
Identification of a Point Mutation in Factor XI11 A Subunit
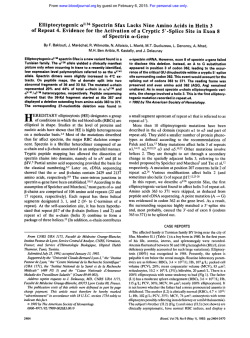
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Identification of a Point Mutation in Factor XI11 A Subunit Deficiency By Philip Board, Marjorie Coggan, and Kris Miloszewski Oligonucleotideprimers have been designed for the amplification of all 15 exons of the human coagulationfactor Xlll A subunit gene. Each exon and its intron flanking regions has been amplified and sequenced from a patient with severe A subunit deficiency. A single G to A transition in the last base of exon 14 has been identified in the homozygous proband and in his heterozygous parents. The mutation would result in the substitution 681 Arg to His in the mature protein product. However, because the mutation is at a splice junction, the deficiency may result from a defect in premessenger RNA splicing. 8 1992by The American Society of Hematology. C DNA sequencing was performed with a kit from Amersham (Sydney, Australia). Southern blots of digested genomic DNA were prepared on Genescreen Plus obtained from Dupont (Wilmington, DE). ct3$ dATP 3,000Ci/mmol was supplied by Amersham. Agarose (type 11) was obtained from Sigma Chemical Co (St Louis, MO). Antibodies to the A subunit of FXIII were obtained from Behringwerke (Marburg, Germany). Oligonucleotide primers were prepared on an Applied Biosystems 380B DNA synthesizer (Applied Biosystems, Foster City, CA). Unless otherwise specified, all chemicals used were of analytical grade. Patient. The patient is a male born in 1975. He bled from the umbilicus a few days after birth. Bleeding continued for 10 days and he received a blood transfusion. Thereafter, he was always covered with bruises, and suffered several large hematomas after minor trauma to the forehead and inside the mouth. Diagnosis of inherited FXIII deficiency was established at 3 years of age. He has been treated prophylactically since with FXIII concentrate and remains very well, free from bleeding manifestations and leading a normal, active life. The patient’s parents are second cousins. A diagnosis of A subunit deficiency was concluded, as a dansylcadaverine incorporation assay showed zero activity and specific A subunit rocket immunoelectrophoresis of plasma and platelet-rich plasma with lysed platelets failed to detect any A subunit protein. B subunit rocket electrophoresis showed 36% of the normal level. Haplotype anaZysis. DNA was isolated from nucleated blood cells12 and digested with BamHI, Bcl I, HindIII, and Taq I according to the conditions specified by the manufacturers. The digested DNA was subjected to agarose electrophoresis and then blotted onto nylon membranes.13The blotted DNA was probed with FXIII A cDNA labeled with ct32pdATP.14 of A subunit exons were PCR amplification. Amplificati~n’~ performed with the oligonucleotide primers listed in Table 1. The primers were phosphorylated by 30 minutes of incubation at 37°C in a reaction mix containing 100 mmol/L Tris/HCl, pH 8.0, 10 mmol/L MgC12, 1 mmol/L ATP, 3 mmol/L dithiothreitol (DTT), 75 pg/mL primer, and 10 U of T4 polynucleotide kinase. The reaction was terminated by heating at 70°C for 10 minutes. In all cases, the PCR reaction mix contained 1x Tag polymerase buffer (Promega), 0.75 pg of both forward and reverse primers, 0.2 mmol/L dATP, 0.2 mmol/L dCTP, 0.2 mmol/L dGTP, 0.2 mmol/L OAGULATION FACTOR XI11 (FXIII) is a zymogen that is converted by thrombin to a transglutaminase that catalyzes the formation of E-(y-glutamy1)-lysyl crosslinks between the y chains and between the a chains of fibrin monomers.’ Plasma FXIII is composed of two A and two B subunits2 The A subunits are joined as a dimer and are responsible for the catalytic a c t i ~ i t y . In ~ ? contrast, ~ the B subunits have no known catalytic activity and are thought to serve as a carrier molecule stabilizing the A subunits in the cir~ulation.~ The A and the B subunits are the products of separate genes that have been mapped to 6~24-25and 1q31-32.1, respectively.5S6 FXIII is essential for normal hemostasis and deficiency can lead to a severe bleeding diathesis.’~~ Inherited deficiency of FXIII has been diagnosed in many countries throughout the world, and does not appear to be associated with any particular ethnic gr0up.l Most cases studied appear to result from deficiency of the catalytic A subunit, and only one well-characterized deficiency of FXIII B subunit has been described.8 In most cases, the diagnosis of A subunit deficiency has been made on the basis of an absence of catalytic activity and the presence or absence of A subunit protein has not always been determined. Therefore, it is not clear how frequently FXIII A subunit deficiency arises from either the absence of protein or from the expression of a defective A subunit protein. In our experience, both types of deficiency can occur. In earlier studies, we identified a family in which an allele coding for an unstable form of A subunit was ~egregating.~,’~ In contrast, deficient individuals from other families did not appear to express A subunit.ll Nothing is known about the molecular nature of the mutations causing FXIII A subunit deficiency. The study reported here was undertaken to develop the procedures required to identify the precise molecular changes responsible for inherited FXIII A subunit deficiency. Oligonucleotide primers have been designed that permit the amplification by polymerase chain reaction (PCR) of all known exons in the A subunit gene. Sequence analysis of amplified DNA from an FXIII A deficient patient has located a point mutation at a splice junction that is likely to be the cause of the deficiency. MATERIALS AND METHODS The restriction enzymesBamH1,Bcl I, HindIII, Tag I, Sma I, and calf intestinal alkaline phosphatase were obtained from Boehringer Mannheim (Sydney, Australia); T4 polynucleotide kinase, Hpa 11, and T4 DNA ligase were obtained from Pharmacia (Uppsala, Sweden). Tag polymerase was supplied by Promega (Madison, WI). The nucleotides dATP, dGTP, dCTP, and dTTP were obtained from Pharmacia. cDNA probes were labeled by random priming with a kit from Besatek (Adelaide, Australia). All Blood, Vol80, No 4 (August 15), 1992: pp 937-941 From the Molecular Genetics Group, John Curtin School of Medical Research, Australian National University, Canberra, Australia; and the Department of Medicine, St James Hospital, University of Leeds, Leeds, UK. Submitted November 27,1991; accepted April 14, 1992. Address reprint requests to Philip Board, PhD, Molecular Genetics Group, John Curtin School of Medical Research, The Australian National University, GPO Box 334, CanberraACT 2601, Australia. The publication costs of this article were defrayed in pari by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section I734 solely to indicate this fact. 8 1992 by The American Society of Hematology. 0006-497119218004-0002$3.00/0 937 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. BOARD, COGGAN, AND MILOSZEWSKI 938 Table 1. Primers and Annealing Conditions for the Amplification of FXlll A Subunit Exons Exon 1 Forward 1 Reverse 2 Forward 2 Reverse 3 Forward 3 Reverse 4 Forward 4 Reverse 5 Forward 5 Reverse 6 Forward 6 Reverse 7 Forward 7 Reverse 8 Forward 8 Reverse 9 Forward 9 Reverse 10 Forward 10 Reverse 11 Forward 11 Reverse 12 Forward 12 Reverse 13 Forward 13 Reverse 14 Forward 14 Reverse 15 Forward 15 Reverse Primer 5’ - 3’ TACTCCCAGCAACTGGTTGC CTGGCTCATAGGGTGCAGG CATGCCTTTTCTGTTGTCTTC CTGGACCCAGAGTGGTGG GATTATITCTTCAACCCTTG TCTACAATGCAACCCATGG AATGGCTTGTGAAATCAACC GAAAACTAAATGTCTGCCTC GTTTGGTAATAGTCACTATG CAATAACAAATTTTAAGTGGC GCTTGCAGAGTGAACACTAG GCAAATGACAGGTGTAACAG CCTTCTCACTTCTCACGGAC AATGTCTTAGAGTGAAGTTTCC GCTGGTGATGTGmAGCTG CATCAGCCAATGCCATTGTC ATTACAGGCATGAGCCACTG TCAGCAATGAAGCAAGTTCC TGGACAGAATTGGAGATGAC AAACAGCACTTTCCTCCAGC ATGATGGCTAATGCTCTCC GAACTCATCTCTGAGTGAC TTGCCTGTCATTATCTCTGG GACAGCGAGTCTCACAAAG AAGTCTTGATGCCAGGCCTG TCTGTTCCAGGATGAGACGC GCTGCTAATGACCTGCATTC ACAGCTCTGCACTGCCTG GATCTTCCGAACCTCTCCTC ATGCCAGGGTTCATCTCAGC 382* 55 230 56 277 52 326 53 184 50 preparations were sequenced with an Amersham kit. All exons were sequenced in both strands. On average, five single-stranded clones were sequenced from each exon. Because of the possible infidelity of Taq polymerase, differences from the published may be due to amplification errors. To confirm differences from the published sequence, appropriate exons were recloned and sequenced from a separate PCR experiment. Restriction analysis of PCR products. The amplified exon 14 DNA was digested with Hpa I1 under the conditions suggested by the supplier (Pharmacia). The digested DNA was subjected to electrophoresis on a 12% acrylamide gel in a buffer comprising 90 mmol/L Tris, 90 mmol/L boric acid, and 2.5 mmol/L EDTA. The gel was stained with ethidium bromide and photographed under UV irradiation. 205 52 RESULTS 262 52 21 1 56 246 56 172 56 266 53 360 52 231 49t 211 52 226* 52 Length of Annealing Product Temperature (bp) (“C) ‘The amplified region extends from nucleotide -268 in the 5’ flanking region. tThis reaction contained 5 pL of dimethyl sulphoxide in total volume of 50 pL. *The amplified region extends to 11 bp beyond the translation stop codon. dTTP, 0.5 to 1 pg template DNA, and 0.5 to 1 U of Taq DNA polymerase (Promega). Denaturation was performed at 96°C for 1 minute, annealing was performed for 1minute at the temperatures indicated for each exon in Table 1, and the extension reaction was performed at 73°C for 1minute. All PCR reactions were performed in an Innovonic Gene Machine (Bartelt Instruments, Melbourne, Australia) and the amplification continued for 30 to 35 cycles. Sequence analysis. The exon DNA amplified by PCR with phosphorylated primers was cloned into M13 phage mp18.16 The mp18 vector DNA was digested with Sma I and treated with alkaline phosphatase to remove 5’ phosphates. The amplified DNA was purified by electrophoresis in 2% agarose in TBE buffer (90 mmol/L Tris, 90 mmol/L boric acid, 2.5 mmol/L EDTA). The DNA was recovered from the gel electrophoretically on an LKB (Stockholm, Sweden) Extractaphore. The amplified exon DNA was ligated to the Sma I-digested mp18 with T4 DNA ligase in “BRL,” blunt end ligation buffer (5x contains 250 mmol/L Tris/HCI, pH 7.6, 50 mmol/L MgCIZ, 5 mmol/L ATP, 5 mmol/L DTT, 25% wtlvol polyethylene glycol 8000 [PEG]) and transformed into competent Escherichia coli (TGI strain) by standard techniques. M13 clones containing inserts in different orientations were identified electr~phoretically~~ and single-stranded DNA Amplification of FXIII A exons. The gene encoding the A subunit of FXIII is composed of 15 exons.*9 Pairs of oligonucleotide primers suitable for the amplification of each exon and its intron splice junctions have been designed (Table l).The amplified exon l fragment contained 5’ flanking nucleotides that extended to -268. Because the 3’ end of exon 15 is not defined, the reverse primer sequence was positioned 11 bp 3’ of the translation stop codon. Under the conditions described in Materials and Methods, each exon was amplified from genomic DNA with little nonspecific contamination (Fig 1). The validity of the amplification of each exon was confirmed by sequence analysis. In normal subjects, the amplified sequences did not differ from the published Haplotype analysis. To determine if the patient we chose to study was potentially a true homozygote, or a compound heterozygote having inherited different FXIIIA mutations from each parent, we studied the restriction fragment length polymorphism (RFLP) haplotypes of the patient and his parents. Two allele RFLPs detected by BamHI, HindIII, and Taq I digestionsI4 and a multiple allele polymorphism detected by Bcl IZ1 digestion were evaluated. As shown in Fig 2, the proband was homozygous for each RFLP and has apparently inherited an identical haplotype from each parent. This suggests that the proband has inherited the same deficiency causing mutation from each parent and is a true homozygote. Sequence analysis. The A subunit exons were amplified from genomic DNA obtained from the proband and sequenced on both strands. A single base transition G + A was detected in the last base of exon 14 (Fig 3). This change alters codon 681 from CGT to CAT and would change the amino acid sequence of the A subunit product from 681Arg to 681 His. The deduced amino acid sequences of all other exons agreed exactly with that derived from the gene,I9 except for residue 651 Glu, which was in agreement with the protein sequence.Z0This difference results from a C to G change in the first base of the codon encoding residue 651. No changes were detected in intron sequences flanking the splice junctions and the GT-AG rule was adhered to in each case. Furthermore, no changes in the 5’ flanking sequence as far as -268 bp were detected. To confirm that this substitution was a property of the From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 939 MUTATION IN FACTOR Xlll DEFICIENCY thcrc was no cvidencc of thc 165-bp fragment. In contrast, both thc 165-bp and the 189-bp fragments could bc detected in thc parental samples. Thcsc rcsults indicate that the proband is homozygous for the cxon 14 G + A transition and his parents arc hctcrozygous for thc samc mutation. It is possiblc that the mutation wc obscrved in the proband and his family is a common polymorphism without dclcterious cffccts. Therefore, we studied the DNA from 20 normal blood donors by this RFLP technique and in each casc we detected the small 165-bp fragment, suggesting that they did not havc the G + A transition and that this mutation is not common and is rclatcd to the deficiency in this family. 154 220 #! 506 I632 DISCUSSION 1 2 3 4 5 6 7 9 10 11 12 13 14 15 8 bP 154 220 298 344 396 506 1632 Fig 1. The PCR reaction product for each pair of primers has been fractionated on 2% agarose gel. The number beneath each track indicates the pair of primers used and the exon amplified. Standard molecular size markers have been run at the side of each gel and their lengths are indicated in base pairs (bp). patient's genomic scqucncc and not dcrivcd from Ta9 polymcrasc infidelity, scvcral MI3 cloncs from two scparatc PCR amplifications of cxon 14 wcrc scqucnccd. In each case. the G + A transition was obscrved. The normal scqucncc (G) was not dctcctcd in any MI3 clonc dcrivcd from the proband. The G + A mutation obscrvcd in thc proband results in thc loss of a Hpa 11 sitc in the PCR amplification product. As shown in Fig 4A, digestion of thc 211-bp cxon 14 amplification product from a normal control with Hpa I1 should give risc to fragments of 165, 24, and 22 bp. In contrast, digestion of thc samc PCR product from thc proband should givc rise to fragments of 189 and 22 bp. To dctcrminc if thc G + A substitution is inherited and could bc dctcctcd in thc proband and his parents, amplified cxon 14 fragments wcrc digested with Hpa I I and fractionated by electrophoresis on acrylamidc gcls. As shown in Fig 4B, thc normal control showcd thc prcscncc of thc cxpcctcd 165-bp fragment. The proband showed a 189-bp fragment and In this study, we have designed oligonucleotidc primers and defined reaction conditions for thc amplification of the 15 FXIll A subunit gene exons. The primers for exon 1 encompass 5' flanking scqucnces extending to nucleotide -268. This rcgion contains sevcral potential regulatory clcments'" and may contain a promotcr, although there is no experimental evidence demonstrating that thcsc clcmcnts contributc to the regulation of FXffU transcription. Except for the 3' cnd of exon 15, the amplified fragments all contain thc cxon coding scquences with their 5' and 3' splicc junctions and immcdiatc flanking regions. Sequencing thc fragments amplified from deficient patients under the conditions dcscribcd in the present experiments should show thc vast majority of mutations giving rise to deficiency of FXIll A subunit. Thc A subunit genc FXIII A is autosomal and has been mappcd to the distal region of the short arm of chromosome 6.s In many autosomal recessive disorders, such as FXlll A deficiency, affectcd individuals are compound hctcrozygotes with two mutations affecting A subunit synthesis or function. Thus, at the site of each mutation, the deficient patient also has a normal allele on the alternate chromosome. If fragments containing particular mutations arc amplificd by PCR, the DNA from the normal and BamHI B BamHI C Hind I11 Taq I Bcl I -++ ++- ++ -+ ++- aa b a a a Fig 2. The 0 family showing the inheritance of Fxlll A subunit deficiency (darkenedsections) and RFLP haplotypes. The RFLPs with two alleles are indicated as or and the Ecl I polymorphism that has multiple alleles has been identified alphabetically. The nomenclature for the 8cl I RFLPs relates only to this family. + - From www.bloodjournal.org by guest on February 6, 2015. For personal use only. BOARD, COGGAN, AND MILOSZEWSKI 940 G Normal G A T C G Exon14 Patient T C C C --G V G T A A A Intron N C A G T A A A G A T C Fig 3. Part of the nucleotide sequence of exon 14 and intron N of the human FXlll A subunit gene. The normal sequence is on the left and the dotted line shows the normalsplice junction. The mutation in the patient is shown by an arrow. mut d chromosomes will be amplified equally and, when cloned in M I 3 for sequencing, will give rise to equal numbers of clones with the normal or mutant sequence. In such cases, many M13 clones from each amplified fragmcnt need to be sequenced to identify the mutation. Altcrnatively, direct sequencing can be used, but these methods have other associated drawbacks. In the present case, the sequence analysis was simplified by the fact that the proband appeared to be a true homozygote because he was homozygous for five closely linked RFLPs and showed the inheritance of an identical RFLP haplotype from each parent. Furthermore, it was known that the parents were second cousins, increasing the probability that the mutation had an identical familial origin. Sequence analysis of amplified exons from the patient identified a G + A transition in the last base of exon 14. Two additional changes were detected in individual clones; however, they could not be confirmed by sequencing other clones from the original amplification or after rcamplification and cloning. We concluded that these changes were amplification artifacts. The mutation we identified was confirmed by sequencing multiple MI3 clones in both orientations and M 13 cloncs dcrivcd from two independent PCR experiments. The G 4 A transition was idcntificd in cvcry clone of amplified exon 14 from the proband. The absence of a normal sequence confirmed his predicted homozygosity. It is not immediately clear what effcct the obscrved mutation has on A subunit function and expression. The point mutation occurs in the coding sequcncc and would result in the amino acid substitution 681 A% to 681 His. Because littlc is known about the active site of the A subunit and the residues required for substrate binding and catalysis, it is not clear whether the change would substantially altcr the mutant subunit's catalytic function, stability, structure, or interaction with B subunits. The lack of any immunologically detectable A subunit in plasma and platelets from the proband suggests that the defect primarily influences its expression or stability. It may be significant that the mutation is located at a splice junction. Introns in higher eukaryotic prc-messenger RNAs (mRNAs) are bounded at the 5' end by the consensus sequence (C/A)AG/ A Normal Patient 165 c CCG Fig 4. (A) The amplified exon 14 fragment is 211 bp and contains two Hp.9 II sites indicated by arrows. The mutation in the patient deletes one site. The expected sizes of the DNA fragments after Hpe II digestion are indicated. (6) Electrophoretic fractionation of amplified exon 14 digested with Hps II. The normal control sample is indicated N and the different members of the 0 family are indicated by the family tree. bP 189 165 CGG 1 189 C CAC B c 22 C CGG From www.bloodjournal.org by guest on February 6, 2015. For personal use only. MUTATION IN FACTOR Xlll DEFICIENCY 941 GU(G/A)AGU.zz,z3Although the GU at the start of the intron (underlined) is largely invariant, variations in other ~ , survey ~ of 5’ splice sitesz4 positions are known to O C C U ~ ? A has shown that, while G is the most common base in the -1 position, A occurred in 8 of 99 sites studied. Although the G --* A transition detected at position -1 in exon 14 does not absolutely exclude normal splicing, there is evidence that components of the flanking exon sequence can influence the site specificity of ~ p l i c i n g . ~ ~ - ~ ~ A number of studiesz3-z5have implicated the hybridization of U1 small nuclear (sn) RNA in the specific recognition and cleavage of 5’ splice junctions. Mutations in the exon sequence adjacent to the splice junction have been shown to directly influence U p R N A hybridization and to modify the efficiency of cleavage. Because the G + A transition observed in these experiments is in the exon immediately adjacent to the normal cleavage site, it is clear that it will substantially decrease potential hybridization of the UlsnRNA in the correct position, which may lead to either a decrease in the efficiency of cleavage, the elimination of cleavage, or even cleavage at an adjacent cryptic site. Thus, the cause of the A subunit deficiency in the present case may be due to a splicing defect. At this stage, it is not possible to conclude if the observed point mutation alters pre-mRNA splicing or if the subunit with the 681Arg +His mutation is unstable. To resolve this question, in future studies it may be possible to express a cDNA clone containing the same mutation and to directly evaluate the properties of the recombinant protein? In conclusion, we have defined oligonucleotide primers that allow amplification of all the coding regions of the FXIII A subunit gene and their intron/exon splice junctions. We have amplified and sequenced all of these regions from a homozygous deficient patient and identified a point mutation that could cause the deficiency. In accordance with the convention established with other coagulation factors, we propose that this FXIII A subunit defect be described as the Canberra I mutation. REFERENCES 1. Lorand L, Losowsky MS, Miloszewski KJM: Human factor XI11 fibrin-stabilizingfactor. Prog Hemost Thromb 5:245,1980 2. Schwartz ML, Pizzo SV, Hill RL, McKee P A Human factor XI11 from plasma and platelets. J Biol Chem 248:1395,1973 3. Board PG: Genetic polymorphism of the A subunit of human coagulation factor XIII. Am J Hum Genet 31:116,1979 4. Mary A, Achyuthan KE, Greenberg CS: B-chains prevent proteolytic inactivation of the a-chains of plasma factor XIII. Biochem Biophys Acta 966:328,1988 5. Board PG, Webb GC, McKee J, Ichinose A Localization of the coagulation factor XIIIA subunit gene (F13A) to chromosome bands 61324 + p25. Cytogenet Cell Genet 48:25,1988 6. Webb GC, Coggan M, Ichinose A, Board PG: Localization of human coagulation factor XIIIB subunit gene (F13B) to chromosome bands 1q31-32.1 and restriction fragment polymorphism of the locus. Hum Genet 81:157,1989 7. Duckert F, Jung E, Schmerling DH: A hitherto undescribed congenital haemorrhagic diathesis probably due to fibrin stabilizing factor deficiency. Thromb Diath Haemorrh 5:179,1960 8. Saito M, Asakura H, Yoshida T, Ito K, Okafugi K, Yoshida T, Matsuda T: A familial factor XI11 subunit B deficiency. Br J Haematol74:290, 1990 9. Castle S, Board PG, Anderson RAM: Genetic heterogeneity of factor XI11 deficiency: First description of unstable A subunits. Br J Haematol48:337,1981 10. Castle S, Board PG: Biochemical characterization of genetically variant and abnormal blood coagulation factor XI11 A subunits. Clin Chim Acta 133:141,1983 11. Board PG, Coggan M, Hamer JW: An electrophoretic and quantitative analysis of coagulation factor XI11 in normal and deficient subjects. Br J Haematol45:633,1980 12. Grunebaum L, Cazenave J-P, Camerino G, Kloepfer C, Mandel J-L, Tolstoshev P, Jaye M, De La Salle H, Lecocq J-P: Carrier detection of haemophilia B using restriction site polymorphism associated with the coagulation factor IX gene. J Clin Invest 73:1491,1984 13. Reed KC, Man D A Rapid transfer of DNA from agarose gels to nylon membranes. Nucleic Acids Res 13:7207, 1985 14. Board PG, Chapple R, Coggan M: Haplotypes of the coagulation factor XIIIA subunit locus in normal and deficient subjects. Am J Hum Genet 42:712,1988 15. Saiki RK, Scharf SJ, Faloona F, Mullis KB, Horn GT, Erlich HA, Arnheim N Enzymatic amplification of P-globin genomic sequences and restriction site analysis for diagnosis of sickle cell anaemia. Science 230:1350,1985 16. Norrander J, Kempt T, Messing J: Construction of improved M13 vectors using oligodeoxy nucleotide-directed mutagenesis. Gene 26:101,1983 17. Messing J: New M13 vectors for MI3 cloning. Methods Enzymol101:20,1983 18. Ichinose A, Hendrickson LE, Fujikawa K, Davie E W The amino acid sequence of the A subunit of human factor XIII. Biochemistry 25:6900,1986 19. Ichinose A, Davie EW: Characterization of the gene for the A subunit of human factor XI11 (plasma transglutaminase), a blood coagulation factor. Proc Natl Acad Sci USA 85:5829,1988 20. Takahashi N, Takahashi Y, Putnam FW: Primary structure of blood coagulation factor XIIIa (fibrinoligase, transglutaminase) from human placenta. Proc Natl Acad Sci USA 83:8019,1986 21. Zoghbi HY, Daiger SP, McCall A, OBrien WE, Beaudet AL: Extensive DNA polymorphism at the factor XIIIa (F13A) locus and linkage to HLA. Am J Hum Genet 42:877,1988 22. Mount SM: A catalogue of splice junction sequences. Nucleic Acids Res 10:459,1982 23. Aebi M, Hornig H, Weissmann C: 5’ Cleavage site in eukaryotic pre-mRNA splicing is determined by the overall 5’ splice region, not by the conserved 5’ GU. Cell 50:237,1987 24. Oshima Y, Gotoh Y: Signals for the selection of a splice site in pre-mRNA computer analysis of splice site junction sequences and like sequences. J Mol Biol195:247,1987 25. Smith CWJ, Patton JG, Nadal-Ginard B: Alternative splicing in the control of gene expression. Ann Rev Genet 23:527,1989 26. Board PG, Pierce K, Coggan M: Expression of functional coagulation factor XI11 in Escherichia coli. Thromb Haemost 63:235,1990 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1992 80: 937-941 Identification of a point mutation in factor XIII A subunit deficiency P Board, M Coggan and K Miloszewski Updated information and services can be found at: http://www.bloodjournal.org/content/80/4/937.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.









© Copyright 2026