and development of H-Ab, of which one was at a high concentration (>0.5 pg/mLI. The figures represent IgG Ab titers to TT in AU per milliliter; 1:250 indicatesthe dilution of serum samples. response after booster vaccination. The geometric mean of the Ab titers (GMT) was highest in children at 4 years of age and lowest in infants at 12 months of age. Pediatric patients. In none of the 4 patients whoreceived a vaccination within 2 days before the start of the conditioning regimen for BMT was anAb response observed. Seventy percent of the other evaluable patients (n = 23) responded to vaccination before BMT (Table 3). irrespective of the prevaccination titer and even when vaccinated as little as S days before the start of the conditioning regimen. The GMT in responders wasmuch lower than in control infants and children, probably as a result of preceding antileukemic treatment. After the first vaccination, at 7 weeks after BMT, 30% of the pediatric recipients responded. There was no statistically significant difference between responders and nonresponders withrespect to prevaccination Ab titers, substitution with gammaglobulins, or treatment with cyclosporin A. Two revaccinations at I 1 and 15 weeks after BMTresulted in a cumulative response rate of 75% of the graft recipients. Although this finding was not investigated systematically. we observed that the maximum Ab titer was reached at 4 weeks or even later after immunization and notat 2 weeks as in adult controls after booster vaccination. Revaccination between 6 and 24 months after BMTresulted in a IO0% response rate and a significantly increased GMT (Table 3). There was no difference between patients with (n = 6) or without ( n = 17) preceding acute GVHD. Booster vaccination at 3 to I O years after RMT resulted in a 100% response rate and a GMT similar to that in controls. Follow-up investigations showed a half-life of Ab titers comparable to that in adult controls (data not shown). Addt patients. There were no significant differences with respect to the percentage of responders between adult patients who received a TCD allogeneic graft (14 of 26) and those who received an autologous graft (4 of 9), nor was there a difference between patients vaccinated 0.5 to 2 years (6 of 17) and those vaccinated more than 2 years after BMT (12 of 18). Also, the GMT was not different between these subgroups. Ten adult patients (about 30%) had an IgG antiTT titer after two DT-IPV immunizations that may not have been protective. ie, less than 0.1 AU/mL. Heterogeneity and Oligoclonnlity qf IgC Anti-TT Controls. TT-specific H-Abwerehardly detectable in cord blood and sera of infants after four DPT-IPV vaccinations (Fig 3A). After revaccination at 4 years of age or in adulthood, either one or two TT-specific H-Ab of low concentration (<0.1 pg/mL) could be observed in serum samples of about 35% of the controls, on top of an overall heterogeneous Ab response (Figs 2B and 3A). BMT patients. TT-specific H-Ab oflow concentration could be observed in preimmunization serum samples of about 25% of the pediatric patients before BMT (Fig 3B). After pre-BMT vaccination, this percentage was SO%, which was not significantly different from healthy children at the age of 4 years and from adults. However, after the first and second post-BMT vaccination, it increased significantly to 75% and 10096, respectively. In addition, the number of HAb per serum sample and the quantity of some H-Abincreased (Figs 2C and D and 3B). After booster vaccination in thesecondhalf year after BMT, H-Ab ata medium and high concentration were found in about SO% of the patients. At follow-up investigation, 3 to I O years after BMT, 7S% of the patients still had H-Ab in their serum. In some cases, these H-Ab were of relatively high concentration, ie, greater than 1.O p d m L (Figs 2D and 3B). In about 30% of the adult graft recipients who responded to TT vaccination, the postimmunization serum showed HAb. These H-Ab were also frequently at a relatively high concentration. In general, there was a strong correlation between the presence and concentration of H-Ab and the quan- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. GERRITSEN ET 4378 Table 3. Quantification of IgG Anti-TT Antibodies After Vaccination Before Vaccination Origin of Serum Samples Response to D(P)T-IPV I Healthy infants9 (3 mo) Pediatric patients (7 wk) Response to D(P)T-IPV II (cumulative) Healthy infants (4 mo) Pediatric patients (1 1 wk) Adult patients ( 18 S mo) Response to D(P)T-IPV 111 (cumulative) Healthy infants (5mo) Pediatric patients (15 wk) Response to booster vaccination A. Controls Infants (12 mo; 19 IV) Children (4 yr; 17 V) Adults (B) 20 B. Pediatric patients Before BMT (-3 wk; 0) 6-24 mo after BMT (IV) >36 mo after BMT (V) Individuals Investigated 20 30* Individuals With Response 9 Responders GMT 15 17 0.44 79 (54-941 0.03-12.3 0.3-9.8 2.6 59 (39-76) NE NE 51 (34-67) 20 24 19 18 95 (75-99) 75 (53-90) 231 23 21 100 (82-100) 100 (80-100) 0.3-9.1 100 (83-100) 16 23 21 Range (47-87)#70 0.1-21.9 100 (88-100) 0.1-14.0 100 (84-100) GMT 0.3-12.30.94 4.5 0.01-0.96 0.03 45 (23-68) 0.5-6.6 2.1 30 (15-49) 19 29** 35 19 17 20 Afier Vacclnatlon % (+2 S D ) 3.5 1.8-31 5.5 1.3-128 8.2 Range 2.8-14.0t 0.7-52.9 .O 2.5 4.4 0.7-53.3 0.3-52.9 0.4-31.0 1.7-57.0 5.1 8.8 1.5 0.8 3.2 0.1-5.9 0.4-4.5 9.0 34.9 15.4 1.3-77.5511 14.2-83.211 4.6-81.411 1.4 2.3 1.6 0.2-6.4 4.9 79.7 27.5 1.0-17.1/1 1.0-184.011 2.4-159.01[ Abbreviations: GMT, geometric mean of lgG anti-lT antibody levels (AU/mL) in serum of responders before and one month after vaccination; NE, not evaluated. * Patients with acute GVHD (n = 8 ) were excluded. t P < .05. One serum sample after vaccination was not available. 5 Values are extrapolated from 4 children investigated 1 month after DPT-IPV IV at 14 months and from 15 children 3 months after DPT-IPV IV at 11 months of age, respectively. /I P < ,001. using analysis of variance; the difference of the GMT of antibody titers after booster vaccination was significant between all subgroups. 1 Patients vaccinated less than 8 days before BMT (n = 4) were excluded. # P < 0.001; using analysis of variance, the response percentage to booster vaccination in pediatric patients before BMT was significantly less than after BMT, and in comparison with controls. * tity of IgG anti-TT in postvaccination sera of BMT recipients. Combination of the quantitative and qualitative data indicates that 40% of the sera with IgG anti-TT levels less than 20 AU/mL contained H-Ab, 20% of whichwere of medium or high concentration. H-Ab were present in 70% of the sera with IgG anti-TT levels greater than 20 AU/mL; 60% of these H-Ab were at a medium or high concentration. In 7 pediatric graft recipients with H-Ab at a high concentration in the first yearafter BMT, WABL and FABL showed that, at 3 to 10 years after BMT, 2 graft recipients had a heterogeneous Ab response and 3 had a restricted pattern with H-Ab produced by the original B-cell clone(s) (Fig 4). The other 2 cases showed, in addition to H-Ab produced by the original B-cell clone, H-Ab at a high concentration produced by new clones, obviously triggered by revaccination. DISCUSSION Our previous study on the recovery of serum Ig isotypes and the occurrence ofMG after BMT’ was extended here to investigate the quantity and quality, in terms of electrophoretic heterogeneity, of the specific IgG Ab formation after vaccination with the T-cell-dependent TT antigen. In accordance with previous reports,”1owe found a quanti- tatively decreased Ab production in recipients of a BM graft early after BMT in comparison with the response on a booster vaccination in healthy controls (but not in comparison with infants who received the first course of 3 vaccinations). IgG antibodies to TT are producedbymemory B cells with the help of T cells. Early after BMT, the number of memory B cells may be low. It has also been shown that the number of T-helper cells and precursors is low.26 In addition, the production of and response to interleukin-2 (IL2) is de~reased~’.’~ and this has a detrimental effect on the proliferative response after stimulation of T cells via the Tcell receptor-CD3 complex by antigens andanti-CD3.28,2’ Therefore, it seems paradoxical that specific Ab production to recall antigens in BMT recipients precedes normalization ofin vitro T-cell responses by a number of months.‘ This finding is in contrast to the finding of a relatively high number of CD4’ CD45RO’ T lymphocytes in peripheral blood after BMT,30unless this population belongs to the TH2 subset.31”2 Alternatively, the majority of T cells in the germinal centers of BMT recipients may be activated by other as yet unknown mechanisms. It is attractive to speculate that alloantigens may be involved in this activation. B cells may interact with activated T cells in a major histocompatibility complex (MHC)-unrestricted and antigen nonspecific way From www.bloodjournal.org by guest on February 6, 2015. For personal use only. CLONAL DYSREGULATION OF THE ANTIBODY RESPONSE CONTROLS A I % V II v IV 111 v v V B V V 100. B PATIENTS v 6-12111 adults >36m v >6m children before BMT after BMT Fig 3. Percentage (and 95% confidence intervals) ofresponders with H-Ab in IgG anti-TT. (A) Healthy pediatric and adult controls before (b) and after (a1 the indicated D(P)T-IPV vaccination (V).(B) Pediatric patients before and after BMT and adult patients after BMT. The sequential DT-IPV vaccinations are indicated (V,see also Table 2). Sera were investigated by WABL before (b) and after (a) vaccination. Note themarked difference in frequency ( * P < .01, **P < .001) and concentration of H-Ab in patients compared with children after DT-IPV V and adults after boostervaccination (see also Fig 2). H-Ab at a (0)low, (W) medium, and (W) high concentration, respectively. The numbersindicate the number of individualsinvestigated all individuals were analyzed before (b) vaccination; only samples of responders were investigated after (a) vaccination. and proliferate and mature to Ig-producing cells in the presence of interleukins (ie, IL-4 and IL-10).31”4Interestingly, Ig levels in graft recipients with acute GVHD are significantly higher than in recipients witho~t.~’ In the present study, we showed that the occurrence of HAb at a low concentration within an otherwise heterogeneous response is a normal phenomenon, because this type of clonal dominance was also found in healthy children after DT-IPV V and in adult controls after booster vaccination. Clonal dominance has also been described in adults after influenza vaccination.36However, in BM graft recipients, the restricted heterogeneity of TT-specific IgG and the development of H-Ab at a relatively high concentration has to be considered as an abnormal response. This oligoclonal Ab response was found both in children receiving grafts of unmodifiedBMand vaccinated before and early after BMT and in adults receiving grafts of either autologous or T-cell- 4379 depleted allogeneic BM who did not receive revaccination early after BMT. Previous studies in immune-deficient mice and in Rhesus monkeys after BMT also showed a similar r e s p o n ~ e . ~There ~ . ~ ’ are at least two possible explanations for this restricted response of prolonged duration. First, it may be the result of the transfer of a limited number of memory B-cell clones from the donor. This hypothesis is in accordance with the finding of a skewed Ig VH repertoire of B cells early after BMT.39 Under certain conditions, booster vaccination of the BM donor 2 weeks before donation has been shown to increase the quantitative Ab response in the recipient^.'^"'"^ On careful observation of the data presented in some of those it can be concluded that this response was also oligoclonal. Second, it may be that only a limited number of memory B cells become activated in view of the restricted possibilities for cell-cell contact with T-helper cells, resulting from underrepresentation of the latter population in germinal centers after BMT. Results of animal experiments are in favor of the latter hypothesis because restricted heterogeneity of Ig and H-Ig develop after thymectomy and disappear again after infusion of peripheral T ~ e l l s . 4However, ’ ~ ~ ~ the persistence of a restricted Ab response and of H-Ab of high concentration in a number of graft recipients many years after BMT, when numbers and functions of specific T cells have become normal,’ indicates that, in addition to abnormalities at the T-cell level, abnormalities at the B-cell level may persist. In murine graft recipients, germinal center reconstitution after BMT has been shown to be oligoclonal after antigenic stimulation? In human BMT, a delayed reconstitution of germinal centers has been described in cases with GVHD.44 Our findings of an impaired specific Ab response postBMT have clinical implications with respect to vaccination policy of BMT recipients. Previous studies showed longlasting but transient persistence of donor immunity in nonvaccinated BMT recipient^.^^.^"^^ Vaccination of the donor before graft donation, together with vaccination of the recipient early after BMT, may contribute to a quantitatively good Ab response. BM graft recipients respond to vaccinations in the following sequence: TD-recall antigens (at about 3+ months), TD-primary antigens (at about 6+ months), and Tcell-independent antigens (atabout l + year).’ This sequence can be observed after BMT with either an unmodified graft,’ a T-cell-depleted graft,I5.l6 or a B-cell depleted graft.47,48 However, under the latter condition, all responses are primary because of the lack of transferred memory Bcell clones.47In the present study, we showed that repeated vaccinations of children early after BMT resulted ina quantitatively enhanced specific humoral immunity at 6 to 24 months after BMT, whereas this response in adults was not yet normal at2 years post-BMT after two vaccinations. However, we do not know whether the qualitative abnormalities, present as a clonally restricted response, will provide adequate protection. It may be that increased quantity compensates for decreased quality of antibodies in the first years after BMT. With our very sensitive technique we have clearly shown long-lasting oligoclonality attheB-cell level after BMT. Preliminary data on the T-cell receptor repertoire, which is of relevance for antigen-specific help for B cells, do not indicate a long-lasting oligoclonality at the T-cell level4’ From www.bloodjournal.org by guest on February 6, 2015. For personal use only. GERRITSENET 4380 WABL A 1984 P I P 1992 B t 1986 1992 C AU/mL 1:250 20.0 t250 1:25 29.0 1:250 150 8.0 1:500 1:400 112.0 1150 10.0 , 1985 1992 FA6 L 1:250 -t AL l ~ 1500 Fig 4. Follow-up investigation of H-Ab in IgG a n t i - n in 3 patients after BMT. WABL (antigen-specific immunoblotting after agar gel electrophoresis) and FABL (antigen-specific immunoblotting afterisoelectric focusing) patterns ofsera from 3 children early after BMT (obtained after DT-IPV 111) and 6 t o 8 years later (obtained after DT-IPV V).(A) Sera of 1984 and of1992 showed an almost identical Ab pattern of restricted electrophoretic heterogeneity and the presence of a l"-specific H-Ab at a high concentration. WABL combined with IgG subclass and light chain type immunoblotting identified this H-Ab as lgGl K (data not shown). FABL patterns showed identityof the dominantclone. The pattern of the latter serum also shows some changes in the expression level of other clones. (B) The serum of 1986 showed a restricted patternand an H-Ab at a high concentration. The serum of 1992 showed a more heterogeneous pattern with other dominant clones in addition t o the original clone. (C) The serum of 1985 showed a restricted pattern with an H-Ab at a high concentration. The serum of 1992 showed a heterogeneous pattern. The values from 8.0 t o 112.0 represent the lgG Ab titer toTT in AU per milliliter. The values from 1:25 t o 1:500 indicate the dilution of the serum samples. ACKNOWLEDGMENT The authors thank D. Paddenburg for skilful technical assistance. REFERENCES I , Lum LC: Immune recovery after bone marrow transplantation. Hematol Oncol Clin North Am 4:659, 1992 2. Storek J, Saxon A: Reconstitution of B-cell immunity following bone marrow transplantation. Bone Marrow Transplant 9:395, 1992 3. Kagan JM, Champlin RE, Saxon A: B-cell dysfunction following human bone marrow transplantation: Functional-phenotype dissociation in the early posttransplant period. Blood 74:777, 1989 4. Small TN, Keever CA, Weiner-Fedus S , Heller G , O'Reilly RJ, Flomenberg N: B-cell differentiation following autologous, conventional or T-cell depleted bone marrow transplantation: A recapitulation of normal B-cell ontogeny. Blood 761647, 1990 5. Aucouturier P, Barra A, lntrator L, Cordonnier C, Schulz D, Duarte F, Vernant JP, Preud'homme JL: Long lasting IgG subclass and antibacterial polysaccharide Ab deficiency after allogeneic bone marrow transplantation. Blood 70:779, 1987 6. Sheridan JF, Tutschka PJ, Sedmak DD, Copelan EA: Immunoglobulin G subclass deficiency and pneumococcal infection after allogeneic bone marrow transplantation. Blood 75:1583, 1990 7. Gerritsen EJA, van To1 MJD, Lankester AC, van der Weijden- Ragas CPM, Jol-van der Zijde CM, Oudeman-Gruber NJ, Rad1 J, Vossen JM: Immunoglobulin levels and monoclonal gammopathies in after bone transplantation. Blood 82:3493, 1993 8. Mitus AJ, Stein R,Rappepo; JM, Antin JH, WeinsteinHJ, Alper CA, Smith BR: Monoclonal and oligoclonal gammopathy after bone marrow transplantation. Blood 742764, 1989 9. Witherspoon RP, Storb R, Ochs HD, Flournoy N. Kopecky U, Sullivan KM, Deeg HJ, Sosa R, Noel DR. Atkinson K, Thomas ED: Recovery of antibody production in human allogeneic marrow graft recipients; influence of time post-transplantation, the presence or absence of chronic graft-versus-host disease. and antithymocyte globulin treatment. Blood 58:360, 1981 IO. Shiobara S , Lum LC, Witherspoon RP, Storb R: Antigenspecific antibody responses of lymphocytes to tetanus toxoid after human marrow transplantation. Transplantation 41567, 1986 11. Ljungman P, Fridell E, Lonnqvist B, Bolme P, Bottinger M, Gahrton G , Linde A, RingdCn 0, Wahren B: Efficacy and safety of vaccination of marrow transplant recipients with a live attenuated measles, mumps and rubella vaccine. J Infect Dis 159:610, 1989 12. Ljungman P, Wiklund-Hammarsten M, Duraj V, Hammarstrom L, Lonnqvist B, Paulin T, RingdCn 0, PepeMS, Gahrton G : Response to tetanus toxoid immunization after allogeneic bone marrow transplantation. J Infect Dis 162:496, 1990 13. Ljungman P, Duraj V, Magnius L: Response to immunization against polio after allogeneic marrow transplantation. Bone Marrow Transplant 7:89, 1991 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. CLONAL DYSREGULATION OF THE ANTIBODY RESPONSE 14. Saxon A, Mitsuyasu R, Stevens R, Champlin RE, Kimata H, Gale RP: Designed transfer of specific immune responses with bone marrow transplantation. J Clin Invest 78:959, 1986 15. Wimperis JZ, Brenner MK, Prentice HG, Reittie JE, Karayiannis P, Griffiths PD, Hoffbrand AV: Transfer of a functioning humoral immune system in transplantation of T-lymphocyte-depleted bone marrow. Lancet 1:339, 1986 16. Wimperis JZ, Gottlieb D, Duncombe AS, Heslop HE, Prentice HG, Brenner MK: Requirements for the adoptive transfer of antibody responses to a priming antigen in man. J Immunol 144:541, 1990 17. Labadie J, To1 van MJD, Dijkstra NH, Zwaan FE, Vossen JM: Transfer of specific immunity from donor to recipient ofan allogeneic bone marrow graft: Effect of conditioning on the specific immune response of the graft recipient. Br J Haematol80:381, 1992 18. Labadie J, To1 van MJD, Dijkstra NH, van der Kaaden M, Jolvan der Zijde CM, de Lange GG, Zwaan FE, Vossen JM: Transfer of specific immunity from donor to recipient ofan allogeneic bone marrow graft: Evidence for donor origin of the antibody producing cells. Br J Haematol 82:437, 1992 19. Vossen JM, Heidt PJ, van den Berg H, Gerritsen EJA, Hermans J, Dooren LJ: Prevention of infection and graft-versus-host disease by suppression of intestinal microflora in children treated with allogeneic bone marrow transplantation. Eur J Clin Microbiol Infect Dis 9:14, 1990 20. van Leeuwen JEM, van To1 MJD, Joosten AM, Wijnen JTh, Meera Khan P, Vossen JM: Mixed T-lymphoid chimerism after allogeneic bone marrow transplantation for hematological malignancies of children is not correlated with relapse. Blood 82:1921, 1993 2 1. Wagemaker G, Heidt PJ, Merchav S, van Bekkum DW: Abrogation of histoincompatibility barriers in Rhesus monkeys, in Baum SJ, Ledney CD, Thierfelder S (eds): Experimental Haematology Today. Basel, Switzerland, Karger, 1982, p 111 22. Jol-van der Zijde CM, van der Kaaden M, Rumke HC, Gemtsen EJA, Vossen JM, van To1 MJD: The antibody response against tetanus toxoid: A longitudinal study in healthy infants and adults, in Chapel HM, Levinsky RJ, Webster ADB (eds): Progress in Immune Deficiency 111. London, UK, Royal Society of Medicine Services Ltd, 1991, p 238 23. Nooy FJM, van der Sluijs-Gelling AJ, Jol-van der Zijde CM, van To1 MJD, Haas H, Radl J: Immunoblotting techniques for the detection of low level homogeneous immunoglobulin components in serum. J Immunol Methods 134:273, 1990 24. Gemtsen EJA, Wels JMA, Jol-van der Zijde CM, Riimke HC,Vossen JM, Radl J, van To1 MJD: Restricted heterogeneity of IgG anti-tetanus toxoid antibodies after allogeneic bone marrow transplantation, in Chapel HM, Levinsky RJ, Webster ADB (eds): Progress in Immune Deficiency 111. London, UK, Royal Society of Medicine Services Ltd, 1991, p 124 25. Tiebout RF, Stricker EAM, Hagenaars R, Zeijlemaker W P Human lymphoblastoid cell line producing protective monoclonal IgGlK anti-tetanus toxin. Eur J Immunol 14:399, 1984 26. Rozans MK, Smith BR, Burakoff SJ, Miller RA: Long-lasting deficit of functional T-cell precursors in human bone marrow transplant recipients revealed by limiting dilution methods. J Immunol 136:4040, 1986 27. Warren HS, Atkinson K, Pembrey RG, Biggs JC: Human bone marrow allograft recipients: Production of, and responsiveness to, interleukin 2. J Immunol 131:1771, 1983 28. Roosnek EE, Brouwer MC, Vossen JM, Roos MThL, Schellekens PThA, Zeijlemaker WP, Aarden LA: The role of interleukin2 in proliferative responses in vitro of T cells from patients after bone marrow transplantation. Transplantation 432355, 1987 29. Yamagami M, McFadden PW, Koethe SM, Ratanatharathorn V, Lum LG: Failure of T-cell receptor-anti-CD3 monoclonal antibody interaction in T cells from marrow recipients to induce increases in intracellular ionized calcium. J Clin Invest 85:1347, 1990 4381 30. Gorla R, Airo P, Ferremi-Leali P, Rossi G, Prati E, Brugnoni D, Cattaneo R: Predominance of “memory” phenotype within CD4’ and CD8’ lymphocyte subsets after allogeneic BMT. Bone Marrow Transplant 11:346, 1993 (letter) 31. van den Eertwegh AJM, Noelle M,RoyM, Shepherd DH, Aruffo A, Ledbetter JA, Boersma WJA, Claassen E: In vivo CD40gp 39 interactions are essential for thymus dependent humoral immunity. I. In vivo expression of CD40 ligand, cytokines, and antibody production delineates sites of cognate T-B cell interactions. J Exp Med 178:1555, 1993 32. Elghazali GEB, Paulie S, Andersson G, Hansson Y,Holmquist G, Sun JB, Olsson T, Ekre HP, Troye-Blomberg M: Number of interleukin-4- and interferon-y-secreting human T cells reactive with tetanus toxoid and the mycobacterial antigen PPD or phytohemagglutinin: Distinct response profiles depending onthe type of antigen used for activation. Eur J Immunol 23:2740, 1993 33. Noelle RJ, Ledbetter JA, Aruffo A: CD40 and its ligand, an essential ligand-receptor pair for thymus-dependent B-cell activation. Immunol Today I3:43 1, 1992 34. Parker DC: T cell-dependent B cell activation. AnnuRev Immunol 1 1:331, 1993 35. Noel DR, Witherspoon RP, Storb R, Atkinson K, Doney K, Mickelson EM, Ochs HD, Warren RP, Weiden PL, Thomas ED: Does graft-versus-host-hsease influence the tempo of immunologic recovery after allogeneic human marrow transplantation? An observation on 56 longterm survivors. Blood 51:1087, 1978 36. Radl J, Hoogeveen CM, van den Wall Bake AWL, Mestecky J: Clonal antibody dominance after influenza vaccination in IgA nephropathy patients and controls, in McGhee J, Mestecky J, Tlaskalova H, Strzl J (eds): Recent Advances in Mucosal Immunology. New York, NY, Plenum, 1994 (in press) 37. van den Berg P, Radl J, Lowenberg B, Swart ACW: Homogeneous antibodies in lethally irradiated and autologous bone marrow reconstituted Rhesus monkeys. Clin Exp Immunol 23:355, 1976 38. Radl J, van der Sluijs-Gelling AJ, Hoogeveen CM, MinkmanBrondijk M,Nooy FJM: Influence of antigenic stimulation at young age on the development of monoclonal gammapathies in the aging C57BL mice, in Rad1 J, van Camp B (eds): Monoclonal Gammapathies 11-Clinical Significance and Basic Mechanisms. Rijswijk, The Netherlands, EURAGE, 1989, p 229 39. Fumoux F, Guigou V, Blaise D, Maraninchi D, Fougereau M, Schiff C: Reconstitution of human immunoglobulin VH repertoire after bone marrow transplantation mimics B-cell ontogeny. Blood 81:3153, 1993 40. Lum LG, Seigneuret MC, Storb R: The transfer of antigenspecific humoral immunity from marrow donors to marrow recipients. J Clin Immunol 6:389, 1986 41. Benner R, van den Akker ThW, Rad1 J: Monoclonal gammapathies in immunodeficient animals-A review, inRadl J, Hijmans W, van Camp B (eds): Monoclonal Gammapathies I: Clinical Significance and Basic Mechanisms. Rijswijk, The Netherlands, EURAGE, 1985, p 97 42. van den Akker ThW, Tio-Gillen AP, Solleveld HA, Benner R, Radl J: The influence of T cells on homogeneous immunoglobulins in sera of athymic nude mice during aging. Scand J Immunol 28:359, 1988 43. Kroese FGM, Wubbena AS, Seyen HG, Nieuwenhuis P: Germinal centers develop oligoclonally. Eur J Immunol 17:1069, 1987 44. Sale GE, Alavaikko M, Schaefers KM, Mahan W. Abnormal CD4:CDS ratios and delayed germinal center reconstitution in lymph nodes of human graft recipients with graft-versus-host disease (GVHD): An immunohistological study. Exp Hematol 20: 1017, 1992 45. Lum LG, Munn NA, Schanfield MS, Storb R: The detection of specific antibody formation to recall antigens after human bone marrow transplantation. Blood 67:582, 1986 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 4382 46. Jin NR, Lum LC: IgG anti-tetanus toxoid antibody production induced by Epstein-Barr virus from B cells of human marrowtransplant recipients. Cell Immunol 101:266, 1986 47. Bar BMAM,Santos GW, DonnenbergAD:Reconstitution of antibody response after allogeneic bone marrow transplantation: Effect of lymphocyte depletion by counterflow centrifugal elutriation on the expression of hemagglutinins. Blood 76:1410. 1990 48.Baumgartner C, Morel1 A, Hirt A,Bucher U, ForsterHK, GERRITSEN ET AL Doran JE, Matter L, Brun del Re G, Wagner HP: Humoral Immune function in pediatric patients treated with autologous bone marrow transplantation for B cell non-Hodgkin’s lymphoma. The influence of ex vivo marrow decontamination with anti-Y 29/55 monoclonal antibody and complement. Blood 7 1 : 12 I 1, 1988 49. Rencher SD, Manif 1, Heslop HE, Turner VE, Brenner MK, Hunvitz JL: Reconstitution of the T-cell receptor c@ repertoire in recipients of allogeneic BMT. Bone Marrow Transplant 10521. 1992 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1994 84: 4374-4382 Clonal dysregulation of the antibody response to tetanus-toxoid after bone marrow transplantation EJ Gerritsen, MJ Van Tol, MB Van 't Veer, JM Wels, IM Khouw, CR Touw, CM Jol-Van Der Zijde, J Hermans, HC Rumke and J Radl Updated information and services can be found at: http://www.bloodjournal.org/content/84/12/4374.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.










© Copyright 2026