
in Mesenchymal Tumors - Europe PubMed Central
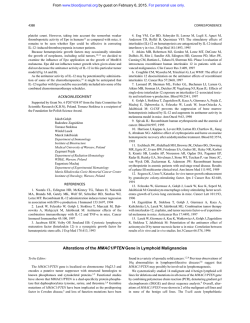
American Journal ofPathology, Vol. 137, No. 5, November 1990 Copyright © American Association of Pathologists Expression of Aminopeptidase N (D1 3) in Mesenchymal Tumors Gunhild Mechtersheimer and Peter Moller From the Institute of Pathology, Heidelberg University, Heidelberg, Federal Republic of Germany For a long time, CD13 molecules have been considered to be restricted to myeloid cells and related neoplasms. Meanwhile, however, expression of CD13 has also been detected in some hepatocellular, gallbladder, renal, and lung carcinomas, and even in somefibrosarcomas and malignant melanomas. In this study, expression of CD13 antigen was immunohistochemically examined in non-neoplastic mesenchymal cells, along with 33 benign and 83 malignant mesenchymal tumors (MET) using CD13 monocolonal antibodies (MAb) My7, U71, WM- 15, and MoU48. In non-neoplastic mesenchymal cells, expression ofCD13 was restricted to perivascularfibrocytes/blasts, tissue histiocytes, osteoclasts, and to the perineurium ofperipheral nerve trunks. Under neoplastic conditions, CD13 was detectable in some tumors of smooth muscle, fibrous, fibrohistiocytic, synovial, osteogenic, and peripheral nerve sheath origin, and even in some tumors of adipose tissue. Tumors of striated muscle origin, ofautonomic ganglia, and of cartilage-forming tissues were CD13-negative throughout. Thus in most but not all tumors studied thepattern ofexpression of CD13 mirrors the situation found in their cells of origin. These findings enrich the data on expression of leukocyte differentiation antigens in extrahematopoietic tissues. Expression of CD13, which meanwhile is known to be identical to aminopeptidase N, an important peptide-cleaving enzyme, in only some MET might reflect a special functional state of these neoplasms. (Am J Pathol 1990, 13 7: 1215-1222) The CD13 antigen, long known as a panmyeloid antigen, is a 150-kd surface glycoprotein1-3 encoded by a gene located on chromosome 15 at bands q25-26.4 Its DNA sequence predicts a 967 amino acid integral membrane protein with a single, 24 amino acid hydrophobic segment near the intracellular amino terminus that is not cleaved but could function both as a signal for membrane insertion and a stable membrane-spanning segment.4 The large extracellular carboxyterminal domain contains a pentapeptide consensus sequence characteristic of members of the zinc-binding metalloprotease superfamily. Recently the CD1 3 molecule has been proved to be identical to aminopeptidase N, an important enzyme of the brushborder membranes of the small intestine, renal proximal tubules, and placenta also found on synaptic membranes of the central nervous system and on the surface of granulocytes and macrophages.5 Originally the CD13 molecule was detected on a proliferative subset of committed human myeloid progenitors as well as on normal marrow granulocytes and monocytes at all stages of differentiation.6 Under neoplastic conditions, CD13 reacts with leukemic blasts of most acute myeloblastic leukemias.267 In contrast, CD1 3 antigen regularly is absent on the surface of normal T and B lymphocytes or on lymphocytic malignancies,267 except for a small group of acute leukemias showing coexpression of CD13 molecules and B-cell markers and having an increased risk of treatment failure.8-10 Outside the hematopoietic system, the CD1 3 molecule has been found in renal proximal tubular cells, in bile duct canaliculi, in fibroblasts, and in osteoclasts.11 In malignancy, CD13 antigen has been observed in hepatocellular, gallbladder, and renal carcinoma cell lines.12'13 Of the CD13 antibody cluster,14 the original monoclonal antibody (MAb) My7, an IgGl antibody,6 together with MAbs U71, WM-15, and MoU48,14 was applied in this study, the objective of which was to investigate the expression of CD13 antigen in a comprehensive series of mesenchymal tumors (MET). Materials and Methods Tissue Representative frozen tissue samples of a comprehensive series of normal tissues containing all kinds of mesenSupported by the Tumorzentrum Heidelberg/Mannheim. Accepted for publication June 29, 1990. Address reprint requests to Dr. med. G. Mechtersheimer, Institute of Pathology, University of Heidelberg, Im Neuenheimer Feld 220, D-6900 Heidelberg, FRG. 1215 1216 Mechterscheimer and MOAler AJP November 1990, Vol 137, No. 5 Controls chymal cells, of 33 benign and 83 malignant well-defined mesenchymal tumors (MET) were collected at our institute during a period of 3.5 years. Diagnosis of each case was established on routine paraffin sections (H&E, PAS, Masson-Goldner and Gomori silver stains) according to standard histopathologic criteria, as described Enzinger and Weiss,15 in conjunction with immunohistochemical analysis using a broad panel of mono- and polyclonal antibodies directed against well-established structural antigens of mesenchymal cells (for review see Enzinger and Weiss15 and Wick and Swanson16). The tissue samples were quick frozen in liquid nitrogen and stored at -70° C. Frozen sections of about 1 cm2 and a thickness of 4 to 6 gm were air dried, acetone fixed at room temperature for 10 minutes, immediately stained, or stored at -20° C for a short period. Negative controls were in each case performed by omitting the primary antibody; no staining was observed, except for scattered granulocytes. This staining was due to endogenous peroxidase, which was not blocked for the benefit of optimal antigenicity. The positive results were confirmed by a control using the isotype-matched MAb HD39, which gave negative results in each case, precluding nonspecific antibody binding. In addition all My7positive and a representative number of My7-negative tumors were examined for expression of CD1 3 by application of CD13 MAbs U71, WM-15, and MoU48. With the exception of the dotlike intracytoplasmic My7 positivity in some tumors of smooth muscle origin, these MAbs confirmed the results obtained by MAb My7. Reagents Evaluation CD1 3 MAb My7 (isotype IgG1) was obtained from Coulter Immunology, Hialeah, FL. MAbs U71, WM-1 5, and MoU48, which also recognize the CD1 3 molecule, were gifts from D. Bourel (Rennes, France), E.J. Favaloro (Westmead, Australia), and R. Whinchester (New York, NY), respectively. CD22 MAb HD39 (isotype IgGl), which was used as an isotype-matched control MAb, was provided by B. Dorken and G. Moldenhauer (Heidelberg, FRG). A biotinylated sheep antibody to mouse Ig (reactive with all mouse isotypes) and a streptavidin-biotinylated peroxidase complex, serving as detection system for the monoclonal primary antibodies, were provided by Amersham, High Wycombe, U.K. 3-Amino-9-ethylcarbazole (AEC) and N'Ndimethylformamide (DMF) were obtained from Sigma Chemical Co., St. Louis, MO. The staining of the tumor cells was evaluated semiquantitatively as follows: +, positive reaction of the entire neoplastic population; +/-, positive and negative tumor cells in various amounts (for details see Results); and -, negative staining of the entire tumor cell population. Dotlike intracytoplasmic staining with MAb My7, which was detectable in a few tumors of smooth muscle origin, is indicated separately in Results and in Table 1. Staining Procedure After rehydration with phosphate-buffered saline solution (PBS; pH 7.4), the frozen sections were incubated for 1 hour with primary MAb at appropriate dilutions (My7 [1: 20], U71 [1:100], WM-15 [1:100], MoU48 [1:100]). The sections were incubated with biotinylated anti-mouse Ig (1:50) and streptavidin-biotinylated peroxidase complex (1:100) for 30 minutes each. All incubation steps were carried out in a humid chamber at room temperature and were followed by double rinsing with PBS. Using AEC as the chromogen (0.4 mg/ml in 0.1 mol/l [molar] acetate buffer, pH 5.0, with 5% DMF and 0.01% H202 for 10 minutes), the peroxidase reaction caused an intense red precipitate. The sections were rinsed in tap water, counterstained with Harris' hematoxylin, and mounted with glycerol gelatin. Results Non-neoplastic Mesenchymal Cells CD1 3 molecule was strongly expressed in perivascular fibrocytes/blasts, tissue histiocytes, osteoclasts, and in the perineurium of peripheral nerve trunks. Smooth muscle cells of the uterus, of blood vessel walls, and of intestinal organs, striated muscle cells of skeletal and cardiac muscle, peripheral nerve fibers, ganglion cells, neuroblasts of adrenal medulla, adipocytes, and chondrocytes were consistently CD13 negative. Tumors of Muscle Tissue Consistent CD13 positivity was observed in one leiomyoma (LM), one leiomyosarcoma (LMS), and one leiomyoblastoma. In two LMs, CD13 was expressed on a major and on a minor tumor cell population, respectively. In three LMSs, CD13 was observed in most tumor cells, and in two LMSs CD13-positive and -negative tumor cells were detectable in about equal amounts. As an exceptional finding, one LM and three LMSs showed a dotlike intra- CD13 in Mesenchymal Tumors 1217 AJP November 1990, Vol. 137, No. 5 Table 1. Expression ofAminopeptidase N (CD13) in Mesenchymal Tumors Number Phenotype + (1)* 1 2 4 11 Leiomyoma 1 5(3)* 10 16 Leiomyosarcoma 8 1 1 Leiomyoblastoma _ 8 8 Rhabdomyosarcoma 1 4 5 SF Fibroadenoma _5 ME _ 2 2 Fibroma 4 4 Aggressive fibromatosis 3 1 4 Fibrosarcoma 1 1 Benign giant cell tumor of tendon sheath 3 1 5 Synovial sarcoma 1 1 Juvenile xanthogranuloma 1 1 Cutaneous fibrous histiocytoma 4 4 2 10 Malignant fibrous histiocytoma 2 2 4 Osteosarcoma 1 1 Chondroma 3 Chondrosarcoma 3 2 1 Neurilemoma 3 _ ~~~~~1 1 Granular cell tumor 6 2 3 11 Malignant schwannoma _2 2 Periph. neuroepithelioma 3 3 Ganglioneuroma _4 4 Ganglioneuroblastoma 3 _3 Neuroblastoma _4 4 Lipoma 7 2 9 Liposarcoma 2 _2 Hemangioma 3 3 Hemangiopericytoma _ 1 1 Angiosarcoma _ ~~~~~~1 1 Lymphangioma _ ~~~~~~1 1 Lymphangiosarcoma Cases showing a dotlike intracytoplasmic staining with MAb My7 +l- are given in parentheses. SF, stromal fibroblasts; ME, myoepithelial cells. n= 118. cytoplasmatic CD1 3 positivity by application of MAb My7 (Figure 1), whereas staining with MAbs U71, WM-1 5, and MoU48 did not reveal any CD13 positivity. One LM and ten LMSs were CD1 3 negative throughout. The eight rhabdomyosarcomas (RMS) studied were completely devoid of any detectable CD13 antigen (Figure 5). Tumors of Fibrous Tissue In four aggressive fibromatoses the entire tumor cell population was strongly CD1 3 positive throughout (Figure 3), and in one fibrosarcoma about one half of the tumor cells exhibited weak CD13 positivity. Three fibrosarcomas and two fibromas were CD13 negative. positive (Figure 7), as were the neoplastic cells in one synovial sarcoma (SS) of monophasic fibrous type. One monophasic fibrous SS exhibited weak staining with CD13 MAb in about one half of the tumor cells, whereas three SSs, also of monophasic fibrous type, were completely CD13 negative (Figure 4). Fibrohistiocytic Tumors One cutaneous fibrous histiocytoma was CD1 3 negative, as was one juvenile xanthogranuloma. The series of malignant fibrous histiocytomas (MFH) studied comprised 8 of storiform pleomorphic, 1 of myxoid, and 1 of giant cell subtype. The lafter showed CD13 positivity in the giant cells and in some of the pleomorphic tumor cells (Figure 8). Furthermore CD1 3 was expressed in the entire tumor cell population in two and, in a minor tumor cell population, in three storiform-pleomorphic MFHs, whereas the remaining three cases as well as the myxoid MFH lacked any detectable CD13 determinants. Tumors of Cartilage and Bone-forming Tissues One chondroma and three chondrosarcomas were CD13 negative throughout. The four osteosarcomas (OS) studied comprised three of osteoblastic and one of fibroblastic subtype. The fibroblastic and one osteoblastic OS expressed CD1 3 on the entire tumor cell population (Figure 9); in two further OS a major and a minor tumor cell population, respectively, were CD13 positive. Osteoclastic giant cells, present in various densities in all cases studied, were CD13 positive. Tumors of Peripheral Nerves Two malignant schwannomas (MS) expressed CD13 on virtually every tumor cell (Figure 2); two MS were composed of CD13-positive and CD13-negative tumor cells in about equal proportions, and one MS as well as one neurilemoma (NL) exhibited CD13 positivity in a minor tumor cell population. However six MSs, two peripheral neuroepitheliomas, and two NLs were completely CD13 negative. Tumors of Autonomic Ganglia Tumors of Synovial Tissue In one benign giant cell tumor of tendon sheath, the total tumor cell population, including the giant cells, was CD13 In three ganglioneuromas, both the ganglion cell and the Schwann cell compartments were CD13 negative. Similarly the ganglion cells in four ganglioneuroblastomas lacked 1218 Mechterscheimer and MOlIer AJP November 1990, VoL 137, No. 5 Figure 1. Spindle cell leiomyosarcoma with moderate cell pleomorphisms. Immunostaining with MAb CD13 t (My7) exhibits a dotlike intracytoplasmic positivity of a major tumor cellpopulation (Immunoperoxidase staining offrozen sections, faint hematoxylin counterstain; same technique for all photographs; X 175). Figure 2. Spindle cell malignant schwannoma with myxoid changes. The tumor cells, surrounded by unstained myxoid material, are consistently CD13 t (My 7) positive (X87,5). Figure 3. Extra-abdominal aggressive fibromatosis. The entire tumor cellpopulation arranged in ill-definedfascicles shows strong immunoreactivity with MAb CD13 t (My7). In addition, perivascular fibrocytes/-blasts are strongly CD13 positive (X 70). Figure 4. Monophasic fibrous synovial sarcoma. The tumor completely lacks any detectable CD13 t (My7) antigen. CD13 positivity ofperivascularfibrocytes/-blasts and of some scattered spindle cells of the adjacent tumor capsule serves as intrinsic positive controlfor the reliability of the immunohistochemical reaction (X 140). Figure 5. Undifferentiated embryonal rhabdomyosarcoma. The small round tumor cells are consistently CD13 t (My7) negative while some scattered tissue macrophages as well as perivascularfibrocytes/-blasts strongly express CD13 antigen (X 175). Figure 6. Neuroblastoma. The undifferentiated, small round neuroblasts lack any detectable CD13 t (My7) antigen. Once again, strongly CD13-positive perivascularfibrocytes/-blasts serve as intrinsic positive controls (X 175). any detectable CD1 3 molecules; the same was true for the small round neuroblasts of these cases as well as for the neuroblastic tumor cell population in three undifferentiated neuroblastomas (Figure 6). Tumors of Adipose Tissue This category comprised four lipomas (one of them an angiolipoma) and nine liposarcomas (LS). All lipomas and CD13 in Mesenchymal Tumors 1219 AJP November 1990, Vol. 13 7, No. 5 seven LSs studied were consistently CD1 3 negative. In one LS a major tumor cell population expressed CD13 molecules; in one other case CD13-positive and CD13negative tumor cells were detectable in about equal proportions. Tumors of Vascular Origin Two cavernous hemangiomas, one benign and two malignant hemangiopericytomas, one angiosarcoma, one lymphangioma, and one lymphangiosarcoma studied were CD13 negative throughout. All in all, CD13 determinants were detectable in some tumors of smooth muscle, fibrous, fibrohistiocytic, synovial, and osteogenic origin as well as in some neoplasms of peripheral nerve sheath origin and of adipose tissue. The tumors of striated muscle and of vascular origin, of cartilage-forming tissues, and the neoplasms of autonomic ganglia studied were characterized by consistent CD1 3 negativity. Discussion Mesenchymal tissues comprise a range of cell types that differ in embryologic derivation, morphology, and function. Presently little is known about the surface antigenic phenotypes of normal or neoplastic mesenchymal cells. Several previous studies, however, have shown that a number of leukocyte surface antigens may be expressed in various normal and/or neoplastic extrahematopoietic mesenchymal cells either constitutively or as the consequence of neoplastic transformation. Thus CD57(HNK-1) antigen is expressed in neurofibromas and in neurofibrosarcomas 17,18 as well as in other spindle cell sarcomas17 and even in Ewing's sarcomas9,20 and in peripheral neuroectodermal tumors.21 CD71 (OKT9) molecules, originally found to bind to immature T cells22 but later shown to recognize the more prevalent human transferrin receptor,23 are broadly distributed in mesenchymal tissues. Flanagan et al24 found CD1 1 c(3.9.) and CD68(EBM1 1) determinants to be expressed in osteoclastlike giant cells in giant cell malignant fibrous histiocytoma; based on the expression of CD4(Leu3), CD1 4(LeuM3), and CD45(T200) antigens, Wood et a125 considered both the mononuclear and the giant cells in benign giant cell tumor of tendon sheath to be of osteoclastic origin. Similarly CD53(HD77), an antibody that has been raised at our laboratory against a 36- to 50-kd pan leukocyte surface antigen,26 reacts with osteoclasts and with osteoclastlike giant cells in malignant fibrous histiocytoma and in benign giant cell tumor of tendon sheath (data not shown). Furthermore Pilkington and Pallesen27 found expression of CD9, CD1 0, and CDW32 antigens .:.1.... l: 8;: :14f :; I A 6 Figure 7. Benign giant cell tumor oftendon sheath. CD13 (My7) antigen shows membrane-bound positivity of both the mononuclear and the multinucleated giant tumor cells (X 175). Figure 8. Giant cell malignant fibrous histiocytoma. The multinucleated giant cells and some of the pleomorphic tumor cells are CD13 (My 7) positive. Furthermore CD13 (My7) MAb reacts with scattered tissue histiocytes (X 175). Figure 9. Osteoblastic osteosarcoma. The tumor cells, some osteoclastlike giant cells included, show membrane-bound staining for CD13 (My7) antigen X224). in some rhabdomyosarcomas, Ewing's sarcomas, and neuroblastomas. CD10 (CALLA), meanwhile known to be identical to neutral endopeptidase,28 has been found in a variety of solid tumors, including gliomas.29 Furthermore we recently demonstrated expression of CD1 0 antigen in a series of MET of diverse histogenesis.0 CD1 3 lately has been identified as aminopeptidase N, an enzyme that in- 1220 Mechterscheimer and MOler AJP November 1990, Vol. 137, No. 5 activates several peptides, including enkephalins.5 Although CD10 and CD1 3 antigens show clear differences in their patterns of expression in hematopoietic cells, both molecules are integral membrane metalloproteases with the characteristic zinc-binding motif in their extracellular carboxyterminal domains27'31 and share the expression in renal proximal tubular cells and in fibroblasts.11'3233 This prompted us to study the expression of CD13 determinants in mesenchymal tumors by application of MAbs My7, U71, WM-15, and MoU48.6"4 We found CD13 molecules to be expressed in some tumors of fibrous, fibrohistiocytic, synovial, osteogenic, and smooth muscle origin, as well as in some tumors of peripheral nerves and of adipose tissue, whereas tumors of striated muscle origin, of autonomic ganglia, and of cartilage-forming tissue were consistently CD1 3 negative. In extrahematopoietic mesenchymal tissues, CD13 molecules have been found in connective tissue elements and in fibroblasts that showed a collagenlike pattern around blood vessels.11 In line with these results, we found CD1 3-positive perivascular and stromal fibroblasts in most of the METs studied. Furthermore CD1 3 antigen was expressed in stromal fibroblasts of five fibroadenomas of the breast. Concerning fibrous tumors, the results were heterogenous. CD13 molecules were expressed consistently in aggressive fibromatoses, whereas fibromas and most of the fibrosarcomas and of the monophasic fibrous synovial sarcomas studied lacked any detectable CD13 antigens. From these data we might speculate that the tumor cells in aggressive fibromatosis exhibit a special functional and/or physiologic state that is different from that found in fibromas and in most of their malignant counterparts. Besides its expression in fibroblasts, CD1 3 antigen also has been described in osteoclasts,1I a feature that we could confirm in multinucleated osteoclastic giant cells in a bone marrow metastasis of bizarre giant cell bronchial carcinoma and in two cases of ossifying myositis (data not shown). In this study, we found CD1 3 positivity in osteoclastlike giant cells in four osteosarcomas and in one malignant fibrous histiocytoma (MFH) of giant cell subtype. Expression of CD13 antigen, however, was not restricted to osteoclastlike giant cells but also was present in pleomorphic and even in spindle tumor cells of all osteosarcomas and of a considerable number of MFHs studied. The histogenesis of MFH is still controversial. Some authors favor a histiocytic origin,3435 while others consider MFH to be of primitive mesenchymal cell origin.-'- Based on the observation of CD13 positivity in various mesenchymal tumors, the expression of this antigen alone cannot be considered a strong argument in favor of a true histiocytic origin of MFH. However it should be noted that our results correspond with those obtained by Strauchen and Dimitriou-Bonae demonstrating positivity for monocyte/macrophage antigens in MFHs, whereas Wood et a137 and Lawson et all did not find expression of any of these antigens in MFHs. Furthermore, in one case of benign giant cell tumor of tendon sheath (GCTTS), both the mononuclear cells and the multinucleated giant cells were CD13 positive. These results correlate with those of Wood et al,25 who found a monocyte/macrophage phenotype of the entire tumor cell population of GCTTS. The authors concluded that GCTTS thus might be a true histiocytic lesion of monocyte/macrophage lineage composed of phenotypically similar mononuclear and giant cells that most closely resemble osteoclasts. Although this might well be the case, the presence of CD13 molecules in GCTTS is but a feable argument on the background of our data. Because normal smooth muscle cells and peripheral nerve fibers are CD13 negative, expression of CD13 in some tumors of smooth muscle origin and of peripheral nerves is remarkable. The significance of CD13 expression in these tumors, however, cannot be explained at present. As an exceptional finding, some tumors of smooth muscle origin showed a dotlike intracytoplasmic CD13 positivity by application of MAb My7, whereas other CD13 MAbs applied gave negative results in these cases. Nonspecific antibody binding could be excluded using an irrelevant, isotype-matched control antibody. Therefore we suggest that My7 detects the CD13 antigen already in its intracytoplasmic form, before it is processed to the cell surface. The CD13 negativity in tumors of striated muscle origin, including small, round, undifferentiated rhabdomyosarcoma in tumors of cartilage-forming tissues and of autonomic ganglia, seems to mirror the situation found in their cells of origin. It should be noted, however, that our in situ findings on CD13 negativity of (ganglio-) neuroblastomas contrast with data presented by Favaloro et al,40 who found strong expression of CD13 in two neuroblastoma cell lines studied. In this context, it would be interesting to study other small, round, blue cell tumors, such as Ewing's sarcomas and even Wilms' tumors, and small cell bronchial carcinomas for expression of CD13 molecules. Although to variable extents, expression of CD13 has been found in a series of METs studied, enriching the data on expression of leukocyte differentiation antigens in extrahematopoietic tissues. Because in acute myeloblastic leukemia expression of CD13 has been found to be associated with decreased survival,41 additional studies increasing the total number of METs examined for CD13 would be of interest in view of possible correlations between CD1 3 expression and biologic and metastatic behavior of METs. References 1. McKolanis JR, Finn OJ, Metzgar RS: Characterization of human myelomonocytic antigens using monoclonal antibodies. CD13 in Mesenchymal Tumors 1221 AJP November 1990, Vol. 13 7, No. 5 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. In Cohan E and Singal DP, eds. Non-HLA Antigens in Health, Aging and Malignancy. New York, Alan R Liss, 1983, pp 145-156 Griffin JD, Linch D, Sabbath K, Lacrom P, Schlossman SF: A monoclonal antibody reactive with normal and leukemic human myeloid progenitor cells. Leuk Res 1984, 8:521-534 Sakai K, Hattori T, Sagawa K, Yokoyama M, Takatsuki K: Biochemical and functional characterization of MCS-2 antigen (CD13) on myeloid leukemic cells and polymorphonuclear leukocytes. Cancer Res 1987, 47:5572-5576 Look AT, Peiper SC, Rebentisch MB, Ashmun RA, Roussel MF, Lemons RS, LeBeau MM, Rubin CM, Sherr CJ: Molecular cloning, expression, and chromosomal localization of the gene encoding a human myeloid membrane antigen (gpl 50). J Clin Invest 1986, 78:914-921 Look AT, Ashmun RA, Shapiro LH, Peiper SC: Human myeloid plasma membrane glycoprotein CD13 (gp150) is identical to aminopeptidase N. J Clin Invest 1989, 83:1299-1307 Griffin JD, Ritz J, Nadler LM, Schlossman SF: Expression of myeloid differentiation antigens on normal and malignant myeloid cells. J Clin Invest 1981, 68:932-941 Griffin JD, Ritz J, Beveridge RP, Lipton JM, Daley JF, Schlossman SF: Expression of MY7 antigen on myeloid precursor cells. Int J Cell Cloning 1983, 1:33-48 Mirro J, Zipf TF, Pui C-H, Kitchingman G, Williams D, Melvin S, Murphy SB, Stass S: Acute mixed lineage leukemia: Clinicopathologic correlations and prognostic significance. Blood 1985, 66:1115-1123 Drexler HG, Sagawa K, Menon M, Minowada J: Reactivity paftern of "myeloid monoclonal antibodies" with emphasis on MCS-2. Leuk Res 1986, 10:17-23 Sobol RE, Mick R, Royston I, Davey FR, Ellison RR, Newman R, Cuttner J, Griffin JD, Colins H, Nelson DA, Bloomfield CD: Clinical importance of myeloid antigen expression in adult acute lymphoblastic leukemia. N EngI J Med 1987, 316: 1111-1117 Hogg N, Horton MA: Myeloid antigens: New and previously defined clusters. In McMichael AJ, ed. Leucocyte Typing ll, Proceedings of the Third International Workshop on Human Leucocyte Differentiation Antigens. Oxford: Oxford University Press, 1987, 567-621 Look AT, Ashmun RA, Shapiro LH, O'Connell PJ, Gerkis V, D'Apice AJ, Sagawa K, Peiper SC: Report on the CD1 3 (aminopeptidase N) cluster workshop. In Knapp W, Dorken B, Gilks WR, Rieber EP, Schmidt RE, Stein H, von dem Borne AEGKr, eds. Leucocyte Typing IV. White Cell Differentiation Antigens. Oxford, Oxford University Press, 1989, pp 784787 Finstad, CL, Cordon-Cardo C, Bander NH, Whitmore WF, Melamed MR, Old LJ: Specificity analysis of mouse monoclonal antibodies defining cell surface antigens of human renal cancer. Proc Natl Acad Sci USA 1985, 82:2955-2959 Gadd S: Cluster report: CD13. In Knapp W, Dbrken B, Gilks WR, Rieber EP, Schmidt RE, Stein H, von dem Borne AEGKr, eds. Leucocyte Typing IV. White Cell Differentiation Antigens. Oxford, Oxford University Press, 1989, pp 782-784 Enzinger W, Weiss SW: Soft Tissue Tumors. St. Louis, CV Mosby, 1988 16. Wick MR, Swanson PE: Immunohistochemistry of Neoplasia. Soft Tissue Tumors. In Colvin RB, Bhan AK, and McCluskey RT, eds. Diagnostic Immunopathology. New York, Raven Press, 1988, pp 365-400 17. Swanson PE, Manivel JC, Wick MR: Immunoreactivity for Leu-7 in neurofibrosarcomas and other spindle cell sarcomas of soft tissue. Am J Pathol 1987, 126:546-560 18. Johnson MD, Glick AD, Davis BW: Immunohistochemical evaluation of Leu-7, myelin basic-protein, S100-protein, glialfibrillary acidic-protein, and LN3 immunoreactivity in nerve sheath tumors and sarcomas. Arch Pathol Lab Med 1988, 112:155-160 19. Kawaguchi K, Koike M: Neuron-specific enolase and Leu-7 immunoreactive small round-cell neoplasms. The relationship to Ewing's sarcoma in bone and soft tissue. Am J Clin Pathol 1986, 86:79-83 20. Pinto A, Grant LH, Hayes FA, Schell MJ, Parham DM: Immunohistochemical expression of neuron-specific enolase and Leu7 in Ewing's sarcoma of bone. Cancer 1989, 64: 1266-1273 21. Llombart-Bosch A, Lacombe MJ, Peydro-Olaya A, PerezBacete M, Contesso G: Malignant peripheral neuroectodermal tumours of bone other than Askin's neoplasms: Characterization of 14 new cases with immunohistochemistry and electron microscopy. Virchows Arch (Pathol Anat) 1988, 412: 421-430 22. Reinherz EL, Kung PC, Goldstein G, Levey RH, Schlossman SF: Discrete stages of human intrathymic differentiation: Analysis of normal thymocytes and leukemic lymphoblasts of T cell lineage. Proc Natl Acad Sci USA 1980, 77:15881592 23. Goding JW, Burns GF: Monoclonal antibody OKT-9 recognizes the receptor for transferrin on human acute lymphocytic leukemia cells. J Immunol 1981, 127:1256-1258 24. Flanagan AM, Chambers TJ: Osteoclasts are present in the giant cell variant of malignant fibrous histiocytoma. J Pathol 1989,159:53-57 25. Wood GS, Beckstead JH, Medeiros W, Kempson RL, Warnke RA: The cells of giant cell tumor of tendon sheath resemble osteoclasts. Am J Surg Pathol 1988, 12:444-452 26. Hadam MR: Cluster report: CD53. In Knapp W, Dorken B, Gilks WR, Rieber EP, Schmidt RE, Stein H, von dem Borne AEGKr, eds. Leucocyte Typing IV. White cell differentiation antigens. Oxford, Oxford University Press, 1989, pp 674678 27. Pilkington GR, Pallesen G: Phenotypic characterization of non-haemopoietic small cell tumors of childhood with monoclonal antibodies to leucocytes, epithelial cells and cytoskeletal proteins. Histopathology 1989, 14:347-357 28. Letarte M, Veera S, Tran R, Addis JB, Onizuka RJ, Quakenbush EJ, Jongeneel CV, Mcinnes RR: Common acute lymphocytic leukemia antigen is identical to neutral endopeptidase. J Exp Med 1988, 168:1247-1253 29. Carrel S, de Tribolet N, Gross N: Expression of HLA-DR and common acute lymphoblastic leukemia antigens on glioma cells. Eur J Immunol 1983, 12:354-357 30. Mechtersheimer G, Moller P: Expression of the common acute lymphoblastic leukemia antigen (CD10) in mesenchymal tumors. Am J Pathol 1989, 134:961-965 1222 Mechterscheimer and Moller AJP November 1990, Vol. 137, No. 5 31. McKerrow JH, Human fibroblast collagenase contains an amino acid sequence homologous to the zinc-binding site of Serratia protease. J Biol Chem 1987, 262:5943 32. Metzgar RS, Borowitz MJ, Jones NH, Dowell BL: Distribution of common acute lymphoblastic leukemia antigen in nonhematopoietic tissues. J Exp Med 1981, 154:1249-1254 33. Braun MB, Martin RJ, Ledbetter JA, Hansen JA: Granulocytes and cultured human fibroblasts express common acute Iymphoblastic leukemia-associated antigens. Blood 1983, 61: 718-725 34. Iwasaki H, Kikuchi M, Takii M, Enjoji M: Benign and malignant fibrous histiocytomas of the soft tissues. Functional characterization of the cultured cells. Cancer 1982, 50:520-530 35. Shirasuna K, Sugiyama M, Myazaki T: Establishment and characterization of neoplastic cells from a malignant fibrous histiocytoma. A possible stem cell line. Cancer 1985, 55: 2521-2532 36. Roholl PJM, Kleyne J, van Unnik JAM: Characterization of tumor cells in malignant fibrous histiocytomas and other softtissue tumors, in comparison with malignant histiocytes. ll. Immunoperoxidase study on cryostat sections. Am J Pathol 1985,121:269-274 37. Wood GS, Beckstead JH, Turner RR, Hendrickson MR, Kempson RL, Warnke RA: Malignant fibrous histiocytoma tumor cells resemble fibroblasts. Am J Surg Pathol 1986, 10:323-335 38. Lawson CW, Fisher C, Gatter KC: An immunohistochemical study of differentiation in malignant fibrous histiocytoma. Histopathology 1987, 11:375-383 39. Strauchen JA, Dimitriu-Bona A: Malignant fibrous histiocytoma. Expression of monocyte/macrophage differentiation antigens detected with monoclonal antibodies. Am J Pathol 1986,124:303-309 40. Favaloro EJ, Bradstock KF, Kabral A, Grimsley P, Zowtyj H, Zola H: Further characterization of human myeloid antigens (gp160,95; gp150; gp67): Investigation of epitopic heterogeneity and non-haematopoietic distribution using panels of monoclonal antibodies belonging to CD-1 lb, CD-13 and CD33. Br J Haematol 1988, 69:163-171 41. Pilkington GR, Wolf MM, Matthews JP, Griffiths JD, Cooper IA, Forster DC, Jose DG: Correlation of CD surface antigen phenotype with FAB subtype, remission induction (CR), and survival of AML patients. In Knapp W, Dorken B, Gilks WR, Rieber EP, Schmidt RE, Stein H, von dem Borne AEGKr, eds. Leucocyte Typing IV. White Cell Differentiation Antigens. Oxford, Oxford University Press, 1989, pp 931-935 Acknowledgments The authors thank Sybille Menges, Margarethe Kaiser, and John Moyers for technical assistance and Karin Tinter and Christine Raulfs for editing the manuscript.






© Copyright 2026