
Semiquantitative Analysis of Integrated Genomes of Human
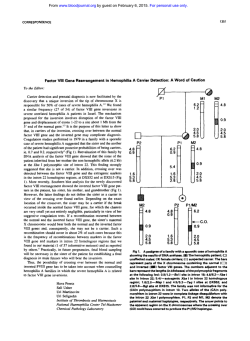
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Semiquantitative Analysis of Integrated Genomes of Human T-Lymphotropic Virus Type I in Asymptomatic Virus Carriers By Osamu Shinzato, Shuichi Ikeda, Saburo Momita, Yasuhiko Nagata, Shimeru Kamihira, Eiichi Nakayama, and Hiroshi Shiku A semiquantitative estimation of human T-lymphotropic virus type I (HTLV-I) integrationby peripheralblood mononuclear cells (PBMC) was performed. Genomic DNA samples derived from 134 HTLV-I carriers were subjected to 40 or 60 cycles of the polymerase chain reaction to amplify the pol region of HTLV-I. The HTLV-I genome was detected by dot hybridization using a UP-labeled oligonucleotide probe for the pol region. The radioactivity of hybridized dot membranes was then counted with an RI Imaging System (Ambis Inc, San Diego, CA) and the HTLV-I genome dose was determined by comparison with standard curve for serially diluted HTLV-I genome-positiveDNA. A wide range of variation of HTLV-I genome integration was observed. When the integrated genome dose was calculated as the number of HTLV-I copies per 100 PBMC, 7 carriers (5%) had more than 10 copies, 56 (42%) had 1 to 10 copies, 46 (34%) had 0.1 to 1 copy, and 24 (18%) had less than 0.1 copy. In one sample, the HTLV-I genome was undetectable, which may indicate that the integrated genome was present at less than 0.01 copies per 100 PBMC. Age- or sex-related variations in the distribution of individuals with different HTLV-I genome were rather limited. However, carriers with a high level of the HTLV-I genome were always more than 30 years old and were predominantlymale (six of seven). o 1991by The American Society of Hematology. H individual. Recently, the polymerase chain reaction (PCR) has been applied for detecting HTLV-I genomes?-” Although this technology enables us to detect the viral integration with extremely high sensitivity, quantitative measurement of the viral genome dose has remained difficult. In this study, we semiquantitatively examined HTLV-I genome dose in the PBMC of asymptomatic HTLV-I carriers by means of the PCR and the RI Imaging System (Ambis Inc, San Diego, CA). A more than 103-foldvariation in the viral genome dose was found among the HTLV-I carriers. The association of the viral genome dose with age was also examined. UMAN T-LYMPHOTROPIC virus type I (HTLV-I) was the first retrovirus to be found in humans’ and is intimately related to several disorders, including adult T-cell leukemia (ATL)’ and HTLV-I-associated myelopathyhropical spastic paraparesis (HAM/TSP).3a4 Seroepidemiologic analyses have shown the presence of at least three different routes of virus transmission: motherto-child transmission via breast feeding,’ transmission via blood transfusion: and husband-to-wife transmission via sexual interco~rse.~ HTLV-I primarily infects CD4+ T cells,’ and for its transmission infected cells need to come into direct contact with uninfected cells. However, it is totally unknown how the virus spreads in infected individuals and how viral infection eventually results in the onset of diseases. It is important to determine the fate of transmitted virions and the dose changes of the viral genome in infected individuals to analyze the pathogenesis of HTLV-I-related disorders and to determine effective methods for the prevention of infection. Infection with HTLV-I has usually been detected by serologic assays, such as immunofluorescence of serum and/or peripheral blood mononuclear cells (PBMC), or by Southern blot analysis of genomic DNA obtained from PBMC. However, these methods are unable to quantitatively measure the level of the viral genome in an infected From the Department of Oncology, Hematology, and Blood Transfusion Service, Nagasaki University School of Medicine, Nagasaki, Japan. Submitted July 2,1990; accepted June 11, 1991. Supported by Special Coordination Funds from the Science and Technology Agency of the Japanese Govemment and by a grant from the Ministry of Health and Welfare of Japan. Address reprint requests to Hiroshi Shiku, MD, Department of Oncology, Nagasaki University School of Medicine, 12-4 Sakamotomachi, Nagasaki 852 Japan. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section I734 solely to indicate this fact. 0 1991 by The American Society of Hematology. 0006-4971191 ~7808-0005$3.00/0 2082 MATERIALS AND METHODS Blood donors. One hundred thirty-four asymptomatic HTLV-I carriers in Nagasaki, one of the endemic areas for HTLV-I infection in Japan, were examined (Table 1).HTLV-I carrier status was determined by the presence of anti-HTLV-I antibodies detected by the gelatin particle agglutination test (Serodia-ATLA, Fujirebio, Tokyo, Japan), enzyme-linked immunosorbent assay (Eitest-ATL; Eisai Co,Tokyo, Japan), or indirect immunofluorescence with HTLV-I’ cells as the targets. Twenty-two patients with HAM/TSP and 23 healthy seronegatives (noncarriers) were also analyzed. Three HTLV-I+ cell lines (MT-2,” HUT-102,’ and ATKS) and fresh ATL cells were used as positive controls, whereas three HTLV-I- cell lines (HUT-78,” HL-60,14 and HLCL-1) were used as the negative controls. PCR. High molecular weight cellular DNA was extracted as described previously” from PBMC prepared by the Ficoll-Hypaque gradient method (Nyegaard, Oslo, Norway). DNA amplification in vitro was performed by the protocol of Saiki et with some modificati~n.’~.’~ Sequences of oligonucleotide primers and detecting probes are shown in Table 2. The reaction mixture contained 0.5 kg of chromosomal DNA, 0.3 kg of each primer, 800 kmol/L of dNTPs (mixture of dATP, dCTP, dGTP, and d’ITP) , 16.6 mmol1L (NH,),SO,, 67 mmol/L Tris-HC1 (pH 8.8), 6.7 mmol/L MgCI,, 10 mmol/L 2-mercaptoethanol, 100 pg/mL of gelatin, and 1U of Taq DNA polymerase (Perkin Elmer Cetus, Nonvalk, CT) in a total volume of 50 kL. Samples underwent 40 cycles of heating to 95°C for 60 seconds to denature the DNA, cooling to 55°C for 90 seconds for annealing of primers, and incubation at 72°C for 90 seconds for primer extension by an automated heat block (Program Temp Control System PC 500 Astec Inc, Fukuoka, Japan). Samples in which HTLV-I genomes Blood, Vol78, No 8 (October 15), 1991: pp 2082-2088 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2083 HTLV-I GENOME DOSES IN VIRUS CARRIERS Table 1. Age and Sex Distributionof HTLV-I Carriers Examined Male Age (vr) Female Age (vr) Range Median No. of Individuals Range Median No. of Individuals 10-19 20-29 30-39 40-49 50-59 60-69 70-79 10-18 20-29 31-39 42-48 50-58 60-67 70-77 17 26 36 44.5 53 64 72 9 10 10 10 10 9 6 16-19 20-27 30-38 40-49 50-59 60-67 72-79 17 26 36 44 53 63 74 11 10 10 10 10 11 8 Total 10-77 43.5 64 16-79 43 70 Age Groups (vr) were undetectable after 40 cycles of amplification were reanalyzed after another 20 cycles of the PCR were performed with the addition of 0.5 U of Taq DNA polymerase. Test samples were run in parallel with standard positive (mentioned later) and negative samples in each experiment. Dot hybridization. Aliquots (10 pL) of the reaction products were spotted onto nylon filters. The filters were dried and prehybridized for 3 to 6 hours at 56°C in 3 mol/L tetramethylammonium chloride, 50 mmol/L Tris-HC1 (pH 8.0), 2 mmol/L EDTA, 100 pg/mL of denatured salmon sperm DNA, 0.1% sodium dodecyl sulfate (SDS), and 5X Denhardt's solution. Then filters were hybridized for 1 hour at 46°C in the same mixture containing a 3zP-endlabeled oligoprobe. Filters were washed twice in 2X SSC (1X SSC: 150 mmol/L sodium chloride, 15 mmol/L sodium citrate) with 0.1% SDS for 5 minutes at room temperature, then stringently washed twice in 5X SSC with 0.1% SDS for 15 minutes at 50°C. Subsequently, filters were washed twice in the hybridization buffer without Denhardt's solution and salmon sperm DNA at 57.5"C for 1 hour. The filters were then exposed to Kodak XAR-5 film (Eastman Kodak, Rochester, NY) at -70°C for 15 to 24 hours using an intensifying screen. Analysis by the RI Imaging System. After dot hybridization, the radioactivity of each dot was counted for 5 to 8 hours using the RI Imaging System. The RI Imaging System images and quantitates with a degree of sensitivityequal to the combined use of autoradiography and scintillation counting. The detector is an enhanced multiwire proportional counter. An array of radiation detectors is created by 34 anode wires and 28 cathode strips that intersect at right angles to form 952 detectors. It detects radioactivity directly from samples without destruction of the sample membrane. The filter membrane analyzed by the RI Imaging System was also processed for standard autoradiography, as described previously. Standard samples. For quantitative analysis of the HTLV-I genome levels in PBMC, standard samples were prepared by diluting DNA from an ATL-derived cell line (ATKS), which has normal diploid 46XY chromosomes and one copy of the HTLV-I genome per cell. Tenfold serial dilutions (from 100% to 0.001%) of HTLV-I-positive cellular DNA, with a constant total DNA content, were prepared by dilution with DNA from HTLV-I- PBMC. Amplification of c-Ki-ras. As an internal control for the PCR, c-hi'-ras amplification was also examined in all samples, using the following primers and oligonucleotide probe: primer A ( 5 ' GACTGAATATAAACTTGTGG-3'),primer B (5'-CTATTGTTGGATCATATTCG-3'), and a '*P-labeled oligoprobe (5'GTTGGAGCTGGTGGCGTAGG-3'). Twenty-five cycles of the PCR were performed. After dot hybridization, each sample was analyzed by the RI Imaging System. Southern blot analysis. DNA samples were digested completely with Pst I restriction enzyme, separated on agarose gel, and transferred to a nitrocellulose filter. Hybridization was performed at 42°C with 1 X lo7cpm/mL of 32P-labeledprobe (P255M-07 for pol of HTLV-I) in 50% formamide, SX SSC, 0.02 mol/L sodium phosphate (pH 6.5), 1X Denhardt's solution, and 0.5 mg/mL of denatured salmon sperm DNA. Each filter was washed with 2X SSC-0.1% SDS and 0.1X SSC-0.1% SDS at 60°C and exposed to x-ray film. RESULTS Detection of the HTLV-I genome by the PCR. When genomic DNA obtained from 134 HTLV-I carriers was amplified by 40 PCR cycles with primers forpol region and then analyzed by dot hybridization, 119 samples showed a positive reaction and 15 samples were negative. After Table 2. Position and Sequence of Primers and Detecting Probes Region Oligonucleotide Primer A B Probe Primer A B Probe Primer A B Probe Primer A B Probe 'Sequence data from Seiki et a1?4 Position Seauence 15' + 3'P 3365-3384 3483-3464 3419-3438 1261-1280 1440-142 1 1380-1361 6116-6139 6236-6217 6196-6173 6834-6853 6929-6910 6877-6896 TACAAAGGCATACTGATCCC CAGGGTTTGGACTAGTCTAC AATCATTAGTGCAGCTGCGG AAGCAAGAAGTCTCCCAAGC TTCGGCCTCTGATATAAGGC GCAAAGGTACTGCAGGAGGT GCGGTACCGGTGGCGGTCTGGCTT CTITGTCCACCTCATGTAGG GGACATGGAGCCGGTAATCCCGCC ATGCTGTITCGCCTTCTCAG GAGAAGAAGGCCGCTGACGT CGGCGCTCCTGCTCITCCTG From www.bloodjournal.org by guest on February 6, 2015. For personal use only. SHINZATO ET AL 2084 amplification by a total of 60 cycles of the PCR, 14 of these 15 samples became positive and only one sample remained negative. All 14 samples that became positive only after 60 PCR cycles were then analyzed by Southern blot hybridization and disclosed specific 119-bpbands. When 23 samples obtained from noncarriers were similarly examined, no sample was positive after 40 or 60 PCR cycles. In all analyses, genomic DNA samples of HTLV-I' and HTLV-Icell lines were also included and provided the expected results. Semiquantitative analysis of the HTLV-I genome dose. Radioactivity of hybridized dot membranes was counted by the RI Imaging System. In each experiment, standard sampleswere also included to determine standard curves (a representative curve is shown in Fig 1). Figure 2 shows a representative result after 40 PCR cycles were used to treat 14 samples from HTLV-I carriers plus standard samples containing various amounts of HTLV-Igenome-positive cellular DNA (0.001% to 100%, lo-* 10-l lo0 lo' /I I I I I I I I I I I lo-' 100 lo' C1 C2 Blank S1 1 2 8 9 C 275 C3 S2 3 10 C4 S3 4 11 C5 C6 S4 S5 5 6 12 13 ................................................ I" C7 S6 7 14 D 00000.. 00 00 00000.0 E lo2 % of genomic DNA of HTLV-I positive cells /i B A lo2 % of genomic DNA of HTLV-I positive cells Flg 1. Ouantkattve analysis of HTLV-I genome doso In standard samples by PCR and dot hybridization. Standard samples were prepared by serially diluting genomic DNA obtainedfrom an HTLV-Ipositive cell line (ATKS), with DNA obtained from HTLV-l-negative PBMC. Samples containing 0.01% to 100% of HTLV-Lpositive genomic DNA were amplified by 40 PCR cycles with primers for the p o l region of HTLV-I. Autoradiography of dot hybridization was then performed (A). The counts per minute (cpm) value of each dot was measured using the RI Imaging System and a standard curve was drawn (B). Fig 2. An example of the analysis of HTLV-I genome dose in PBMC from carriers. (A) C1 and C2, HTLV-I seronegative individuals; C3, HL-60; C4, HUT-78; C5, MT-2; C6, fresh ATL cells; C7, HUT-102; Blank, sample buffer without genomic DNA; S1 through S6, standard samples containing HTLV-Lpositive genomic DNA in a range from 0.001% to 100%; 1 through 14, HTLV-I seroposkive individuals. Samples underwent 40 PCR cycles with primers for the pol region of HTLV-I (B through D) or 25 PCR cycles with primers for the c-Ki-res gene (E). A standard curve was drawn based on the cpm data for samples S1 through S6 as determined by the RI Imaging System (B). Autoradiography of dot hybridization using the pol region probe (C) or the c-Ki-res probe (E) was then performed. In (D),test samples have been classified into five groups accordingto the viral genome dose, as described in Results. (01,High; (01,moderately high; (0).moderately low; (0).low; (0).undetectable. Samplesfromcarriers 6 and 11were negative after 40 PCR cycles but became positive after 60 cycles, and were classified as low. ie, 0.001 to 100 copies of the HTLV-I genome per 100 cells). Positive dot hybridization was consistently obtained in samples with more than 0.1% HTLV-I genome positivity (equivalent to 0.1 copies of the genome per 100 cells). HTLV-I genome dose was determined using standard curves obtained from the serially diluted positive control samples, and the carriers' samples were classified into five groups depending on the genome dose. These groups were as follows: high, equivalent to more than 10 copies of the HTLV-I genome per 100 PBMC; moderately high, equivalent to 1to 10 copies; and moderately low, equivalent to 0.1 to 1 copy. Samples that were estimated to contain less than 0.1 copy of the HTLV-I genome per 100 PBMC were classified as low. After 60 PCR cycles, standard samples containing 0.01 copy of the HTLV-I genome per 100 PBMC became consistently positive in dot hybridization, and those containing 0.001 copy were occasionally positive. Therefore, samples that were negative after 40 PCR cycles but From www.bloodjournal.org by guest on February 6, 2015. For personal use only. HTLV-I GENOME DOSES IN VIRUS CARRIERS were positive after 60 cycles were also classified as low. A sample in which the HTLV-I genome was undetectable after 60 PCR cycles was classified as undetectable. All samples were examined at least three times. Whenever results were inconsistent, additional analyses were performed until repeatable results were obtained. To exclude the possibility that DNA preparations from particular samples could be inappropriate for the PCR, eg, due to contamination by enzyme inhibitors, each sample was also examined for c-Ki-ras gene expression. Consistent and uniform results were obtained for all samples, with a less than 20% standard deviation in cpm being detected (examples are shown in Fig 2). Analysis of the HTLV-I genome dose by the PCR for pol, pX, gag, and env regions. To determine the specificity of the PCR, 38 samples were analyzed in parallel forpol, pX, gag, and env regions of HTLV-I. Primers and detecting probes for each region are listed in Table 2. Thirty-five samples showed essentially similar results by the PCR for all four regions in terms of HTLV-I genome dose. One sample determined as moderately high genome dose by the PCR forpol became moderately low genome dose when the three other regions were examined. The remaining two samples determined as high genome dose by the PCR for pol, gag, andpX became either moderately low or undetectable genome dose by the PCR for env region. An example of comparative analysis is shown in Fig 3. In addition, selected samples were also analyzed by the standard Southern blot analysis. As shown in an example (Fig 4), expected bands were consistently detected by Southern blot analysis in samples with high genome dose and occasionally detected in samples with moderately high genome dose. Bands have never been detected in samples with lower genome doses. HTLV-I genome dose in HTLV-I carriers. In the PBMC of 134 asymptomatic HTLV-I carriers, we observed a wide range of variation of the integrated HTLV-I genome dose from more than 10 copies to less than 0.1 copy per 100 PBMC. Figure 5 shows the variations of HTLV-I genome dose with age in males and females. High genome dose was detected only in a limited number of carriers, who were predominantly males over 30 years old. Otherwise, no apparent differences in the proportion of carriers with different genome doses were observed among the various age groups. DISCUSSION The determinationof host viral genome dose is extremely important for understanding the pathogenesis of virally related diseases, but reliable estimation of the viral dose is a matter of considerable technical difficulty. Thus, in the case of HTLV-I, the probable causative agent of ATL and several other disorders including HAM/TSP, only limited information on host genome levels has been available. In this analysis we applied the PCR and the RI Imaging System to the determination of HTLV-I genome dose in viral carriers. Because HTLV-I is known to infect PBMC, particularly CD4' T cells, we analyzed PBMC genomic DNA. Thepol region was amplified by the PCR for detailed A Blanks1 S2 S3 S4 S5 S6 1 2 3 4 5 6 7 B Fig 3. An example of the analysis of HTLV-I genome doso by the PCR for pol. pX gag, and env regions. Standard samples IS1 through S6) contained HTLV-l-positive genomic DNA in a range from 0.001% to 100%, and are as follows: S1, 0.001%; S2, 0.01%; S3. 0.1%; S4. 1%; S5, 10%; S6, 100%. Seven samples of HTLV-I seropositive individuals (1 through 7) were also analyzed. Samples underwent 40 PCR cycles with primers for the listed regions. The sequence of primers and detecting probes is described in Table 2. Sample no. 2 became clearly positive by 60 PCR cycles in all regions examined. (A) Samples. (B) Dot hybridization. analysis of HTLV-I genome dose. Sufficient specificity and sensitivitywere obtained for the PCR and dot hybridization by using predetermined HTLV-I' and HTLV-I- cells as controls and also by using the c-Ki-ras gene as an internal control. The semiquantitative results obtained from each sample based on standard curves for HTLV-I' genome DNA were also found to be specific and sufficiently repeatable. However, in several samples semiquantitative estimation by the RI Imaging System was not consistent in repeated experiments. Therefore, we had to repeat experiments for these samples four to five times before we obtained conclusive results. The variations may have been caused at various steps of preparation of samples, PCR, and analysis by the RI Imaging System. Among 134 samples from HTLV-I carriers with anti- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. SHINZATO ET AL 2086 SlS2S3S4SSS6S7 1 2 3 4 5 6 2.5 kb Fig 4. Southem blot analysis for detection of HTLV-Igenome with "P-labeled probefor thepol region. Standard samples (S1 through S7) were prepared by serially diluting genomic DNA obtained from an HTLV-l-poskive cell line (ATKS), with DNA obtained from HTLV-l-negative PBMC. Concentratlonsof HTLV-Igenome in standard samples are as follows: S1,100%; S2,20%; S3,10%, S4,5%; S5,2%; S6,1%; S7,0.5%. The HTLV-I genome doses of six sampler from HTLV-I carriers (1 through 6) were predetermined by the RI Imaging System as follows: 1 and 2, high genome dose; 3 and 4. moderately high genome dose; 5 and 6, moderately low genome dose. DNA was digested by Pst 1. The presence of HTLV-I proviral genome was detected by =P-labeled DNA probe for the pol of HTLV-I. HTLV-I antibodies, only one sample failed to show any evidence of HTLV-I genome integration by amplification of all four regions of HTLV-I. In this sample, the HTLV-I genome was also undetectable by a standard Southern blot analysis. Presence and specificity of anti-HTLV-I antibodies in the serum of this carrier were confirmed by an absorption test of the enzyme-linked immunosorbent assay as well as by a Western blotting assay. This result could have been due to an extremely low level of the HTLV-I genome, an unusual location of the genome, or even the absence of genome in this particular individual. A wide variation of the HTLV-I genome dose (more than 10)-fold)was observed among these asymptomatic HTLV-I carriers. These HTLV-I genome doses may reflect a proportion of HTLV-I genome positive cells based on the assumption of one proviral copy per cell. Most of HTLV-I carriers Age Male Female % (1 1 )(1 O X 1 OXlO)(lO)(ll) (9) (6) 100 (8) I c U IC 5 .2 , In0 a 8 'f 50 zg c m .- z> -I g-l &% 10s 20s 30s 40s 50s 60s 70s Age 0 10s 20s 30s 40s 50s 60s 70s Age Fig 5. Distribution of the HTLV-I genome doso in the PBMC of carrier8 in different age groups. Viral genome dose was graded as follows: (m), high; (W), moderately high; (0). moderately low; (0).low; (0). undetectable. Numbers in parentheses denote the actual number of carriers examined. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2087 HTLV-I GENOME DOSES IN VIRUS CARRIERS were classified as having a moderately low or moderately high genome dose. Seventy-six percent (102 of 134) of the carriers had 0.1 to 10 HTLV-I genome copies in every 100 PBMC, while another 18% of the carriers (24 of 134) had less than 0.1 copy per 100 PBMC (low). Only seven carriers (5%) had more than 10 HTLV-I copies per 100 PBMC (high). Little age-related variation was observed in the proportion of individuals with low to moderately high HTLV-I genome dose. However, carriers with a high HTLV-I genome dose all were found to be more than 30 years old. This finding may suggest that the HTLV-I genome dose is largely determined shortly after viral transmission and does not change drastically afterwards, except in a rather limited number of individuals. Alternatively, a gradual increase of the HTLV-I genome dose after transmission may not have been detected in our study because of an increase of newly infected individuals among the older age groups. Sero-epidemiologic surveys in HTLV-I endemic areas have repeatedly shown that the rate of viral carriers, as determined by positivity for anti-HTLV-I antibody, apparently increases in parallel with aging.I9vmThis increase could be at least partly explained by the possibility of antibody response to a latent virus infection acquired early in life, as proposed by Blattner et a1.” Yoshida et alZZrecently reported that integration of HTLV-I was detectable in 29% of asymptomatic carriers by the standard Southern blot analysis, whereas it was detected in 82% of patients with HAM/TSP. These results suggest that the levels of integrated HTLV-I genomes are higher in HAM/TSP patients than in asymptomatic carriers. Gessain et al’ reported that 3% to 15% of the PBMC from HAM/TSP patients were infected by HTLV-I, after investigating 10 patients by dilution experiments using Southern blot hybridization assays. Although these analyses were performed in different populations and by different methods, it appears that HAM/TSP patients have a relatively high HTLV-I genome dose. In our preliminary analyses of 22 HAM/TSP patients, seven patients were determined as high genome dose, eight were moderately high genome dose, and the remaining seven were moderately low genome dose (data not shown). None were determined as low genome dose or undetectable genome dose. Our results are compatible with the previously mentioned reports and indicate an apparently higher level of HTLV-I genome dose in HAM/TSP patients. However, it has to be determined whether moderately high to high HTLV-I genome dose in asymptomatic virus carriers might be a risk factor for the development of HAM/TSP. The presence of the abnormally shaped nucleus lymphoid cells is more frequent in carriers with high or moderately high HTLV-I genome dose than in those with lower genome dose (data not shown). Cytologic similarity between these cells and ATL cells suggests that they may be polyclonally proliferating HTLV-I-positive cells. These cells are also frequently found in peripheral blood samples of HAM/TSP patients. Therefore, it has to be determined if the appearance of these cells is directly relevant to the development of ATL and/or HAM/TSP. ACKNOWLEDGMENT We thank Dr Yasuaki Yamada for providing the ATKS cell line, and Hiroto Okuda, Minoru Fujii, and Shigehiro Nakajima for supplying the carriers’ samples and technical assistance. We also thank Drs Ryozo Moriuchi and Tsutomu Miyamoto for providing us with the P255M-07 DNA probe for the pol region and some oligonucleotides for PCR. REFERENCES 1. Poiesz BJ, Ruscetti FW,Gazdar AF, Bunn PA, Minna JD, Gallo R C Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc Natl Acad Sci USA 77:7415,1980 2. Yoshida M, Miyoshi I, Hinuma Y: Isolation and characterization of retrovirus from cell lines of human adult T-cell leukemia and its implication in the disease. Proc Natl Acad Sci USA 79:2031, 1982 3. Osame M, Usuku K, Izumo S, Ijichi N, Amitani H, Igata A, Matsumoto M, Tara M: HTLV-I associated myelopathy: A new clinical entity. Lancet 1:1031,1986 4. Gessain A, Barin F, Vernant JC, Gout 0, Maws L, Calender A, de T h t G: Antibodies to human T-lymphotropic virus type-I in patients with tropical spastic paraparesis. Lancet 2:407, 1985 5. Nakano S, Ando Y, Ichijo M, Moriyama I, Saito S, Sugamura K, Hinuma Y: Search for possible routes of vertical and horizontal transmission of adult T-cell leukemia virus. Gann 75:1044,1984 6. Okochi K, Sato H, Hinuma Y: A retrospective study on transmission of adult T cell leukemia virus by blood transfusion: Seroconversion in recipients. Vox Sang 46:245,1984 7. Tajima K, Tominaga S, Suchi T, Kawagoe T, Komoda H, Hinuma Y, Oda T, Fujita K Epidemiological analysis of the distribution of antibody to adult T-cell leukemia-virus-associated antigen: Possible horizontal transmission of adult T-cell leukemia virus. Gann 73:893, 1982 8. Gotoh Y, Sugamura K, Hinuma Y: Healthy carriers of a human retrovirus, adult T-cell leukemia virus (ATLV): Demonstration by clonal culture of ATLV-carrying T-cells from peripheral blood. Proc Natl Acad Sci USA 79:4780, 1982 9. Duggan DB, Ehrlich GD, Davey FP, Kwok S, Sninsky J, Goldberg J, Baltrucki L, Poiesz BJ: HTLV-I-induced lymphoma mimicking Hodgkin’s disease. Diagnosis by polymerase chain reaction amplification of specific HTLV-I sequences in tumor DNA. Blood 71:1027,1988 10. Kwok S, Ehrlich G, Poiesz B, Kalish R, Sninsky JJ: Enzymatic amplification of HTLV-I viral sequences from peripheral blood mononuclear cells and infected tissues. Blood 7 2 1 117,1988 11. Abbott MA, Poiesz BJ, Byrne BC, Kwok S, Sninsky JJ, Ehrlich GD: Enzymaticgene amplification: Qualitative and quantitative methods for detecting proviral DNA amplified in vitro. J Infect Dis 158:1158,1988 12. Miyoshi I, Kubonishi I, Yoshimoto S, Akagi T, Ohtsuki Y, Shiraishi Y, Nagata K, Himuma Y: Type C virus particles in a cord T-cell line derived by co-cultivating normal human cord leukocytes and human leukemic T cells. Nature 294:770, 1981 13. Gazdar AF, Carney DN, Bunn PA, Russell EK, Jaffe ES, Schechter GP, Guccion JG: Mitogen requirements for the in vitro propagation of cutaneous T-cell lymphomas. Blood 55:409,1980 14. Collins SJ, Gallo RC, Gallagher RE: Continuous growth and From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2088 differentiation of human myeloid leukemic cells in suspension culture. Nature 270:347,1977 15. Maniatis T, Fritsch EF, Sambrook J (eds): Molecular Cloning: A Laboratory Manual. Cold Spring Harbor, NY, Cold Spring Harbor Laboratory, 1982 16. Saiki RK, Scharf S, Faloona F, Mullis KB, Horn GT, Erlich HA, Arnheim N Enzymatic amplification of f3-globin genomic sequences and restriction site analysis for diagnosis of sickle cell anemia. Science 230:1350,1985 17. Nagata Y, Abe M, Kobayashi K, Saiki S, Kotake T, Yoshikawa K, Ueda R, Nakayama E, Shiku H: Point mutations of c-ras genes in human bladder cancer and kidney cancer. Jpn J Cancer Res 81:22,1990 18. Nagata Y, Abe M, Kobayashi K, Yoshida K, Ishibashi T, Naoe T, Nakayama e,Shiku H: Glycine to aspartic acid mutations at codon 13 of the c-Ki-ras gene in human gastrointestinal cancers. Cancer Res 50480,1990 19. Hinuma Y, Komoda H, Chosa T, Kondo T, Kohakura M, Takenaka T, Kikuchi M, Ichimaru M, Yunoki K, Sato I, Matsuo R, Takiuchi Y, Uchino H, Hanaoka M: Antibodies to adult T-cell leukemia-virus-associated antigen (ATLA) in sera from patients with ATL and controls in Japan: A nation-wide sero-epidemiologic study. Int J Cancer 29:631,1982 SHINZATO ET AL 20. Clark J, Saxinger C, Gibbs WN, Lofters W, Lagranade L, Deceulaer K, Ensroth A, Guroff MR, Gallo RC, Blattner W A Seroepidemiologic studies of human T-cell leukemia/lymphoma virus type I in Jamaica. Int J Cancer 3637,1985 21. Blattner WA, Nomura A, Clark JW, Ho GYF, Nakao Y, Gallo R, Robert-Guroff M Modes of transmission and evidence for viral latency from studies of human T-cell lymphotrophic virus type I in Japanese migrant populations in Hawaii. Proc Natl Acad Sci USA 83:4895,1986 22. Yoshida M, Osame M, Kawai H, Toita M, Kuwasaki N, Nishida Y, Hiraki Y, Takahashi K, Nomura K, Sonoda S, Eiraku N, Ijichi S, Usuku K Increased replication of HTLV-I in HTLV-Iassociated myelopathy. Ann Neurol26:331,1989 23. Gessain A, Saal F, Gout 0, Daniel MT, Flandrin G, de Th6 G, Peries J, Sigaux F High human T-cell lymphotropic virus type I proviral DNA load with polyclonal integration in peripheral blood mononuclear cells of French West Indian, Guianese and African patients with tropical spastic paraparesis. Blood 75:428,1990 24. Seiki M, Hattori S, Hirayama Y, Yoshida M: Human adult T-cell leukemia virus: Complete nucleotide sequence of the provirus genome integrated in leukemia cell DNA. Proc Natl Acad Sci USA 803618,1983 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1991 78: 2082-2088 Semiquantitative analysis of integrated genomes of human T-lymphotropic virus type I in asymptomatic virus carriers O Shinzato, S Ikeda, S Momita, Y Nagata, S Kamihira, E Nakayama and H Shiku Updated information and services can be found at: http://www.bloodjournal.org/content/78/8/2082.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.





© Copyright 2026