
Benefit highlights
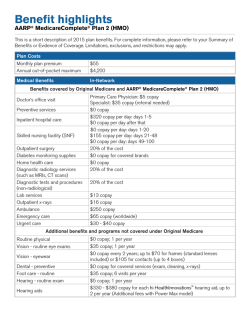
Benefit highlights AARP® MedicareComplete® Plan 1 (HMO) This is a short description of 2015 plan benefits. For complete information, please refer to your Summary of Benefits or Evidence of Coverage. Limitations, exclusions, and restrictions may apply. Plan Costs Monthly plan premium Annual out-of-pocket maximum $29 $5,500 Medical Benefits In-Network Benefits covered by Original Medicare and AARP® MedicareComplete® Plan 1 (HMO) Doctor’s office visit Preventive services Inpatient hospital care Skilled nursing facility (SNF) Outpatient surgery Diabetes monitoring supplies Home health care Diagnostic radiology services (such as MRIs, CT scans) Diagnostic tests and procedures (non-radiological) Lab services Outpatient x-rays Ambulance Emergency care Urgent care Primary Care Physician: $10 copay Specialist: $45 copay (referral needed) $0 copay $395 copay per day: days 1-4 $0 copay per day after that $0 copay per day: days 1-20 $155 copay per day: days 21-56 $0 copay per day: days 57-100 20% of the cost $0 copay for covered brands $0 copay 20% of the cost 20% of the cost $13 copay $16 copay $250 copay $65 copay (worldwide) $30 - $40 copay Additional benefits and programs not covered under Original Medicare Routine physical Vision - routine eye exams Vision - eyewear Foot care - routine Hearing - routine exam Hearing aids NurseLineSM $0 copay; 1 per year $45 copay; 1 per year $0 copay every 2 years; up to $70 for frames (standard lenses included) or $105 for contacts (up to 4 boxes) $45 copay; 6 visits per year $10 copay; 1 per year $330 - $380 copay for each hi HealthInnovations™ hearing aid, up to 2 per year (Additional fees with Power Max model) Speak with a registered nurse (RN) 24 hours a day, 7 days a week Prescription Drugs Your Cost Annual prescription deductible Initial coverage stage $0 Tier 1, Tier 2, and Tier 5; $180 for Tier 3 and Tier 4 Standard Retail Preferred Mail Order (30-day) (90-day) $2 copay $4 copay $8 copay $16 copay Tier 1: Preferred Generic Drugs Tier 2: Non-Preferred Generic Drugs Tier 3: Preferred Brand Drugs Tier 4: Non-Preferred Brand Drugs Tier 5: Specialty Tier Drugs Coverage gap stage Catastrophic coverage stage $45 copay $95 copay $125 copay $275 copay 33% of the cost 33% of the cost After your total drug costs reach $2,960, you will pay no more than 65% of the total cost for generic drugs or 45% of the total cost for brand name drugs, for any drug tier during the coverage gap After your total out-of-pocket costs reach $4,700, you will pay the greater of $2.65 copay for generic (including brand drugs treated as generic), $6.60 copay for all other drugs, or 5% of the cost Optional riders available – See the Summary of Benefits or Evidence of Coverage for information Plans are insured through UnitedHealthcare Insurance Company or one of its affiliated companies, a Medicare Advantage organization with a Medicare contract. Enrollment in the plan depends on the plan’s contract renewal with Medicare. Benefits, formulary, pharmacy network, provider network, premium and/or co-payments/co-insurance may change on January 1 of each year. The benefit information provided is a brief summary, not a complete description of benefits. For more information, contact the plan. You must continue to pay your Medicare Part B premium, if not otherwise paid for under Medicaid or by another third party. Limitations, copayments, and restrictions may apply. Y0066_MABH_FINAL_H1286002 ACCEPTED AAWA15HM3574838_000


© Copyright 2026