
Selective Expression of CD45 Isoforms Defines CALLA
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
Selective Expression of CD45 Isoforms Defines CALLA’ Monoclonal B-Lineage
Cells in Peripheral Blood From Myeloma Patients as Late Stage B Cells
By Gitte S.Jensen, Michael J. Mant, Andrew J. Belch, James R. Berenson, Bernard A. Ruether, and Linda M. Pilarski
The peripheral blood lymphocytes from 42 patients with
multiple myeloma (MM) and 13 patients with monoclonal
gammopathy of undetermined significance (MGUS) were
studied by three-color immunofluorescence (IF) using antibodies directed to a broad range of B-cell markers (CD19, CD20,
CD21, CD24). CALLA (CD10). PCA-1 (a plasma cell marker),
and t o the high and low molecular weight isoforms of the
leukocyte common antigen, CD45RA (p205/220) and CD45RO
(p180). CD45RA is expressed on pre-B and B cells, and a
transition from CD45RA t o CD45RO defines differentiation
towards plasma cells. Peripheral blood mononuclear cells
(PBMC) from patients with myeloma included a large subset
of B-lineage cells (mean of 39% t o 45%) that were CALLA+
and PCA-l+in all patients studied, including newly diagnosed
patients and patients undergoing chemotherapy. Southern
blot analysis indicated the presence of monoclonal Ig rearrangements in PBMC and a substantial reduction in the
germ-line bands consistent with the presence of a large
monoclonal B-cell subset. Avoidance of purification methods
involving depletion of adherent cells was essential for detec-
tion of the abnormal B cells. Phenotypically, this abnormal
B-cell population corresponded t o late B or early pre-plasma
cells (20% t o 80% of PBMC), as defined by the concomitant
expression of low densities of CD19 and CD20, moderate
densities of CALLA and PCA-1, and strong expression of
CD45RO on all B cells, with weakly coexpressed CD45RA on a
small proportion. Heterogeneity in the expression of CD45RA
and CD45RO within the abnormal B-cell population from any
given patient suggested multiple differentiation stages. Abnormal B cells similar t o those in M M were also detected in
MGUS, although as a lower proportion of PBMC (26%).
Abnormal B cells from patients with MGUS expressed predominantly the CD45RO isoform, but had a lower proportion
of CALLA+and PCA-1+cells than were found on B cells from
MM. This work indicates that the large subset of circulating
monoclonal B lymphocytes from myeloma patients are at a
late stage in B-cell differentiation, continuously progressing
towards the plasma cell stage.
Q 1991b y The American Society of Hematology.
M
a distinction is only made between high and low molecular
mass isoforms, because the monoclonal antibodies (MoAbs) available recognize either the low molecular mass
isoform, 180-Kd isoform, UCHL-1,29,30
termed CD45R0, or
the high molecular mass 205/220-Kd isoform, termed
CD45RA, and defined by a large number of MoAbs. The
expression of CD45 isoforms has been extensively studied
for T cells, and has been a valuable tool for identifying
Antigen-inexperistages of thymocyte differentiati~n.”.’~
enced T cells bear CD45RA only, but with activation
CD45RA is gradually lost concomitant with the acquisition
of CD45RO. Coexpression of both isoforms delineates a
transitional stage of differentiati~n.~~.’~
We have recently
shown that a similar transition from expression of the high
(CD45RA) to the low (CD45RO) molecular mass isoforms
of the CD45 antigen also characterizes normal B-cell
~ , ~B cells express
differentiati~n.~~
All stages of p ~ e - B ’and
the high molecular mass isoform CD45RA; a transition to
the low molecular mass CD45RO occurs late after B-cell
activation. Consequently, as normal B cells differentiate
ULTIPLE MYELOMA (MM) has traditionally been
regarded as a malignancy that, at least initially, is
predominantly sited in the bone marrow (BM). It is
characterized by osteolytic bone lesions and/or osteoporosis, a large monoclonal Ig component, and infiltration of the
BM with often atypical plasma cells.’vzIn these patients, the
ability to produce polyclonal Ig is severely reduced? as is
thc umber of normal, polyclonal B cells in peripheral
b!
mononuclear cells (PBMC).’ The remaining B cells
h.
high proportion of anti-idiotypic reacti~ity.~,~
Howe!
ecent studies have shown that B cells belonging to the
ma’ ,iant clone are also present in the peripheral blood
(PB)?I4 These cells were originally thought to be pre-B
cells, based on the surface expression of the CALLA
antigen (CD10),’03’5-’9
a neutral endopeptidase:’ expressed
on all fetal pre-B and B cells,” on adult pre-B cells,22on
C-ALL cells,z3and a variety of other lymphohematopoietic
ma1ignan~ies.I~
However, the abnormal PBMC B cells in
myeloma also express the plasma cell markers PCA-1 and
PC-1, as well as other plasma cell markers.8,’o-’2Thus,
controversy exists regarding the phenotype and stage of
differentiation of this PB monoclonal B-cell subset, and as
to whether the cells are pre-B cells abnormally expressing
PCA-1 or plasma cells with anomalous CALLA expression.
BecPwe the subset is thought to be part of the malignant
clone, aberrant expression of markers not normally present
at a particular stage of differentiation may be expected.
However, the CALLA antigen has recently been described
on activated B cells,24and its expression does not seem
confined to early B-cell stages of differentiation.
The leukocyte common antigen, CD45, is a family of
transmembrane glycoproteins composed of different isoforms transcribed from a single gene and processed through
alternative splicing of messenger RNA (mRNA).25There
exist at least four different isoforms with molecular masses
of 180, 190, 205, and 220 Kd, respectively, each having
different glycosylations.26-28
Usually, in phenotypic analysis,
Blood, Vol78, No 3 (August 1). 1991: pp 711-719
From the Departments of Immunology and Medicine, University of
Alberta, Edmonton; the Department of Medicine, University of Calgary, Alberta, Canada; and the VA Wadsworth-UCLA Medical
Center, Los Angeles, CA.
Submitted November 7,1990; accepted April 3, 1991.
Supported by the National Cancer Institute of Canada. G.S.J.is an
Alberta Cancer CenterBoard Research Fellow, previously supported by
the Danish Cancer Society and the Danish Medical Research Council.
Address reprint requests to Linda M. Pilarski, PhD, Department of
Immunology, 845E Medical Science Bldg, University of Alberta,
Edmonton, Alberta, Canada T6G 2H7.
The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with 18 U.S.C.section I734 solely to
indicate this fact.
0 1991 by The American Society of Hematology.
0006-4971I9117803-0028$3.00/0
711
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
JENSEN ET AL
712
The cells were incubated for 45 minutes at 4"C, centrifuged at 2,000
towards pre-plasma cells, they lose surface CD45RA and
rpm for 3 minutes, and washed twice in cold PBS + FCS + NaAz.
acquire CD45RO. Early plasma cells continue to express the
After resuspension in 50 pL goat-antimouse Ig Biotin, the cells
low molecular weight CD45RO isoform only, while end
stage plasma cells eventually lose all CD45 e ~ p r e s s i o n . ' ~ ~ ~ ~were incubated for 30 minutes at 4°C. After washing twice in
PBS + FCS + NaAz,the cells were resuspended in PBS + FCS +
In this study, analysis of CD45 isoform expression has
NaAz containing 1 pg/mL IgG from mouse serum (BioCan) for
been used to define the stage of differentiation of the PB
blocking, and incubated for 10 minutes at room temperature. Cells
monoclonal CALLA+ PCA-1' B-lineage cells in MM. Our
were centrifuged and resuspended in 20 ILL Streptavidin
data show that a large proportion (20% to 80%) of PBMC
DUOCHROME or TANDEM. The other two MoAbs coupled to
from MM patients belong to a pre-plasma cell stage of
FITC and PE were added directly and 25 ILLof PBS + FCS +
differentiation, defined by concomitant expression of CD19,
NaAz added. This mixture was incubated for 20 minutes at 4°C.
PCA-1, and CD45RO. Monoclonality of these cells was
Cells were washed twice and fixed in 1% formalin for flow
cytometric analysis.
confirmed by Southern blot analysis of Ig rearrangements.
~
b
~
e
~
~
a
t
i
o
n
the
~
,
abnor'
~
~
'
~
~ Analysis
~ ~ ~ ~ of
~ the three-color IF. Samples were analyzed on a
In accordance with earlier
FACScan (Becton Dickinson) in which a single laser was used to
mal B cells in PB of MM patients express the CALLA
excite FITC (green), PE (orange), and DUOCHROME (red).
antigen. The coexpression of PCA-1 and CD45RO on the
Dead and red cells were excluded by gating on fonvard-angle light
abnormal B-cell subset of PBMC in MM patients defines
scatter. Files were collected of 20,000 cells from each sample, and
this subset as late B cells or early pre-plasma cells.
information was obtained on the three fluorochromes along with
MATERIALS AND METHODS
the side scatter as a measure of the granularity of the stained cells.
We did not set any gates on forward-angle light scatter and side
scatter, because the abnormal B-cell subsets are enlarged and
highly granular compared with normal circulating B cells. Threecolor data was analyzed from list mode by electronic gating on
CD19' cells followed by analysis of the other two markers. Controls
for CD19-FITC (direct) and CD19DUOCHROME or TANDEM
(indirect) were IgG1-FITC or IgGlDUOCHROME, respectively.
The controls for the rest of the antibodies were evaluated by gating
on CD19' cells, and then defining the background fluorescence
using isotype-matched control antibodies. When evaluating the
expression of any given surface marker, the samples were gated on
basis of CD19 positivity, and the gates were set according to the
corresponding isotype background. This procedure was crucial to
correct interpretation, because in indirect IF the abnormal B-lineage cells from the myeloma patients have high backgrounds, as do
normal B cells. Distinguishing between dimly and brightly positive
cells, and in comparison with identically gated isotype control
staining, CD19-FIT(?" was between channels 200 and 350, and
CD19-FITPgh'between channels 360 and 500. CD20-FITC/RDd'"
was between channels 180 and 500, and CD20-FITC/RDbngh'was
between channels 500 and 1,012. For CD19iTANDEM (indirect
IF) a dim expression was from channel 250 to 500, and a brighter
expression was from channel 500 to 1,012.
Southem blot analysis. Genomic DNA was prepared from
PBMC and granulocytes from normal donors and myeloma patients. Parallel samples of the DNA were digested with either
BamHI, EcoRI, or Hind111 (Bethesda Research Laboratories,
Bethesda, MD) overnight. The digested DNA was size-fractionated by electrophoresis in 0.7% agarose gels at 1V/cm for 48 hours,
and transferred to nylon membranesy3 Samples of similarly
digested DNA from normal granulocytes and patients' PBMC were
run in parallel lanes on the same agarose gel. The recombinant
probe for the human heavy chain Ig gene segment J, was kindly
provided by Dr P. Leder (Harvard Medical School, Boston MA).
The 2.5-kb Sau3A restriction fragment5' was cut and purified,
labeled with '*P-CTP (Amersham, Quebec, Canada) and hybridized with the DNA overnight. Autoradiography using X-ray films
and intensifying screens was performed at -70°C overnight, or up
to 5 days.
Patients. After informed consent was obtained, studies were
performed on PBMC from 42 patients with MM, of which 21
patients were receiving intermittent chemotherapy treatment, and
21 patients were studied at the time of diagnosis before any
treatment. Thirteen patients diagnosed as having a monoclonal
gammopathy of undetermined significance (MGUS) were also
studied.4'," Patients receiving chemotherapy were studied at least 4
weeks after the most recent treatment. To define the phenotypic
characteristics of normal B-lineage cells, we performed parallel
analysis on PBMC from 12 healthy individuals.
Purification ofPBMC. PBMC were purified by centrifugation of
heparinized blood over a Ficoll-Paque (Pharmacia, Domal, Quebec, Canada) density gradient. The cells recovered from the
interface were washed twice in RPMI (GIBCO, Grand Island, NY)
and resuspended in phosphate-buffered saline (PBS) plus 1% fetal
calf serum (FCS; HyClone Labs, Logan, UT) plus 0.1% sodium
azide (NaAz) for immunofluorescence (IF) studies. We have
avoided any manipulations such as carbonyl iron depletion or
plastic adherence normally used for monocyte depletion because
the abnormal B cells in MM are adherent and are depleted by
these procedures. Normal B cells are not depleted and the
procedure does not affect the intensity of staining with CD19 or
CD20.
Antibodies. The following MoAbs directly coupled to a fluorochrome were purchased from Becton Dickinson (San Jose, CA):
IgGl fluorescein isothiocyanate (FITC), IgGl phycoerythrin (PE),
IgG2FITC, IgG2PE, HLE-lFITC(CD45), LeuM3PE(CD14),
Leu2FITC(CD8), Leu3PE(CD4), and Leu4PE(CD3). From Coulter
(Hialeah, FL) we purchased mouse-antihuman IgMPE,
J5FITC(CD10), B4FITC(CD19), BlFITC(CD20), B2RD(CD21),
and PCA-1. The following antibodies were used for indirect
staining with goat-antimouse IgBiotin (BioCan Scientific, Mississauga, Ontario, Canada), Streptavidin-DUOCHROME (Becton
Dickinson), or streptavidin-TANDEM (Southern Biotech, Birmingham, AL): B4(CD19) and PCA-1 from Coulter, BA-1(CD24)4s,*
from Hybritech (San Diego, CA), 50H.10(CD9)47from Dr B.M.
Longenecker, G1.19 and 3AC5 (CD45RA)@from Dr J.A. Ledbetter or FMC44PE (CD45RA)",4y from Dr H. a l a , UCHL-1
(CD45RO)".3a from Dr P. Beverley, and IgGl and IgG2a isotype
control antibodies.
RESULTS
Three-colorZF. For the study of expression of surface antigens
we used a combined indirect and direct staining proced~re."~~~ Detection of a large subset of CDI9+ cells in the PB of MM
patients. A large proportion (20% to 80%) of circulating,
PBMC (3 x 105/well)were resuspended in 50 pL of unconjugated
MoAbs diluted appropriately in PBS plus 1% FCS, 0.2% NaAz.
phenotypically abnormal CD19+ CD20+ CD21- B cells
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
713
CIRCULATING CALLA+ CELLS IN MULTIPLE MYELOMA
were identified in MM. These cells coexpressed CD24,
CALLA (CDlO), and PCA-1 (Table 1). The expression of
CD19, CD20, and CD24, and the lack of CD4, CD8 (Table
1) or LeuM3 (CD14, data not shown), defines the cells as
B-lineage cells. Normal B cells include only 13% CALLA'
cells (Table l), whereas the CD19' subset in MM included
80% to 95% CALLA' cells for both newly diagnosed and
treated patients. For most untreated MM, the intensity of
CD19 expression was within the same range as found on
normal B cells. In contrast, the abnormal B cells from
treated MM had an intensity of CD19 that was fivefold to
10-fold lower than for normal B cells. A very high proportion of CALLA'CD19' cells was most consistently seen
among treated patients. More than 80% of CD19' cells in
MM also expressed PCA-1, a plasma cell marker, indicating
that the vast majority of these cells coexpress CALLA and
PCA-1. Coexpression of CALLA, PCA-1, and CD20 does
not correspond to a recognized stage in normal postnatal
B-cell differentiationwhere expression of CD20 and CALLA
has been shown to be mutually exclusive,52although fetal B
cells coexpress CDlO and CD20.2'
Patients with MGUS also had a relatively large proportion of CD19' B-lineage cells (26%) that included 59%
CALLA+ and 52% PCA-1' cells. Like untreated MM but
different from treated MM, the expression of CD19 on B
cells from MGUS was of an intensity comparable with that
of normal B cells. There is as yet no evidence to determine
whether the B cells in MGUS that lack CALLA and PCA-1
are abnormal. There appears to be a progressive increase in
the number of abnormal B cells over time of disease, as
approximated by the sequence of MGUS (7% to 39%),
untreated MM (14% to 70%), and treated MM (20% to
SO%), with decreasing CD19 intensity and increasing proportion of CALLNPCA-1.
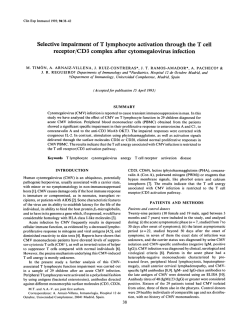
Abnormal B cells are lost with monocyte-depletionmethods.
The studies presented here avoided monocyte-depletion
methods, because this particular cell subset adheres to
plastic surfaces (not shown).53Figure 1 shows the presence
Ficoll Hypaque
I
I
I
Carbonyl Irontficoll HypaqL
I
C D I9
CD19
I
I
I
L
0
n
l
l
5%
75 %
I
I
I
I
I
CALLA
CALLP
I
/I
I
I
35 Yo
I%
I
I
io1
ioz
I
103
Fluorescence Intensity
Fig 1. Carbonyl iron depletion removes abnormal CALLA' B cells.
A complete loss of the CD1Sd1"B-cell subset after carbonyl iron
treatment of PBMC from a treated myeloma patient. Only the small
subset of phenotypically normal, CALLA- CD19b"gMB cells remains.
(-) CD19 or CALLA positivity on PBMC; (----)the appropriate isotype
background. The vertical dotted line indicates the gates applied to
producethe percentages of positive cells. Fluorescence intensity is on
a logarithmic scale. CD19 was detected using BCFITC, and CALLA
using J5-FITC in single IF.
of a CD19' CALLA' B-cell population that is removed by
carbonyl iron depletion. In contrast, the CALLA- B-cell
subset remains after this depletion procedure.
PBMC from myeloma include cells with a clonally rearranged ZgJHsegment. We performed Southern blot analysis
on genomic DNA from myeloma PBMC. As controls, DNA
from normal PBMC or granulocytes was analyzed in parallel. On probing Southern blots with a J, cDNA probe,
PBMC DNA from 6 of 15 myeloma patients showed clonal
Ig gene rearrangement, consistent with the observation
that, for unknown reasons, rearrangements are detectable
Table 1. Expression of B- and T-cell Markers on CD19' Cells
Percentage of CD19' Cells Expressing the Markers Below:
% CD19' Cells
Normal donors
MGUS patients
MM, untreated
MM, treated
in PB*
CD20
CD21
CD24
CALLA
PCA-1
CD4
CD8"
11 f 1.3
(12)
26 ? 2 . 5 W
(13)
39 t 4 . l t
(21)
46 t 3 . l t
(21)
88 f 5.3
26 f 3.3
(7)
5.4 f 1.4t
(5)
10 f 2.8t
(11)
7.1 f 1.7t
(16)
97 f 1.1
(8)
93 f 3.5
(3)
76 2 7.3
(9)
68 f 9.4
(10)
13 f 2.3
(4)
59 f 6.0t§
(10)
74 f 6.6tll
(14)
95 f 1.5t
(11)
19 f 2.2
(4)
52 f 7.8t§
(13)
72 f 6.6t
(17)
83 f 2 . l t
(19)
2
(1)
2.2 f 0.8
(13)
1.4 f 0.6
(14)
1.6 f 0.4
(10)
1
(1)
4.2 f 1.1
(13)
3.3 t 1.0
(13)
3.4 f 0.7
(10)
(7)
79 f 4.6
(12)
82 r 3.6
(16)
88f 2.3
(20)
Three-color IF analysis on freshly isolated PBMC. Percentage of CD19+ cells was established, then gates were set on CD19' cells and the
expression of the other markers was evaluated (see Material and Methods). Results are presented as mean f SE. The number of individuals tested is
given in brackets. "MM, treated" refers to blood samples analyzed after 4 weeks or more after chemotherapy.
*The range for % CD19' cells in PB was 6% to 15% of PBMC for normal donors; 7% to 39% for MGUS patients; 14% to 70% for untreated MM
patients; and 20% to 80% for treated MM patients.
tP < ,002 compared with normal donors.
SP = ,001 compared with MM, untreated.
§P < ,001 compared with MM, treated.
IF' = ,008compared with MM, treated.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
JENSEN ET AL
714
in only about one-third of myeloma BM samples (Berenson,
unpublished). None of these six patients had detectable
plasma cells in PB at the time when the Southern blot was
performed, but they had abnormally high percentages of
CD19+ B-lineage cells in PBMC, and represented all stages
of disease (Table 2). Figure 2 shows clonal rearrangement
of J, gene segment within myeloma PBMC, digested with
two different restriction enzymes, demonstrating clonality
within the PB B-cell population. The substantial reduction
of the germline band confirms that a majority of the PBMC
from this patient are indeed monoclonal B-lineage cells.
Insufficient BM was available for Southern analysis.
The abnormal B-cell subset consists of pre-plasma cells, as
demonstratedby an observed ship in CD45 isoform expression,
concurrent with acquisition of PCA-I. Selective expression
of CD45 isoforms provide a means of defining the differentiation stage of B-cell sub~ets.9**'~
As B and T cells differentiate after activation, they lose the CD45RA isoform and
acquire CD45RO. To examine the differentiation stage of
the CD19' subset in MM PBMC, we performed a series of
three-color IF analyses with the PCA-1 antibody, which
defines plasma cells, and antibodies to CD45 isoforms
CD45RA and CD45RO. The results demonstrate that the
CD19' B-cell subset consists of pre-plasma cells, based on
its expression of both PCA-1 and the low molecular weight
isoform, CD45R0, which are expressed only on very late
stage B cells. Figure 3 shows the pattern of CD45 isoform
expression (CD45RA, CD45RO) on CD19+ cells from an
MM patient, and the expression of the high molecular
weight form, CD45RA, versus the plasma cell marker,
PCA-1. Very few cells express only the CD45RA isoform,
and the majority of the cells either express exclusively
CD45R0, or coexpress low densities of CD45RA and high
densities of CD45RO. This pattern is consistent with the
view that these cells represent a series of differentiation
stages from late B lymphocytes to pre-plasma cells. Thus,
the gradual loss of surface CD45RA can be used in staging
Patient
No.
lsotype of
Paraprotein
1
2
IgA
IgAK
IgAK
IgG
IgGA
A light chain
3
4
5
6
+
+
+
+
+
+
Atypical
IA
II A
II A
111 A
111 B
36
47
34
40
40
28
G M
GI
G-.
3
Fig 2. Ig rearrangements in PBMC from a myeloma patient.
Myeloma PBMC DNA ("M") and normal granulocyte DNA ("G") was
digested with either BamHl or Hindlll restriction enzymes, and
analyzed by Southern blotting using a J. probe, as described in
Materials and Methods. We demonstrated clonal rearrangements
with both restriction enzymes and also with EcoRI-digested DNA (not
shown). Germline bands are marked with (G-) and the rearranged
bands with (D).The size of the germline band is 17 kb for BamHI, and
10 kb for Hind 111. Minigels were run during and after digestion with
restriction enzymes: size-fractionation showed a homogeneoussmear
confirming complete digestion of the DNA.
CD19* CELLS
Table 2. Monoclonality Within CDl9+ PB B Cells of Myeloma
Patients
Yo
Clonal
Stage
CD19+
Rearrangement
at
Cells in
in PBL
Diagnosis
PBL
Hind III
BamHI
G M
Plasma Cells
in PBL
(morphology)
None
None
None
None
None
None
The presence of monoclonal B-lineage cells in the PB of six patients
was confirmed by IF analysis. No plasma cells were detectable among
PBMC or in blood smears, as defined by morphologic criteria. The table
presents data from the six of 15 patients, from whom we were able to
detect clonal rearrangements by Southern blot analysis of DNA digested with EcoRl and BamHl (patients 1 through 5) or BamHIIHindlll
(patient 6). Patient 6 is also represented in Fig. 2. These same
treatments readily detected monoclonal rearrangements in B-cell chronic
lymphoid leukemia and lymphoma. Experiments always included DNA
from PBMC of normal donors, identically treated and run on the same
gel as patient DNA to confirm the germline pattern.
io1
102
CD45 RO
103
IO'
102
103
PCA-I
Fig 3. Expression of CD45RA. CD45R0, and PCA-1 isoforms on
CD19' cells from a myeloma patient. PBMC from an untreated M M
were gated t o include only CD19' cells, and the expression of CD45
isoforms and PCA-1was evaluated. Quadrant markers were set based
on identically gated isotype controls. Fluorescenceis on a logarithmic
scale. Three-color IF staining was with BCFITC, 3AC5-PE, and UCHL-1
or PCA-l/duochrome (indirect). This pattern was representative of
the majority of myeloma patients so analyzed. This particular patient
was diagnosed as having smoldering M M after being classified as
MGUS for 5 years.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
CIRCULATING CALLA+ CELLS IN MULTIPLE MYELOMA
715
the differentiation of these late B cells. By comparing the
loss of the CD45RA with the acquisition of the two markers
CD45RO and PCA-1, a very similar pattern is observed (Fig
3). As the late stage B cells differentiate further towards a
pre-plasma cell stage, they acquire both CD45RO and
PCA-1.
The two B-cell subsets found in treated MM have different
pattems of CD45 isoform expression. Two subpopulations
of B cells, CD19bngh'
and CD19d",were detectable in treated
MM patients. The CD19b"@"
B cells in treated MM (1% to
5% of PBMC), unlike the CD19d'"set (20% to 80% of
PBMC), do not usually express either CALLA or PCA-1
(not shown), and are not depleted by carbonyl iron (Fig 1).
Analysis of CD45 isoform expression further distinguishes
these two sets of B cells (Fig 4). Ninety percent of the
CD19br'at
subpopulation have strong expression of CD45RA,
and few cells expressing only CD45RO (7%). The CD1gd'"'
subpopulation exhibits the pattern expected of late B
cells/pre-plasma cells, which are losing CD45RA and acquiring CD45RO. Thus, the CD19b"gh'
cells are more similar to
normal B cells than are the CD19d" B cells, suggesting that
they represent an earlier differentiation stage.
Evaluation of the CD45 isofom expression on diferent
groups of donors. The overall pattern of CD45 isoforms on
PB B cells in MM patients and normal donors is shown in
Fig 5. In normal donors, the majority of B cells (88% 5 2%)
express the high molecular weight isoform CD45RA. A
small subset (12% 2 2%) of normal PB B cells are in the
late stages of differentiation towards pre-plasma cells and
express either CD45RA and CD45R0, or CD45RO only. It
should be remembered that only 6% to 15% of normal
PBMC are B cells. In contrast, the pattern of CD45 isoform
expression in the large set of CD19' B cells in MM was
almost completely opposite to that of normal B cells. A
small amount of myeloma B cells (8% 2 1%)expressed
only the high molecular weight isoform CD45RA. Based on
a comparison of CD45 isoform expression, it seems likely
1
UORM4L 30NORS
MGLS
io1
io*
io1
UM.TREbTED
that the less mature CD45RA'RO- subset of the CD19b"Bh'
abnormal B cells in MGUS and untreated MM corresponds
B cells in treated MM (Fig 4). A variable
to the CD19bngh'
proportion were transitional cells, coexpressing CD45RA
and CD45RO. Between 50% and 90% of the CD19' cells
had exclusive expression of CD45RO. In all MM patients
the CD45RO' and CD45RA'RO' transitional phenotype
predominated. The patterns of CD45 isoform expression in
MGUS were nearly the same as those in MM, supporting
the suggestion that these are highly abnormal B cells,
although present in lower numbers (Table 1). Approximately 10% to 14% of B cells in MM or MGUS had a normal
CD45 phenotype (mean & SE of percent CD45RA'RO-:
MM [treated/off] = 6 2 1, MM [untreated] = 12 2 3,
MGUS = 10 2 3, and normals = 88 & 2). We have not yet
been able to identify any clear correlation between the
phenotypic analysis of the abnormal B cells and stage of
disease.
NORMAL
CDISb"gh' cells
103
.'
Fig 5. The expression of CD45 isoforms on CD19+ PBMC in
different groups of donors: myeloma patients, treated and untreated,
MGUS patients, and normal donors. EBch bar represents the CD45
isoform distribution on CD19' cells. The height of one bar corresponds to 100% of CD19' cells, and the composition of CD45 isoforms
within a given CD19+ population demonstrated by the three different
CD45RA only; (B) CD45WCD45RO; (MICD45RO only.
shades. (0)
Differences in the CD45RA'RO- expression are statistically different
between M M or MGUS patients and normal control donors (P < .001).
M U L T I P L E MYELOMA
CDISdtm cells
MU.UNTRREATED
io2
CD19'
103
io1
calls
io2
103
C D 4 5 RO
Fig 4. CD45RA and CD45RO isoforms on CD19"" and CDISb"' B cells from a myeloma patient (MM) and a normal donor. Total PBMC from a
representative treated myeloma patient were gated for CD1Sdh cells and CD1Sb"' cells, respectively, and the pattern of CD45 isoform expression
was evaluated. The first dot plot shows the expression of CD45RA versus CD45RO on the CDlSd'" (CDZOd" CALLA+)subset, and the second dot
plot shows CD45 isoforms on the smaller subset of CD1gb"' (CD20"'ght CALLA ) subset of B cells. PBMC from the normal donor were gatgd on
total CD19' cells, and the third dot plot shows the distribution of CD45 isoforms on normal CD19' PBMC B cells. Corresponding isotype controls
were identically gated to determine nonspecific staining for the appropriate subset of PBMC. Fluorescence intensity is on a logarithmic scale.
Three-color IF staining was as described for Fig 3.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
JENSEN ET AL
716
neity among the aggregate CD19' population of each
individual
patient. Figure 6 presents a diagrammatic repreIn characterizing peripheral blood lymphocytes present
sentation
of
the B-cell differentiation pathway, as defined
in myeloma patients, we detected an abnormally large
by selective expression of CD45 isoforms.
population of B-lineage cells (20% to 80% of PBMC).
Because phenotypically abnormal B cells in MGUS and
These B cells comprise a heterogeneous population in
untreated
MM express a density of CD19 comparable with
terms of phenotype and stage of differentiation, with a
of
normal
B cells, we have not been able to distinguish
that
phenotype corresponding to late B cells or early pre-plasma
subpopulations based on CD19. However, in MM patients
cells. They are monoclonal B cells as shown by Southern
on intermittent chemotherapy, we were usually able to
analysis of J, gene rearrangements. These observations are
detect
a large CD19d'" and a small CD19'"@" subset. The
consistent with previously published works from a number
CD19h"ghr
subset, contributing only a few percent of total
of investigators who have reported circulating B-lineage
PBMC, was also CD20'"ah*, and lacked both CALLA and
cells, in some cases shown to have clonal Ig gene rearrangePCA-1. The CD45 isoform pattern on this subset was
ments, in PB of MM patients.*14The results confirm the
similar to the pattern on normal PB B cells, suggesting that
view that the malignant B-cell compartment in myeloma
this minor CD19b"8hrsubset represents an earlier stage of
extends to the PB. Similar results have been found in
differentiation than the CD19d" set or the major CD19b"ghh'
patients with Waldenstrom's macrogl~bulinemia.'~~~~
abnormal B-cell population found in untreated MM and
The maturational stage of this subset of monoclonal B
MGUS. The trend towards fivefold to 10-fold reduced
cells in MM has been disputed. Some investigators have
expression of CD19 on B cells from treated patients
described the circulating, tumor-related B cells as activated
supports the view that these B cells are more terminally
B cells or early plasma cells. Other interpretations define
differentiated than the corresponding B-cell populations
this B-cell subset as immature pre-B cells, based on their
seen in untreated MM and MGUS.
expression of CALLA (CD10). Circulating CALLA' cells
in myeloma patients have previously been r e p ~ r t e d , * " ~ " ~ ' ~Among
~ ~ ~ the aggregate abnormal B-cell population in all
MM
and MGUS, the shift in CD45 isoforms towards
but have been observed only in a small proportion of
expression of CD45RO and loss of CD45RA is consistent
patients examined. We detected CALLA expression on the
with the existence of continuously ongoing differentiation
circulating, tumor-reIated B-lineage cell subset in all paof the abnormal B-lineage cells in vivo. We speculate that a
tients analyzed. The inability of some investigators to detect
shift
in CD45 isoform expression towards the more mature,
a circulating, CALLA' monoclonal B-cell population may
low molecular weight isoform CD45RO may indicate inbe due to the use of plastic adherence or carbonyl ironduced maturation of the (pre-)malignant cells. Thus,
depletion procedures. The work reported here shows the
CD45RO expression might define less aggressive disease
abnormal B cells are lost when PBMC are purified using
and correlate with a stable or plateau phase of the disease.
extensive depletion methods for adherent cell subsets. The
In contrast, expression of CD45RA signifies less differentimajority of CD19' B cells in MM PBMC also expressed
ated B cells, and may indicate relatively greater generative
PCA-1, a plasma cell marker. The coexpression of CALLA
potential. If these speculations are correct, analyses of
and plasma cell markers defines an unusual B-cell populaCD45 isoform expression may have prognostic value. We
tion. However, CALLA has recently been found on activated B eeIIs,24 and does not seem to be confined to early
stages of B-cell differentiation. The expression of the
21
.B cell
Transitional
CALLA glycoprotein, a neutral
may be
octivation phenotype
fundamental to the survival ability of these B cells, perhaps
.I
I
by modulating their response to, or production of interleukin-1 (IL-l).56
The analysis of CD45 isoform expression on the abnormal B-cell subset has proved to be a valuable tool in
defining their stage of differentiation. The expression of
CD45RO indicates that the abnormal B cells in MM cannot
be pre-B cells. The earliest stages of pre-B cells express very
low densities of total CD45 and of CD45RA, which gradually increase during maturation of pre-B cells?'~3y~Jo~61
CD45RA increases, although transiently, after B-cell activation:* and appears to be involved in the early proliferative
stages of PBMC and tonsil B c e l l ~ . 6Concomitant
~*~~
with
acquisition of PCA-1, B cells lose CD45RA and acquire
CD45R0.'8 CD45RA, CD45R0, and CD45 common deterFig 6. The changing pattern of CD45 isoform expression during
minants are lost as the cells mature to end-stage plasma
B-cell development: a working hypothesis. Parts of the model procells (this st~dy).'"~"~'By these criteria, the abnormal
posed here include extrapolation from our data on myeloma patients
CD45RO' CD19' cells in myeloma PBMC are in the late Bto approach events in healthy individuals after antigenic challenge.
or early pre-plasma-cell stage, with considerable heteroge(a)
Coexpressionof both CD45RA and CD45RO.
DISCUSSION
c
iT
M,
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
717
CIRCULATING CALLA+ CELLS IN MULTIPLE MYELOMA
are currently performing long-term studies on a selected
group of MM patients to approach these questions.
We have demonstrated this large, abnormal, circulating
late B/pre-plasma-cell subset in all patients tested so far,
the material comprising newly diagnosed patients as well as
patients with stable or active disease, even though the PBL
counts in MM patients are lower than normal. The presence of large numbers of the abnormal monoclonal B cells
in the blood of patients on intermittent chemotherapy
indicates that this B-cell subset is resistant to treatment.
Significantly, this abnormal B-cell subset is also found in
patients with MGUS, albeit at considerably lower proportion and with a smaller proportion of CALLA- and PCA-1positive B cells. The abnormal B cells in MGUS, like those
in MM, are predominantly CD45RO'. Their existence in
MGUS suggests that the abnormal B cells pre-exist active
disease and may provide a target for malignant transformation. Omede et a164have recently described a nonadherent
PCA-l+ population of peripheral lymphocytes, not found in
MGUS, whose presence correlates with shorter survival
times. Based on the phenotypic properties of this cell type,
it seems probable that it represents a nonadherent subset of
the abnormal B-cell population reported here.
The circulating late stage B cells may be in transit,
homing to the BM. This hypothesis is supported by the
expression of a large number of adhesion and homing
molecules on the surface of this cell subset (Jensen and
Pilarski, in preparation). The neoplastic BM plasma cells in
myeloma have only minimal self-renewal and proliferative
activity in vivo.65 The circulating, tumor-related B-cell
population appears to have at least some of the properties
that might be expected of cells giving rise to the malignant
end-stage plasma cells, raising questions as to whether the
circulating B-cell subset itself is truly malignant, or whether
it gives rise to a small subset of cells with invasive and
metastatic abilities. These circulating B cells may comprise
a drug-resistant stem cell compartment giving rise to tumor
relapse, which, although monoclonal and perhaps able to
give rise to malignant progeny, are not themselves necessarily malignant. In addition to the BM plasma cells, the
tumor-related clone in MM appears to consist of both an
undefined stem cell compartment and circulating B-lineage
cells that are actively and continuously differentiating
towards the plasma cell stage. Experiments are in progress
to determine whether or not these continuously differentiating, monoclonal late stage B cells possess malignant
characteristics of growth and invasion.
ACKNOWLEDGMENT
We are grateful to Eva Pruski and Rucy Vergidis for dedicated
and skilled technical assistance. The Canadian Red Cross Blood
Transfusion Service generously provided blood samples from
normal donors. Drs Peter Beverley, Jeffrey A. Ledbetter, Heddy
Zola, and B. Michael Longenecker kindly provided us with the
MoAbs used in this study. We are thankful to Marian Laderoute
for critical review of this manuscript.
REFERENCES
1. Durie BGM, Salmon SS: Staging, kinetics, and flow cytometry
of multiple myeloma, in Wiernik P, Canellos G, Kyle R, Schiffer C
(eds): Neoplastic Diseases of the Blood, vol 2. New York, NY,
Churchill Livingstone, 1985, p 513
2. Fritz E, Ludwig H, Kundi M: Prognostic relevance of cellular
morphology in multiple myeloma. Blood 63:1072,1984
3. Broder S, Humphrey R, Durm M, Blackman M, Meade B,
Goldman C, Strober W, Waldmann T: Impaired synthesis of
polyclonal (non-paraprotein) immunoglobulins by circulating lymphocytes from patients with multiple myeloma. Mass Med SOC
2932387,1975
4. Pruzanski W, Gidon M, Roy A Supression of polyclonal
immunoglobulins in multiple myeloma: Relationship to the staging
and other manifestations at diagnosis. Clin Immunol Immunopathol 17:280,1980
5. Pilarski LM, Mant MJ, Ruether BA, Belch A Severe deficiency of B lymphocytes in peripheral blood from multiple myeloma patients. J Clin Invest 74:1301, 1984
6. Pilarski LM, Piotrowska-Krezolek M, Gibney DJ, Winger L,
Winger C, Mant MJ, Ruether B A Specificityrepertoire of lymphocytes from multiple myeloma patients. I. High frequency of B cells
specific for idiotypic and F(ab')2 region determinants on immunoglobulin. J Clin Immunol5:275, 1985
7. Pilarski LM, Mant MJ, Ruether B A Review: Analysis of
immunodeficiency in multiple myeloma: Observations and hypothesis. J Clin Lab Anal 1:214, 1987
8. Boccadoro M, Omede P, Massaia M, Dianzani U, Pioppo P,
Battaglio S, Meregalli M, Pilieri A Human myeloma: Several
subsets of circulating lymphocytes express plasma cell-associated
antigens. Eur J Haematol40:299,1988
9. Berenson J, Wong R, Kim K, Brown N, Lichtenstein A
Evidence for peripheral blood B lymphocyte but not T lymphocyte
involvement in multiple myeloma. Blood 70:1550,1987
10. Grogan TM, Durie BGM, Lomen C, Spier C, Wirt DP,
Nagle R, Wilson GS, Richter L, Vela E, Maxey V, McDaniel K,
Rangel C: Delineation of a novel pre-B cell component in plasma
cell myeloma: Immunochemical, immunophenotypic, genotypic,
cytologic, cell culture, and kinetic features. Blood 70:932,1987
11. King MA, Nelson DS: Tumor cell heterogeneity in multiple
myeloma: Antigenic, morphologic, and functional studies of cells
from blood and bone marrow. Blood 73:1925,1989
12. Ruiz-Arguelles GJ, Katzmann JA, Greipp PR, Gonchoroff
NJ, Garton JP, Kyle RA: Multiple myeloma; circulating lymphocytes that express plasma cell antigens. Blood 64:352, 1984
13. Van Riet I, Heirman C, Lacor P, Waele MD, Thielemans K,
Van Camp B: Detection of monoclonal B lymphocytes in bone
marrow and peripheral blood of multiple myeloma patients by
immunoglobulin gene rearrangement studies. Br J Haematol
73:289, 1989
14. Chiu EKW, Ganeshaguru K, Hoffbrand AV, Metha AB:
Circulating monoclonal B lymphocytes in multiple myeloma. Br J
Haematol72:28,1989
15. LeBien TW, McCormack RT: The common acute lymphoblastic leukemia antigen (CD10)-Emancipation from a functional
enigma. Blood 73:625,1989
16. Epstein J, Barlogie B, Katzmann J, Alexanian R: Phenotypic
heterogeneity in aneuploid multiple myeloma indicates pre-B cell
involvement. Blood 71:861, 1988
17. Caligaris-Cappio F, Bergui L, Tesio L, Pizzolo G, Malavasi
F, Chilosi M, Campana D, Van Camp B, Janossy G: Identification
of malignant plasma cell precursors in the bone marrow of multiple
myeloma. J Clin Invest 76:1243,1985
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
718
18. Duperray C, Klein B, Durie BGM, Zhang X, Jourdan M,
Poncelet P, Favier F, Vincent C, Brochier J, Lenoir G, Bataille R:
Phenotypic analysis of human myeloma cell lines. Blood 73:566,
1989
19. Wearne AJ, Joshua DE, Brown RD, Kronenberg H: Multiple myeloma: The relationship between CALLA (CD10) positive
lymphocytes in the peripheral blood and light chain isotype
suppression. Br J Haematol67:39,1987
20. Letarte M, Vera S, Tran R, Addis JL, Onizuka RJ, Quackenbush ET, Jongeneel CV, McInnes RR: Common acute lymphocytic
leukemia antigen is identical to neutral endopeptidase. J Exp Med
168:1247,1988
21. LeBien TW,Wormann B, Villablanca JG, Law C-L, Steinberg LM, Shah VO, Loken M R Multiparameter flow cytometric
analysis of human fetal bone marrow B cells. Leukemia 4:354,1990
22. Hokland P, Nadler LM, Griffin JD, Schlossman SF,Ritz J:
Purification of common acute lymphoblastic leukemia antigen
positive cells from normal human bone marrow. Blood 64:662,1984
23. Greaves MF, Hariri G, Newman RA, Sutherland DR, Ritter
MA, Ritz J: Selective expression of the common acute lymphoblastic leukemia (gp100) antigen on immature lymphoid cells and their
malignant counterparts. Blood 61:628,1983
24. Kiyokawa N, Kokai Y, Ishimoto K, Fujita H, Fujimoto J,
Hata J: Characterization of the common acute lymphoblastic
leukemia antigen (CDlO) as an activation molecule on mature
human B cells. Clin Exp Immunol79:322, 1990
25. Thomas M L The leukocyte common antigen family. Annu
Rev Immunol7:339,1989
26. Trowbridge IS: Interspecies spleen-myeloma hybrid producing monoclonal antibodies against mouse lymphocyte surface
glycoprotein, T200. J Exp Med 148:313,1978
27. Woollett GR, Barclay AN, Puklavec M, Williams AF:
Molecular and antigenic heterogeneity of the rat leukocytecommon antigen from thymocytes and T and B lymphocytes. Eur J
Immunol15:168,1985
28. Dalchau R, Fabre J: Identification with a monoclonal
antibody of a predominantly B lymphocyte-specific determinant of
the human leukocyte common antigen. Evidence for structural and
possible functional diversity of the human leukocyte common
molecule. J Exp Med 153:753,1981
29. Smith SH, Brown MH, Rowe D, Callard RE, Beverly PC:
Functional subsets of human helper-inducer cells defined by a new
monoclonal antibody, UCHL1. Immunology 5863,1986
30. Terry LA, Brown MH, Beverley PCL The monoclonal
antibody, UCHL1, recognizes a 180,000 MW component of the
human leukocyte-common antigen, CD45. Immunology 64:331,
1988
31. Pilarski LM, Gillitzer R, Zola H, Shortman K, Scollay R:
Selective expression of CD45 (T200) antigens during human
thymocyte differentiation.Eur J Immunol 19:589,1988
32. Pilarski LM, Deans JP: Selective expression of CD45 isoforms and maturation antigens during human thymocyte differentiation: Observations and hypothesis. Immunol Lett 21:187,1988
33. Beverley PC: Human T cell subsets. Immunol Lett 14:263,
1987
34. Serra HM, Ledbetter JA, Krowka JF, Pilarski LM: Loss of
CD45R (Lp220) represents a post-thymic T cell differentiation
event. J Immunoll401435,1988
35. Sanders ME, Makoba MW, Sharrow SO, Stephany D,
Springer TA, Young HA, Shaw S: Human memory T lymphocytes
express increased levels of three cell adhesion molecules (LFA-3,
CD2, and LFA-1) and three other molecules (UCHL1, CDw29,
and Pgp-1) and have enhanced IFN-gamma production. J Immunol
140:1401,1988
36. Akbar AN, Terry L, Timms A, Beverley PCL, Janossy G:
JENSEN ET AL
Unidirectional phenotypic changes within the T200 complex during activation of T cells. J Immunol 140:2171, 1988
37. Deans JP, Boyd AW, Pilarski LM: Transitions from high to
low molecular weight isoforms of CD45 involve rapid activation of
alternate mRNA splicing and slow turnover of surface CD45R. J
Immunol143:1233,1989
38. Jensen GS, Poppema S, Mant MJ, Pilarski LM: Transition in
CD45 isoform expression during differentiation of normal and
abnormal B cells. Int Immunol1:229,1989
39. Tedder TF, Clement LT, Cooper MD: Human lymphocyte
differentiation antigens HB-10 and HB-11. I. Ontogeny of antigen
expression. J Immunol134:2983,1985
40. Shah VO, Civin CI, Loken MR: Flow cytometric analysis of
human bone marrow IV. Differential expression of T-200 common
leukocyte antigen during normal hemopoiesis. J Immunol 140:
1861,1988
41. McMichael M E : Leukocyte typing 111. White cell differentiation antigens. Oxford, UK, Oxford University, 1987
42. Kurabayashi H, Kubota K, Murakami H, Tamura J, Sawamura M, Nogiwa E, Shinonome S, Miyawaki S, Sato S, Omine M,
Naruse T, Shirakura T, Tsuchiya J: Ultrastructure of myeloma cells
in patients with common acute lymphoblastic leukemia antigen
(CALLA)-positive myeloma. Cancer Res 48:6234, 1988
43. Kyle RA: ‘Benign’ monoclonal gammopathy. A misnomer?
JAMA 251:1849,1984
44. Kyle RA, Greipp PR: Monoclonal gammopathies of undetermined significance, in Wiernik PH, Canellos GP, Kyle RA, Schiffer
CA (eds): Neoplastic Diseases of the Blood, vol2. New York, NY,
Churchill Livingstone, 1985, p 653
45. LeBien T, Kersey J, Nakazawa S, Minato K, Minowada J:
Analysis of human leukemidlymphoma cell lines with monoclonal
antibodies BA-1, BA-2 and BA-3. Leuk Res 6:299,1982
46. Pirruccello SJ, LeBien TW: The human B cell-associated
antigen CD24 is a single chain sialoglycoprotein. J Immunol
136:3779,1986
47. Seehafer JG, Longenecker BM, Shaw ARE: Biochemical
characterization of human carcinoma surface antigen associated
with protein kinase activity. Int J Cancer 34:821,1984
48. Ledbetter JA, Clark E A Surface phenotype and function of
human tonsillar germinal center and mantle zone B cell subsets.
Hum Immunol15:30,1986
49. Deans JP, Shaw J, Pearse MJ, Pilarski LM: CD45R as a
primary signal transducer stimulating IL-2 and IL-2R mRNA
synthesis by CD34-8human thymocytes. J Immunol 143:2425, 1989
50. Southern EM: Detection of specific sequences among DNA
fragments separated by gel electrophoresis. J Mol Biol98:503,1975
51. Ravetch JV, Kirsch IR, Leder P: Evolutionary approach to
the question of immunoglobulin heavy chain switching: Evidence
from cloned human and mouse genes. Proc Natl Acad Sci USA
77:6734,1980
52. Loken MR, Shah VO, Dattilio KL, Civin CI: Flow cytometric analysis of human bone marrow. 11. Normal B lymphocyte
development. Blood 70:1316,1987
53. Berenson JR, Lichtenstein AK: Clonal rearrangement of
immunoglobulin genes in peripheral blood of multiple myeloma
patients. Br J Haematol73:425,1989
54. Jensen GS, Andrews EJ, Vergidis R, Ledbetter JA, Mant
MJ, Pilarski LM: Transitions in CD45 isoform expression indicates
continuous differentiation of a monoclonal CD5+ CDllb+ B
lineage in Waldenstrom’s macroglobulinemia. Am J Hematol 1991
(in press)
55. Jongeneel CV, Quackenbush EJ, Ronco P, Verroust P,
Carrel S, Letarte M: Common acute lymphoblastic leukemia
antigen expressed on leukemia and melanoma cell lines has neutral
endopeptidase activity. J Clin Invest 83:713,1989
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
CIRCULATING CALLA+ CELLS IN MULTIPLE MYELOMA
56. Pierat ME, Najdovski T, Applebloom TE, DeschodtLanckman MM: Effect of human endopeptidase 24.11 (“enkephalinase”) on IL-1-induced thymocyte proliferation assay. J
Immuno11403808,1988
57. Kawano M, Tanaka H, Ishikawa H, Nobuyoshi M, Iwato K,
Asaoku H, Tanabe 0, Kuramoto A Interleukin-1 accelerates
autocrine growth of myeloma cells through interleukin-6 in human
myeloma. Blood 73:2145,1989
58. Tanaka Y, Shirakawa F, Oda S, Eto S, Yamashita U:
Expression of IL-1 receptors on human peripheral B cells. J
Immunol142:167,1989
59. Lichtenstein A, Berenson J, Norman D, Chang M, Carlile A
Production of cytokines by bone marrow cells obtained from
patients with multiple myeloma. Blood 74:1266,1989
60. Cozzolino F, Torcia M, Aldinucci D, Rubartelli A, Miliani
A, Shaw AR, Lansdorp PM, Guglielmo RD: Production of interleukin-1 by bone marrow myeloma cells. Blood 74:380,1989
719
61. Masellis-Smith A, Jensen GS, Seehafer JG, Slupsky JR,
Shaw ARE: Anti-CD9 mAb induce homotypic adhesion of pre-B
cell lines by a novel mechanism. J Immunol144:1607,1990
62. Gruber MF, Bjomdahl JM, Nakamura S, Fu SM: Anti-CD45
inhibition of human B cell proliferation depends on the nature of
activation signals and the state of B cell activation. A study with
Anti-IgM and Anti-CDw40 antibodies. J Immunol 142:4144,1989
63. Mittler RS, Greenfield RS, Schacter BZ, Richard NF,
Hoffman M K Antibodies to the common leukocyte antigen (T200)
inhibit an early phase in the activation of resting human B cells. J
Immunol138:3159,1987
64. Omede P, Boccadoro M, Gallone G, Fieri R, Battaglio S,
Redoglia V, Pilieri A Multiple myeloma: Increased circulating
lymphocytes carrying plasma cell-associated antigens as an indicator of poor survival. Blood 76:1375,1990
65. Pilieri A, Tarocco RP: In vivo kinetic studies in human
myeloma. Haematologica 5910,1974
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1991 78: 711-719
Selective expression of CD45 isoforms defines CALLA+ monoclonal
B- lineage cells in peripheral blood from myeloma patients as late
stage B cells
GS Jensen, MJ Mant, AJ Belch, JR Berenson, BA Ruether and LM Pilarski
Updated information and services can be found at:
http://www.bloodjournal.org/content/78/3/711.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.



© Copyright 2026