
Natural Protection Against Severe Plasmodium falciparum
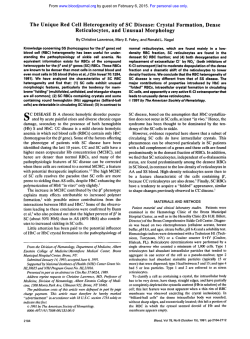
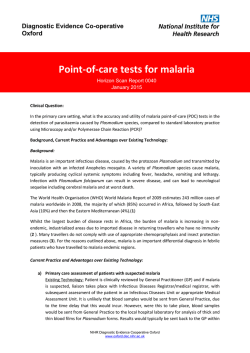
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Natural Protection Against Severe Plasmodium falciparum Malaria Due to Impaired Rosette Formation By Johan Carlson, Gerard B. Nash, Vilma Gabutti, Fadwa AI-Yaman, and Mats Wahlgren Genes for two lethal diseases, thalassemia and sickle cell anemia, are favored by evolutionbecause, in their heterozygous form, they protect against cerebral malaria. Rosette formation, the binding of uninfected redcells (RBCsI to Plssmodium fabiparuminfected RBCs (PRBCsI, has previously been foundto be associatedwith cerebral malaria,the most important sovere manifestation of P fa/ciparum malaria. We show here that thalassemic RBCs and, under certain conditions, even hemoglobinS (HMI-containing RBCs possess an impaired abilityto bind to PRBCs, forming small and weak erythrocyte rosettes compared with rosettes formed by normal RBCs. This decreasedrosetting a b i l i is associated with the small size of the thalassemic RBCs and with distortion of the mechanical properties of HbS-containing RBCs. The impairment of rosette formation may hinder the development of cerebral malaria by abatement of sequestration. 0 7994 by The American Society of Hematology. E cerebral malaria exhibit an impaired rosette-forming ability, with data suggesting that this is a mechanism that could mediate natural protection against the disease. XCESSIVE BINDING of Plasmodium falciparum-infected erythrocytes [parasitized red blood cells (PRBCs)] to endothelial cells and to uninfected red blood cells (RBCs) seems crucial for the occurrence of microcirculatory obstruction in human cerebral malaria, but the underlying processes that lead to this state of infection are comp l e ~ . "One ~ attractive approach to the understanding of the pathophysiologic mechanism is the study of the red cell defects known to protect against severe malaria. It has been shown that individuals with a- and &thalassemia and with sickle cell trait (HbAS) can acquire P fakiparum malaria, but that they experience reduced fatality and seventy of the disease;"" eg, the protection against cerebral malaria in children with HbAS is more than 90%, but the effect on parasite densities is less pronounced." Blood group 0 was recently found also to be associated with significant resistance to cerebral malaria as compared with blood group A or B (Hill" and Hill et al, personal communication, 1992). It has been suggested that the hampered growth and an increased tendency to sickling of HbAS-infected cell^'^"^ and neoantigen expression on thalassemic RBCS'~.'~ are the reasons for the protective effects. However, while these mechanisms may play roles in the resistance to malaria, they do not fully explain the absence of microcirculatory obstruction seen in individuals with aberrant red cells. Could it be that these RBCs are less prone to forming rosettes and to binding to endothelial cells and, therefore, hinder the development to coma and death? Increased frequency of spontaneous erythrocyte rosetting around PRBCs has been shown to be associated with cerebral m a l a ~ i a .At ~ . ~autopsy Hidayat et a l l 8 observed "rosetting of the parasitized erythrocytes . . . within the partially occluded lumens," and in exvivo experiments, the obstruction of the blood flow was found to be considerably more pronounced with a rosette-forming parasite than with a nonrosetting parasite that merely bound to the vascular endothelium." Moreover, anti-rosetting antibodies were frequent in sera of children with mild malaria but absent or only present at low levels in those with severe di~ease.4.~ Thus, rosetting has been proposed to play a keyrole in the excessive sequestration of PRBCs and RBCs in the microvasculature and in the pathogenesis of cerebral disea~e.4.'.'~-~~ Therefore, it could be postulated that the protective effect of certain red cell disorders against cerebral malaria is mediated via impaired rosette formation. We investigated a number of red cell disorders with respect to their impact on rosetting and report that RBCs from individuals naturally protected against Blood, Vol 84, No 11 (December l ) , 1994: pp 3909-3914 MATERIALS AND METHODS P falciparum culture. The P falciparum R'PA1 parasite, a cloned, rosetting parasite obtained from the Palo Alto Ugandan strain, was cultured according to standard procedures**with10% h 'serum added to the buffered malaria culture menormal AB+ R dium (MCM). Erythrocytes. Blood was drawn into heparinized tubes or tubes containing citrate phosphate dextrose (CPD), and the RBCs were washed three times in TRIS-Hanks' solution. AB0 blood group typing was performed by hemagglutination with monoclonal antibodies specific for the different blood group antigens (BioCarb, Lund, Sweden). RBC morphology was evaluated by light microscopy, and the erythrocyte mean cell volume (MCV) and hemoglobin concentration were measured by a Coulter S Plus (Coulter Electronics Ltd, Luton, UK). Hemoglobin electrophoresis and electrofocusing were used to quantify the hemoglobin type of the RBCs. RBCs were obtained from four individuals with sickle cell disease (HbSS), from three that were of the sickle cell trait (HbAS), and from one exhibiting the hemoglobin SC (HbSC) phenotype. Samples from nine Papua New Guineans with Southeast (SE) Asian ovalocytosis contained 11.8% to 89.2% ovalocytic cells as counted in 500 RBCs with a 40X objective lens. Of the 19 individuals with P-thalassemia From the Microbiology and Tumor Biology Center, Karolinska Institute, and the Swedish Institute for Infectious Diseases Control, Stockholm, Sweden: the Department of Infectious Diseases, Uppsala University9 Akademiska sjukhuset, Uppsala, Sweden: the Department of Haematology, University of Birmingham, Birmingham, UK; the Department of Pediatrics, University of Torino, Torino, Italy: and the Institute of Medical Research, Madang, Papua New Guinea. Submitted January 18, 1994; accepted July 27, 1994. Supported by grants from the United Nations Development Program/World BanVWorld Health Organization Special Programme for Research and Training in Tropical Diseases (TDR), The Maud and Birger Gustavsson Foundation, the Swedish Medical Research Council, the Swedish Agency for Research Cooperation with Developing Countries (SAREC), and the Swedish Society of Medicine. Address reprint requests to Mats Wahlgren, MD, Microbiology and Tumor Biology Center, Karolinska Institute, Box 780, S-l71 77 Stockholm, Sweden. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 W.S.C. section 1734 solely to indicate this fact. 0 1994 by The American Society of Hematology. 0006-4971/94/8411-0041$3.00/0 3909 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. CARLSON ET AL 3910 trait, 14were ItaliansorWestAfricanswith 8'. one was a Thai with the b/p-thalassemia type. and three were West Africans with combined p+/HbS. All the 0-thalassemic RBCshad a lowMCV. Three of four individuals with a-thalassemia trait were of the athal I phenotype, while one (Thai) was of the Hb Constant Spring phenotype. All of these RBC samples exhibited a moderate microcytosis. RBCs werealso obtained from three patients with microcytic anemia(secondary to chronicirondeficiency or severebacterial infection), and from six samples of cord blood with high HbF contents (67% to 85% HbF). Assessment of rosette formationand disruption of rosettes. The R+PAI strain grown in 0' RBCs was subcultivated in blood from donors with normal (HbAA), &thalassemia trait, or HbAS RBCs, and assessment for rosette formation was made as described previously.'.' The rosetting rate was defined as the number of PRBCs in rosettes, expressed as a percentage of the total number of latestage (trophozoite and schizont) PRBCs. The individual rosette size was defined as the mean number of uninfected RBCs bound to each PRBC." Rosettes in culture were disrupted mechanicallyby drawing the erythrocyte mixture through a narrow gauge injection needle six to eight times.', Assessment of rosette formation was made after spontaneous reformation of rosettes, and different aliquots from the same culture were compared after different pretreatments. Carboq-Juorescein diacetate (C-FDA)-labelingof RBCs and assessment of rosette-forming capacip. The relative rosette-forming capacity of RBCs from patients with various red cell disorders was measured as described before, by a method where C-FDA-labeled RBCs were allowed to compete for rosetting with unlabelled RBCs." The R'PAI strain was cultured in blood group 0 (HbAA) RBCs, and rosettes were disrupted by addition of heparin (50 IUlmL; Kabi Pharmacia AB, Stockholm, Sweden). Fractionation and deoxvgenation of HbS-containing RBCs. HbSS or HbSC RBCs were fractionated ona Ficoll-Isopaque continuous density gradient (Pharmacia AB, Uppsala, Sweden), andthe less dense cells were harvested as described." Cyclical deoxygenation-reoxygenation was performed for 15 hours with a Cyclical Gas Exchanger(WolfsonResearchLaboratories,Birmingham, UK),'s causing changes in cell hydration and deformability that mimic the deterioration that occurs for dense cells in vivo.'" In separate experiments, HbAS, HbSS, or HbSC RBCs were deoxygenated by adding a mixture of sodium dithionite and disodium hydrogen phosphate (2 v01 0.1 14mol& Na2S20, + 3 v01 0. I 14 molL Na'HPO,;pH 6.8) to the erythrocyte suspension in proportion 1 : I .'' The morphologyof the RBCs was studied before and after cyclical deoxygenation-reoxygenation or treatment with dithionite, after fixation with I % glutaraldehyde.HbASRBCsandlessdenseHbSS RBCs were essentially discocytic, except that the latter contained a few distorted, boat-shaped cells (irreversibly sickled cells, ISCs). Treatment with dithionite led to the formation of distortedcells and of ISCs, and few discocytes remained (about 30% for HbAS cells and less for HbSS cells). Cyclical deoxygenation of the less dense HbSSRBCs also led to formation of distortedRBCs, as well as some ISCs(8% on average). A distinction shouldbe made, however, between dithionite-treated cells, which are distortedby the formation of polymerized HbS, and cells subject to cyclical deoxygenationreoxygenation, which dehydrate and accumulate membrane damage but do not contain polymer when reoxygenated for further study. No changes were seen in HbAARBCs treated with either ofthe above-mentioned methods. Measurement of eythrocyte binding strength bv a micropipette in method. Samples of malaria cultures werediluted100-fold MCM,andthesuspensionwasplaced in a micropipette chamber where the binding strength of individual RBCs within rosettes was studied by a dual-micropipettemethod (Fig l), as describedpreviously.*' The aspiration pressure (P) required to detach cells from Fig 1. The dual-micropipettetechnique.Theparasitized RBC (right) is held by the larger holding pipette, and a bound RBC is detached by increasingthe aspiration pressurein the smaller pipette (left). rosettes by a micropipette (internal diameter, D) was recorded, and theforcewascalculated [F = (n/4)(D2)P]. In someexperiments, after all the cells had been stripped froma rosetting, parasitizedcell, other cells in the chamber were picked up with one of the pipettes and brought into contact with the stripped parasitized cell, allowing cell-cell binding to occur. After a delay of 3 minutes, the force to detach the nonparasitized cell was measured, as described.2R RESULTS RBCs from individuals with various red cell disorders were examined for their capacity to form rosettes in competition with normal(HbAA) 0,Rh' RBCs. Whereas cord RBCs with a high HbF content or RBCs from individuals with SE Asian ovalocytosis bound equally well or only slightly less as compared with normalRBCs, thalassemic RBCs and other microcytic RBCs exhibited a reduced rosette-forming capacity, as did HbS-containing RBCs under deoxygenated conditions (Fig 2). Thus, both a- and 0-thalassemic RBCs exhibited a reduced rosette-forming capacity when competing with RBCs from normal (HbAA) individuals (Fig 2). When RBCs from four individuals with 0-thalassemia trait were comparedwith RBCs fromfivenormal (HbAA) individuals, a significant From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 391 1 IMPAIRED ROSETTE FORMATION IN MALARIA reduction in mean binding strengthwas found forthe smaller ,&thalassemic RBCs (Fig 3). These studies also confirmed thepreviouslyreportedfinding of astrain-specific A B 0 blood group preferencein rosette-forming capacity. Ahigher bindingcapacityandlarger rosetteswere foundfor the R'PA1 clone with blood group A/AB RBCs compared with group O/B RBCS,'~ and similarly, when using the same P 5 4 I HbAA I T 6 T T 3 HbF 2 8 Ovalocytosis I 1 HbAs 0 I &thalassemia HbAA Fig 3. Force required to detach individual uninfected RBCs bound i n a spontaneous rosette aroundP falciparum-infected RBCs. Values given are mean values 2 SD. The binding strength wascompared by measuring 50 t o 68 RBCs from every patient. The 0-thalassemia trait was P+-type1. AB0 blood group of donors: A, A; 0, B; 0 0.Statistical analysis was performed between themean detachment force of the t w o groups of patients using the nonparametric Mann-Whitney U test (P= .0121. Hbss HbSC HbEF HbAA microcytosis 0 20 40 60 80 100 120 Rosette forming capacity (% of control) Fig 2. Relative rosetting capacity of various C-FDA-labeled RBCs to HbAA infected RBCs. The tested RBCs were from nine individuals of normal hemoglobin phenotype Inorrno-or microcytic) or from 35 individuals with various red cell disorders (CS, Hb Constant Spring; S / p , mixed HbS/p-thal trait). m, RBCs under normal ambient 0,; 0, RBCs treated by cyclical deoxygenationlreoxygenation;a, RBCs deoxygenated by sodium dithinonite.The binding of C-FDA-labeled RBCs from an 0 Rh+ donor wasused as index (100%). and the blood group A/AB preference of the strain was compensated for as described p r e v i o ~ s l y . ~ ~ falciparum clone here, stronger binding forces were seen for RBCs from the HbAAhlood group A donors than for RBCs from the HbAAhiood group B or 0 donors (Fig 3). Also with the P-thalassemic individuals, small ABO-differences could be noted (Fig 3). When the R'PA1 clone was cultured in RBCs from 12 individualswith ,&thalassemia traitand in RBCs from three normal HbAA controls,asignificant correlation between the rosette-forming capacityof the abberant RBCs and the MCV was found (Fig 4A), imposed on the blood group ABO-related differences already known to exist. A similar correlation was also seen between the erythrocyte MCV and the mean individual rosette size: the lower the MCV, the smaller the rosettes (Fig 4B). No significant difference wasseen inthe rosetting rate orin the parasitemias of the cultures (data not shown). RBCsfromindividuals withmicrocytic anemiadue to other disorders (eg, severe chronic bacterial infection, iron deficiency, or HbE disease) were also found to bind poorly in rosettes when competing with normocytic cells (Fig 2). A significant reduction ( P < .01, Mann-Whitney U test) in binding strength for microcytic cells compared with normocyticred cells wasfound when RBCsfromtwo patients From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3912 CARLSON ET AL with microcytic anemia secondary to iron deficiencykhronic bacterial infection were compared with ABO-matched controls (binding force: mean, 1.4 X IO"" and 1.6 X 10 -li) N, respectively, for the microcytic RBC populations; 2.2 X IO-^'" and 2.5 X 10 "l N for the normocytic). HbSS or HbAS RBCs bound normally to P falcipururninfected RBCs when competing withHbAA RBCs under normal oxygen pressure, but after exposure of HbSS cells to cyclical deoxygenation-reoxygenation or when deoxygenated with dithionite before the assay, the binding capacity A 4 h I2O] 50 1 60 . I 70 . I 80 MCV . I After Reformation Deoxy Control HB/HbAS 3.3 It_ 0.8 3.5 2 0.7 2.4 2 0.6 3.3 't 0.6 P < ,0001 NS Deoxy Control NS/HbSS 4.2 f 1.1 4.5 It_ 1.2 3.3 2 0.9 4.2 t_ 1.1 P < ,0001 Deoxy Control 4.2 f 1.2 4.2 f 1.2 3.2 2 0.9 4.0 2 0.9 P NNHbAS NS 'r. ,0001 NS I 90 100 90 100 2 50 Before Disruption + 51 ' Donor Initials/ Phenotype The P fakiparum clone R PA1 was cultured in untreated RBCs and RBCs deoxygenated by dithionite (see Materials and Methods) from three different donors. The cultures were assessed for mean individual rosette size (the number of uninfected RBCs bound toparasitized RBCs f SD) by counting 50 rosettes, and each determination was performed twice. Statistical analysis was performed between the individual rosette sizes before and after reformation using the nonparametric Mann-Whitney U test. Abbreviation: NS, not significant. 0 601". Table l.Mean Individual Rosette Size Before Disruption and After Spontaneous Reformation of Rosettes in P falciparum Cultures Grown in HbAS and HbSS RBCs 60 70 80 MCV Fig 4. The relationship betweenMCV and the relative erythrocyterosetting capacity or mean individual rosette size. RBCs were obtained from 12 individuals with @thalassemia trait (/3'-type 1) or from three individuals with normal (HbAA) RBCs and with different AB0 blood group: A, A; AB; U, B; 0, 0. Patients with normal (HbAA) hemoglobin phenotypeare indicated as AA. In both analyses, 50 rosettes wereassessed t w i c e and ontwo independent occasions. (A) MCV versus erythrocyte-rosetting capacity of C-FDA-labeled RBCs (when the blood group phenotype has been compensated for)?' The statistical analysis was performedwith simple regression analysis: r = 0.95; 9 = 0.91; P < ,0001.(B)MCV versus mean individual rosette size. Statistical analysis was performedwith multipleregresparasion analysis, taking intoaccount that, when using the R+PAI site, RBCs of the AlAB phenotypes form larger rosettes than 018 phenotypes, independent of other parameters": r = .90 8 = .81; P < .001. +, was reduced (Fig 2). When P falciparum (clone R+PAl) was cultured in REKs from two individuals with sickle cell trait (HbAS) and one with sickle cell disease (HbSS), no significant difference was seen in the rosetting rate, the mean individual rosette size, or the parasitemia compared with cultures withHbAA RBCs of corresponding A B 0 blood group (data not shown). However, chemical deoxygenation of the blood, followed by mechanical disruption and spontaneous reformation of rosettes, induced a significant drop in mean individual rosette size in the HbAS and HbSS cultures compared with untreated HbAS/SS controls (Table 1). By using the micropipette technique, it could also be shown that HbSS discocytes had a mean binding force not differing from that of discocytes from a normal (HbAA) individual (Fig 5). After cyclical deoxygenation-reoxygenation of the HbSS RBCs, significantly impaired binding capacity was found in the ISCs and also in the moderately distorted, dehydrated RBC population (Fig 5). DISCUSStON Using three independent assays we report that certain aberrant RBCs form small and weak erythrocyte rosettes and hypothesize that this reduced ability to form erythrocyte rosettes may protect against severe P fakiparum malaria, ie, by preventing the formation of large stable red cell aggregates and obstructing the cerebral microvasculature otherwise seen in cerebra1 malaria. Low cell volume, a common denominator of the a- and P-thalassemias, is associated with a reduced rosette-forming capacity.29Here we also show that the reduction in rosetting seems to be related to the low red cell volume (MCV) per se, irrespective of the origin of microcytosis, as small erythrocytes from HbAA patients with other causes of microcytosis as wellof those with HbE and HbC form weak From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 391 3 IMPAIRED ROSETTE FORMATION IN MALARIA Fig 5. Force required to remove individualuninfected RBCs attached to a rosetting P fakiparumparasitized cell for 3 minutes. Values given are mean attachmentforce (? SD) as measured by micromanipulation of 28 to 36 uninfected RBCs per assessed cell population. Cyclical deoxygenation/ reoxygenation was performed with a Cyclical Gas Exchanger (see MaterialsandMethods). Donors (initials and hemoglobin phenotype):U, BCIHbAA; a, MS/HbAA; 0,BT/HbSS; 0 NS/HbSS; @, C S / HbSS. Statisticalanalysis was performed with Student's ttest for each HbSS donor between thediscocyte and the distorted RBC population and betweenthe discocyte andthe ISC populations, respectively. All differences in mean detachment forces between the various RBC populations were statistically significant (all P values < .001). 01 I HbAA H ~ S Sdiscocytes discocytes before cyclical de-/reoxygenation rosettes. Other investigators have studied features of microcytic cells that might protect against malaria, such as restriction of parasite growth or impairment of cytoadherence of infectedcells,but have not foundconvincingcorrelaa common tions.'"."" Restricted rosetteformationmaybe protective mechanism for microcytic RBCs, thus conferring significant clinical protection against cerebral malariain disorderswithprofound microcytosis likethe thalassemias. This hypothesis is supported also by the recentreport by other investigators of impaired rosette formationof thalassemic RBCs.?' The possible protective effect of impaired rosette formation in other disorders might be moredifficult to assess (eg, iron deficiency, with a mixed pattern of microcytosis)although malnutrition-andespecially iron deficiency-has in factbeenclaimedtoconfer protection against malaria. However, this issue is highly controversial, and polar views have been A diminished rosette-formingcapacity wasevident already for deoxygenated, slightly distorted HbAS, HbSC, or HbSS cells. In addition, after repeated sickling of HbSC or HbSS cells, rosetting was inhibited even when the cells were oxygenated. Thus, already moderate changes in cellularmechanical properties, knowntooccurnotonly with HbSS R B C S ~but ~ also withbothinfected and uninfected HbAS RBCsunder unfavorableconditions,"j cause asignificant loss of rosette-binding capacity. The obstruction of the microvasculature and the concomitant lower oxygen tension seen in cerebral malaria seems likely to be such an unfavorof inducing changes able or even extreme condition capable in the rheologic properties of a significant number of HbAS cells. Acknowledging thewell-known difficulties in extrapolating in vitro data to in vivo conditions, we nevertheless suggest that the impaired rosette-forming ability expressed even in moderatelychangedHbASRBCs,inconjunction with other potential protective phen~mena,'.""~ may contribute to the protection against cerebral malaria. Paradoxically, thispotential mechanism of resistance, aswellasothers previously de~cribed,'~.~' seemstoinvolve all HbS-con- Discocytes Distorted RBcS I IsCS HbSS cells after cyclical deoxygenationheoxygenation taining RBCs, despite the factthat individuals with homozygoussicklecelldisease oftensuffer more severely from malarial disease with high mortality. However, this fact may mostlikely be attributed to the sickle cell disease per se despiteaninnateresistanceto malarialinfection existing also in homozygote^.^'^^^ Rosette formation is mediated by protein ligands, rosettins, on the infected RBCs that bind to carbohydrate receptors on the uninfected R B C S . ~ ~ , *Whether ~ . ~ " the decreased rosette binding with microcytotic RBCs is due to a lower availability and/or a lower expression of the carbohydrate structures remains to be investigated. For HbSS and HbAS RBCs, on the other hand, it is not lack of receptors but the accessibility of them, influenced by the distortion or rigidification of the cells, that abatesbinding, as therosetting capacity is dependent on the ambient oxygen pressure. Some studies also give support for a modifying role of SE Asian and Melanesian ovalocytosisand HbF in P falciparum malaria.41,42However, the protection conferred by SE Asian ovalocytosis or a high HbF content does not seem to involve erythrocyte rosetting. ACKNOWLEDGMENT We thank all blooddonorsthatparticipated in thisstudyand Drs Rosa Bachetta (DNAX Research Institute, Palo Alto, CA) and Michael Alpers (Institute of Medical Research, Madaug, Papua, New Guinea)forinvaluablehelpwiththebloodsamples.Thehelpful advice on the statistics givenby Johan Bring (Department of Statistics, Uppsala University, Uppsala, Sweden) is also acknowledged. REFERENCES 1. Trager W, Rudzinska MA, Bradbury PC: The fine structure of Plasmodiumfulci~~arum and its host erythrocyte in natural malarial infections in man. Bull WHO 35383, 1966 2. Luse SA, Miller LH: PlasmodiLlm~u~ciparum malaria: Ultrastructure of parasitized erythrocytes in cardiac vessels. Am J Trop Med Hyg 20:650, 1971 3. Udomsangpetch R, WIhlin B, Carlson J , Berzins K, Torii M, Aikawa M, Perlmann P, Wahlgren M: Plasmodium fulciparum-in- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3914 fected erythrocytes form spontaneous erythrocyte rosettes. J Exp Med169:1835,1989 4. Carlson J, Helmby H, Hill AVS, Brewster D, Greenwood BM, Wahlgren M: Human cerebral malaria: Association with erythrocyte rosetting andlackof anti-rosetting antibodies. Lancet 336:1457, 1990 5. Treutiger CJ, Hedlund I, HelmbyH, Carlson J, Jepson A, Twumasi P, Kwiatkowski D, Greenwood BM, Wahlgren M: Rosette formation in Plasmodium falciparum isolates and anti-rosette activity of sera from Gambians with cerebral or uncomplicated malaria. Am J Trop Med Hyg 46503, 1992 6. MacPherson GG, WarrellMJ, White NJ, Looareesuwan S, Warrell DA: Human cerebral malaria. A quantitative ultrastructural analysis of parasitized erythrocyte sequestration. Am J Pathol 119:385, 1985 7. Aikawa M, Iseki M, Barnwell JW, Taylor D, 00MM, Howard RJ: The pathology of human cerebral malaria. Am J Trop Med Hyg 43:30, 1990 (suppl) 8. Allison AC: Protection afforded by sickle-cell trait against subtertian malarial infection. Br Med J 1:290, 1954 9. Willcox M, Bjorkman A, Brohult J, Pehrson P-0, Rombo L, Bengtsson E: A case-control study in northern Liberia of Plasmodiumfalciparum malaria in haemoglobin S and P-thalassaemia traits. Ann Trop Med Parasitol 77:239, 1983 IO. Yates SNR, Snow R, Allsopp CEM, Newton CRJC, Anstey N, Kwiatkowski D, Palmer D. Peschu N, Greenwood BM, Marsh K, Newbold CI, Hill AVS: a-thalassemia and malaria: Case-control studies in East and West Africa. Proceedings of the British Society for Parasitology 5th Malaria Meeting. Oxford, 1993 (abstr) I I . Hill AVS, Allsopp CEM, Kwiatkowski D, Anstey NM, Twumasi P, Rowe PA, Bennett S, Brewster D, McMichael AJ, Greenwood BM: Common West African HLA antigens are associated with protection from severe malaria. Nature 352:595, 1991 12. HillAVS: Malarial resistance genes: A natural selection. Trans Roy Soc Trop Med Hyg 86:225, 1992 13. Luzzatto L, Nwachuku-Janet ES, Reddy S: Increased sickling of parasitised erythrocytes as mechanism of resistance against malaria in the sickle-cell trait. Lancet 1:319, 1970 14. Pasvol G, Weatherall DJ, Wilson RJM: Cellular mechanism for the protective effect of haemoglobin S against P. falciparum malaria. Nature 274:701, 1978 15.FriedmanMJ: Erythrocytic mechanism of sickle cell resistance to malaria. Proc Natl Acad Sci USA 75:1994, 1978 16. Luzzi GA, MerryAH, Newbold Cl, Marsh K, Pasvol G: Protection by a-thalassemia against P lasmodiumfalciparum malaria: Modified surface expression rather than impaired growth or cytoadherence. lmmunol Lett 30:233, 1991 17.Luzzi CA, Meny AH, Newbold Cl, Marsh K, Pasvol G, Weatherall DJ: Surface antigen expression on Plasmodium f a k i parum-infected erythrocytes is modified in a- and P-thalassemia. J Exp Med 173:785, 1991 18. Hidayat AA, Nalbandian RM, Sammons DW, Fleischman JA, Johnson TE: The diagnostic histopathologic features of ocular malaria. Ophthalmology 100:1183, 1993 19. KaulDK,Roth EF Jr, Nagel RL, Howard M,Handunnetti SM: Rosetting of Plasmodium fakiparum-infected red cells with uninfected red cells enhances vasooclusion in an ex vivo microvascular system. Blood 78:812, 1991 20. Wahlgren M, Femandez V, Scholander C, Carlson J: Rosetting. Parasitol Today 10:73, 1993 21. Howard RJ, Gilladoga AD: Molecular studies related to the pathogenesis of cerebral malaria. Blood 74:2603, 1989 CARLSON ET AL 22. Trager W, Jensen JB: Human malaria parasites in continuous culture. Science 193:673, 1976 23. Carlson J. Holmquist G, Taylor DW, Perlmann P, Wahlgren M: Antibodies to a histidine rich protein (PMRPl) disrupt spontaneously formed Plasmodium falciparum erythrocyte rosettes. Proc Natl Acad Sci USA 87:2511, 1990 24. Carlson J, Wahlgren M: Plasmodium falciparum erythrocyte rosetting is mediated by promiscuous lectin-like interactions. J Exp Med 176:1311, 1992 25. Ellory JC, Nash GB, Stone PCW, Culliford SJ, Horwitz E, Stuart J: Mode of action and comparative efficacy of pharmacological agents that inhibit calcium-dependent dehydration of sickle cells. Br J Pharmacol 106:972, 1992 26. Nash GB, Johnson CS, Meiselman HJ: Rheologic impairment of sickle RBCs induced by repetitive cycles of deoxygenation-reoxygenation. Blood 72:539, 1988 27. Dacie JV, Lewis SM: Practical Haematology (ed 4). London, UK, Churchill, 1968, p 187 28. Nash GB, Cooke BM, Carlson J, Wahlgren M: Rheological properties of rosettes formed by red blood cells parasitised by Plasmodium falciparum. Br J Haematol 82:757, 1992 29. Carlson J, Nash GB, Gabutti V, Alpers M, Wahlgren M: Decreased rosetting ability confers protection against severe Plasmodiumfalciparum malaria. XIIIth International Congress for Tropical Medicine and Malaria. Jomtien, Pattaya, Thailand, 1992 (abstr) 30. Luzzi GA, Toni M, Aikawa M, Pasvol G: Unrestricted growth of Plasmodium falciparum in microcytic erythrocytes in iron deficiency and thalassemia. Br J Haematol 74:519, 1990 31. Udomsangpetch R, Sueblinvong T, Pattanapanyasat K, Dharmkrongat A, Kittlkalayawong A, Webster HK: Alteration in cytoadherence and rosetting of Plasmodium falciparum-infected thalassemic red blood cells. Blood 82:3752, 1993 32. Ahmad SH, Moonis R, Shahab T, Khan HM, Jilani T: Effect of nutritional status on totalparasite count in malaria. Indian J Pediatr 52285, l985 33. Oppenheimer SJ, Gibson FD, Macfarlane SB, Moody JB, Harrison C. Spencer A. Bunari 0: Iron supplementation increases prevalence and effects of malaria: Report on clinical studies in Papua New Guinea. Trans Roy SOCTrop Med Hyg 80:603, 1986 34. Snow RW, Byass P, Shenton FC, Greenwood BM: The relationship between anthropometric measurements and measurements ofiron status and susceptibility to malaria in Gambian children. Trans Roy Soc Trop Med Hyg 85:584, 1991 35. Nash GB, Johnson CS, Meiselman HJ: Influence of oxygen tension on the viscoelastic behavior of red blood cells in sickle cell disease. Blood 67:l IO, 1986 36. Serjeant GR: Sickle Cell Disease (ed 2). Oxford, UK, Oxford University Press, 1992, p 415 37. Friedman MJ, Roth EF, NagelRL, Trager W: Plasmodium falciparum: Physiological interactions with the human sickle cell. Expl Parasitol 47:73, 1979 38. Nagel RL: Innate resistance to malaria: The intraerythrocytic cycle. Blood Cells 16:321, 1990 39. Nagel RL: Innate resistance to malaria: The intraerythrocytic cycle. Blood Cells 16:348, 1990 (reply to commentary) 40. Helmby H, Cavelier L, Pettersson U, Wahlgren M: Rosetting Plasmodium fakiparum-infected erythrocytes express unique antigens on their surface. Infect Immun 61:284, 1993 4 I . Serjeantson S, Bryson K, Amanto D, Babona D: Malaria and hereditary ovalocytosis. Hum Genet 37:161, 1977 42. Pasvol G, Weatherall DJ, Wilson RJM: Effects of foetal haemoglobin on susceptibility of red cells to Plasmodium falciparum. Nature 270: 171, 1977 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1994 84: 3909-3914 Natural protection against severe Plasmodium falciparum malaria due to impaired rosette formation J Carlson, GB Nash, V Gabutti, F al-Yaman and M Wahlgren Updated information and services can be found at: http://www.bloodjournal.org/content/84/11/3909.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.




© Copyright 2026