
Download
NEWSLETTER JANUARY - FEBRUARY ESTRO | EUROPEAN SOCIETY FOR RADIOTHERAPY & ONCOLOGY SOCIETY LIFE The ESTRO vision on multidisciplinarity by the President NATIONAL SOCIETIES Relationship between ESTRO and the national societies: survey results ESTRO CONFERENCES 3rd ESTRO Forum: Topics, highlights and sessions not to be missed N° 98 | BIMONTHLY | JANUARY - FEBRUARY 2015 CONTENTS Editorial Society Life NEWSLETTER N° 98 JANUARY - FEBRUARY 2014 3 6 Clinical 10 Read it before your patients 16 Brachytherapy 30 Physics 40 RTT 54 Radiobiology 66 ESTRO School 83 Young ESTRO 104 Health Economics Institutional Membership 119 National Societies 123 ESTRO Conferences 128 Calendar of events 115 154 View of Barcelona, Spain, where the 3rd ESTRO FORUM will take place, 24-28 April 2015. ESTRO | EUROPEAN SOCIETY FOR RADIOTHERAPY & ONCOLOGY EDITORIAL “In the Society Life Corner you will be able to find an important note on multidisciplinary cancer care indicating ESTRO’s position on the topic. This is an important matter that affects all of us in our daily work” Dear friends and colleagues, I hope you all had a relaxing holiday season to finish 2014 happily, and that the year 2015 will be full of promise and plenty of opportunities for you to flourish. Just before the end of last year, we held an Extraordinary General Assembly at the ESTRO office on 16 December 2014. The outcome of the meeting can be read in the Society Life Corner. The Board will again present the material at the General Assembly at the 3rd ESTRO Forum in Barcelona on 27 April, for information for those who could not be present. The 3rd ESTRO Forum is now just a few months away and the busy work continues more than ever. I would like to thank all of you who submitted an abstract to the Forum as we have just hit a new record for our fora with an amazing 1,637 abstracts received, just slightly below the ESTRO 33 total of 1,737… not bad for such a young event! This record was reached through a generally high number of submissions, with a large increase in clinical abstracts. Congratulations, and especially to the RTTs for their highest ever total of 197 submitted abstracts. I would like to point out that a joint ALATRO, SEOR and SPRO national day will take place onsite, in the afternoon of 24 April. The agenda will focus on breast cancer and young radiation oncology professionals with Spanish and Portuguese as the scientific language. Work has also continued on the decisions taken at the June strategy review (JSR). We propose to adapt the structure of ESTRO to the changing environment. Three councils, focusing on scientific dissemination, stakeholder policy and education respectively, will be better suited to the modern needs of an international organisation like ESTRO. Another suggestion is that standing committees will no longer report to just one council; instead they will be active in their own right and approached by each council for their specific expertise. An indirect consequence of the work resulting from the JSR is that the young task force will become a standing committee, which will be launched officially at the 3rd ESTRO Forum. We will keep you informed of upcoming actions resulting from the JSR in subsequent newsletters. Finally, in the Society Life Corner you will be able to find an important note on multidisciplinary cancer care indicating ESTRO’s position on the topic. This is an important matter that affects all of us in our daily work. I wish you all a successful 2015 and hope to see you in the splendid city of Barcelona to experience and enjoy together the 3rd ESTRO Forum. Philip Poortmans ESTRO President CLINICAL & TRANSLATIONAL MEETING PHYSICS BIENNIAL MEETING 24 - 28 April 2015 Barcelona, Spain GEC - ESTRO - ISIORT MEETING PREVENT AND TARGET MEETING RTT MEETING WWW.ESTRO.ORG SOCIETY LIFE INTRODUCTION ESTRO WORKS WITH ECCO TO RESTORE BALANCE IN GAME OF THRONES IN EUROPE SOCIETY LIFE “The nature of multidisciplinary relationships within the European oncology landscape is changing” Dear friends and colleagues, The nature of multidisciplinary relationships within the European oncology landscape is changing. ESMO’s decision to end its collaboration with ECCO on the European Cancer Congress will have a big impact and raises serious questions about the future balance between all the different disciplines involved in caring for the cancer patient. To keep you informed of the latest developments and ESTRO’s views on this issue, I have included a brief description in this newsletter; we will update you whenever we have any further news. Our priority will always be to enable radiation oncology professionals to care for patients in the best possible way. PHILIP POORTMANS Philip Poortmans ESTRO President EXTRAORDINARY GENERAL ASSEMBLY The ESTRO Extraordinary General Assembly (EGA) took place on Tuesday 16 December 2014 at 18.30-19.00 hrs CET at the ESTRO office in Brussels. In accordance with the framework of good governance, the EGA was called to approve the budget for 2015 and to approve ESTRO’s choice of the external auditor. The EGA was quorate and both issues were voted on and approved. Members were invited to participate in the EGA either by being present at the ESTRO office or by joining using the teleconferencing system and INTRODUCTION voting using an electronic voting system (the same as that used for the last two Board members and President elections). The budget will be presented again at the General Assembly at the 3rd ESTRO Forum in Barcelona at the end of April, for information for those who could not be present. The full minutes of the Extraordinary General Assembly are available to all members upon request from the ESTRO office ([email protected]). ESTRO WORKS WITH ECCO TO RESTORE BALANCE IN GAME OF THRONES IN EUROPE SOCIETY LIFE ESTRO WORKS WITH ECCO TO RESTORE BALANCE IN GAME OF THRONES IN EUROPE PHILIP POORTMANS INTRODUCTION After a separation of two years, ESMO joined ECCO again in 2007. This followed a period of negotiations about money and about the reorganisation of the former European Federation of Cancer Societies (FECS). According to the contract, a period of ten years was agreed to rebrand this organisation with an agreement for joint congresses up to and including 2017. However, at the ESMO congress in Madrid, the board supported the ESMO president Rolf Stahel in his decision to stop the collaboration with ECCO for the organisation of the annual congresses after 2015. On the other hand, ESMO wants to stay in the part of ECCO (currently under reorganisation) that is related to relations with their stakeholders. Moreover, ESMO invited the other founding members of ECCO (ESSO, EACR, EONS, SIOPE, ESTRO) to contribute every two years to the annual ESMO congress, which will be an annual event from 2016 onwards. It goes without saying that the ESMO decision has a huge impact on multidisciplinary relationships in the European oncological landscape and puts great pressure on the viability of the ECCO congress because of the important relationship between the pharmaceutical companies and the medical oncologists. ESMO’s proposal for the other societies to join their congress cannot be accepted because it impacts heavily on the fairness of the, sometimes difficult, oncological equilibrium in Europe by overemphasising the central role of medical oncologists. This is especially disturbing as, with a high variation from one Eu- ropean country to another, medical oncologists prescribe only an estimated 30-40% of all cancer drugs in Europe and even more so as it is neglecting and even denigrating the contribution of the non-drug based oncological disciplines, including all related and supporting healthcare workers. The ESTRO Board decided to make an effort to take the opportunity created by ESMO and view it as a founding phase for the future of multidisciplinary cancer care. Therefore, we will support ECCO and its members in their quest to find a solution to the current challenge. We have started joint discussions and preparatory work to increase the speed at which ECCO undergoes its restructuring, opening itself completely to all healthcare workers that are active in the field of oncology so that they can participate at an equal level. The goal should be to support the best oncological cure and care for all patients, taking into account their personal, socio-cultural and spiritual circumstances. This should be, of course, in a fully multidisciplinary environment that respects the role of all those who contribute on an equal basis. I am sure that we will succeed in our goal to restore the balance in the game of thrones of oncology in Europe. Philip Poortmans ESTRO President ESTRO WORKS WITH ECCO TO RESTORE BALANCE IN GAME OF THRONES IN EUROPE 2015 ESTRO MEMBERSHIP Join ESTRO and benefit from services specially designed to support your career FULL Active Membership (95 EUR) Supporting Ambassador (250 EUR) ASSOCIATE In Training Membership (75 EUR) Affiliate (55 EUR) Corporate Representative (55 EUR) TAKE ADVANTAGE OF THE MANY BENEFITS THE ESTRO MEMBERSHIP HAS ON OFFER. THESE BENEFITS ARE IN RELATION TO THE LEVEL OF INVOLVEMENT WITHIN THE SOCIETY. Subscription to the Green Journal Reduced fees for attending ESTRO conferences, teaching courses and joint events Online access to scientific information through DOVE (events webcasts, delineation cases, etc.) Eligibility for grants, awards, working groups, faculties and governance positions And much more! INSTITUTIONAL MEMBERSHIP ESTRO offers European institutes the possibility to purchase several individual memberships in a batch (minimum of five) for their members. Not only is this very economical, but it also offers several other advantages. Please contact us at [email protected] For more information on the available package deals and to download the application forms: http://www.estro.org/members/institutional-membership/institutional-membership > 2015 MEMBERSHIP AVAILABLE ON WWW.ESTRO.ORG CLINICAL INTRODUCTION INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH CLINICAL “Data exchange becomes increasingly important for research in radiation oncology” Dear colleagues, Data exchange is becoming increasingly important for research in radiation oncology. There are many complexities, such as handling of dose plans, advanced imaging, large-scale bioinformation, high quality outcome parameters and, of course, legal issues. However, major research institutions in Europe and worldwide have identified this area as a priority area for future research because of its importance in generating evidence, as well as its use as a novel technology in radiation oncology. Below is a report from a multi-institutional workshop held in Dresden last year organised by OncoRay/ German Research Consortium for Translational research and EUROCAN. If you have comments or an interest in joining such an initiative, please let me know: [email protected] DANIEL ZIPS Daniel Zips Chair of the Clincal Committee INTRODUCTION INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH CLINICAL INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH MECHTHILD KRAUSE INTRODUCTION TOMAS SKRIPCAK This report summarises the fundamental ideas behind a new initiative for a data exchange strategy in radiotherapy, described in greater detail within a white paper (Radiother Oncol, epub). On 26 November 2013 a workshop organised by the German Cancer Consortium (DKTK) and EurocanPlatform was hosted in Dresden, Germany, to examine radiotherapy-research-specific IT platforms established within Europe. Current IT solutions from the European Society for Radiotherapy and Oncology (ESTRO) and several regional, national and international initiatives were presented. This workshop resulted in a conclusion, where all participating parties agreed on the necessity of setting up a collaborative effort to accelerate and harmonise ongoing data collection activities (via the utilisation of international, vendor neutral standards) and to promote open access to reusable radiotherapy research datasets. The main reason for rapid pooling of study data is an acceleration of translational research to speed up the application of healthcare innovations in the day-to-day treatment of cancer patients. The possibilities of reproducing the original study results, performing further analyses on existing research data to generate new hypotheses, or developing computational models to support Figure 1 Large-scale multi-centre studies produce raw data pools, which can be used to generate application-specific prediction models or knowledge bases (adapted from Skripcak et al., manuscript submitted) INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH medical decisions (e.g.risk/benefit analysis of treatment options) represent just a fraction of the potential benefits of medical data-pooling. Distributed machine learning and knowledge exchange from federated databases are among several attractive approaches for knowledge generation within “Big Data”. Resulting research data pools represent the primary input for the generation of medical knowledge bases (see Figure 1) with a broad range of applications, including predictive models for decision-support systems based on clinical data [1] and discovery of prognostic features in radiomics [2]. Predictive model research has the potential not only to improve quality of life but also to increase survival, for example by using isotoxic strategies [3]. The recent innovations in clinical data standardisation [4] together with the European Commission’s data protection reform in progress [5] suggest that now it is the ideal time to start analysing and establishing the necessary processes for multi-institutional data exchange. The newly formed initiative will trigger and harbour the activities that will lead to a formal definition of the radiotherapy-specific data exchange strategy, which is a fundamental prerequisite moving towards federated internationally interoperable research data sets. The initiative will include the following activities: • Establishing an international network of multidisciplinary professionals involved in the radiotherapy research field in order to establish INTRODUCTION collaboration in data exchange strategy requirements analysis, development and maintenance possibilities. • Communication with other existing initiatives to keep a track of recent developments and to try to harmonise their activities with each other. • Re-using, adopting or defining new guidelines for radiotherapy research data collection, including recommendations for the utilisation of clinical information models, ontologies, data elements and medical terminologies. • Analysing solutions for the protection of patient privacy and the relation to informed consent, as well as secondary use of research data in view of the very different interpretation and application of confidentiality and privacy rules and laws between different countries, different states within countries, and sometimes even between different ethical committees. • Providing sustainable open source IT solutions to support research data collection, analysis and transparent data and medical knowledge publication will make re-using research data straightforward and thus will stimulate research in radiation therapy and oncology. In future, the data pools might even be used for personalised medicine by means of generating predictions on outcome for individual patients based on analyses of their patient-tumour- and treatment-related data, which would facilitate treatment choice, either by physicians or through shared decision-making. Additionally, this initiative could be of great importance from a health economic perspective, by enabling evaluation of the efficacy and cost-benefit of different approaches, such as new technologies and/or new combined modality treatments. Mechthild Krause Radiation oncologist TU Dresden, Med. Faculty Carl Gustav Carus Dresden, Germany Tomas Skripcak IT scientist TU Dresden, Med. Faculty Carl Gustav Carus Dresden, Germany All of this will require the sincere commitment and engagement of involved professionals, but may result in great benefit to clinical as well as translational cancer research. When the first draft of the data exchange strategy is released, an international “dummy run” will be set up as a test case/prototype for evaluating its robustness. INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH REFERENCES 1. Lambin P, van Stiphout RGPM, Starmans MHW, Rios-Velazquez E, Nalbantov G, Aerts HJWL, et al. Predicting outcomes in radiation oncology – multifactorial decision support systems. Nature Reviews Clinical Oncology 2012;10:27–40. 2. Aerts HJWL, Velazquez ER, Leijenaar RTH, Parmar C, Grossmann P, Cavalho S, et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nature Communications 2014;5. 3. Reymen B, van Baardwijk A, Wanders R, Borger J, Dingemans A-MC, Bootsma G, et al. Long-term survival of stage T4N0-1 and single station IIIA-N2 NSCLC patients treated with definitive chemo-radiotherapy using individualised isotoxic accelerated radiotherapy (INDAR). Radiotherapy and Oncology 2014;110:482–7. 4. J. de Montjoie A. Introducing the CDISC Standards: New Efficiencies for Medical Research. CDISC; 2009. <http://www.cdisc.org>. 5. Data Protection Day 2014: Full Speed on EU Data Protection Reform. <http://europa.eu/rapid/press-release_MEMO-14-60_en.htm> INTRODUCTION INITIATIVE FOR CREATING A DATA EXCHANGE STRATEGY FOR RADIOTHERAPY RESEARCH DYNAMIC ONCOLOGY VIRTUAL ESTRO DOVE THE ESTRO PLATFORM FOR SCIENTIFIC AND EDUCATIONAL DATA DOVE is the e-library developed by ESTRO giving you access to educational and scientific material, produced and disseminated by the Society: the Green Journal articles, conference abstracts, webcasts, e-posters, slides, access to FALCON (our delineation tool), guidelines, our newsletter, etc. HOW DOES IT WORK? DOVE works as a search engine encompassing all kinds of data in radiation oncology. Just type in your key words and then refine your search by ticking the boxes if you are looking for a particular type of support (abstract, webcast, etc.). Or simply type a key word to see all the information available linked to the topic. HOW TO ACCESS DOVE? Simply go to www.estro.org: DOVE appears on the welcome page. The level of free access to the content you search will depend on your membership type. WWW.ESTRO.ORG READ IT BEFORE YOUR PATIENTS INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS Too important to miss... A digest of essential reading for all radiation oncologists PHILIPPE LAMBIN BY PHILIPPE LAMBIN, DIRK DE RUYSSCHER AND HANS KAANDERS DIRK DE RUYSSCHER HANS KAANDERS INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS BREAST Cognitive function after the initiation of adjuvant endocrine therapy in earlystage breast cancer: an observational cohort study. Ganz PA, Petersen L, Castellon SA, Bower JE, Silverman DH, Cole SW, Irwin MR, Belin TR. J Clin Oncol. 2014 Nov 1;32(31):3559-67. doi: 10.1200/ JCO.2014.56.1662. Epub 2014 Sep 29. PURPOSE This report examines cognitive complaints and neuropsychological (NP) testing outcomes in patients with early-stage breast cancer after the initiation of endocrine therapy (ET) to determine whether this therapy plays any role in posttreatment cognitive complaints. PATIENTS AND METHODS One hundred seventy-three participants from the Mind Body Study (MBS) observational cohort provided data from self-report questionnaires and NP testing obtained at enrolment (T1, before initiation of ET), and six months later (T2). Bivariate analyses compared demographic and treatment variables, cognitive complaints, depressive symptoms, quality of life, and NP functioning between those who received ET versus not. Multivariable linear regression models examined predictors of cognitive complaints at T2, including selected demographic variables, depressive symptoms, ET use, and other medical variables, along with NP domains that were identified in bivariate analyses. differences in NP test performance. Multivariable regression on LC at T2 found higher LC complaints significantly associated with T1 LC score (P < .001), ET at T2 (P = .004), interaction between ET and past hormone therapy (HT) (P < .001), and diminished improvement in NP psychomotor function (P = 0.05). Depressive symptoms were not significant (P = 0.10). CONCLUSION Higher LC complaints are significantly associated with ET six months after starting treatment and reflect diminished improvements in some NP tests. Past HT is a significant predictor of higher LC complaints after initiation of ET. RESULTS Seventy percent of the 173 MBS participants initiated ET, evenly distributed between tamoxifen or aromatase inhibitors. ET-treated participants reported significantly increased language and communication (LC) cognitive complaints at T2 (P = .003), but no significant INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS BREAST Circulating tumour cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. Jeffrey B. Smerage, William E. Barlow, Gabriel N. Hortobagyi, Eric P. Winer, Brian Leyland-Jones, Gordan Srkalovic, Sheela Tejwani, Anne F. Schott, Mark A. O’Rourke, Danika L. Lew, Gerald V. Doyle, Julie R. Gralow, Robert B. Livingston and Daniel F. Hayes. Presented in part as an oral presentation at the San Antonio Breast Cancer Symposium, San Antonio (USA), December 10-14, 2013. INTRODUCTION BREAST PURPOSE and 13 months, respectively (P < 0.001). Increased circulating tumour cells (CTCs; five or more CTCs per 7.5 mL of whole blood) are associated with poor prognosis in metastatic breast cancer (MBC). A randomised trial of patients with persistent increase in CTCs tested whether changing chemotherapy after one cycle of first-line chemotherapy would improve the primary outcome of overall survival (OS). PATIENTS AND METHODS CONCLUSION This study confirms the prognostic significance of CTCs in patients with MBC receiving firstline chemotherapy. For patients with persistently increased CTCs after 21 days of first-line chemotherapy, early switching to an alternate cytotoxic therapy was not effective in prolonging OS. For this population, there is a need for more effective treatment than standard chemotherapy. Patients with MBC who did not have increased CTCs at baseline remained on initial therapy until progression (arm A). Patients with initially increased CTCs that decreased after 21 days of therapy remained on initial therapy (arm B). Patients with persistently increased CTCs after 21 days of therapy were randomly assigned to continue initial therapy (arm C1) or change to an alternative chemotherapy (arm C2). RESULTS Of 595 eligible and evaluable patients, 276 (46%) did not have increased CTCs (arm A). Of those with initially increased CTCs, 31 (10%) were not retested, 165 were assigned to arm B, and 123 were randomly assigned to arm C1 or C2. No difference in median OS was observed between arm C1 and C2 (10.7 and 12.5 months, respectively; P = 0.98). CTCs were strongly prognostic. Median OS for arms A, B, and C (C1 and C2 combined) were 35 months, 23 months, PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS PROSTATE Vasectomy and risk of aggressive prostate cancer: a 24-year follow-up study. Siddiqui MM, Wilson KM, Epstein MM, Rider JR, Martin NE, Stampfer MJ, Giovannucci EL, Mucci LA. J Clin Oncol. 2014 Jul 7. pii: JCO.2013.54.8446. [Epub ahead of print] PURPOSE Conflicting reports remain regarding the association between vasectomy, a common form of male contraception in the United States, and prostate cancer risk. We examined prospectively this association with extended follow-up and an emphasis on advanced and lethal disease. PATIENTS AND METHODS Among 49,405 US men in the Health Professionals Follow-Up Study, age 40 to 75 years at baseline in 1986, 6,023 patients with prostate cancer were diagnosed during the follow-up to 2010, including 811 lethal cases. In total, 12,321 men (25%) had vasectomies. We used Cox proportional hazards models to estimate the relative risk (RR) and 95% CIs of total, advanced, high-grade, and lethal disease, with adjustment for a variety of possible confounders. disease. Additional analyses suggested that the associations were not driven by differences in sex hormone levels, sexually transmitted infections, or cancer treatment. CONCLUSION Our data support the hypothesis that vasectomy is associated with a modest increased incidence of lethal prostate cancer. The results do not appear to be due to detection bias, and confounding by infections or cancer treatment is unlikely. RESULTS Vasectomy was associated with a small increased risk of prostate cancer overall (RR, 1.10; 95% CI, 1.04 to 1.17). Risk was elevated for highgrade (Gleason score 8 to 10; RR, 1.22; 95% CI, 1.03 to 1.45) and lethal disease (death or distant metastasis; RR, 1.19; 95% CI, 1.00 to 1.43). Among a sub-cohort of men receiving regular prostate-specific antigen screening, the association with lethal cancer was stronger (RR, 1.56; 95% CI, 1.03 to 2.36). Vasectomy was not associated with the risk of low-grade or localised INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS PROSTATE Relationship between male pattern baldness and the risk of aggressive prostate cancer: an analysis of the prostate, lung, colorectal, and ovarian cancer screening trial. Zhou CK, Pfeiffer RM, Cleary SD, Hoffman HJ, Levine PH, Chu LW, Hsing AW, Cook MB. J Clin Oncol. 2014 Sep 15. pii: JCO.2014.55.4279. [Epub ahead of print] PURPOSE Male pattern baldness and prostate cancer appear to share common pathophysiologic mechanisms. However, results from previous studies that assess their relationship have been inconsistent. Therefore, we investigated the association of male pattern baldness at age 45 years with risks of overall and subtypes of prostate cancer in a large, prospective cohort – the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. METHODS We included 39,070 men from the usual care and screening arms of the trial cohort who had no cancer diagnosis (excluding non-melanoma skin cancer) at the start of follow-up and recalled their hair-loss patterns at age 45 years. Hazard ratios (HRs) and 95% CIs were estimated by using Cox proportional hazards regression models with age as the time metric. 0.97; 95% CI, 0.72 to 1.30) prostate cancer risk but was significantly associated with increased risk of aggressive prostate cancer (HR, 1.39; 95% CI, 1.07 to 1.80). Adjustment for covariates did not substantially alter these estimates. Other classes of baldness were not significantly associated with overall or subtypes of prostate cancer. CONCLUSION Our analysis indicates that frontal plus moderate vertex baldness at age 45 years is associated with an increased risk of aggressive prostate cancer and supports the possibility of common pathophysiologic mechanisms. RESULTS During follow-up (median, 2.78 years), 1,138 incident prostate cancer cases were diagnosed, 571 of which were aggressive (biopsy Gleason score ≥ 7, and/or clinical stage III or greater, and/ or fatal). Compared with no baldness, frontal plus moderate vertex baldness at age 45 years was not significantly associated with overall (HR, 1.19; 95% CI, 0.98 to 1.45) or non-aggressive (HR, INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS PROSTATE Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N, Vizziello D, Sun M, Karakiewicz PI, Menon M, Montorsi F, Briganti A. J Clin Oncol. 2014 Sep 22. pii: JCO.2013.54.7893. [Epub ahead of print] PURPOSE The role of adjuvant radiotherapy (aRT) in treating patients with pN1 prostate cancer is controversial. The authors tested the hypothesis that the impact of aRT on cancer-specific mortality (CSM) in these individuals is related to tumour characteristics. score 7 to 10, pT3b/pT4 stage, or positive surgical margins (HR, 0.30; P = .002); and (2) patients with PLN count of 3 to 4 (HR, 0.21; P = .02), regardless of other tumour characteristics. These results were confirmed when OM was examined as an end point. CONCLUSION METHODS A total of 1,107 patients with pN1 prostate cancer treated with radical prostatectomy and anatomically extended pelvic lymph node dissection between 1988 and 2010 at two tertiary care centres were evaluated. All patients received adjuvant hormonal therapy with or without aRT. Regression tree analysis stratified patients into risk groups on the basis of their tumour characteristics and the corresponding CSM rate. Cox regression analysis tested the relationship between aRT and CSM rate, as well as overall mortality (OM) rate in each risk group separately. The beneficial impact of aRT on survival in patients with pN1 prostate cancer is highly influenced by tumour characteristics. Men with low-volume nodal disease (≤ two PLNs) in the presence of intermediate- to high-grade, non-specimen-confined disease and those with intermediate-volume nodal disease (three to four PLNs) represent the ideal candidates for aRT after surgery. RESULTS Overall, 35% of patients received aRT. At multivariable analysis, aRT was associated with more favourable CSM rate (hazard ratio [HR], 0.37; P < .001). However, when patients were stratified into risk groups, only two groups of men benefited from aRT: (1) patients with positive lymph node (PLN) count ≤ 2, Gleason INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL Comment by Professor Dr Karin Haustermans, Department of Radiation Oncology, University Hospital Leuven, Belgium This paper by Abdollah and colleagues discusses the impact of adjuvant radiotherapy on the survival of patients with node positive prostate cancer. The authors evaluated 1,107 patients with pN1 prostate cancer who underwent a radical prostatectomy and extended lymph node dissection between 1988 and 2010 performed in two expert centres. All patients received hormonal treatment with or without adjuvant radiotherapy. Overall, 35% of the patients received adjuvant radiotherapy. Adjuvant radiotherapy was associated with an improved cancer specific survival. Patients with low volume nodal disease (not more than two pathological lymph nodes) and intermediate to high grade prostate cancer with positive section margins and patients with three to four pathological lymph nodes benefitted most. The authors validated their model by using the National Cancer Institute’s Surveillance, Epidemiology and End Results program (SEER) data set from 1999 to 2009, which consisted of 3,158 patients with node positive disease. With these data the authors confirm their previous findings on a smaller patient group. Moreover, they introduce further substratification for INTRODUCTION BREAST patients with more than two pathological lymph nodes. This study suffers from a few limitations. Firstly, it is a retrospective study and not a phase III randomised trial. Secondly, use of adjuvant radiotherapy was left to the clinical judgement of the treating physician, which might have introduced a selection bias. Thirdly, this study covers a long time period during which staging, surgery techniques and radiotherapy might have changed as well as the clinical judgement of the treating physicians. Fourthly, a pathology review was not performed. We know from previous studies that a central pathology review is important in this disease (van der Kwast et al., 2006). Although this study has some drawbacks, it also clearly demonstrates that prostate cancer patients with node positive disease are a heterogeneous group of patients with cancer specific survival at eight years varying between 72% and 99% and an overall survival of 78%, which is a very good result. Although patients treated with adjuvant radiotherapy had worse disease characteristics, adjuvant radiation did still improve outcome. These results do not come as a surprise. We know from three phase III randomised trials (Stephenson et al., 2012) that patients with pT3 pT4 pN0 prostate cancer benefit from adjuvant radiotherapy without adjuvant hormonal treatment. We also know from the Messing trial (Messing et al., 2006) that patients with pN1 disease benefit from PROSTATE HEAD AND NECK immediate hormonal treatment versus delayed hormonal treatment. Ideally, a randomised phase III trial should be performed. Carefully selected patients (and this paper could be used as a guidance) should be randomised after surgery between adjuvant hormonal treatment alone or adjuvant hormonal treatment with adjuvant radiotherapy. A large patient number would be required and surgeons would need to be trained in the technique of extended lymphadenectomy. Central pathology review and quality assurance of radiotherapy would be essential. Moreover, we have shown in our own studies that, with superextended lymphadenectomy, 13% affected nodes were found that would not have been detected with a classical extended lymphadenectomy (Joniau et al., 2013). Also, serial sectioning of all removed lymph nodes and the addition of cytokeratin staining led to the detection of 15% more positive lymph nodes compared to routine pathological examination with H&E staining (unpublished data). On top of this we have to face the fact that urologists remain reluctant to refer patients for adjuvant radiotherapy and prefer the “early salvage” approach. Given all these concerns, such a trial would have a high risk of failing. But let’s remain optimistic: there is a clear tendency today to be much more aggressive towards patients with highrisk disease, offering them a trimodality treatment. And the paper of Abdollah and colleagues provides strong evidence for this approach. OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS HEAD AND NECK Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. Cohen EE, Karrison TG, Kocherginsky M, Mueller J, Egan R, Huang CH, Brockstein BE, Agulnik MB, Mittal BB, Yunus F, Samant S, Raez LE, Mehra R, Kumar P, Ondrey F, Marchand P, Braegas B, Seiwert TY, Villaflor VM, Haraf DJ, Vokes EE. J Clin Oncol. 2014 Sep 1;32(25):2735-43. doi: 10.1200/ JCO.2013.54.6309. Epub 2014 Jul 21. PURPOSE Induction chemotherapy (IC) before radiotherapy lowers distant failure (DF) rates in locally advanced squamous cell carcinoma of the head and neck (SCCHN). The goal of this phase III trial was to determine whether IC before chemoradiotherapy (CRT) further improves survival compared with CRT alone in patients with N2 or N3 disease. PATIENTS AND METHODS Treatment-naive patients with non-metastatic N2 or N3 SCCHN were randomly assigned to CRT alone (CRT arm; docetaxel, fluorouracil, and hydroxyurea plus radiotherapy 0.15 Gy twice per day every other week) versus two 21-day cycles of IC (docetaxel 75 mg/m(2) on day 1, cisplatin 75 mg/m(2) on day 1, and fluorouracil 750 mg/m(2) on days 1 to 5) followed by the same CRT regimen (IC + CRT arm). The primary end point was overall survival (OS). Secondary end points included DF-free survival, failure pattern, and recurrence-free survival (RFS). more common in the IC arm (47% v 28%; P = .002). With a minimum follow-up of 30 months, there were no statistically significant differences in OS (hazard ratio, 0.91; 95% CI, 0.59 to 1.41), RFS, or DF-free survival. CONCLUSION IC did not translate into improved OS compared with CRT alone. However, the study was underpowered because it did not meet the planned accrual target, and OS was higher than predicted in both arms. IC cannot be recommended routinely in patients with N2 or N3 locally advanced SCCHN. RESULTS A total of 285 patients were randomly assigned. The most common grade 3 to 4 toxicities during IC were febrile neutropenia (11%) and mucositis (9%); during CRT (both arms combined), they were mucositis (49%), dermatitis (21%), and leukopenia (18%). Serious adverse events were INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS HEAD AND NECK p16 protein expression and human papillomavirus status as prognostic biomarkers of nonoropharyngeal headand neck squamous cell carcinoma. Chung CH, Zhang Q, Kong CS, Harris J, Fertig EJ, Harari PM, Wang D, Redmond KP, Shenouda G, Trotti A, Raben D, Gillison ML, Jordan RC, Le QT. J Clin Oncol. 2014 Sep 29. pii: JCO.2013.54.5228. [Epub ahead of print] INTRODUCTION BREAST PURPOSE Although p16 protein expression, a surrogate marker of oncogenic human papillomavirus (HPV) infection, is recognised as a prognostic marker in oropharyngeal squamous cell carcinoma (OPSCC), its prevalence and significance have not been well established in cancer of the oral cavity, hypopharynx, or larynx, collectively referred as non-OPSCC, where HPV infection is less common than in the oropharynx. PATIENTS AND METHODS p16 expression and high-risk HPV status in non-OPSCCs from RTOG 0129, 0234, and 0522 studies were determined by immunohistochemistry (IHC) and in situ hybridisation (ISH). Hazard ratios from Cox models were expressed as positive or negative, stratified by trial, and adjusted for clinical characteristics. and non-OPSCC, patients with p16-positive OPSCC have better PFS and OS than patients with p16-positive non-OPSCC, but patients with p16negative OPSCC and non-OPSCC have similar outcomes. CONCLUSION Similar to results in patients with OPSCC, patients with p16-negative non-OPSCC have worse outcomes than patients with p16-positive non-OPSCC, and HPV may also have a role in outcome in a subset of non-OPSCC. However, further development of a p16 IHC scoring system in non-OPSCC and improvement of HPV detection methods are warranted before broad application in the clinical setting. RESULTS p16 expression was positive in 14.1% (12 of 85), 24.2% (23 of 95), and 19.0% (27 of 142) and HPV ISH was positive in 6.5% (six of 93), 14.6% (15 of 103), and 6.9% (seven of 101) of non-OPSCCs from RTOG 0129, 0234, and 0522 studies, respectively. Hazard ratios for p16 expression were 0.63 (95% CI, 0.42 to 0.95; P = .03) and 0.56 (95% CI, 0.35 to 0.89; P = .01) for progression-free (PFS) and overall survival (OS), respectively. Comparing OPSCC PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS OESOPHAGUS Importance of surveillance and success of salvage strategies after definitive chemoradiation in patients with oesophageal cancer. Sudo K, Xiao L, Wadhwa R, Shiozaki H, Elimova E, Taketa T, Blum MA, Lee JH, Bhutani MS, Weston B, Ross WA, Komaki R, Rice DC, Swisher SG, Hofstetter WL, Maru DM, Skinner HD, Ajani JA. J Clin Oncol. 2014 Oct 20;32(30):3400-5. doi: 10.1200/ JCO.2014.56.7156. Epub 2014 Sep 15. INTRODUCTION BREAST PURPOSE Patients with oesophageal carcinoma (EC) who are treated with definitive chemoradiotherapy (bimodality therapy [BMT]) experience frequent relapses. In a large cohort, we assessed the timing, frequency, and types of relapses during an aggressive surveillance programme and the value of the salvage strategies. PATIENTS AND METHODS Patients with EC (N = 276) who received BMT were analysed. Patients who had surgery within six months of chemoradiotherapy were excluded to reduce bias. We focused on local relapse (LR) and distant metastases (DM) and the salvage treatment of patients with LR only. Standard statistical methods were applied. compared with those patients with LR only who were unable to undergo surgery (9.5 months; 95% CI, 7.8 to 13.3). CONCLUSION Unlike in patients undergoing trimodality therapy, for whom surveillance/salvage treatment plays a lesser role, in the BMT population approximately eight percent of all patients (or 36% of patients with LR only) with LRs occurring more than six months after chemoradiotherapy can undergo salvage treatment, and their survival is excellent. Our data support vigilant surveillance, at least in the first 24 months after chemotherapy, in these patients. RESULTS The median follow-up time was 54.3 months (95% CI, 48.4 to 62.4). First relapses included LR only in 23.2% (n = 64), DM with or without LR in 43.5% (n = 120), and no relapses in 33.3% (n = 92) of patients. Final relapses included no relapses in 33.3%, LR only in 14.5%, DM only in 15.9%, and DM plus LR in 36.2% of patients. Ninety-one percent of LRs occurred within two years and 98% occurred within three years of BMT. Twenty-three (36%) of 64 patients with LR only underwent salvage surgery, and their median overall survival was 58.6 months (95% CI, 28.8 to not reached) PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS LUNG Use of thoracic radiotherapy for extensive stage small-cell lung cancer: a phase III randomised controlled trial. Slotman BJ, van Tinteren H, Praag JO, Knegjens JL, El Sharouni SY, Hatton M, Keijser A, Faivre-Finn C, Senan S. Lancet Oncol. 2014 Sep 12. pii: S0140-6736(14)61085-0. doi: 10.1016/S0140-6736(14)61085-0. [Epub ahead of print] BACKGROUND Most patients with extensive stage small-cell lung cancer (ES-SCLC) who undergo chemotherapy, and prophylactic cranial irradiation, have persistent intrathoracic disease. The investigators assessed thoracic radiotherapy for treatment of this patient group. METHODS The investigators did this phase III randomised controlled trial at 42 hospitals: 16 in Netherlands, 22 in the UK, three in Norway, and one in Belgium. Patients were enrolled with WHO performance score 0-2 and confirmed ESSCLC who responded to chemotherapy. They were randomly assigned (1:1) to receive either thoracic radiotherapy (30 Gy in ten fractions) or no thoracic radiotherapy. All underwent prophylactic cranial irradiation. The primary endpoint was overall survival at one year in the intention-to-treat population. Secondary endpoints included progression-free survival. survival at one year was not significantly different between groups: 33% (95% CI 27-39) for the thoracic radiotherapy group versus 28% (95% CI 22-34) for the control group (hazard ratio [HR] 0.84, 95% CI 0.69-1.01; p=0.066). However, in a secondary analysis, two-year overall survival was 13% (95% CI 9-19) versus 3% (95% CI 2-8; p=0.004). Progression was less likely in the thoracic radiotherapy group than in the control group (HR 0.73, 95% CI 0.61-0.87; p=0.001). At six months, progression-free survival was 24% (95% CI 19-30) versus 7% (95% CI 4-11; p=0.001). We recorded no severe toxic effects. The most common grade 3 or higher toxic effects were fatigue (11 vs 9) and dyspnoea (three vs four). INTERPRETATION Thoracic radiotherapy in addition to prophylactic cranial irradiation should be considered for all patients with ES-SCLC who respond to chemotherapy. FINDINGS The investigators randomly assigned 498 patients between February 18, 2009, and December 21, 2012. Three withdrew informed consent, leaving 247 patients in the thoracic radiotherapy group and 248 in the control group. Mean interval between diagnosis and randomisation was 17 weeks. Median follow-up was 24 months. Overall INTRODUCTION BREAST PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL Comment by Professor Dr Ursula Nestle, University Hospital Freiburg, Germany Treatment of small cell lung cancer (SCLC) is still a mostly disappointing issue. In contrast to non-small cell lung cancer, where quite a lot of promising development on local and systemic treatment is going on, this disease is subject more to therapeutic nihilism than to good news. Beyond the backbone of – still improvable – systemic therapy, which is mandatory due to the tendency for early disseminated (ED) metastatic spread, current practice involves standard thoracic radiotherapy for patients with limited disease (LD) only. From this population we know about the positive effect of local treatment to the main tumour burden on local control and survival. For years, we have also been aware about the benefit of PCI on the incidence of brain metastases in both ED and LD responding after first line treatment. The Slotman study confirms again that - even with disseminated disease - in regions of high tumour burden, the addition of radiotherapy may help to overcome the deficits of systemic treatment. Until now, thoracic radiotherapy in ED-SCLC patients has been limited to patients needing INTRODUCTION BREAST palliative treatment or may have been given beyond current guidelines in individual cases with very limited metastatic spread, good performance status and excellent response. Therefore, due to the encouraging increase of the rate of long-time survival and despite the negative result with respect to the primary endpoint, this study will definitively be practice-changing. Also, the low rate of toxicity reported by Slotman et al. will encourage us to offer modern thoracic radiotherapy more often to patients with ED-SCLC with good performance status who respond after first line systemic treatment. Depending on more detailed analyses of these data, future studies with advanced radiotherapy techniques may investigate giving even higher doses of thoracic radiotherapy as compared to the 30 Gy in 10 fractions given by Slotman et al. factors predicting the benefit of such an approach (biomarkers? quality of staging? limited vs. disseminated metastatic spread? site of metastases?) and to ensure the intelligent inclusion of thoracic radiotherapy into future guidelines and clinical pathways for ED-SCLC. Yet the survival rates in SCLC are still disappointing and leave room for improvement. Therefore, in comparison to the oligometastatic approaches in other cancers, future studies on ED-SCLC should now include multimodal concepts combining – optimised – systemic treatment with more aggressive local treatments like thoracic radiotherapy and radiotherapy to a limited burden of distant metastases. Furthermore, it will be our task to identify other PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL READ IT BEFORE YOUR PATIENTS PURPOSE To provide the four-week prevalence estimates of mental disorders in cancer populations. PATIENTS AND METHODS PSYCHOSOCIAL Four-week prevalence of mental disorders in patients with cancer across major tumour entities. Mehnert A, Brähler E, Faller H, Härter M, Keller M, Schulz H, Wegscheider K, Weis J, Boehncke A, Hund B, Reuter K, Richard M, Sehner S,Sommerfeldt S, Szalai C, Wittchen HU, Koch U. J Clin Oncol. 2014 Nov 1;32(31):3540-6. doi: 10.1200/ JCO.2014.56.0086. Epub 2014 Oct 6. INTRODUCTION BREAST We enrolled adult patients with cancer from in- and outpatient care facilities, using a proportional stratified random sample based on the nationwide cancer incidence in Germany. Patients who scored nine or above on the Patient Health Questionnaire (PHQ-9) were administered to the standardised computerassisted Composite International Diagnostic Interview for mental disorders adapted for cancer patients (CIDI-O). A random sample of those with a PHQ-9 score that was less than nine were selected for a CIDI-O. dependence (0.3%; 95% CI, 0.1% to 0.6%), any mental disorder resulting from general medical condition (2.3%; 95% CI, 1.7% to 2.9%), and any eating disorder (0%). The highest prevalence for any mental disorder was found in patients with breast cancer (41.6%; 95% CI, 36.8% to 46.4%), followed by patients with head and neck cancer (40.8%; 95% CI, 28.5% to 53.0%). The lowest prevalence was found in patients with pancreatic cancer (20.3%; 95% CI, 8.9% to 31.6%) and stomach/oesophagus cancers (21.2%; 95% CI, 12.8% to 29.6%). CONCLUSION Our findings provide evidence for the strong need for psycho-oncological interventions. RESULTS A total of 5,889 patients were identified, which led to 4,020 participants (a 68.3% response rate); of those, 2,141 patients were interviewed. The four-week total prevalence for any mental disorder was 31.8% (95% CI, 29.8% to 33.8%); this included any anxiety disorder (11.5%; 95% CI, 10.2% to 12.9%), any adjustment disorder (11.1%; 95% CI, 9.7% to 12.4%), any mood disorder (6.5%; 95% CI, 5.5% to 7.5%), any somatoform/conversion disorder (5.3%; 95% CI, 4.3% to 6.2%), nicotine dependence (4.5%; 95% CI, 3.6% to 5.4%), alcohol abuse/ PROSTATE HEAD AND NECK OESOPHAGUS LUNG PSYCHOSOCIAL BRACHYTHERAPY INTRODUCTION EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 BRACHYTHERAPY “We look forward to sharing GEC-ESTRO brachytherapy activities with you in 2015” Welcome to the Brachytherapy Corner. We wish you a Happy New Year and look forward to sharing GEC-ESTRO brachytherapy activities with you in 2015. In this Corner you will find three reports on recent brachytherapy highlight papers. Read on to learn more about: • Vaginal morbidity after image-guided brachytherapy in cervix cancer • 3D dosimetry in low energy brachytherapy • Brachytherapy boosting in rectal cancer. You can also read about the activities of the GECESTRO head and neck working group, chaired by György Kovacs. And last but not the least, we invite you to take part in a competition for which there is a prize to win. See the end of this Corner. PETER HOSKIN BRADLEY PIETERS Peter Hoskin, Bradley Pieters and Kari Tanderup KARI TANDERUP GEC-ESTRO ASSEMBLY Sunday 26 April 2015 at the 3rd ESTRO Forum, Barcelona 13.30-14.30 INTRODUCTION EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS BRACHYTHERAPY Manifestation pattern of early-late vaginal morbidity after definitive radio(chemo)therapy and image guided adaptive brachytherapy for locally advanced cervical cancer – an analysis from the EMBRACE study Kathrin Kirchheiner Int J Radiat Oncol Biol Phys. 2014 May 1;89(1):88-95. Highlight Brachytherapy Papers Long-term results of a randomised trial in locally advanced rectal cancer: no benefit from adding a brachytherapy boost Ane Appelt Int J Radiat Oncol Biol Phys. 2014 Sep 1;90(1):110-8. doi: 10.1016/j. ijrobp.2014.05.023. Epub 2014 Jul 8. On the feasibility of polyurethane based 3D dosimeters with optical CT for dosimetric verification of low energy photon brachytherapy seeds Justus Adamson Med Phys. 2014 Jul;41(7):071705. doi: 10.1118/1.4883779. INTRODUCTION EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS BRACHYTHERAPY MANIFESTATION PATTERN OF EARLYLATE VAGINAL MORBIDITY AFTER DEFINITIVE RADIO(CHEMO)THERAPY AND IMAGE GUIDED ADAPTIVE BRACHYTHERAPY FOR LOCALLY ADVANCED CERVICAL CANCER – AN ANALYSIS FROM THE EMBRACE STUDY. Kirchheiner K, Nout RA, Tanderup K, Lindegaard JC, Westerveld H, Haie-Meder C, Petrič P, Mahantshetty U, Dörr W, Pötter R. Int J Radiat Oncol Biol Phys. 2014 May 1;89(1):88-95. Corresponding author: Kathrin Kirchheiner Department of Radiation Oncology Medical University of Vienna, Vienna, Austria [email protected] Highlight Brachytherapy Papers WHAT WAS YOUR MOTIVATION FOR INITIATING THIS STUDY? Brachytherapy in the treatment of locally advanced cervical cancer has changed substantially due to the introduction of combined intracavitary/ interstial applicators and an adaptive target concept, which is the focus of the prospective, multi-institutional EMBRACE (European study on MRI-guided brachytherapy in locally advanced cervical cancer) study (www.embracestudy.dk) on image-guided adaptive brachytherapy (IGABT). This new target concept has improved local control substantially and also significantly impacts on the dose to some organs at risk. Especially for the vagina, the dose can vary, with some patients receiving much less dose to the vagina and some receiving considerably more. However, the information on the clinical consequences of these doses in the vagina, and the impact on the patient’s quality of life, is very limited. Therefore, the motivation for this EMBRACE report was to evaluate as a first step the ways in which vaginal morbidity manifests itself during the first two years of follow-up. WHAT WERE THE MAIN CHALLENGES DURING THE WORK? KATHRIN KIRCHHEINER INTRODUCTION The main challenge of this work was to report the vaginal morbidity in a comprehensive way, that EDITORS’ PICKS gives insight into individual vaginal symptoms with regard to their contribution to the overall vaginal morbidity and to the manifestation pattern of symptoms over time in a large, multi-institutional patient cohort. Therefore, crude incidence rates, actuarial probabilities and prevalence rates were analysed in 588 patients with a median follow-up of 15 months and information on vaginal morbidity. Vaginal morbidity was prospectively assessed at baseline, every three months during the first year and every six months in the second year according to CTCAE v3.0 regarding vaginal stenosis, dryness, mucositis, bleeding, fistula and other symptoms. WHAT ARE THE MOST IMPORTANT FINDINGS OF YOUR STUDY? Two years after treatment, there was a low actuarial probability of developing any serious vaginal side effects (G3 and G4: 3.6%), but a high probability of having any G≥1 vaginal morbidity (89%), of which the majority occurred already within the first six months after treatment. Vaginal stenosis was most frequent, with the highest actuarial probability rates both for G≥1 (75%) and for G≥2 (22%), followed by vaginal dryness GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS Highlight Brachytherapy Papers (G≥1: 62% and G≥2: 8%). Both the prevalence rates of vaginal stenosis and dryness increased during follow-up. In contrast, vaginal bleeding decreased substantially after treatment and, together with mucositis, remained stable at low levels during follow-up. WHAT ARE THE IMPLICATIONS OF THIS RESEARCH? gradually increase or stabilise over time. Nevertheless, quality of life studies have shown that mild and moderate vaginal symptoms and associated sexual dysfunction can cause long-term distress in cervical cancer survivors. Therefore, future research on dose adaption and optimisation is necessary to establish a highly individualised and tailored treatment. Severe G3/G4 vaginal morbidity following definitive radio(chemo)therapy including IGABT for locally advanced cervical cancer within two years is limited and significantly less than in previous studies with radiographic treatment planning. Thus, the new adaptive target concept including the use of intracavitary/interstitial techniques seems to be a safe treatment with regard to major morbidity in the vagina being an organ at risk. However, mild to moderate morbidity occurs in the majority of patients within the first two years after the end of treatment and is still a substantial problem, which deserves further attention. With additional follow-up in the present EMBRACE study, it is expected that the findings will be further substantiated and will provide more insight into the question whether the overall vaginal morbidity and/or the individual symptoms will INTRODUCTION EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS BRACHYTHERAPY ON THE FEASIBILITY OF POLYURETHANE BASED 3D DOSIMETERS WITH OPTICAL CT FOR DOSIMETRIC VERIFICATION OF LOW ENERGY PHOTON BRACHYTHERAPY SEEDS. Adamson J, Yang Y, Juang T, Chisholm K, Rankine L, Adamovics J, Yin FF, Oldham M Med Phys. 2014 Jul;41(7):071705. doi: 10.1118/1.4883779. Corresponding author: Justus Adamson Assistant Professor Department of Radiation Oncology Duke University Medical Center, USA [email protected] Highlight Brachytherapy Papers WHAT WAS YOUR MOTIVATION FOR INITIATING THIS STUDY? We had previously applied polyurethane based 3D dosimetry to some low energy applications (keV micro-irradiator) and to brachytherapy (Cs-137). The natural next step was to combine knowledge learned from these two for application to LDR brachytherapy sources. for these very low energy brachytherapy sources. That is surprising given their very low energy, and is encouraging for application in other challenging settings. Another advantage we found for 3D dosimetry about a symmetric source is that the dose falloff with distance from the source is partially offset by the increased number of sample points at distance. WHAT WERE THE MAIN CHALLENGES DURING THE WORK? WHAT ARE THE IMPLICATIONS OF THIS RESEARCH? Using the 3D dosimeter with the LDR sources requires a channel in the centre of the dosimeter to place the source. This causes a number of challenges including accurate machining of the channel, registration of the source within the channel, and dealing with potential artefacts created in the tomographic dose reconstruction due to the presence of the channel. I think the overall takeaway message is that 3D dosimetry technology is developing to the point where it can be applied in diverse settings now, including those for which dosimetry is difficult (low energy, low dose rate, high dose gradient). It can serve as a great complement to Monte Carlo simulations and point dose measurements. WHAT ARE THE MOST IMPORTANT FINDINGS OF YOUR STUDY? JUSTUS ADAMSON INTRODUCTION One of the most interesting things we found is that with some of the new polyurethane formulations there is potential to create a dosimeter that has the same attenuation characteristics as water EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS BRACHYTHERAPY LONG-TERM RESULTS OF A RANDOMISED TRIAL IN LOCALLY ADVANCED RECTAL CANCER: NO BENEFIT FROM ADDING A BRACHYTHERAPY BOOST. Appelt AL, Vogelius IR, Pløen J, Rafaelsen SR, Lindebjerg J, Havelund BM, Bentzen SM, Jakobsen A. Int J Radiat Oncol Biol Phys. 2014 Sep 1;90(1):110-8. doi: 10.1016/j.ijrobp.2014.05.023. Epub 2014 Jul 8. Corresponding author: Ane Appelt Department of Oncology, Vejle Hospital, Vejle, Denmark and Faculty of Health Sciences, University of Southern Denmark, Odense, Denmark [email protected] Highlight Brachytherapy Papers WHAT WAS YOUR MOTIVATION FOR INITIATING THIS STUDY? Locally advanced (T3-4) rectal cancer (LARC) is commonly treated with neoadjuvant (chemo-) radiotherapy, followed by total mesorectal excision. The role of radiation dose has not been well understood, and consequently this randomised phase III study was initiated to improve our knowledge of rectal cancer dose-response. A combination of brachytherapy and external beam radiotherapy was chosen: the extensive nodal targets in the pelvis require external beam irradiation, while brachytherapy allowed for localised tumour dose escalation. A promising phase II trial based on this concept had previously been conducted in our department. For the phase II trial, we tested whether the addition of a 2 x 5Gy endocavitary brachytherapy boost to preoperative long-course chemoradiotherapy (50.4 Gy plus UFT) would improve tumour response and patient outcome. We have previously reported on the primary trial endpoint, pathological complete response (pCR) at the time of surgery. The study was negative – the rate of pCR was similar in the two arms – but there was an increase in near-complete tumour regression amongst patients receiving ANE APPELT INTRODUCTION EDITORS’ PICKS brachytherapy boost, especially in T3 tumours. Tumour regression has been shown to correlate with late outcome, so this was encouraging. However, tumour regression has not been confirmed as a valid surrogate endpoint for LARC, so for the present publication we wanted to assess disease control and survival. WHAT WERE THE MAIN CHALLENGES DURING THE WORK? The trial was initiated in our tertiary cancer centre, and all patients (except a small group in Canada) received neoadjuvant therapy here. Patients were subsequently re-referred to surgical departments all over Denmark and followed there after treatment completion. This setup complicated data collection, and two aspects proved particularly challenging: recording of local recurrences and scoring of late toxicity. Neoadjuvant chemoradiotherapy for LARC has only been shown to prevent local recurrences, not improve overall survival, so a major point of interest was the rate of locoregional failure. The trial protocol did not provide a detailed definition of locoregional recurrence, and some pelvic recurrences occurring secondary to distant metastatic disease were not biopsy confirmed. We GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 EDITORS’ PICKS Highlight Brachytherapy Papers reviewed patient records (and archived imaging when necessary) for all recurrences, to ensure consistent classification of locoregional failures. This was obviously a time-consuming task. with external beam radiotherapy alone – to treatment responders, but those patients apparently did not do better in the long run. Despite follow-up visits generally conducted as per protocol, the majority of patients were not evaluated for late radiotherapy side effects as planned; thus we were unable to collect reliable late toxicity data. However, our group is currently planning a quality-of-life study, including patient-reported outcome, among disease-free survivors. WHAT ARE THE IMPLICATIONS OF THIS RESEARCH? WHAT ARE THE MOST IMPORTANT FINDINGS OF YOUR STUDY? We found no difference in five-year overall survival (70.6% vs 63.6%) or progression-free survival (63.9% vs 52.0%) in the standard compared to the boost arm for the 221 patients analysed. Freedom from locoregional failure was borderline worse in the control arm (93.9% vs 85.7%). More detailed data analysis indicated the presence of “response migration”: the brachytherapy boost seemed to convert some patients – who would not have had major tumour regression INTRODUCTION Despite increased tumour regression at the time of surgery, we observed no benefit on late clinical outcome, and possibly an adverse effect on local control. Consequently, dose escalation using a brachytherapy boost for preoperative treatment of LARC cannot be recommended based on the findings of this trial. The role of brachytherapy for other patient groups, such as patients with early rectal cancer treated with definite chemoradiotherapy or patients treated with palliative intent, remains open. Moreover, improved tumour regression does not necessarily lead to a relevant clinical benefit when the neoadjuvant treatment is followed by high quality surgery. Tumour regression score is a well-established prognostic factor, but we did not find it to be a useful surrogate endpoint. EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 BRACHYTHERAPY In the past year the GEC-ESTRO ENT working group (ENT-GEC WG) focused on the following activities: 1. ENT COBRA PROJECT GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 By György Kovács, coordinator The project represents a retrospective and later prospective registry data pool between experienced centres in order to perform effective data mining and acquire evidence for the advantages and disadvantages of head and neck brachytherapy. There is a particular focus on oropharynx/oral cavity tumours as well as recurrences following previous radiotherapy. The participating groups agreed previously to a time schedule proposal as well as to the participation rules. Information on the set-up status of the project was given at the first GEC-ESTRO workshop in Brussels. In the past year we finished all preparations according to the planned timeline. Now a dummy run of the web-based data transfer is running to prove the software changes according to sharpened EU data transfer guidelines. Luca Tagliaferri, from the Catholic University in Rome, presented a report on the details at the second GEC-ESTRO workshop in Brussels on 4 December 2014. 2. INTERDISCIPLINARY ENT BRACHYTHERAPY TEACHING COURSE A couple of years ago we started a course series of interdisciplinary teaching in ENT brachytherapy at the Kiel, and later at the Lübeck UniverGYÖRGY KOVÁCS INTRODUCTION EDITORS’ PICKS sity in Germany. The last edition of this ESTRO endorsed course was held 27-30 November 2014 at the Catholic University in Rome, Italy. An announcement, including the course flyer with the final programme, is at http://www.brachiterapiaitalia.it/ENTcourse/ENT_course/Home.html; it is also posted on the ESTRO homepage and on the educational site of the home page of ELEKTA´s BrachyAcademy (https://www.brachyacademy. com/?s=ENT+teaching+course). The teaching staff include members of the GEC-ESTRO ENT working group (from Europe and India), as well members of ENT surgical societies. As a new topic in the teaching programme, a separate session focussing on findings of molecular biology and their influence on patient selection for different kinds of treatments was included. Due to the high degree of interest, it is also planned to offer the course more frequently than in the past. We plan to alternate the course between Europe and India, with the first course starting in India in 2015. There is agreement with the Tata Hospital experts in India that, in the future, they take care of the local organisation to cover the education needs in ENT brachytherapy and interdisciplinary cooperation of the region. A participant report is planned for one of the future newsletters. 3. UPDATE OF THE GEC- ESTRO HEAD AND NECK BRACHYTHERAPY RECOMMENDATIONS The ENT working group published the first issue of recommendations in 2009 in the Green GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 Journal (Mazeron et al. Radiother Oncol. 2009 May; 91(2):150-6. doi: 10.1016/j.radonc.2009.01.005. Epub 2009 Mar 28.). Since the time of the preparation of this paper, several developments in image guidance, interdisciplinary cooperation, as well hardware and software for head and neck brachytherapy technology has improved. Now, it is time to update the recommendations. Therefore, a writing group was organised on the ENT working group meeting in Brussels and a completed "ACROP Check-list" will be sent to ACROP (Advisory Committee on Radiation Oncology Practice) in order to perform the necessary formal registration of the future manuscript. 4. PUBLICATIONS BY ENT-BT WORKING MEMBERS IN 2013/2014 1. Chapter 18: ENT tumours. In: Strnad V, Pötter R, Kovács G (Eds) “Practical handbook of brachytherapy”. UNI-MED Verlag, Bremen-London-Boston, pp 166-183, 2014 2. Strnad V, Lotter M, Kreppner S, et al. “Re-irradiation with interstitial pulsed-dose-rate brachytherapy for unresectable recurrent head and neck carcinoma”, Brachytherapy 13(2):187195, 2014 3. Kovács G. “Modern head & neck brachytherapy: From radium towards intensity modulated interventional radiotherapy (IMBT)”, Journal of Contemporary Brachytherapy, in review, 2014 4. Takácsi-Nagy Z, Oberna F, Koltai P, et al. INTRODUCTION “Long-term outcomes with high-dose-rate brachytherapy for the management of base of tongue cancer”. Brachytherapy 12(6):535-541, 2013 5. Guinot J-L, Arriba L, Tortajada MI, et al. “From low-dose-rate to high-dose-rate brachytherapy in lip carcinoma: equivalent results but fewer complications”. Brachytherapy , 12:528-534, 2013 6. Teudt I, Meyer JE, Ritter M, et al. “Perioperative image-adapted brachytherapy for the treatment of paranasal sinus and nasal cavity malignancies”. Brachytherapy 13(2):178-186, 2013 The next formal meeting of the head and neck working group will be organised during the third GEC-ESTRO workshop in 2015, where all ENT-BT interested ESTRO members are cordially invited. In the meantime, for information/remarks related to the work or different working packages of the ENT working group or in other ENT brachytherapy-related issues, please contact the coordinator of the group ([email protected]). IRIDIUM 192 IMAGE COMPETITION GEC-ESTRO is looking for an appropriate image for the Iridium 192 award. At present the award carries the face of the awardee. This will now change to have a standard image appear on all awards. To this end, GEC-ESTRO is inviting all brachtherapy enthusiasts and creative minds to take part in a competition to decide on the best and appropriate image to be used. The image or design should capture the spirit of the Iridium 192 award. Interested? Please submit your proposal of an image to Evelyn at [email protected] Deadline for submission: 31 March 2015 The winner of the competition will be announced at the 3rd GEC-ESTRO workshop, 19 November 2015, and will receive €200.00 as prize. The Current Iridium award medal carries the face of the awardee EDITORS’ PICKS GEC-ESTRO HEAD AND NECK BRACHYTHERAPY WORKING GROUP REPORT 2014 PHYSICS INTRODUCTION PHYSICS MEMBERS SURVEY WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS Dear colleagues, PHYSICS First of all, we wish you the very best for 2015. This year we plan to work hard on making this Corner a success. “This year we plan to work hard on making this Corner a success” During the summer of 2014 the physics committee conducted a survey among the ESTRO physics members. The survey comprised questions on background information, ESTRO meetings, education, and other ESTRO physics activities. In this edition, Catharine Clark presents the results of this survey. MISCHA HOOGEMAN Emanuele Scifoni has written a comprehensive report on the workshop on Translational Research in Ion Beam Cancer (TRIBCT 2014). The report describes a very successful meeting, demonstrating the definite need for fundamental physics and biology research in the field of particle therapy. Finally, four editor’s picks, highlighting recent papers on a wide range of physics topics, make this winter edition very worthwhile reading. LUDVIG MUREN Mischa Hoogeman ([email protected]) Ludvig Muren ([email protected]), Frank Van den Heuvel ([email protected]), FRANK VAN DEN HEUVEL PHYSICS MEMBERS ASSEMBLY Saturday 25 April 2015 at the 3rd ESTRO Forum, Barcelona 13.30-14.30 INTRODUCTION PHYSICS MEMBERS SURVEY WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS PHYSICS ESTRO PHYSICS MEMBERS SURVEY CATHARINE CLARK INTRODUCTION During the summer of 2014 the physics committee (PC) conducted a survey of the physics members of ESTRO with the aim of better engaging with their needs and interests. This took the form of a Survey Monkey questionnaire with questions on background information, ESTRO meetings, education and other physics ESTRO activities. aspects were the teaching lectures (42%), followed by symposia (24%), proffered papers (17%) and debates (14%). Ninety-two percent go in person to look at the paper posters and 57% look at the e-posters, with 23% doing this at the meeting and 35% after they return home. The majority agree that the number of paper posters should be limited. Overall, 90% said that the A total of 708 responses were ‘Seventy percent did not realise that it balance between the different received (54% of physics is now possible to submit suggestions aspects of the meeting was apmembers) from 62 different to the physics committee for topics for propriate for their needs. countries (mainly in Europe, future meetings’ but all over the world); 48% The new format of having a were medical physics experts, 35% qualified medForum with a multi-disciplinary approach is ical physicists and 8% in training with 65% being popular with two thirds of respondents; howmale. Sixty percent work full time in radiotheraever, many acknowledged that this did come at py, with the rest having a range of duties, but prethe cost of some loss of visibility for the physics dominantly in imaging and protection. Sixty-two meeting. Seventy percent did not realise that it is percent spend more than 80% of their time in now possible to submit suggestions to the physics the clinic, while only five percent are in full time committee for topics for future meetings, so look research. out in your email inbox for information on how to do this. A third of members attend the annual ESTRO meeting each year, with a further third having Pre-meetings are popular and a third of memonly ever attended between one and three meetbers have already attended one or more. Many ings. The most important reasons for attending interesting suggestions were made for future a scientific meeting were to be updated on the pre-meetings, as well as for the topics within the latest scientific advances; however, 40% and 26% main meeting. The physics scientific advisory also cited continuing professional development committee will be looking carefully at these sugand networking as two of their main reasons for gestions to identify the best combinations for the attending. After this, presenting their own recoming years. search and visiting the technical exhibition were important. With regards to specifically attendAt the last two ESTRO meetings there has been a ing an ESTRO meeting, the top most important physics members assembly; however, 62% PHYSICS MEMBERS SURVEY WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS replied that they did not realise that this had happened. At the 3rd Forum in Barcelona, the physics members assembly will be held on Saturday 25 April from 13.30-14.30 hrs, so put it in your diary. Overall, the majority would like to hear a presentation of the PC activities as well as have the opportunity to have an open floor discussion of these activities at future physics meetings. This is your opportunity to have a face-to-face meeting with your representatives in ESTRO, so come along and make the most of it. However, if you cannot make it, then please contact us at the email address at the bottom of this report. ‘Two thirds of ESTRO physics members have attended an ESTRO course’ Figure 2 The choices of journal for submission of physics research work. Figure 1 The ESTRO courses which have been attended by physics members. INTRODUCTION PHYSICS MEMBERS SURVEY Two thirds of ESTRO physics members have attended an ESTRO course (see figure 1). The most popular is physics for clinical radiotherapy (38%), closely followed by IMRT and other conformal techniques in practice (35%), dose modelling and dose verification for external beam radiotherapy (29%) and basic clinical radiobiology (27%). There were also many suggestions given for future courses and the PC, with the education committee, is actively considering appropriate new courses. Some of the suggestions were for topics that already exist in the current courses, so it may be that not everyone is fully up-to-date with what is available. There is lots of information on the website for all the courses, including all the new developments (http://www.estro.org/school). WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS The Physics Corner in the newsletter is read by Following this survey the PC want to follow up 79% of members, although only 13% manage to actively on your suggestions and will be addressread all, 66% manage to read ing the lack of information on most or occasional issues. Of ‘The Physics Corner in the newsletter course content and the links is read by 79% of members’ the 12% who don’t read it, to the core curricula. We will 26% lack the time, but 68% be looking into new effective didn’t know it was here. The most useful sections communication channels and will hold a physics are the recent paper highlights (33%), the classic members’ assembly at the 3rd Forum in Barcemedical physics papers (28%) and the “back to lona with an open floor discussion so that we school” section (25%). can continue this conversation with you. In the meantime, if you wish to contact the PC about For information on daily practice the top four any of the issues addressed in this survey or any most popular journals are Medical Physics, Radiother ESTRO physics matter please contact physotherapy and Oncology, International Journal of [email protected]. Radiation Oncology Biology Physics, and Physics in Medicine and Biology. These are also the first choices for submission of work (see figure 2). Catharine Clark Physics committee member A new PC endeavour is to provide mentors to National Physical Laboratory help applicants contact centres for mobility grant Teddington, UK placements; 84% did not know this, so please remember that you have this opportunity if you want to apply for a mobility grant and you don’t know who to contact in the centre you’d like to go to. When asked how the PC could engage better with members, mailshots were the most popular suggestion, with a discussion forum on the ESTRO website also popular; however, only 20% thought that a Facebook page would work well for communication. INTRODUCTION PHYSICS MEMBERS SURVEY WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS PHYSICS WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY (TRIBCT 2014) Nanoscale physics meets particle therapy EMANUELE SCIFONI INTRODUCTION Translational research, interdisciplinary approach, multi-scale analysis: these phrases are often used (and abused) in recent research programmes. However, when it comes to particle therapy, also called ion beam therapy, it is very clear that fundamental physics, as well as chemistry and biology, on a wide range of physical scales and biological contexts should play an important role. But what can the nanoscale physicists, chemists and biologists learn from those working on improving and providing clinical radiotherapy protocols? And what promises can this type of research offer for improving the outcome of particle therapy? Is it indeed possible for useful communication to take place between experts on, say, molecular quantum dynamical modelling and clinical radiobiologists or medical physicists? This was one of the challenging questions to be met by the TRIBCT workshop (Translational Research in Ion Beam Cancer Therapy). The meeting took place from 30 September to 2 October 2014 in Aarhus, Denmark and was organised jointly by Aarhus University and Aarhus University Hospital [*]. The workshop was staged at the new university hospital site in Skejby and represents one of the final phases of a recent European Cooperation in Science and Technology (COST) action, nano-IBCT (nanoscale insights in ion beam cancer therapy - http://fias.uni-frankfurt.de/nano-ibct/ overview/). This COST action was dedicated to the detailed exploration of the mechanisms, from PHYSICS MEMBERS SURVEY nanoscale physics to chemical and radiobiological level, which underpin the ion therapy process. The action was originally motivated by a growing interest in the fundamental atomic and molecular physics community in the physics of ion beam therapy, where this interest was to a great extent stimulated by the discovery that low energy electrons can be very effective in the destruction of biomolecules [1]. For example, it was very clear that the energy spectra of secondary electrons, from heavy ion collisions at Bragg peak energies, are peaked at sub kiloelectronvolt (keV) energies, indeed typically as low as tens of electronvolts (eV) and thus in a region where low energy molecular and atomic physics plays an important role. The aim of the nano-ICBT programme was to provide a better understanding of the complex multi-scale scenario of radiation damage induced by ion beams. The ultimate goal was to allow a more informed and better control of the irradiation parameters in clinical treatment. Thus the potential outcome of nano-ICBT should be enhanced treatment programmes, fully exploiting the physical and radiobiological advantages of ion beams. The essential purpose of the TRIBCT meeting was to explore the path between clinical practice and fundamental research in proton and heavy ion therapy. The primary aim was that those performing basic physics, chemistry and biology research should be aided in their appreciation of the place of their work with respect to actual treatment and the relation that their results could have to clinical practice. An additional and related aim WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS followed, emphasising the special role of dosimetry. The problem of quenching of detectors under high LET (linear energy transfer) irradiation was pointed out. In connection with this, in his talk Niels Bassler presented something of a challenge to the nanoscale community. He underlined the analogy between the relative response of a dosimeter at different radiation qualities and the relative biological effectiveness (RBE), and then suggested a focus on the description of the quenching of a simple radiation detector, rather than struggling with complex cellular systems. This, he suggested, was the best way forward to elucidate the characteristics of high LET radiation and its associated radiobiology. The participants of the meeting at the Aarhus University Hospital, Skejby was to present new concepts and paradigms for ion beam-induced radiation damage, emerging from research at physical, chemical and biological levels, as always looking for clinical impact. The meeting was especially timely, since a proton therapy centre, the Danish Centre for Particle Therapy, is to be built in Aarhus by the Aarhus University Hospital, Aarhus University and the local Health Authority (opening 2018). The organisers of the meeting, lead by David Field for atomic and molecular physics and Kevin Prise, Niels Bassler, Jørgen Petersen and Cai Grau for the clinical-oriented research, crafted an excellent programme in a top-down fashion, start- INTRODUCTION ing from the very basic definition of the medical issues and progressing step by step towards the fundamental physics of IBCT. The first part of the meeting was in the form of a tutorial, where selected experts in the various disciplines of radiotherapy and oncology placed the clinical problem in the proper context. Following some basic talks on cancer radiotherapy from leading practitioners, Jan Alsner illustrated aspects at the cellular and molecular biology scale and Ludvig Muren and Per Poulsen overviewed modern medical radiation physics techniques, focusing on adaptive radiotherapy and motion management. A comprehensive talk by Claus Andersen then PHYSICS MEMBERS SURVEY The stage was then set for Jens Overgaard, who warned about the possible risks of models, even on a very macroscopic, phenomenological scale and stressed the importance of extending experimental campaigns for in vivo measurements. Immediately afterwards, Cai Grau showed how the evidence-based medicine requirements are still lacking in proton therapy, despite obvious demonstrations of success. It is evident that a great deal more clinical work is required to work out, on a purely observational basis, for example what is the optimal fractionation schedule and, further, to establish the answer to this fundamental clinical question for different types of cancer. Brita Sørensen then presented the latest results of the first follow-up of a large-scale in vivo experiment performed at GSI (Helmoholtz center for WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS Heavy Ion Research) in July; that is, the initial, normal tissue complication probability (NTCP) data for early effects with photon and carbon ions, extracting from them an RBE value. Kevin Prise went on to show, with his recent measurements, the importance of a correct radiobiological description all along a spread-out Bragg peak irradiation, contrasting this with the commonly used over-simplification to a constant RBE value. Michael Krämer showed how RBE is implemented in active scanned particle therapy, fully accounting for the mixed radiation field, through the treatment planning system TRiP98. He also mentioned recent studies using novel ion beams, such as helium, which presents potential specific indications for paediatric cases, or oxygen, whose high LET offers selective advantages for irradiation of hypoxic regions. For all these ion beams, Paola Maria Frallicciardi presented a novel monitoring technique based on simultaneous detection of prompt photons and secondary particle emission. This will be implemented, she reported, in the Italian National Centre of Hadrontherapy for Cancer Treatment (CNAO) beamline in Pavia. During the track simulation session, macroscopic radiation transport codes (FLUKA and SHIELDHIT) were presented as well as nanoscale 3D track structure models (PARTRAC, LEPTS, TRAX, EPOTRAN) and so called amorphous track models, in which the radial dose deposition along the track is considered (LEM). Christophe Champion showed the advances in quantum me- INTRODUCTION From left to right: Cai Grau, giving his tutorial lecture on cancer radiotherapy; Michael Krämer, discussing the biological effect based optimisation in treatment planning for particle therapy; Brita Singers Sørensen, stressing the importance of new in vitro/in vivo data for relative biological effectivess (RBE) assessment. (Pictures by Niels Bassler) chanical calculations of electron induced ionisation processes. These are basic input for radiation track structure simulations, as well as for positron transport, the nature of which has an important role in assessing the resolution of positron emission tomography (PET). Jorge Kohanoff described the ability of ab initio modelling to aid in understanding radiation damage mechanisms at the molecular level, specifically with reference to the breaking of bonds in DNA and other biomolecules. Andrey Solov’yov mentioned the role of shock waves generated in the medium by the passage of fast ions, resulting in sudden intense local heating in PHYSICS MEMBERS SURVEY the Bragg peak region, as a possible contribution to the overall damage. Pavel Kundrat showed the accurate description available in PARTRAC code of the physico-chemical and chemical stages involved in IBCT. PARTRAC allows the prediction of the nature and concentration of chemically-active species produced (radicals, solvated electrons) as a function of the LET of the incident particle. The studies introduced in this part of the meeting could provide important insights, for example, in modelling the oxygen enhancement ratio in IBCT. The hypoxia issue, “adored and ignored” [2], was identified as a major topic of research, WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS following a couple of instructive talks from Michael Horsman and Jens Overgaard. The need to consider the microenvironment as an additional parameter for the biological optimisation was quite evident. Particle therapy promises a valuable contribution in specifically targeting this issue, especially thanks to the high flexibility of the full active scanning dose delivery and through different approaches such as LET painting (Aarhus) and killing painting (GSI). In the final part of the meeting, dedicated to new insights, nanoparticle-aided therapy became one of the focus of discussion. Fred Currell showed a brilliant example of successful translational research in this topic, starting from a track structure analysis of the Auger electrons emitted in gold nanoparticles under photon irradiation, and reproducing the observed cell-killing enhancement. But, as he mentioned, while the use of metallic nanoparticles as radio-sensitisers with photon therapy has been suggested for more than a decade, it is not obvious if an additional sensitisation effect could be achieved in particle therapy as well. This is despite recent positive in vitro and in vivo results. In this connection the birth of a new Marie Curie international training network, ARGENT (Advanced radiotherapies generated by exploiting nanoprocesses and technologies http://itn-argent.eu/) has been announced, dedicated to the investigation of possible combination of ion beam irradiation with metallic nanoparticles. INTRODUCTION The poster session was also very stimulating, with several outstanding contributions. For example, Ivana Dokic presented a systematic in vitro analysis with the four ion beams available at HIT, Heidelberg Ion Therapy centre (protons, helium, carbon, oxygen), pointing out how in vitro research is still needed fully to characterise these “new” beams and fully to exploit their selective advantages. Over 40 delegates from all over the world participated in the conference, bringing together their view on the basic challenges in particle therapy and pointing out where research directions should be concentrated. The participant list included representatives from the facilities for active scanned carbon therapy, which are currently operating (CNAO and HIT), or completed the pilot project (GSI), as well as from the major European laboratories in the area of fundamental physics, chemistry and biology. The meeting was really successful, with many stimulating discussions, sometimes quite animated, both during the talks and the breaks, frequently among scientists who have never had the opportunity to interact before. In conclusion, it is clear that particle therapy is a growing reality that can offer a significant contribution to the palette of treatments in European radio-oncology and worldwide. It is clear that much research in many diverse topics is still needed to provide a solid evidence-based treatment, and to enhance the range of cancers that PHYSICS MEMBERS SURVEY can be treated [3]. The meeting underlined that fundamental research can definitely provide useful insights and suggest treatment enhancement, but the complexity of the field requires a close collaboration between radiation oncology professions, to design optimal clinical trials. TRIBCT 2014 then emphasised to those involved in basic physics, chemistry and biology the necessary spirit of caution with which promising experimental and theoretical results must be viewed in relation to cancer treatment [#]. We look forward to a TRIBCT 2015! Emanuele Scifoni Biophysics Department GSI Helmholtz centre for Heavy Ion Research, Darmstadt, Germany [email protected] REFERENCES * More information, Book of Abstract and references therein on http://tribct2014.au.dk/ 1. B. Boudaïffa et al., Science (2000) 287, 1658. 2. J. Overgaard, J. Clin. Oncol. (2007) 25, 4066. 3. J.S. Loeffler and M. Durante, Nature Rev. Clin. Oncol. (2013) 10, 411. # Thanks to David Field, Niels Bassler and Ludvig Muren for precious assistance in summarising this event. WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS EDITORS’ PICKS PHYSICS Highlight Radiotherapy Physics Papers Detector to detector corrections: a comprehensive experimental study of detector specific correction factors for beam output measurements for small radiotherapy beams Godfrey Azangwe Medical Physics 41, 072103 (16pp.) (2014), online: http://dx.doi. org/10.1118/1.4883795 Institutional patient-specific IMRT QA does not predict unacceptable plan delivery Stephen F. Kry International Journal of Radiation Oncology Biology Physics (in Press) INTRODUCTION PHYSICS MEMBERS SURVEY Proton range verification through prompt gamma-ray spectroscopy Joost Verburg Physics in Medicine and Biology 59 (2014) 7089–7106 Direct use of multivariable normal tissue complication probability models in treatment plan optimisation for individualised head and neck cancer radiotherapy produces clinically acceptable treatment plans Roel G.J. Kierkels Radiotherapy & Oncology, in press accepted September 2014 WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS EDITORS’ PICKS Highlight Radiotherapy Physics Papers PHYSICS DETECTOR TO DETECTOR CORRECTIONS: A COMPREHENSIVE EXPERIMENTAL STUDY OF DETECTOR SPECIFIC CORRECTION FACTORS FOR BEAM OUTPUT MEASUREMENTS FOR SMALL RADIOTHERAPY BEAMS Godfrey Azangwe, Paulina Grochowska, Dietmar Georg, Joanna Izewska, Johannes Hopfgartner, Wolfgang Lechner, Claus E. Andersen, Anders R. Beierholm, Jakob Helt-Hansen, Hideyuki Mizuno, Akifumi Fukumura, Kaori Yajima, Clare Gouldstone, Peter Sharpe, Ahmed Meghzifene, and Hugo Palmans. Medical Physics 41, 072103 (16pp.) (2014), online: http://dx.doi.org/10.1118/1.4883795 CORRESPONDING AUTHOR: Godfrey Azangwe National University of Science and Technology Bulawayo, Zimbabwe What was your motivation for initiating this study? The study provides a comprehensive set of detector-specific correction factors for dosimetry of small photon fields using a wide range of real time and passive detectors. The motivation for the study was the lack of data in this area, which has reportedly led to radiation accidents in the past. It also addresses the needs of a code of practice for small field photon beam dosimetry under development by an IAEA-AAPM working group to arrive at a dosimetry approach consistent with protocols for broad beam dosimetry such as the IAEA TRS 398 and AAPM TG 51. Such a link is critical as some high precision treatment units do not allow set up in reference conditions (i.e. 10 × 10 cm2 field size at a distance from the source of 100 cm). What where the challenges during the work? The study encountered the challenges of gathering a wide range of detectors (operated by different research groups) and of accurate positioning of detectors especially for the passive detectors in a solid phantom in the smallest field sizes. What is the most important finding of your study? The results from the study demonstrate how ignoring effects such as volume averaging, perturbation and differences in material properties of detectors can potentially lead to large errors in dose determination. It also provides data that will be incorporated in the new IAEA-AAPM code of practice. What are the implications of this research? Based on the results from this study, the authors recommend the use of detectors that require relatively little correction, such as unshielded diodes, diamonds, micro-chambers and organic scintillators, as well as passive detectors such as alanine, TLDs, and fibre coupled OSL detectors such as Al2O3:C. Some larger volume ionisation chambers required unacceptably high corrections due to the larger volume averaging correction required and non-water equivalence and, therefore, are not recommended for small beam dosimetry. GODFREY AZANGWE INTRODUCTION PHYSICS MEMBERS SURVEY WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS EDITORS’ PICKS Highlight Radiotherapy Physics Papers PHYSICS INSTITUTIONAL PATIENT-SPECIFIC IMRT QA DOES NOT PREDICT UNACCEPTABLE PLAN DELIVERY Stephen F. Kry, Andrea Molineu, James R. Kerns, Austin M. Faught, Jessie Y. Huang, Kiley B. Pulliam, Jackie Tonigan, Paola Alvarez, Francesco Stingo, David S. Followill. International Journal of Radiation Oncology Biology Physics (in Press) CORRESPONDING AUTHOR: Stephen F. Kry Assistant Professor IROC Houston QA Center Department of Radiation Physics The University of Texas MD Anderson Cancer Center Houston, USA [email protected] What was your motivation for initiating this study? The Imaging and Radiation Oncology Core at Houston (IROC Houston) intensity-modulated radiation therapy (IMRT) credentialing phantoms are managed like a patient by the hospital, including simulation, planning, and treatment delivery. Dosimeters measure the dose throughout the target volume from the clinical delivery of the plan. Thus, the IROC Houston phantoms evaluate the overall accuracy of the hospital’s IMRT treatments. In-house IMRT quality assurance (QA) aims to evaluate much the same thing: was the delivered dose distribution that which was intended? Although there are differences for IMRT QA, the expectation is that both IMRT QA and credentialing phantoms should provide the same result: they should detect the error if the planned dose is not delivered to the target. However, credentialing phantoms show approximately 20% of plans have problems, whereas IMRT QA typically reports this number to be 1-3%. This surprising disparity motivated us to directly compare in-house IMRT QA results to credentialing phantom results based on the IROC Houston phantom programme. What where the challenges during the work? STEPHEN F. KRY INTRODUCTION One major challenge of this work was that the inhouse IMRT QA data submitted by each institution PHYSICS MEMBERS SURVEY for their phantom irradiation showed the heterogeneity present in the community. Different devices, delivery methods, analysis methods, and acceptance criteria were all used and needed to be meaningfully sorted to understand the data. What is the most important finding of your study? Current IMRT QA techniques had poor sensitivity for detecting a plan that would fail an IROC Houston credentialing phantom. This was particularly true at commonly used acceptability criteria for IMRT QA, where three percent agreement or 90% of pixels passing a 3%/3mm gamma agreement showed extremely poor sensitivity. However, across all criteria (evaluated with ROC analysis) current IMRT QA methods showed no good criteria that provided reasonable sensitivity and specificity. In short, two systems that the radiation oncology community largely believes should yield the same result, do not actually agree. What are the implications of this research? This work highlights that we, as a field, must better understand how we are evaluating IMRT treatments. We must identify methods that are shown to work, and these should be broadly and consistently implemented throughout the community. WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS EDITORS’ PICKS Highlight Radiotherapy Physics Papers PHYSICS What was your motivation for initiating this study? PROTON RANGE VERIFICATION THROUGH PROMPT GAMMARAY SPECTROSCOPY Joost M. Verburg and Joao Seco. Physics in Medicine and Biology 59 (2014) 7089–7106 http://iopscience.iop.org/0031-9155/59/23/7089/article CORRESPONDING AUTHOR: Joost Verburg Harvard Medical School and Massachusetts General Hospital, Department of Radiation Oncology Boston, USA [email protected] Proton radiotherapy uses the Bragg peak and the finite range of protons to deliver a highly conformal dose distribution to the target, while reducing the integral dose to the patient by a factor of two to three as compared to x-ray radiotherapy. The advantage of the sharp distal dose gradient, however, cannot yet be fully exploited, because of uncertainty in the end-of-range of the beam when delivered to the patient. To further improve treatments, it would be highly desirable, therefore, to verify the range of proton beams in real-time. For this reason, we are developing a system to perform in vivo range verification by detecting prompt gamma-rays induced by proton-nuclear reactions. What where the challenges during the work? JOOST VERBURG INTRODUCTION The proton range verification method we propose is based on measurements of prompt gamma-rays with discrete energies resulting from specific nuclear reactions, which we related to gamma-ray emission cross sections to determine the absolute range of the proton beam. The method relies on quantitative measurements of prompt gamma-rays, which are challenging to perform during proton irradiation. The detector, electronics, PHYSICS MEMBERS SURVEY algorithms and software were designed to handle high radiation levels, to automatically adapt calibrations, and to separate the proton-induced gamma-rays from neutron-induced background. Previous data on the relevant nuclear reactions were limited, so we also measured cross sections required by our models. What is the most important finding of your study? The experiments with our prototype detector showed that the method accurately verifies the absolute range of proton beams. A unique feature of the method is the simultaneous determination of elemental composition of the irradiated tissue, which provides robust range verification in any type of tissue. What are the implications of this research? We believe that prompt gamma-ray spectroscopy combined with quantitative modelling of protonnuclear interactions is a very promising approach to in vivo range verification of proton beams. The next step is to develop a full scale system for clinical trials. WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS EDITORS’ PICKS Highlight Radiotherapy Physics Papers PHYSICS DIRECT USE OF MULTIVARIABLE NORMAL TISSUE COMPLICATION PROBABILITY MODELS IN TREATMENT PLAN OPTIMISATION FOR INDIVIDUALISED HEAD AND NECK CANCER RADIOTHERAPY PRODUCES CLINICALLY ACCEPTABLE TREATMENT PLANS. Kierkels R.G.J., Korevaar E.W., Steenbakkers R.J.H.M., Janssen T., van ’t Veld A.A., Langendijk J.A., Schilstra C, van der Schaaf A. Radiotherapy & Oncology, in press accepted September 2014 CORRESPONDING AUTHOR: Roel G.J. Kierkels Medical physicist Department of Radiation Oncology, University of Groningen, University Medical Center Groningen Groningen, The Netherlands ROEL G.J. KIERKELS INTRODUCTION What was your motivation for initiating this study? Generally, IMRT dose distributions are created by optimising a composite objective function (OF), which relies on dose-volume objectives and often also on biologically motivated indices such as the generalised equivalent uniform dose (gEUD) formalism. However, these OFs are not directly linearly correlated with clinical response. Therefore, application of more sophisticated multivariable NTCP models, comprising dose parameters of multiple organs at risk and additional prognostic clinical factors (e.g. age and baseline toxicity scores), would be more clinically meaningful. We investigated the feasibility of incorporating these multivariable NTCP models directly in the optimiser for inverse treatment planning of head and neck cancer radiotherapy. What where the challenges during the work? During conventional IMRT planning, trade-off objectives are iteratively changed by the planner, which means that IMRT plan quality is highly dependent on the expertise of the dosimetry planner. To objectively compare two optimisation techniques (i.e. inverse planning optimisation using OFs based on multivariable NTCP models or the gEUD), we used so-called “pseudo” Pare- PHYSICS MEMBERS SURVEY to front comparisons. Therefore, per patient and per technique, a database of treatment plans was automatically created in the Pinnacle treatment planning system. The calculation of the required databases of treatment plans was, however, very time-consuming. What is the most important finding of your study? We demonstrated that inverse planning optimisation with direct use of multivariable NTCP models in the optimisation process is feasible and led to clinically realistic treatment plans for head and neck cancer patients. The optimisation techniques resulted in treatment plans with only small differences. However, the use of an NTCPbased OF resulted in dose distributions which would lead to slightly lower NTCP estimates. What are the implications of this research? The objective functions based on multivariable NTCP models have the advantage of fewer unknown optimisation parameters. Additionally, the prognostic clinical factors will facilitate personalised optimisation. It is believed that these properties reduce the effort of finding optimal planning objective settings. In clinical practice, this could lead to a more efficient search of the optimal treatment plan per patient. WORKSHOP ON TRANSLATIONAL RESEARCH IN ION BEAM CANCER THERAPY EDITORS’ PICKS RTT INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM Welcome to the January/February edition of the ESTRO newsletter. I hope you had a merry Christmas and are enjoying winter, maybe with some days out of the office for a small winter holiday. I would like to wish you a happy and prosperous new year. RTT “We would like to wish you a happy and prosperous new year” The first RTT Corner of this year consists of three interesting articles. In the first article, Paul Bijdekerke (VVRO) and Aude Vaandering (AFITER. be) give us an insight into the national societies of Belgium, by describing their current situation, as well as the composition and aims of these societies. PHILIPP SCHERER In the second part of this Corner, Andreas Osztavics reviews two current articles on hot topics that shouldn't be missed. Read them before you get the information from your colleagues or patients. Last but not least, Martijn Kamphuis, chair of the scientific advisory group, and Filipe de Moura, chair of the pre-meeting course, present a sneak preview of the scientific programme of the 3rd ESTRO Forum, which will be held from 24-28 April 2015 in Barcelona. A teaser that, in addition to the city of Barcelona itself, should convince you to join us for an enjoyable and fruitful meeting. MARTIJN KAMPHUIS We hope you'll enjoy reading our RTT Corner. If you want to contribute or have ideas for future inclusions in this Corner or the ESTRO newsletter, please don't hesitate to contact us at [email protected] or [email protected] – every input is welcomed. Philipp Scherer and Martijn Kamphuis INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM RTT THE BELGIAN NATIONAL SOCIETIES Even though Belgium is a small country, like many small countries it is subdivided into different regions, languages, entities and legislative bodies. However, through this complex network, two associations have been created and have collaborated in order to represent the 25 radiotherapy departments of Belgium (six in Brussels, seven in Wallonia and 12 in Flanders): the VVRO (Vereniging voor Verpleegkundigen Radiotherapie en Oncologie ) and AFITER.be (Association Francophone des Infirmiers et Technologues Exerçant en Radiothérapie Belge). Most professionals who perform treatments in the Belgian radiotherapy centres are nurses. Legally, in Belgium, the only profession allowed to work in radiotherapy is a nurse (law dating from 1991). However, Belgian law is no longer in line with the reality of radiotherapy department needs. Nurses are not the only professionals found at the treatment workstation, or in simulation or treatment planning. Throughout the years, other professions such as laboratory technicians, physiotherapists and midwives have also been hired in the different departments. And more recently, the radiographers have found a new place in radiotherapy and are appreciated for their skill in manipulating this fast evolving technology. AUDE VAANDERING INTRODUCTION PAUL BIJDEKERKE have an excellent level of quality. However, the educational background of the nurses and radiographers working as radiation therapists (RTTs) is insufficient, especially when comparing it to European standards such as the ESTRO RTT core curriculum. They do benefit from on-site training as well as specific modules set up by education institutions or private initiatives. However, it is essential that the proper training in accordance with internal recommendations has to be encouraged and subsidised by governmental entities. In parallel, the Belgian professional recognition of RTTs needs to be legally established. The VVRO and AFITER.be have become active partners in the quest to obtain the proper training and professional recognition of Belgian RTTs. aul Bijdekerke (VVRO) and Aude Vaandering (AFITER.be) present the two societies, their composition and aims. The recent Belgian clinical audits (QUATRO), which have been carried out in the majority of the Belgian radiotherapy departments, have been able to demonstrate that the Belgian departments THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM VVRO (Vereniging voor Verpleegkundigen Radiotherapie en Oncologie) AFITER.BE (Association Francophone des Infirmier et Technologues Exerçant en Radiothérapie Belge) By Paul Bijdekerke, chair of the radiotherapy workgroup in the VVRO www.vvro.be > Most of the RTTs are nurses (approximately 90%), although the number of nurses varies among the different centres. Flanders has an umbrella organisation, the VVRO, that represents nurses who administer chemotherapy as well as nurses working in the radiotherapy centres. This association includes multiple workgroups such as the radiotherapy workgroup, chemotherapy workgroup, child oncology workgroup, breast nurses workgroup and others. The 16 members of the radiotherapy workgroup represent ten of the Dutch-speaking departments. During our meetings we share experiences, but our main goal is to organise several training sessions a year, such as interactive workshops where colleagues from the different departments can discuss protocols, methods and problems they encounter while working. During the conference, RTTs can be trained on the latest developments in radiotherapy. We also make arrangements to enable colleagues to visit another centre for a day. INTRODUCTION Along with physicists and physicians, we perform clinical audits using the Quatro (Quality Assurance Team for Radiation Oncology) IAEA (International Atomic Energy Agency) methodology. This initiative of the College of Physicians for radiotherapy departments is carried out in the five Belgian radiotherapy centres each year. The College is an advisory body to our Minister of Health. An annual report is sent to the Minister of Health and the Federal Agency for Nuclear Control. We also participate in different projects, such as writing a reference book on oncology for student nurses, writing skin care protocols and cooperating with the representatives of the Dutch-speaking colleges in relation to the training of oncology nurses. THE BELGIAN NATIONAL SOCIETIES By Aude Vaandering vice president of AFITER.BE www.after.be > The project to create the association AFITER.BE was born about a year and a half ago. The founding members met for the first time on 22 February 2013. In fact, the French-speaking region of Belgium did not have a structure to represent nurses and radiation therapists practicing in radiotherapy. Therefore, the founding members of the AFITER.BE met and reflected on the professional profile of RTTs, which had substantially evolved with the technological developments in the past decade. The fledgling organisation then formulated specific objectives and the association was legally recognised on 3 May 2014. AFITER.BE is an association that represents and promotes the RTT profession. At the centre of its concerns are the patient and the quality of care in a modern and constantly evolving radiotherapy world. The objective of the association are thus to: • Facilitate the creation of networks between the Belgian RTTs in the different radiotherapy PAPER REVIEWS 3RD ESTRO FORUM departments (nurses, radiographers, technicians,…) • Define and delimit the Belgian RTTs’ scope of practice • Participate in the continuous improvement of RTT patient care and technical related procedures through the exchange of experiences, technical procedures and training between the different radiotherapy departments • Provide objective advice and recommendations to the competent authorities concerning RTT professional recognition, qualifications and training • Organise seminars, training and workshops • Create and maintain international contacts and synergies with other professional associations directly or indirectly connected with radiation therapy • Support and help in the fight against cancer. tient quality of care by endorsing the professional recognition of RTTs. We hope to achieve this in the coming years. Read the National societies Corner of this newsletter on p 123> AFITER.be has organised its first, very successful conference (22 November 2014). Furthermore, its founding members have already been involved in the creation of a six European Credit Transfer and Accumulation System (ECTS) radiotherapy course, open mostly to nurses and radiographers already working in radiotherapy departments and wanting to solidify their competences. The association is also involved in an educational working group aiming to create a 60 ECTS radiotherapy specialisation course accessible to nurses and radiographers. Along with the VVRO, AFITER.be promotes pa- INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM PAPER REVIEWS RTT by Andreas Osztavics Paper review by Andreas Osztavics Radiation Therapist Medical University of Vienna (AT) The impact of stool and gas volume on intrafraction prostate motion in patients undergoing radiotherapy with daily endorectal balloon Evaluation of treatment plan quality of IMRT and VMAT with and without flattening filter using Pareto optimal fronts Wang KK, Vapiwala N, Bui V, Deville C, Plastaras JP, Bar-Ad V, Tochner Z, Both S.et al. Radiotherapy and Oncology, Volume 109, Issue 3, Dec. 2013, pages 437–441 Wolfgang Lechner, Gabriele Kragl, Dietmar Georg Radiotherapy and Oncolgy, Volume 112, Issue 1, July 2014, Pages 89–94 INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM PAPER REVIEWS by Andreas Osztavics RTT BACKGROUND THE IMPACT OF STOOL AND GAS VOLUME ON INTRAFRACTION PROSTATE MOTION IN PATIENTS UNDERGOING RADIOTHERAPY WITH DAILY ENDORECTAL BALLOON Wang KK, Vapiwala N, Bui V, Deville C, Plastaras JP, Bar-Ad V, Tochner Z, Both S.et al. Radiotherapy and Oncolgy, Volume 112, Issue 1, July 2014, Pages 89–94 The effect of an endorectal balloon (ERB) on prostate intrafraction motion has been assessed. No studies have addressed the impact of variable rectal stool/gas volume, when a daily ERB is used. In this study the aim was to assess the impact of rectal stool/gas volume on intrafraction 3D prostate displacements, analysed as a function of treatment time. Therefore, a group of 30 prostate cancer patients treated with daily ERB were followed prospectively using cone-beam computed tomography (CBCT) and Calypso-based localisation and tracking. METHODS Patients were provided with bladder-filling protocols and dietary guidelines. A daily regimen for emptying the rectum prior to each treatment was reinforced for all study subjects. Patients were immobilised in a supine position using an indexed knee wedge and foot lock device and an indexed-lumen, 100 ml water-filled ERB. A total of 494 datasets with CBCT and tracking information were available for analysis. Motion in LR, CC, and AP directions was evaluated. The average radiation delivery time was four minutes, and the maximum time was six minutes. The INTRODUCTION THE BELGIAN NATIONAL SOCIETIES rectum and stool/gas volumes were contoured, along with the dimension of the ERB. The total stool/gas volume was defined as the volume difference between rectum and ERB contoured on the CBCT. FINDINGS The time-dependent distributions of 3D prostate displacement are remarkably different between the small and large stool/gas volume groups. The volume and location of the rectum stool/gas can impact the effectiveness of ERB in immobilising the prostate. RELEVANCE TO RADIATION THERAPISTS (RTTS) Modern equipment and treatment techniques for prostate patients have their limits, and they are reflected in the safety margins. Patient management and more individualised immobilisation devices for high-precision treatment will be crucial in radiotherapy in the near future. In all these working fields RTTs will have an important role. Patient management will be more important and also the evaluation of the data sets from the verification systems to adapted immobilisation strategies for the individualised tailored treatment. PAPER REVIEWS 3RD ESTRO FORUM PAPER REVIEWS by Andreas Osztavics RTT INTRODUCTION EVALUATION OF TREATMENT PLAN QUALITY OF IMRT AND VMAT WITH AND WITHOUT FLATTENING FILTER USING PARETO OPTIMAL FRONTS With flattening filter-free photon beams being available in clinical practice, the differences in treatment plan quality of IMRT and VMAT treatment plans applied with flattening filter (FF) and without flattening filter (FFF) are of interest. Besides the dosimetric treatment plan quality, this study focused on the differences in delivery time between all investigated modalities. Wolfgang Lechner, Gabriele Kragl, Dietmar Georg MATERIALS AND METHODS Radiotherapy and Oncology, Volume 109, Issue 3, Dec. 2013, pages 437–441 INTRODUCTION Pareto optimal fronts were generated for six prostate and head and neck cancer patients using 9-field static IMRT and 360° single arc VMAT with and without flattening filter, respectively. The Pareto optimal fronts described the relationship between target coverage and the capability of sparing the primary organ at risk. For these calculations, the beam model of an Elekta Precise (Elekta AB, Crawley, UK) capable of delivering FFF-beams was used. Additionally, the efficiency and low dose exposure of the treatment plans was assessed by estimating the delivery times and the volume that received five Gy or more for each treatment technique. Statistical analysis of the Pareto optimal fronts was performed using the sign-test; the analysis of the delivery time was performed using student's t-test. THE BELGIAN NATIONAL SOCIETIES RESULTS No significant difference between the treatment plan quality of treatment plans calculated with flatting filter compared to treatment plans calculated without flattening filter was found. These results were independent of the investigated treatment site. However, with respect to treatment plan efficiency, a significant decrease of delivery time of IMRT treatment plans without flattening filter compared to those with filter was found. On average, the delivery time decreased by 18% and 4% for prostate and head-and-neck cases, respectively. This could be attributed to the higher dose rate in the flattening filter-free mode. In contrast to that, the delivery time of VMAT treatment plans without flattening filter was significantly increased by 22% and 16% for prostate and headand-neck cases, respectively. A reason for this was that the maximum leaf velocity of the standard multi-leaf-collimator limited the dose rate of the flattening filter free mode substantially. RELEVANCE TO RADIATION THERAPISTS (RTTS) One of the interesting factors for RTTs is that the potentially higher dose rate available for FFFbeams does not necessarily translate into a reduction of delivery time. In particular, for complex PAPER REVIEWS 3RD ESTRO FORUM PAPER REVIEWS by Andreas Osztavics dynamic treatments, such as VMAT for head and neck cancer patients, this effect was greater. Therefore, the impact for the management of the schedule for the daily treatments on the Linacs should be analysed carefully at the beginning of implementation of FFF-beams in each department. INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM 3RD ESTRO FORUM RTT RTT Meeting - Scientific programme 3rd ESTRO Forum 24-28 April, 2015 Barcelona, Spain Martijn Kamphuis Filipe Moura INTRODUCTION THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM 3RD ESTRO FORUM RTT Meeting - Scientific programme RTT "The main subjects in our programme deal with topics that are applicable to the everyday practice of modern radiotherapy" The 3rd ESTRO Forum, which will be held from 24-28 April 2015, is approaching. I’m proud to say that within this Forum the Radiation TherapisTs (RTTs) have a clear programme of their own. The main subjects in our programme deal with topics that are applicable to the everyday practice of modern radiotherapy. Besides that, there will also be sufficient time spent on developments that will affect our practice in the near future. The meeting will be preceded by a course on the implementation of SBRT. Course director Filipe Moura gives you more information on the pre-meeting course in this very Corner. The main programme of the RTT track will deal with the following topics: vision on what should be done to improve the RTT world. The meeting will end with an attractive debate on online versus offline position verification. We look forward to your participation in this debate and in the whole conference to enhance this scientific programme and to share and develop knowledge, know-how and experience. Martijn Kamphuis Chair, scientific advisory group for the RTT meeting • IGRT, margin calculation and minimising treatment volumes • Advanced treatment planning techniques • A site-specific symposium on breast cancer • Proton therapy • MRI imaging throughout the treatment chain MARTIJN KAMPHUIS INTRODUCTION The last day of the conference is a day of reflection. We will spend time looking at the future of the RTT discipline. After an extensive overview of the current situation by Mary Coffey, speakers from different parts of the globe will share their THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM 3RD ESTRO FORUM RTT Meeting - Scientific programme RTT IMPLEMENTING OF SBRT AND SRS: A REVIEW OF CURRENT PRACTICE RTT pre-meeting course 24 April 2015 Highly conformal techniques have been developed over the past couple of years. At the same time a revolution in image guided radiotherapy has taken place which makes stereotactic body radiotherapy feasible and a reality in many clinical institutions. Increased levels of confidence and implementation over planning and delivering hypofractionation and single dose regimens have led to an even safer radiotherapy environment, helped by the experience gained by departments from across Europe and the rest of the world during the last decade. The course on the review of clinical practice in the implementation of SBRT and stereotatic radiosurgery (SRS) will join synergies from several institutes. This will provide participants with the theoretical background to implement SBRT in a safe environment, which will enable the development of new skills and competences for advanced treatment strategies. FILIPE MOURA INTRODUCTION for the implementation of new techniques. An equipment-oriented session will provide a global understanding of new features, and the pros and cons of each method. To complete the course, participants will have the opportunity to assist in an online (live) practical planning session coupled with video streaming on treatment verification and delivery. For the grand finale, attendees will make use of the digital turning point system, which will help with each person’s level of understanding of the knowledge gained during the course. The final debate and concluding remarks with the faculty will complete the educational loop to ensure maximum understanding of the common practices from each specialised institution. We are expecting a very productive course, full of new insights and up-to-date information ready to be taken home. Teaching lectures will give the attendees basic and advanced concepts for their clinical daily routine, coupled with site-specific sessions for a more practically-oriented approach. On behalf of the faculty and the RTT committee, I welcome you to this course and I hope you enjoy the wonderful city… Visca Barça! Software and hardware technology is spreading and evolving quickly, and is becoming crucial Filipe Moura Course Director THE BELGIAN NATIONAL SOCIETIES PAPER REVIEWS 3RD ESTRO FORUM RADIOBIOLOGY INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ RADIOBIOLOGY “We present two innovations that could have a strong impact on our research in the coming years” Dear Radiobiology Corner reader, This month there is no specific focus to this Radiobiology Corner. However we present two innovations that could have a strong impact on our research in the coming years. We report on a meeting on Small Animal Precision Image-Guided Radiotherapy, which was held this summer in Vancouver, Canada. Furthermore we will introduce you – via an interview – to an exciting novel Citizen Science approach to immunohistochemistry scoring, incorporated into a downloadable game app. Finally, three PhD students from Martin’s group present recent papers on different topics, which are of interest to them and perhaps to you too. We would also draw your attention to a further paper in the “Read it before your patients” section on p 25, namely “p16 protein expression and human papillomavirus status as prognostic biomarkers of non-oropharyngeal head and neck squamous cell carcinoma” by Christine H. Chung et al, published in J Clin Oncol. 2014 Sep 29. The authors investigated the prevalence and significance of p16 protein expression in the oral cavity, hypopharynx, or larynx, collectively referred as non-OPSCC, where HPV infection is less common than in the oropharynx. MARTIN PRUSCHY ANNE KILTIE We hope you enjoy reading this section. Anne Kiltie, Conchita Vens, Martin Pruschy CONCHITA VENS As usual we encourage you to contact Conchita Vens, Anne Kiltie and Martin Pruschy with comments (good or bad) at our “electronic” mail address [email protected] INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ RADIOBIOLOGY SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY 11 - 13 August 2014 Vancouver, BC, Canada ESTRO recommended event The second Symposium on Small Animal Precision Image-Guided Radiotherapy was held this summer in Vancouver, Canada. This exciting meeting brought together biologists, physicists and physicians working on precision irradiation of small animals for preclinical studies. Presentations covered a wide range of themes, from irradiation and imaging technologies that enable precision radiotherapy studies, to the development and assessment of tumour models, as well as contributions from the field of curative radiotherapy for larger animals such as dogs. Other topics included preclinical trials, immunological and abscopal INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS effects, radio-modifiers and experimental animal facilities with proton beams. There was also a discussion on the need for standardisation, common protocols and networking in this new field, to optimally exploit its mix of specialities. The meeting opened with a keynote address from Albert van der Kogel (University of Wisconsin, Madison). Relating to earlier animal irradiation studies, he discussed the higher dose tolerances reported when small targets are irradiated and covered many research areas that were revisited in subsequent conference talks, including the validity of the linear-quadratic (LQ) model, effects of the very high doses used in stereotactic body radiotherapy, optimisation of PAPERS YOU MAY WANT TO READ heterogeneous dose distributions and the effects of low dose baths in modern radiotherapy. The symposium saw young researchers lauded for their work. Sarah Krueger (Beaumont Health System) won the Best Young Speaker award, for her presentation “Use of a small animal image-guided irradiator in the development of a rat model of radiation cystitis”. Although haemorrhagic cystitis is a major long-term chronic side effect of pelvic irradiation that is seen in 5-10% of patients, no high-quality clinical trials have been performed in this area and treatment options are not well established. It is, therefore, an ideal candidate for a well-controlled preclinical investigation. Krueger and colleagues used a combination of a precision irradiator, CT-guidance and an automated system to show that, compared to older studies using larger radiation fields, high doses from CT-guided small tailored fields were far better tolerated. The model will now be utilised to evaluate agents (such as immunosuppressants, for example) that could mitigate radiotherapy side effects. Robert Weersink (Princess Margaret Hospital) was the winner of the award for Second Best Young Speaker. In his presentation, “Targeting accuracy tests of bioluminescence imaging integrated INTRODUCTION with cone-beam CT for image-guided small animal irradiation”, he discussed the need for bioluminescence imaging, integrated with modern animal irradiation cabinets equipped with precision irradiation and CT, to image and precisely target early-stage tumours. Weersink described his work on various optical source reconstruction algorithms, noting the high complexity of the problem, due to the dependence of optical photon scatter and absorption on the wavelength, depth and distribution of the optical source. Studies in homogenous phantoms showed good targeting capabilities for parallel-opposed radiation beams and more complex beam arrangements. He noted that source reconstruction is hampered by heterogeneous mouse geometries, but that more sophisticated reconstruction techniques may help. One of the meeting’s youngest speakers, Hwan Lee (British Columbia Cancer Center), delivered a presentation that provoked much discussion. Lee described experiments investigating the abscopal effect, a purportedly immune-mediated inhibition of distant tumours upon primary tumour irradiation. The studies used mouse models with subcutaneously implanted breast cancer cells at each shoulder, one of which was treated with a hypofractionation scheme of 4 x 12 Gy. Lee and SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS colleagues assessed tumour response using FDG PET/CT scans and calliper measurements and saw that both irradiated and non-irradiated tumours on the same animal showed significant growth inhibition, as well as increased FDG uptake, compared with a control group. Orthotopic tumours One recurrent theme during the symposium was the use of orthotopic tumour models for image-guided radiotherapy, preferably based on bioluminescent imaging, to better mirror clinical situations and ease translation of study results into clinical trials. Rebecca Bütof (OncoRay), who was also awarded Third Best Young Speaker, and colleagues have studied the implantation of orthotopic tumours (those situated in their naturally occurring site) in the lung and brain of mice. Such models are hypothesised to represent human tumours better than the commonly used human xenograft tumours implanted subcutaneously in mice. The research revealed many details regarding the practicality of cone-beam CT and optical bioluminescence imaging of orthotopic tumours and should help pave the way towards more realistic tumour preclinical studies. PAPERS YOU MAY WANT TO READ Frank Giordano (University Hospital Mannheim) used a similar tumour model to demonstrate proof-of-principle of high-precision irradiation using three beams and a fractionated treatment schedule to spare oesophageal and tracheal structures. Jay Dorsey (University of Pennsylvania) combined gold nanoparticles with high-precision irradiation of orthotopic glioblastoma tumours and observed improved survival. He noted that the combination of gold and superparamagnetic iron oxide nanoparticle (SPION)-loaded micelles could provide an MRI contrast agent with sufficient sensitivity to detect and delineate tumours for treatment planning. Sanaz Yahyanejad (Maastricht University) demonstrated good correlation between contrast-enhanced CT and luminescence imaging and observed a dose-dependent irradiation effect on orthotopic glioblastoma growth. The second model examined was the orthotopic lung tumour, originating from cells or tumour piece implantation, or from spontaneous genetic models. Rebecca Bütof showed that tumour piece implantation is preferable to cell injections to prevent growth in the injection channel and early metastatic spread. Using mice that spontaneously develop lung tumours and integrated breath-hold techniques, Ashley Rubinstein examined whether the cone-beam CT of a small-animal irradiator can be used to investigate the relationship between tumour image features and characteristics such as aggressiveness (a study by MD Anderson’s Laurence Court). INTRODUCTION The final model presented was the metastasising cervix tumour model established by the group of Richard Hill (University of Toronto). The team used an eight-beam protocol with daily target imaging prior to fractionated irradiation combined with various other therapeutic agents. All treatment modalities demonstrated enhanced primary tumour response and reduced growth of lymph nodal metastases when combined with radiation, without significant short-term gastro-intestinal toxicities. All of these studies provide evidence that new, clinically relevant tumour models are available to fully exploit the capabilities of novel small-animal irradiators combined with imaging technology. Such developments will enable researchers to better mimic clinical radiotherapy practice using complex preclinical radiation delivery strategies. tion for small animals. They can also be assessed by http://www.sciencedirect.com/science/journal/ aip/09393889 This is an abstract of a full report authored by four workers from Maastro Clinic and Maastro Lab in Maastricht, The Netherlands, who also co-organised the meeting. Frank Verhaegen is Head of Clinical Radiotherapy Physics Research, Ludwig Dubois is Assistant Professor in Molecular Biology, Patrick Granton is a recent PhD graduate from the Physics Research group and Stefan van Hoof is a PhD student in the same group. The full report can be found at: http://medicalphysicsweb.org/cws/article/opinion/58887 Of note, there will soon appear a special issue of the journal Zeitschrift fuer Medizinische Physik, with several invited papers on precision irradia- SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ RADIOBIOLOGY “REVERSE THE ODDS”: THE NEW EXCITING GAME APP ON IMMUNOHISTOCHEMISTRY Interview with Anne Kiltie Contributor to “Reverse the Odds” game ANNE KILTIE INTRODUCTION Anne Kiltie at the University of Oxford has been involved in the development of an exciting new game app, which gets members of the public to score images from immunohistochemistry slides. In the interview below you can learn more about it and find out how you can get involved: Martin Pruschy: Hi Anne, could you quickly summarise what this game is all about? Anne Kiltie: Well, Martin, “Reverse the Odds” is a fun and unique puzzle mobile game for Apple, Android and Amazon phones and tablets aimed at casual gamers of all ages. Every player is helping Cancer Research UK scientists by analysing real cancer slides as they progress through the game. The story revolves around the world of the SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS “Odds”, cute creatures whose world has become a desolate wasteland. Gamers need to help revive the Odd-world back to its glory using special potions. Players earn potions through a puzzle game of “reversi” and by analysing cancer data. The potions are then used to revitalise the desolate wasteland the Odds live in, into an amazing wonderland. The more people who play the game, and the longer they play for, the more the scientists are helped. The cancer analysis itself takes seconds and is one part of a highly engaging game. There are over 350 levels and is easy to learn with increasing challenge and difficulty. MP: But how does it work exactly? AK: The principle behind this is that we take PAPERS YOU MAY WANT TO READ tissue images they see contain a particular molecule (represented as colour) and how much of that molecule there is (the intensity of the colour) or to count how many of a particular type cell they see (percentage of coloured cells). The samples were taken from patients’ tumours before they had their treatment so they contain cancer cells. The actual cores are 0.6 mm diameter but for the purposes of the game these are split into thirty six square segments, each 0.1 mm x 0.1 mm, so that the cells are a good size when seen on a mobile phone (looking at the whole core would mean that the cells would be too small). Each square is then analysed 25 times. lots of samples of patients’ tumours. Each tumour sample is split into hundreds of smaller cores of tissue, which we give a score depending on the cells we see. This can generate a huge amount of data. And buried in all these data are important answers that could transform cancer treatments. But it takes a long time to analyse, meaning researchers end up with data bottlenecks. Citizen science has the power to speed up this process by using the power of the crowd. “Reverse the Odds” accelerates data analysis with the aim of unveiling clues about cancer sooner, thus saving researchers valuable time. In order to progress through levels in the game, members of the public are asked to judge if the INTRODUCTION The data are processed by Zooniverse (www.zooniverse.org) to collate all the squares and scores for each sample, to give a result similar to that generated by scientists. These can then be compared with a subset of the images that have been scored in the lab by “experts”. Our lab is interested in muscle-invasive bladder cancer and we have approximately 850 images per tissue microarray set and will have 18 stained sets, some of which can be scored for nuclear, cytoplasmic and membranous proteins, so around 25 sets in total. On a rough calculation that makes 19 million classifications, but we had already achieved one million classifications within three weeks of going live. Colleagues from Southampton are interested in how the immune system can be harnessed to help treat cancer and have SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS images that are being scored from other tumour types, including lung cancer. The idea is that other people can add their data sets in future. MP: Is it only a game or will you use these data? AK: This is certainly not “only a game”. We will use the scores generated by the citizen scientists to compare with clinical outcome data from radiotherapy and surgical patients to try to identify biomarkers that are prognostic in bladder cancer and also those that are predictive of outcome after specific treatment modalities. Promising markers will then need to be validated in independent data sets. MP: How does the game as a game work? Does it get more difficult? AK: The game is comprised of two elements, playing “reversi” and scoring the images. The images alternate between the bladder cancer and immunology sets, which give variety in the images people are scoring. The analysis itself takes seconds and doesn’t get progressively more difficult, although some images are trickier to score than others. The reversi puzzle game starts off as quite easy to play and then gets more challenging, but never impossible because you can win “potions” when you score images well, which can be used to help win a game. On each round of the game you go into the lab to score images before going back to the reversi puzzle game. That way you are always contributing to the science part and are rewarded with potions when your answers match others. PAPERS YOU MAY WANT TO READ Screenshot of app page asking players to decide whether there are tumour cells present on the images or not. The ‘Not Sure’ button takes them to a tutorial with further images, to help them decide. Screenshot of app page asking players to decide what proportion of the cells are positively stained (blue). The player can select from a range of percentages, and if unsure, they can press the ‘Not Sure’ button first to be taken to a tutorial with further images, to help them decide. Screenshot of app page asking players to decide how intensely stained the cells on the image are, from weak, through medium, to strongly stained. The ‘Not Sure’ button takes them to a tutorial with further images, to help them decide. MP: Who is the target audience? And how could you use the data? Any experience on quality? Comparisons with scoring by experts? AK: The game is aimed at casual gamers of all ages but we know many people who don’t usually play mobile games are playing “Reverse the Odds” because they want to help in the fight against cancer and are enjoying it! We would never have been able to do this whole project on our own, so the additional manpower through the public getting involved is key. Now we only have to score 10% of the images for comparison with the scores of the citizen scientists. Also, having multiple opinions on each image should make the results more robust than taking the opinions of only a small number of research- ers. Zooniverse does all the processing of the data, so we get something that can be directly compared with our results in the lab, from three trained scientists reaching a consensus score. We plan to look at 10% of each dataset for comparison with the data generated by citizen scientists. When the game was being tested during development, the results being generated were very INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ similar to the lab data, so we’re excited to see the results of this. MP: Are you planning to publish these data? AK: Yes, we are hoping to publish the data in terms of the pathology, but it would also be good to publish on this approach and what we have learnt from it. MP: What is the major purpose of the app? Public awareness? Fund-raising? AK: The major purpose of the app is to accelerate our research and allow scope for analysis of many more markers, cells and molecules in our tumour samples than we would have ever been able to do ourselves. However, it is a great opportunity for the lab to get involved with public engagement in science. We also hope that the game will raise public awareness of cancer research and be fun for the gamers. “Reverse the Odds” is not about fundraising. Channel 4 TV and Stand up to Cancer have been careful to separate promotion of the game from their fundraising efforts. People playing the game are already making a huge contribution to cancer research by carrying out the scoring for us. MP: How did you get involved with this whole endeavour? AK: I was approached by Cancer Research UK in January 2014 for my opinion on current and future demand for pathology analysis in research. INTRODUCTION They contacted me again in March to see if I would be interested in getting involved in a game that was being developed by Cancer Research UK, Channel 4 TV as part of Stand up to Cancer, Maverick, Chunk and Zooniverse, to score our tissue microarrays. through the employee ranks by mapping your route through the densest areas of Element Alpha, collecting as much of it as possible, while destroying asteroids along the way. You can find links to the science behind the game here: genesin-space.org We sent in some example images and the game developers felt they could work with these, and over the following few months we had to get the various regulatory and ethical approvals in place in order to be able to send our images for inclusion in the game. We also had to work on questions to include in the tutorials, which are embedded in the game, to ensure that people were scoring the slides correctly. Meanwhile the game developers were busy at their end and, in a very exciting and productive face-to-face meeting of the project team in London in July, we got to see the prototype game and ironed out a few technical issues. Things then moved very quickly from there with the launch of the game on 3 October 2014. MP: In general, what is the benefit of involving the public in the mass-analysis of such data? Are members of the public better than computers? AK: One of the key attributes of the project is the inherent ability of humans to recognise patterns. Computer algorithms on image analysis programs don’t always work very well, or the ‘tweaking’ required is so time-consuming that it is quicker to do the scoring yourself. MP: I realise that this is not the only game produced by Cancer Research UK. What does the other one involve? AK: The other game is called “Play to Cure: Genes in Space” and it lets the public rapidly analyse significant amounts of microarray data which would have taken scientists hours to do. The mission of “Genes in Space” is to collect a fictional substance dubbed “Element Alpha”. This represents genetic cancer data, which might underpin certain types of cancer. You get to rise SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS By transforming our research data into exciting and engaging formats we can get the general public involved in this analysis, so they can stand with us in our fight against cancer. With thousands more eyes on the data, we can greatly accelerate the time it takes to clear the data backlogs, and answer more questions that will help to on develop new ways to beat cancer sooner. MP: Does the app cost anything and how much does CRUK support this approach? AK: No, the app is free to download. The game has been commissioned by Channel 4 as part of Stand Up To Cancer, and was produced by Maverick TV’s Multiplatform team and developed by Chunk. Cancer Research UK is showing great innovation in using the public to help accelerate PAPERS YOU MAY WANT TO READ research. The pioneering approach is now embedded into the charity, where they want to continue working with more scientists on more products in the future to help speed up accurate research to help bring forward the day when all cancers are cured. The mobile app has already seen more than two million images analysed by citizen scientists and has been translated into French, German, Spanish and Italian. TO DOWNLOAD THE APP: You can download it for free, and join the fight against cancer from your mobile at cruk.org/reversetheodds: · Download from the Apple App Store: itunes.apple.com/gb/app/id915440727?mt=8 > MP: Did I forget something? AK: Yes, you forgot to ask how to access the game! Please download the game and give it a try. You can download it for free to your smartphone or tablet from the Apple App Store, Google Play and the Amazon AppStore – just search “Reverse the Odds”. Also, please share the app with your colleagues, friends and family online. Whether it’s on Twitter, Facebook or LinkedIn, every share will help Cancer Research UK to recruit new players and increase the impact of “Reverse the Odds”. You can find out more here: cruk.org/reversetheodds · Download from Google Play play.google.com/store/apps/details?id=com. channel4.hardcell > · Download from Kindle AppStore: www.amazon.com/gp/mas/dl/android?p=com.channel4.hardcell > · Visit the Reverse The Odds website: www.cancerresearchuk.org/support-us/citizen-science-apps-and-games-from-cancerresearch-uk/reverse-the-odds > Lastly, if anyone is interested in finding out more about the programme or wants to work with them in the future, you can contact them on [email protected] MP: Thanks, Anne, for this interview, I am actually interested to get some feedback from the ESTRO community about this very innovative approach. Why don’t you all download this “game”, get some experience with this citizen science/crowd sourcing approach and send us your feedback to [email protected]. INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ RADIOBIOLOGY PAPERS YOU MAY WANT TO READ PAK1 tyrosine phosphorylation is required to induce epithelial–mesenchymal transition and radioresistance in lung cancer cells Cisplatin-mediated radiosensitisation of nonsmall cell lung cancer cells is stimulated by ATM inhibition Cancer Res. 2014 Oct 1;74(19):5520-31 EunGi Kim, HyeSook Youn, TaeWoo Kwon, et al. Radiother Oncol. 2014; 111:228-36 Toulany M, Mihatsch J, Holler M, Chaachouay H, Rodemann HP The retinoblastoma tumour suppressor modulates DNA repair and radioresponsiveness Clin Cancer Res. 2014 Nov 1;20(21):5468-82 Chellappagounder Thangavel, Ettickan Boopathi, Steve Ciment, et al. INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ RADIOBIOLOGY PAK1 TYROSINE PHOSPHORYLATION IS REQUIRED TO INDUCE EPITHELIALMESENCHYMAL TRANSITION AND RADIORESISTANCE IN LUNG CANCER CELLS EunGi Kim, HyeSook Youn, TaeWoo Kwon, et al. Cancer Res. 2014 Oct 1;74(19):5520-31 Paper review by Ashish Sharma PhD-student Dept. Radiation Oncology University Hospital Zürich Switzerland INTRODUCTION As I am a PhD student working on resistance mechanisms triggered by irradiation, this current study is of great interest as it demonstrates the role of a novel pathway i.e. JAK2, PAK1 and Snail in conferring radioresistance in non-small cell lung cancer. This study deals with the critical and urgent therapeutic need to identify new targets in order to overcome treatment resistance and improve treatment outcome. Radiotherapy, along with surgery and chemotherapy, is the primary treatment approach for locally advanced non-small cell lung cancer (NSCLC). However, the clinical outcomes are still disappointing with the five-year survival rate being only approximately 20%. Improvement in treatment outcomes requires development of novel treatment modalities, which can overcome radio-resistance and enhance the IR-induced cell cytotoxicity. In this recent study published in Cancer Research, EunGi Kim and colleagues revealed that p21-activated Ser/Thr kinase 1 (PAK1) and JAK2 are the key molecules that confer radio-resistance in NSCLC. They demonstrate that ionising radiation (IR)-induced phosphorylation of PAK1 on Tyr residues by JAK2 and its subsequently increased stability play important roles in survival signal transduction in NSCLC cells. SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS Previously, they evaluated whole-transcriptome alteration in radio-resistant A549 cells in response to irradiation and identified PAK1, which was significantly up-regulated. They hypothesised that IR-dependent up-regulation of PAK1 might lead to epithelial to mesenchymal transition (EMT), migration and inflammatory processes [1]. In the current study, they demonstrate that PAK1 is differentially up-regulated, tyrosine phosphorylated, and translocated to the nucleus. JAK2 controls the tyrosine phosphorylation of PAK1 and was essential for protein stability and binding to Snail. PAK1-Snail binding was validated using peptide fingerprinting, and functional interactions were determined using curated databases. Snail actively regulates epithelial to mesenchymal transition (EMT) through promotion of transcriptional repression of several genes, including epithelial marker proteins (E-cadherin). Inhibition of Tyr phosphorylation of PAK1 can reduce IR-dependent EMT. JAK2 inhibitors can also counteract the tyrosine phosphorylation of PAK1 leading to radiosensitisation and reduced in vivo EMT in a lung carcinoma-derived xenograft mouse model. In a nutshell, the authors demonstrate that Tyr PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ phosphorylation of PAK1 confers radioresistance to lung carcinoma cells. This novel regulatory mechanism of radioresistance includes functional involvement of JAK2, PAK1 and Snail in response to irradiation. JAK2 inhibitors could be used as potent radiosensitisers and promising agents to counteract IR-induced EMT. 1. Yang HJ, Kim N, Seong KM, Youn H, Youn B. Investigation of radiation-induced transcriptome profile of radioresistant non–small cell lung cancer A549 cells using RNA-seq. PLoS ONE 2013;8: e59319. INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ RADIOBIOLOGY THE RETINOBLASTOMA TUMOUR SUPPRESSOR MODULATES DNA REPAIR AND RADIORESPONSIVENESS Chellappagounder Thangavel, Ettickan Boopathi, Steve Ciment, et al. Clin Cancer Res. 2014 Nov 1;20(21):5468-82 Paper review by Sabine Bender PhD-student Dept. Radiation Oncology University Hospital Zürich Switzerland INTRODUCTION Molecular characterisation of tumours is crucial to individualise cancer therapy and is becoming increasingly more important for radiation therapy. By targeting the driving force, the tumour can be sensitised to radiation treatment and normal tissue toxicity can be lowered. The retinoblastoma protein is one of the best-studied tumour-suppressor genes and it is inactivated in various types of cancer. Therefore, there is a clear imperative to investigate the impact of the retinoblastoma status on radiation sensitivity. The retinoblastoma protein (RB1) is a tumour suppressor protein that regulates G1-S cell cycle progression. In a dephosphorylated state, RB1 binds and inhibits E2F-regulated gene promoters. Phosphorylation inactivates RB1 and allows transcription of E2F-regulated genes, which are required for cell cycle progression. Retinoblastoma is functionally inactivated in several tumour types. In prostate cancer, it occurs during progression of the disease in only five percent of primary tumours, but approximately 30-40% of metastatic and castration-resistant prostate cancers show retinoblastoma inactivation. Although the retinoblastoma inactivation rate is relatively high in prostate cancer, so far only a few studies have investigated its role in radiation responsiveness. SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS The study by Thangavel et al. shows for the first time that loss of the retinoblastoma function results in increased radiosensitisation of human prostate cancer cells. The authors demonstrate increased radiosensitivity of retinoblastoma-deficient prostate cancer cell lines compared to their retinoblastoma proficient pairs, in both hormone-sensitive and castrate-resistant cancer cells. No differential response in cell cycle distribution was observed after radiation of the cell lines, regardless of their retinoblastoma status. However, the amount of IR-induced double-strand breaks was significantly higher in retinoblastoma-deficient cells suggesting that retinoblastoma loss alters DNA damage and repair capacity in response to radiation. As retinoblastoma is involved in anti-apoptotic signalling, the effect of retinoblastoma loss on apoptosis was investigated. In response to radiation, retinoblastoma-deficient cells show increased levels of NF-κB and elevated transport to the nucleus where it acts as a transcription factor. It binds to the promoter region of the polo-kinase 3 (PLK) and mediates apoptosis via PLK3 transcripts. Differential radiosensitivity was further demonstrated in xenograft models, where retinoblastoma depletion showed a tumour growth delay. Additionally, prostate specific antigen (PSA) levels were significantly lower in PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ animals carrying retinoblastoma-deficient xenografts. In a retrospective study, a set of biopsies was analysed retrospectively where patients developed local recurrence after radiation treatment. All samples were stained positive for retinoblastoma, strengthening the hypothesis that these cells are more radiation resistant. This raises the question as to whether the retinoblastoma status could be considered as a biomarker upon which to base therapeutic decisions. Cyclin-dependent kinase (CDK) inhibitors could provide an approach to halt cellular proliferation in retinoblastoma-proficient tumours, whereas retinoblastoma-deficient tumours could be treated with DNA-damaging agents to hypersensitise them to genotoxic stress. INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ RADIOBIOLOGY CISPLATIN-MEDIATED RADIOSENSITISATION OF NONSMALL CELL LUNG CANCER CELLS IS STIMULATED BY ATM INHIBITION Toulany M, Mihatsch J, Holler M, Chaachouay H, Rodemann HP Radiother Oncol. 2014; 111:228-36 Paper review by Andrea Orlando Fontana PhD-student Dept. Radiation Oncology University Hospital Zürich Switzerland INTRODUCTION As I work on cancer and DNA repair, this paper has offered me interesting insights into how specific molecular mechanisms, which are linked to the DNA repair machinery, are also responsible for treatment resistance to classic clinically-relevant chemotherapeutical compounds such as cisplatin. Cisplatin (cis-diamminedichloroplatinum(II), CDDP) is a widely used chemotherapeutic agent for sarcoma and carcinoma, especially for lung and ovarian carcinoma. CDDP primarily acts as a cross-linking agent, forming intrastrand DNA adducts, which are mainly repaired by the nucleotide excision repair pathway. Indeed, cells defective in this pathway are hypersensitive to cisplatin. Following NER activation, a cascade of downstream proteins are activated, which bind to the cisplatin-induced distortions in the DNA, leading to delayed DNA damage repair, cell cycle arrest and induction of apoptosis. Among these proteins, recruitment of ATM (ataxia telangiectasia mutated protein) kinase leads to repair of the damaged DNA by promoting DNA-PKcs transphosphorylation and BRCA1 activation through its BRCT domain. ATM activation also induces cell cycle checkpoint activation, cell cycle arrest and autophagy, ensuring that the cell can survive SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS DNA damage. Resistance to cisplatin can be multifactorial. Reduced drug uptake, increased drug inactivation and increased DNA adduct repair all contribute to resistance. Interestingly, over-expression or activation of specific DNA repair proteins, including ATM, has recently been shown to be a serious candidate mechanism for clinically observed cisplatin-resistance. In this study Mahmoud Toulany investigated the radiosensitising effect of cisplatin and its molecular background in the non-small cell lung cancer cell line A549 and H460. Interestingly, cisplatin sensitised H460 cells but not A549 cells to ionising radiation. Lack of radiosensitisation in A549 cells was associated with increased cytoplasmic ATM phosphorylation at serine-1981, which exerts several pro-survival effects thereby counteracting the cytotoxic effects of ionising radiation. Indeed, combined treatment with cisplatin and the potent ATM inhibitor KU-55933 strongly sensitised both H460 and A549 cells, indicating a pro-survival effect of cisplatin-mediated activation of ATM. Toulany et al. also demonstrated a strong involvement of the ATM/AMPK-pathway, which is part of the cellular metabolic and energy regulation machinery, in the observed cisplatin-resistance in the A549 cells. PAPERS YOU MAY WANT TO READ PAPERS YOU MAY WANT TO READ The role of ATM kinase in DNA damage recognition after cisplatin treatment was further investigated. Surprisingly, a strong reduction in residual γH2AX foci was observed in response to treatment with cisplatin and the ATM inhibitor despite the synergistic effect of KU-55933 and cisplatin at the level of clonogenic survival. These results suggest a limited recognition of radiation-induced DNA breaks rather than a lower frequency of initial radiation-induced DNA double strand breaks in cells pre-treated with the ATM inhibitor alone or in combination with cisplatin. According to the model proposed by the authors, ATM activation following cisplatin-treatment leads to the activation of several pro-survival mechanisms including reduction of apoptosis, autophagy and improved energetic metabolism through the AMPK pathway. Therefore, selective blockage of the ATM kinase in combination with cisplatin could improve the radiation response especially in tumour cells with reduced treatment responses to platinum compounds alone. INTRODUCTION SYMPOSIUM ON SMALL ANIMAL PRECISION IMAGE-GUIDED RADIOTHERAPY REVERSE THE ODDS PAPERS YOU MAY WANT TO READ ESTRO SCHOOL INTRODUCTION E-LEARNING COURSE REPORTS E-ESO ESTRO SCHOOL “The course directors and teaching staff have been chosen because they are international experts in their fields” Education has always been a central theme for ESTRO and the remit of the Education and Training Committee (ETC) has now expanded to the extent that the Board agreed that it would be appropriate for the Core Education Committee to become a full ESTRO Council in 2015. The structure and composition of this new Council is being drafted currently and more details will be presented to the Education and Training Committee in February. The education courses on offer for 2015 are designed to cover comprehensively the core curricula for radiation oncologists, radiation physicists and RTTs. As always, the course directors and teaching staff have been chosen because they are international experts in their fields who also have a track record of excellent teaching. Participation in live ESTRO courses supplements teaching at national levels and allows participants to interact with their peers from other countries, to harmonise their training to European standards and to achieve the knowledge and skills required for tomorrow’s practices. Of course, it is not always possible to attend all of the four-day live courses that you would like to during the year. Alternative ways to benefit from the high quality ESTRO teaching on offer are to sign up for one of the online courses or one of the one-day pre-meeting courses. Check out the exciting possibilities listed on the programme for 2015. FIONA STEWART Core member, Education and Training Committee CHRISTINE VERFAILLIE ESTRO Chief Operating Officer Finally, we are happy to welcome Fiona Stewart to the editorial team of the School Corner. Fiona has been involved with ESTRO for many years, specifically in the School activities. She is a core member of the current ETC and she will now contribute to developing this Corner to best reflect how stimulating our educational activities are. Richard Pötter, Christine Verfaillie and Fiona Stewart INTRODUCTION E-LEARNING COURSE REPORTS RICHARD PÖTTER Chairman, Education and Training Committee E-ESO ESTRO SCHOOL E-LEARNING Future horizons for Online FALCON workshops It was almost two and a half years ago that I was invited to participate in the first “pilot” Online FALCON (Fellowship in Anatomic deLineation and CONtouring) contouring workshop in breast cancer. I still remember perfectly that first online meeting. The whole idea seemed so innovative and exciting. Since then, I have participated as a tutor and have been able to witness at first hand how certain aspects have evolved slightly, while always maintaining the spirit of a very interactive, close and personal teaching experience, even though we are all many kilometres apart. This is what I find the most outstanding feature of these workshops, and I believe that this is the reason for their success. Thanks to the small size of the groups (maximum 20-25), the faculty and tutors establish a special connection with the participants, and the participants also have the opportunity to get acquainted with each other. How FALCON workshops began ELEONOR RIVIN DEL CAMPO INTRODUCTION The background of the FALCON project comes from the well-known importance of contouring definition of target volumes in radiation oncology. There is a continuous evolution of the definitions of Gross and Clinical Target Volumes (GTVs and CTVs), as well as for Organs At Risk (OARs). Therefore, even though specifications are available in ICRU reports, and guidelines/recommendations have been published by international societies like ESTRO and the Radiation Thera- E-LEARNING py Oncology Group (RTOG), many single and multi-institutional trials have also contributed to this body of literature. This led ESTRO to focus on this subject in order to reduce contouring uncertainties (both the intra- and inter-observer variability), aiming to gain in tumour control while minimising morbidity. Initially, FALCON was used for onsite, interactive delineation workshops performed at annual ESTRO meetings and live ESTRO teaching courses (Eriksen et al. Four years with FALCON – An ESTRO educational project: Achievements and perspectives. Radiother Oncol; Jul 2014). The first Online FALCON contouring workshop was held in October 2012, in breast cancer. The experts were Birgitte Offersen and Philip Poortmans, and the tutors were Sofia Rivera and Arturo Navarro. The next topic to be taught in this format was head and neck cancer. And, just recently, two workshops have been held in gynaecological cancer (the first one in external beam radiotherapy and the second in brachytherapy). All of these workshops were fully booked, and in the last one there was outstanding interaction between the faculty, tutors and participants. Dynamics of the Online FALCON workshop The structure of Online FALCON workshops is identical. The live sessions are held through an online platform for interactive presentations, the WebExTM system. During the first session the COURSE REPORTS E-ESO Screenshots of the breast cancer Online FALCON contouring workshop, showing the teacher, Birgitte Offersen (left) and one of the tutors, Eleanor Rivin del Campo (right). case is presented, as well as the FALCON contouring system (EduCaseTM software, http://estro. educase.com/), the teachers, the tutors and the participants. Each interactive live online session is between 1-1.5 hours long. The participants are invited to contour certain Regions Of Interest (ROIs) during the first week. The second session is when the guidelines for the specific tumour site are presented and the contours from the first week are reviewed. Contours may be shown anonymously, which improves the quality of the discussions, since the participants feel comfortable commenting on the strengths and weaknesses of the anonymous contours. During the second week they are asked to re-contour the case. The INTRODUCTION third and final live WebEx meeting consists in presenting the contours from the first and second week, compared with those from the teacher, as well as between weeks, and there is a question and answer session. Looking ahead The Online FALCON contouring workshop family has steadily grown, with new incorporations of faculty and tutors, allowing them to broaden the scope of tumour sites within the frame of the ESTRO School. The enthusiasm of all of the components of each Online FALCON contouring workshop team seems to be contagious, attract- E-LEARNING ing more and more experts and tutors to this new teaching method. All of this has allowed the Online FALCON workshop team to begin planning for the future. Their goal is to establish an annual programme of workshops, as already exists, and in parallel, with the ESTRO live courses. The initial tumour sites under discussion are gynaecology (brachytherapy as well as external beam radiotherapy, in separate workshops), head and neck, prostate, accelerated partial breast irradiation, organs at risk and paediatric. However, if more experts come forward in other fields, COURSE REPORTS E-ESO the more the merrier! Ideally, approximately seven to ten Online FALCON workshops may be held in total, per year. This would allow more participants to enrol in these workshops, as the demand is quite high. And finally, an even more ambitious project is the possibility of trying to integrate ESTRO live courses with the Online FALCON workshops. This will take careful thought and planning, but may give very interesting results. Eleonor Rivin del Campo Specialist in radiation oncology Gustave Roussy Cancer Campus Villejuif, France [email protected] INTRODUCTION E-LEARNING COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL Accelerated partial breast irradiation Advanced treatment planning 6 - 9 September 2014 | Barcelona, Spain 20 - 25 September 2014 | Budapest, Hungary Clinical practice and implementation of imageguided stereotactic body radiotherapy Image guided radiotherapy in gynaecological cancers with a focus on adaptive brachytherapy 7 - 11 September 2014 | Florence, Italy Basic treatment planning 16 - 20 September 2014 | Budapest, Hungary INTRODUCTION E-LEARNING 28 September - 2 October 2014 | Florence, Italy Best practice in radiation oncology: a workshop to train RTT trainers 20 - 24 October 2014 | Vienna, Austria COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL ACCELERATED PARTIAL BREAST IRRADIATION 6 - 9 September 2014 Barcelona, Spain COURSE DIRECTOR: Philip Poortmans Radiation oncologist Radboud University Medical Center Nijmegen, The Netherlands Holá BCN! 4 dies. For many of us this was the first contact with the city of Barcelona (a four-day travel card). In this beautiful city of Cataluña, an ESTRO teaching course specially focused on accelerated partial breast irradiation (APBI) was held for four days. For many years, APBI used to be incorporated into teaching courses that were dedicated only partially to breast cancer. This was the first time in the history of the ESTRO School that this increasingly popular treatment modality in early breast cancer became a focal point of the whole course. ESTRO intends to organise this kind of course at regular two-year intervals. The venue was in the new part of the Hospital de la Santa Creu i Sant Pau. This event gathered more than 60 participants from all around Europe, some from Asia and Latin America. The atmosphere during coffee breaks was very cosmopolitan and enriched with lively discussions. The academic programme was well balanced and based on a multidisciplinary approach, ranging from pathology, imaging, surgery, to radiation oncology and physics. PAVOL LUKACKO INTRODUCTION The first day started with an essential introduction to early breast cancer, and various imaging E-LEARNING modalities in breast and breast histology as well. We were guided through illustrative documentation from a radiologist and pathologist, followed by technical aspects of various techniques in APBI. An interesting presentation on target volume delineation was, for me personally, the highlight of the first day. GEC-ESTRO guidelines transformed to actual contours on computed tomography and presented slice by slice were very descriptive and truly helpful. At the end of the first day, we all enjoyed a guided tour and welcome reception in the spectacular Hospital de la Santa Creu i Sant Pau, which is a UNESCO World Heritage Site. The second day was dedicated to risk factors for recurrence in breast cancer, indications of APBI and details of most frequently-used APBI techniques. Pictures with evidence-based data helped us better understand various approaches to this specific type of irradiation, all the more so that the course teachers were renowned experts in their particular fields. All of this was complemented with a presentation about the physical principles underpinning each technique. An excellent dinner served on the beach only reminded us that Barcelona is a seaside Mediterranean city with a unique atmosphere and delicious food. COURSE REPORTS E-ESO COURSE REPORTS Is APBI ready for prime-‐@me? Is APBI ready for prime-‐@me? Yes for all techniques Yes for all techniques Yes for EBRT Yes for EBRT Yes for mul@catheter BT Yes for mul@catheter BT Yes for single-‐catheter BT Yes for single-‐catheter BT Yes for IORT linacs Yes for IORT linacs Yes for Intrabeam Yes for Intrabeam No for all techniques No for all techniques 29% 11% 2% 2% 7% 29% 11% 7% 16% 16% 2% 0% 2% 0% 2% 0% 2% 0% 4% 4% 20% 20% 7% 7% 38% 38% Before debate AMer debate Before debate AMer debate 62% 62% Voting results of course participants before (blue) and after (red) the debate entitled “Is APBI ready for prime-time?” External radiotherapy APBI and the surgical point of view were the main topics of the third day. It was dominated by an impressive and controversial debate among teachers arguing for and against APBI being routinely used outside of clinical trials. Day four summarised treatment-related toxicity and future perspectives of breast radiotherapy. At the beginning of the course all participants were given contouring homework consisting of two cases of early breast cancer with an indication for APBI. To complete our task we used the ESTRO contouring tool – FALCON Educase software. It was very interesting to see how the real- INTRODUCTION isation of contours differed from participant to participant. Pictorial guidelines of contouring the volume for APBI and practical tricks were gone through interactively in detail during the course. The delineation workshop was divided into two sessions and we watched the whole process on our laptops, complemented with additional comments by our course teachers. An interactive voting system gave an opportunity to all participants to take part in case-specific treatment decisions, which were then discussed among the audience. I believe that the first ESTRO teaching course to focus exclusively on APBI was a great success E-LEARNING and I can only recommend it to all colleagues in their work in treating early breast cancer patients. The next course will take place in two years. I am convinced that everyone involved in this area of medicine is looking forward to the next couple of years, as more new data will become available on APBI from a number of large clinical trials exploring this technique. Pavol Lukacko St. Elisabeth Oncological Institute Bratislava Department of radiation oncology Bratislava, Slovakia [email protected] COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL CLINICAL PRACTICE AND IMPLEMENTATION OF IMAGE-GUIDED STEREOTACTIC BODY RADIOTHERAPY 7 - 11 September 2014 Florence, Italy COURSE DIRECTORS: Dirk Verellen Physicist UZ Brussel (VUB) - Brussels, Belgium Matthias Guckenberger Radiation oncologist University Hospital Zurich - Zurich, Switzerland The third edition of “Clinical practice and implementation of image-guided stereotactic body radiotherapy (SBRT)” was my first ESTRO course. I did not know what to expect but I was full of enthusiasm on my way to the airport. MARIE LAMBRECHT INTRODUCTION Indeed, I was going to need this positive attitude to get me through the first day of travelling because nothing went right. Due to a strike by the E-LEARNING Italian air controllers my flight was cancelled, as were most of the flights to Italy. For me and for other participants trapped in their own country, the time for creativity had come. After 10 hours of brainstorming in the airport I took off for Spain and even slept in Barcelona airport! I finally arrived the next morning in Florence and went directly to the venue. Even If I wasn’t as well prepared as I could have been if I had rested, I COURSE REPORTS E-ESO COURSE REPORTS surprised myself by listening attentively. For performing the miracle of keeping my attention after a long 24 hours, I am grateful for a very skilled and animated teaching committee. The lectures were designed to enable participants, composed of radiation oncologists, physicists and radiation technologists, to build a gradual and thorough understanding of the stereotactic techniques. After an historical background from frame-based SRT to the most advanced image guided frameless SBRT, two case demonstrations were shown. Then the afternoon was dedicated to biological benefices of hypo-fractionation but also awareness of correlated toxicity risks. Following a logical order, the next day was designed around target management, starting with static sites to breathing-impacted locations. Planning evaluation and quality assurance for these treatments were then discussed. We retained the message that no matter which device and techniques we choose, the challenge of delivering high dose to a small volume is first to have a good communication and understanding between us regarding what we are doing, which prescription to which volume, homogenous or heterogeneous dose inside the planning target volume, or which means to compensate for target motion. INTRODUCTION In the evening we were invited to the social event held in the heart of Florence, a few footsteps from the Duomo. At first I was surprised that the event was more about snacks and drinks than a dinner. However, my lasagne mourning did not last long, as my colleagues and I started dancing. The night was very enjoyable and accelerated our group cohesion. morning. After a summary and a statement about how to start a SBRT programme, we left each other as new disciples of the good practice of SBRT and SRT. The next morning, despite the beautiful weather, we were still just as eager to increase our knowledge. Lectures focused on the treatment of nonsmall cell lung cancer and the first presentation was from a surgeon. It was much appreciated to have their point of view. Surgery is the concurrent and still preferred option in case of operable small lesions. On behalf of the others participants I thank the organisational team for the management of the event. I felt very lucky to attend this course, and I would encourage every novice or confirmed stereotactic lover to attend and share their questions and experiences with this invaluable teaching team. During the afternoon we were split into several groups. These split sessions were very practical and informative, and gave us real insights. We were encouraged to ask questions and share our experience on the topic of the session. Wednesday was designed similarly, with interesting lectures in the morning about SBRT for oligometastasis and split up sessions during the afternoon. Marie Lambrecht PhD student Catharina Ziekenhuis Eindhoven, The Netherlands [email protected] The five days went smoothly, split by coffee and pastry breaks, and nice lunches held in the cloister of the old monastery. There was a particular but indefinable emotion amongst the group as we finally came to the last E-LEARNING COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL BASIC TREATMENT PLANNING 16 - 20 September 2014 Budapest, Hungary COURSE DIRECTOR: Michelle Leech Associate Professor TCD Discipline of Radiation Therapy Dublin, Ireland Budapest has always fascinated me for being one of the most beautiful cities of Europe. It has a true blend of modern architecture and medieval European architecture. When I was offered the opportunity to attend ESTRO’s basic treatment planning course to be held in Budapest, I jumped at the opportunity and was truly excited. AUN MUHAMMED INTRODUCTION At that point I did not realise that these few days E-LEARNING would be some of the most memorable and rewarding days of my life. Not only did I get the opportunity to meet some wonderful new colleagues from all over the world, ranging from South America to Europe, Middle East and the whole of Europe, but we also had the opportunity to be trained by one of the finest ESTRO faculties. Michelle Leech, the director of the course, and Viviane Van Egten, the programme manager, COURSE REPORTS E-ESO COURSE REPORTS did their utmost to make this course successful. Sadly Michelle is going to leave the course directorship next year, but fortunately she will remain in the faculty. Not only did we have the opportunity to have basic hands-on training from different faculty members but there were also many fascinating, engaging and brain storming sessions in which participants very actively participated with questions and comments. Although mainly a physics and treatment planning workshop, we were also lucky to have frequent clinical inputs from Charles Gillham and Paul Kelly. How can I forget the most wonderful social dinner organised by the popular Viviane, who always had a courteous smile and was ready to help everybody with any issue. The magic host of the dinner made the evening even more memorable by singing the finest songs from almost all the countries of the participants. The way he sang a Chinese song spontaneously left our Chinese colleagues mesmerised. Talking to different participants, who have also attended previous ESTRO courses, they commented that this had undoubtedly been one of the best. The learning and training, which we got INTRODUCTION from this course, has increased our confidence in handling treatment planning and will definitely help us in our future work. The contacts that we made during the course with the wonderful faculty members and colleagues will stay with us for a long time. Finally, I would like to thank the vendors and the local organisers who worked tirelessly behind the scenes to make this course successful, so that E-LEARNING learning treatment planning was a fruitful experience for every one of us. Aun Muhammed Speciality registrar Royal Marsden Hospital London, UK COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL ADVANCED TREATMENT PLANNING 20 - 25 September 2014 Budapest, Hungary COURSE DIRECTOR: Gert Meijer Physicist UMC - Utrecht, The Netherlands CO-CHAIR Neil Burnet, Radiation oncologist Cambridge University - Addenbrooke’s Hospital, UK I have recently started training as a medical physicist and I came across this course while browsing through the ESTRO School calendar. I was looking for a course that would provide me with a solid background as well as practical skills in advanced treatment planning techniques, and this course fully satisfied my educational needs. CHRYSI PAPALAZAROU INTRODUCTION Already, before the course began, I appreciated the focus on hands-on practice, which was clear E-LEARNING from the course schedule. The general structure of the five-day course was as follows: each morning, a number of lectures addressed specific topics in advanced treatment planning. After the lunch break, the practical part of the day was introduced by a lecture on physical and/or clinical considerations relevant to the case discussed on that day. This was followed by a presentation on practical planning aspects, which gave useful guidelines and tips for the case at hand. The COURSE REPORTS E-ESO COURSE REPORTS The teaching staff consisted of a well-balanced group of expert physicists, clinicians and RTTs, who together created a structured, yet informal and intimate teaching atmosphere despite the number of participants (approximately 100). I very much appreciated the staff’s openness and readiness for discussion, both during and between lectures. four cases were selected to be sufficiently challenging for planners with little to medium experience. During the rest of the afternoon sessions the participants, working in groups of two to three people, were assigned to a treatment planning system (TPS) station and planned the case. The results of each day were discussed in the first session of the following morning, where some representative plans made by participants were presented and discussed. The participants voted for the best plan each day, which was a nice way to keep us motivated to generate quality plans. INTRODUCTION The ESTRO basic and advanced treatment planning courses (which were organised back-to-back in Budapest) presented a unique opportunity; namely, several different TPSs were set up in different rooms, accompanied by company representatives. This was a rare opportunity to get hands-on experience with TPSs, something that is not available at one’s own institution and an invaluable experience for someone in training such as myself. Even for someone with no experience in a certain TPS, it was possible with the help of the company representatives, and other more experienced participants, to generate good quality plans. E-LEARNING Budapest is a city rich in cultural life, history and architecture. We had the chance to admire some of its most famous monuments, beautifully illuminated, during the social dinner aboard a cruise ship on the Danube, accompanied by Hungarian and other delicacies and live folk music. All in all, this was an excellent course, highly recommended for those with some experience in treatment planning who want to sharpen their skills in advanced techniques. Chrysi Papalazarou Medical physicist in training Erasmus MC Rotterdam, The Netherlands COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL IMAGE GUIDED RADIOTHERAPY IN GYNAECOLOGICAL CANCERS WITH A FOCUS ON ADAPTIVE BRACHYTHERAPY 28 September - 2 October 2014 Florence, Italy COURSE DIRECTORS: Christine Haie-Meder Radiation oncologist Institut Gustave Roussy - Villejuif, France Richard Pötter Radiation oncologist Medical University Hospital - Vienna, Austria REKHA NEUPANE INTRODUCTION Having treated patients with cervical cancers in the orthogonal era for a long time, it was only in the past couple of years I treated patients with image guidance (CT in India and, more recently, MRI at the Clatterbridge centre on the Wirral in the UK). Of course, it was self taught and I learnt from what I saw my peers doing. Hence, I was keen to attend this course and hoped to gain from it. It far exceeded my expectations. E-LEARNING The course was extensive and thorough, going from the basics with attention to detail, to the recent advances and results. It covered cross-sectional anatomy (with particular emphasis for external beam radiotherapy and brachytherapy), contouring, aspects and perspectives from physics; it dealt with intracavitary, interstitial techniques for cervical cancers and for endometrial, vulval and vaginal cancers. In addition there COURSE REPORTS E-ESO COURSE REPORTS I have to now speak of the faculty; all I can say is they were knowledgeable, experienced and passionate about disseminating this. We could see that they were keen to promote good practice and make this as uniform as possible across the world, especially as the incidence of cervical cancer is greater in the developing countries. The social programme on the third day was well attended and enjoyable. The workshop venue and Florence were the perfect settings for this extremely well-presented and run course. The evenings were lovely with friendly delegates from various countries, which was a lot of fun too. were case discussions and contouring exercises for various scenarios with plenty of scope for interaction and questions, with the discussions being robust. Other useful and interesting topics covered were the inter and intrafraction uncertainties and imaging strategies, nodal and parametrial boosts and midline blocks. Parallel workshops for clinicians and physicists and radiation therapists were popular as well. INTRODUCTION The quality of the presentations and the experience of the faculty was so good that the attendance was almost 100% on all days for all of the day, with some drop off only on the last day towards the end as the delegates had to catch their flights back home. Even then, most tried to stay on as long as possible. There were video presentations of interstitial brachytherapy at lunch times; again this was enthusiastically attended and this spoke of the interest generated by the faculty. E-LEARNING Finally, I have to note that the faculty and the organiser were friendly and allowed the programme to be interactive and that we thoroughly enjoyed it. It was easily the best course I have attended. Rekha Neupane Consultant clinical oncologist North Wales Cancer centre, UK [email protected] COURSE REPORTS E-ESO COURSE REPORTS ESTRO SCHOOL BEST PRACTICE IN RADIATION ONCOLOGY: A WORKSHOP TO TRAIN RTT TRAINERS 20 - 24 October 2014 Vienna, Austria COURSE DIRECTORS: Mary Coffey School of Medicine Trinity College - Dublin, Ireland Guy Vandevelde High School of Health Sciences University of Brussels, Belgium IGLIKA MIHAYLOVA INTRODUCTION PETKO TSENOV DOBROMIRA DECHKOVA It was a great pleasure to attend the five-day course, organised by ESTRO and supported by IAEA, on the topic of “Best practice in radiation oncology: a workshop to train RTT trainers” in 2014 in Vienna, Austria. The participants were radiation therapists (RTTs), physicians, physicists and engineers from 11 different countries in Eastern Europe, Western and Central Asia. E-LEARNING The main objective of the training was preparing for the practical organisation of a course for RTTs on a particular topic, relevant to the respective country and clinic. As participants, we appreciated this type of training (a brilliant idea of the course director Mary Coffey) aimed at the direct contractors of the radiotherapy process – the RTT. COURSE REPORTS E-ESO COURSE REPORTS practice. The presentations of the leading lecturers discussed the following topics: factors to consider when preparing a short course, professional presentation techniques, organising a practical workshop, practical organisation of the course, and running a journal club. ESTRO and IAEA Core Curricula / Benchmarking revision 2003 and 2014 were presented during the first day. The topics, highlighted and emphasised during the training, encompassed the role of the RTT in the radiotherapy team, the RTT’s roles and responsibilities to deliver optimum treatment to patients, to optimise the radiotherapy process for patients, and to develop the role and promote the profile of the RTT within the multidisciplinary team. In addition, other topics focused on enabling the RTT to distinguish between good and bad practices and to always accept only best practices, to meet new challenges and adapt to changes in the environment, as well as to engage in reflective INTRODUCTION The course format was well structured with lectures, followed by workshops. The faculty were very warm, enthusiastic and constantly in contact with groups from different countries. They gave their valuable advice and recommendations for the future organisation of courses on relevant topics in the respective countries. The lecture “Practical organisation of a teaching course” helped the participants to suggest an adequate framework for future courses. After four days of intensive work the course ended with each group, having prepared a draft programme for a forthcoming course in their country. The social dinner was held in a traditional Austrian restaurant with national cuisine that enabled communication between the course participants in an informal setting. Vienna, the city of music, with its beautiful sights – gothic cathedrals, palaces with art galleries and beautiful parks – allowed the participants to fully relax after a long working day. E-LEARNING The training course, with its perfect organisation, selected team of experienced lecturers and moderators, combined with the charm of the city of Vienna, will be remembered by all participants as a rewarding and valuable experience. Therefore, we would like to highly recommend this course to RTTs involved in teaching and training. Dobromira Dechkova Radiation therapist Specialised Hospital for Active Treatment in Oncology Sofia, Bulgaria [email protected] Iglika Mihaylova Radiation oncologist Specialised Hospital for Active Treatment in Oncology Sofia, Bulgaria [email protected] Petko Tsenov Radiation therapist Tokuda Hospital Sofia, Bulgaria [email protected] COURSE REPORTS E-ESO ESTRO SCHOOL E-ESO Free distance learning programmes on the internet The European School of Oncology, in co-operation with Nature Reviews Clinical Oncology and Critical Reviews in Oncology Haematology, is holding a series of free distance learning programmes on the internet, called “e-sessions”: e-grandrounds and e-oncoreviews. e-grandrounds are bi-monthly sessions on hot-topics organised without commercial sponsorship and are CME and ESMO-MORA accredited. e-oncoreviews are monthly sessions designed to offer a balance and comprehensive overview on a specific topic, be it a tumour type, a type of therapy, diagnostic or therapeutic approach. Some e-oncoreviews are organised in collaboration with the School’s sponsors, whilst ESO-organised sessions are held in co-operation with Nature Reviews in Clinical Oncology and Critical Reviews in Oncology Haematology; they are CME and ESMO-MORA accredited. ing and after the live sessions. Questions received before and during the session will be answered during the session directly. Questions received after the sessions will be answered by email. Registration to e-ESO is free but is required in order to provide a high-quality personalised service. www.e-ESO.net Participants are invited to attend the sessions: • live e-grandround: these take place on the second and fourth Thursday of every month at the same time (18.15-19.00 hrs CET) • live e-oncoreview: the first Tuesday of the month at the same time (18.15-19.00 hrs CET) • recorded session: available 24 hours after the live session. Attendants can participate remotely, without a webcam and without appearing in the system. Questions can be sent to our experts before, dur- INTRODUCTION E-LEARNING COURSE REPORTS E-ESO INTRODUCTION E-LEARNING COURSE REPORTS E-ESO ESTRO SCHOOL OF RADIOTHERAPY AND ONCOLOGY 2015 WWW.ESTRO.ORG COMPREHENSIVE QUALITY MANAGEMENT IN RADIOTHERAPY: QUALITY ASSESSMENT AND IMPROVEMENT CANCER SURVIVORSHIP 1 - 4 February 2015 | Turin, Italy 16 - 19 May 2015 | Manila, The Philippines ESTRO/EANM COURSE ON MOLECULAR IMAGING AND RADIATION ONCOLOGY BIOLOGICAL BASIS OF PERSONALISED RADIATION ONCOLOGY 14 - 16 May 2015 | Brussels, Belgium ADVANCED TREATMENT PLANNING NEW! 22 - 25 February 2015 | Madrid, Spain BASIC CLINICAL RADIOBIOLOGY 7 - 11 March 2015 | Brussels, Belgium 30 August - 3 September 2015 | Dublin, Ireland 22 - 24 May 2015 | Seoul, South Korea 8 - 12 March 2015 | Paris, France TARGET VOLUME DETERMINATION: FROM IMAGING TO MARGINS 13 - 16 March 2015 | Amman, Jordan MODERN BRACHYTHERAPY TECHNIQUES 15 - 18 March 2015 | Limassol, Cyprus DOSE MODELLING AND VERIFICATION FOR EXTERNAL BEAM RADIOTHERAPY 14 - 17 June 2015 | Beijing, China PHYSICS FOR MODERN RADIOTHERAPY EVIDENCE BASED RADIATION ONCOLOGY 15 - 19 March 2015 | Barcelona, Spain A CLINICAL REFRESHER COURSE WITH A METHODOLOGICAL BASIS 21 - 26 June 2015 | Moscow, Russia 3rd ESTRO FORUM PRE-MEETING COURSES BRACHYTHERAPY FOR PROSTATE CANCER 24 April 2015 | Barcelona, Spain 28 - 30 June 2015 | Vienna, Austria IMAGE-GUIDED RADIOTHERAPY IN CLINICAL PRACTICE ADVANCED SKILLS IN MODERN RADIOTHERAPY 10 - 14 May 2015 | Prague, Czech Republic 28 June - 2 July 2015 | Copenhagen, Denmark RADIOTHERAPY TREATMENT PLANNING AND DELIVERY BIOLOGY 3 - 5 September 2015 London, United Kindgom NEW! ESTRO/ESOR MULTIDISCIPLINARY APPROACH OF CANCER IMAGING 15 - 17 October 2015 | Brussels, Belgium BEST PRACTICE IN RADIATION ONCOLOGY A FOUR PHASE PROJECT TO TRAIN RTT TRAINERS IN COLLABORATION WITH THE IAEA 19 - 21 October 2015 | Vienna, Austria IMAGING FOR PHYSICISTS IMAGE-GUIDED RADIOTHERAPY AND CHEMOTHERAPY IN GYNAECOLOGICAL CANCER: FOCUS ON ADAPTIVE BRACHYTHERAPY 13 - 17 September 2015 | Leiden, The Netherlands 1 - 5 November 2015 | Utrecht, The Netherlands BASIC TREATMENT PLANNING COMBINED DRUG-RADIATION TREATMENT: BIOLOGICAL BASIS, CURRENT APPLICATIONS AND PERSPECTIVES NEW! 3 - 6 September 2015 | Prague, Czech Republic 8 - 11 June 2015 | Florence, Italy A JOINT COURSE FOR CLINICIANS AND PHYSICISTS 14 - 18 June 2015 | Ljubljana, Slovenia HAEMATOLOGICAL MALIGNANCIES RESEARCH MASTERCLASS IN RADIOTHERAPY PHYSICS MULTIDISCIPLINARY MANAGEMENT OF BREAST CANCER MULTIDISCIPLINARY MANAGEMENT OF HEAD AND NECK ONCOLOGY PARTICLE THERAPY MULTIMODAL CANCER TREATMENT CLINICAL PRACTICE AND IMPLEMENTATION OF IMAGE-GUIDED STEREOTACTIC BODY RADIOTHERAPY 13 - 17 September 2015 | Lisbon, Portugal ADVANCED TREATMENT PLANNING 18 - 22 September 2015 | Lisbon, Portugal MULTIDISCIPLINARY MANAGEMENT OF BRAIN TUMOURS 4 - 6 October 2015 | Turin, Italy IMRT AND OTHER CONFORMAL TECHNIQUES IN PRACTICE 4 - 8 October 2015 | Brussels, Belgium 15 - 18 November 2015 | Vienna, Austria PAEDIATRIC RADIATION ONCOLOGY 19 - 21 November 2015 | Izmir, Turkey BASIC CLINICAL RADIOBIOLOGY ENDORSED BY ESTRO 21 - 24 November 2015 | Brisbane, Australia 4 - 8 October 2015 | Budapest, Hungary QUANTITATIVE METHODS IN RADIATION ONCOLOGY: MODELS, TRIALS AND CLINICAL OUTCOMES MULTIDISCIPLINARY MANAGEMENT OF LUNG CANCER ADVANCED TECHNOLOGIES TARGET VOLUME DETERMINATION FROM IMAGING TO MARGINS 15 - 17 October 2015 | Athens, Greece IMAGING BEST PRACTICE 6 - 9 December 2015 | Brussels, Belgium 6 - 10 December 2015 | India YOUNG ESTRO INTRODUCTION EORTC-ROG MEETING ESTRO YOUNG TASK FORCE MOBILITY REPORT YOUNG ESTRO Welcome to this new issue of the Young Corner. The European Organisation for Research and Treatment of Cancer (EORTC) Radiation Oncology Group (ROG) held its autumn meeting at The Institut Gustave-Roussy, France, and Orit Person, chair of the young group, reports on the YROG-SFjRO joint session that took place during that meeting. CATHARINE CLARK We finish our series of Young Task Force interviews with Jean-Emmanuel Bibault and Wouter Van Elmpt’s answers and we also publish Alexis Dimitriadis’ mobility grant report about his stay at the VU medical centre in Amsterdam. We hope you’ll like this new issue. Catharine Clark and Jean-Emmanuel Bibault INTRODUCTION JEAN-EMMANUEL BIBAULT EORTC-ROG MEETING ESTRO YOUNG TASK FORCE MOBILITY REPORT YOUNG ESTRO Radiation Oncology Group of EORTC SFjRO and YROG joint session: YOUNG RADIATION ONCOLOGISTS PRESENT THEIR RESEARCH AT THE EORTC-ROG MEETING At the Institut Gustave Roussy Villejuif, France ORIT KAIDAR-PERSON INTRODUCTION THOMAS LEROY The European Organisation for Research and Treatment of Cancer (EORTC) Radiation Oncology Group (ROG) held its autumn meeting at the Institut Gustave Roussy, Villejuif, France. During this meeting the Young Radiation Oncologists Group (YROG) held its third session. The YROG is a new working party (WP) within the ROG, which aims to incorporate young radiation oncologists in the work done within the ROG to encourage a new generation of radiation oncologists who are dedicated to clinical research. This session was unique as it was a joint session with the French Society of Young Radiation EORTC-ROG MEETING Oncologists (SFjRO), the young division of the French national society of radiation oncologists. SFjRO, in contrast to the YROG, is a “veteran” group of young radiation oncologists since it has been active for over 11 years in promoting the education and training of the speciality in France. SFjRO organises teaching courses twice a year, delineation workshops, developing advanced learning tools (such as applications for smart phones), has free access to scientific journals, courses and more. SFjRO also has a very active website which maintains an updated database of learning courses, video courses and more [visit http://www.sfjro.fr]. A questionnaire conducted ESTRO YOUNG TASK FORCE MOBILITY REPORT by SFjRO of the motivations for choosing the radiation oncology speciality among the French residents, indicated that the main driver was an interest in innovation, technology, imaging and research. This was a basis for a successful collaboration between these two young groups, YROG and SFjRO, both aiming to inspire the young members. The session moderators were Thomas Leroy, the secretary of SFjRO and Orit Kaidar-Person, the chair of the YROG. The scientific agenda was composed of presentations by young radiation oncologists who showed studies conducted in their institutions on various novel subjects such as intensity-modulated radiation therapy (IMRT) for breast cancer, stereotactic body radiation therapy (SBRT) for hepatic cellular carcinoma, and dosimetric aspects for two irradiation techniques of benign brain tumours. These great presentations stimulated discussions and highlighted the potential benefit of young radiation oncologists joining the ROG and participating in the YROG session. The topics aired during this session will be the backbone of the future clinical trials launched in Europe in the framework of the EORTC. It was also a good example of the importance of the collaboration of the YROG with young national societies such as SFjRO, and having SFjRO members join and participate in the YROG and ROG activities. The YROG sessions are a platform for INTRODUCTION young radiation oncologists to present research proposals, local studies and innovative ideas, and to be noticed in the European arena; joining the ROG activities is an opportunity to work side by side with world leaders in oncology and to take part in the planning and conducting of a wide variety of clinical trials within the EORTC. Fellowship opportunities are also available for young radiation oncologists (EvDS fellowship, for more details please go to the EORTC website). The YROG will also benefit from the experience and expertise of the SFjRO executive committee who have devoted many years to promoting young members. The ROG Paris meeting was highly scientific, included stimulating lectures from three continents, and also an enchanting dinner on a cruise boat on the river Seine. The idea of collaboration between the YROG and other European young national societies also gained the support of ESTRO, thanks to the assistance of ESTRO’s President, Professor Philip Poortmans, and of the Chair of ESTRO’s National Society Committee, Professor Umberto Ricardi, which will undoubtedly lead to a productive collaboration for all. PLEASE JOIN US AT THE NEXT ROG MEETINGS: 12 -13 March 2015 EGAM, Crowne Plaza Hotel Brussels, Belgium 8 -10 October 2015 Las Palmas, Canaries For more details regarding the YROG please go to the EORTC website: www.eortc.org or email: Dr Orit Kaidar-Person, YROG Chair, [email protected] For more details regarding the YROG please go to SFjRO website: www.sfjro.fr Orit Kaidar-Person YROG chair Thomas Leroy Secretary of SFjRO EORTC-ROG MEETING ESTRO YOUNG TASK FORCE MOBILITY REPORT ESTRO YOUNG TASK FORCE (YTF) YOUNG ESTRO Focus on the ESTRO Young Task Force (YTF) Initiated in 2011, the Young Task Force (YTF) is appointed by the ESTRO Board and is involved at governance level. Their mission is to support ESTRO in the development of actions for the benefit of their young col- Interview with Wouter van Elmpt Member of the YTF INTRODUCTION EORTC-ROG MEETING leagues from the radiation oncology area. In each issue, we introduce some of the YTF members so that you get to know your representatives within ESTRO better. Interview with Jean-Emmanuel Bibault Member of the YTF ESTRO YOUNG TASK FORCE MOBILITY REPORT ESTRO YOUNG TASK FORCE (YTF) YOUNG ESTRO INTERVIEW WITH WOUTER VAN ELMPT Member of the YTF PhD Department of Radiation Oncology (MAASTRO) Maastricht University Medical Centre Maastricht, The Netherlands. Email: [email protected] Tell us about your training and your current employment. I studied Applied Physics (Eindhoven, The Netherlands) with a specialisation in Medical Physics. After that I took up a research position at the Department of Radiation Oncology (MAASTRO) at the Maastricht University Medical Centre (The Netherlands) and defended my PhD in 2009 on the topic of treatment verification for advanced radiotherapy. A three-year post-doc at the Maastricht University followed and now I am a senior scientist at MAASTRO supported by a four-year fellowship from the Dutch Cancer Society to study the use of multi-modality imaging for the optimisation of lung cancer treatment. What is your main area of interest? Individualised patient treatment, with a focus on lung cancer. My specific research focuses around molecular imaging, i.e. metabolic and hypoxia imaging, and dose delivery techniques such as dose-painting by numbers/contours. Also treatment response assessment of both tumour and normal tissues using (functional) imaging is one of my key research interests. When did you join ESTRO? In 2004 as a student member to present a poster at the ESTRO meeting in Amsterdam. From that year onwards I have been an In Training member of ESTRO. What does your involvement with ESTRO and the young task force (YTF) mean to you? I would like to connect all the young ESTRO members that have an interest in research. A lot of high quality research is performed in Europe but I think it can be strengthened even more if we combine efforts. Finding other young researchers with similar interests can be used to facilitate collaborations in Europe. Besides that, it is fun to talk and work together with other young ESTRO members. How do you balance research and clinical work? At the moment I can devote the majority of my time to research. However, that does not mean that I am not involved in the clinic. I start and supervise many projects that introduce my research findings in clinical practice. Therefore, a link to clinical work needs to be present. WOUTER VAN ELMPT INTRODUCTION EORTC-ROG MEETING ESTRO YOUNG TASK FORCE MOBILITY REPORT ESTRO YOUNG TASK FORCE (YTF) What advice would you have for new young members entering the world of radiation oncology? Look around you! A lot of enthusiastic people are united in ESTRO, and willing to help you if necessary. Do not be afraid to ask questions if you see a nice presentation at an ESTRO conference or read an interesting article in Radiotherapy and Oncology. THE ESTRO JOB FAIR AT THE 3RD ESTRO FORUM 25 - 26 April 2015 Barcelona, Spain The job fair at the 3rd ESTRO Forum is certainly an opportunity not to be missed by our young colleagues. The job fair is a unique occasion at which to meet people from leading European institutions, offering jobs for young talents in the field of clinical radiation oncology, medical physics, radiation biology as well as radiation therapists. Do not miss this opportunity to discuss your plans for your future in radiation oncology with people from research and clinical departments during this event. Daniela Thorwarth, on behalf of the Young Task Force INTRODUCTION EORTC-ROG MEETING ESTRO YOUNG TASK FORCE MOBILITY REPORT ESTRO YOUNG TASK FORCE (YTF) YOUNG ESTRO INTERVIEW WITH JEAN-EMMANUEL BIBAULT Member of the YTF MD, MSc Department of Radiation Oncology Hôpital Européen Georges Pompidou Paris, France Email: [email protected] Tell us about your training and your current employment. I’ve just taken a new position as Assistant Professor in Paris after five years of residency in Lille and a Master’s Degree in radiobiology at the Gustave Roussy Institute in Villejuif. What is your main area of interest? My main areas of interest include radiobiology, biomarkers, bioinformatics and genomics. I truly believe these tools will open new possibilities in cancer care. I’m also very interested in new technologies such as mobile health IT and social media with several side projects involving programming. When did you join ESTRO? I joined ESTRO during my third semester in 2010 to attend ESTRO 29 in Barcelona. I’ve been involved in ESTRO activities since January 2013 when I became the editor of the Young Corner of ESTRO’s newsletter with Catharine Clark and later joined the Young Task Force of ESTRO. What does your involvement with ESTRO and the young task force (YTF) mean to you? JEAN-EMMANUEL BIBAULT INTRODUCTION I think ESTRO is a great way to meet other European radiation oncology professionals to share our experiences for better patient care. In that perspec- EORTC-ROG MEETING tive, participating in the YTF is a great way to promote exchange between young members. I think the YTF is trying to bring together young ESTRO members and should continue to do so through the use, for example, of digital and online tools. How do you balance research and clinical work? To this day, I’ve either been working in a clinical setting or in a lab. I’ve never had to mix the two. But I guess I’ll eventually have to do it. I might actually enjoy it because it’s a great way to keep variety and interest in one’s everyday tasks. I’ve always been fascinated by the translation of basic research in the clinical field so I can’t wait to make that part of the job. What advice would you have for new young members entering the world of radiation oncology? I’m still a little bit young to be giving advice, but anyway I think the best advice I could give is simply to do what you really like and not force yourself. If you like basic science, clinical research or patient care, there’s plenty to do in each one of these fields. Just pick what you like and go for it. Don’t be shy and don’t hesitate to contact and exchange information with your mentors, fellow residents etc. ESTRO YOUNG TASK FORCE MOBILITY REPORT YOUNG ESTRO MOBILITY REPORT INTRACRANIAL STEREOTACTIC RADIOSURGERY WITH THE NOVALIS TX SYSTEM Alexis Dimitriadis HOST INSTITUTE: VU medical centre, Amsterdam, The Netherlands DATE OF VISIT: 29 September - 10 October 2014 ALEXIS DIMITRIADIS INTRODUCTION Alexis Dimitriadis with his co-workers from the VUmc team First of all, I would like to thank ESTRO for the award of a mobility grant to visit VUmc in Amsterdam. I’m glad to state that the visit not only met but exceeded my expectations. I found the two weeks I spent in Amsterdam extremely beneficial both to my professional role and research interests. I am currently pursuing my PhD and my interests lie in developing the methodology for an end-to-end audit of stereotactic radiosurgery. I am also employed by the St Luke’s Cancer Centre, a department that will be installing a Novalis Tx radiosurgery unit in early 2015. This gave me two reasons for wanting to visit a centre with experience in this field. The VUmc was an ideal destination as it is one of the first centres in Europe to install a Novalis Tx linac. They have accrued substantial experience with it, proven by a series of publications and talks at various con- EORTC-ROG MEETING ferences. The main aims of my visit were to gain a better understanding of the challenges involved in running a radiosurgery programme, and to observe the local quality assurance procedures. I was fortunate that my visit coincided with the delivery of a locally engineered phantom for an end-to-end test, or as the Dutch say “ketentest”. The phantom was specifically designed to be used for stereotactic treatments and I had the opportunity to help perform the first tests with it. In liaison with the radiation technicians, we performed the local stereotactic protocol in acquiring a high resolution CT-scan of the phantom. I then used the treatment planning facilities to delineate four metastatic brain lesions within the “brain” of the phantom. Using the Eclipse system and with the guidance of a planning team, a VMAT plan ESTRO YOUNG TASK FORCE MOBILITY REPORT Plan on phantom Cross section of the phantom showing the dose distribution in the plan created was developed using the two non-coplanar arc technique developed at VUmc: a full 360 arc with the couch at 0˚ and a 180˚ “Mohawk” arc with the couch at 90˚. This plan was then delivered to the phantom and, using EBT3 Gafchromic film in two planes, dosimetric tests were performed in the low dose region between the four high dose areas. The results showed a substantial agreement between the predicted and measured doses in the low dose regions between the metastatic lesions. However, the limited time spent there did not allow for any repeat measurements. Therefore, we can say that even though the results were not conclusive, they revealed the potential of the phantom’s use for such tests and they also were indicative of some minor adaptations that could improve the phantom. My participation in this project also allowed observation of the use of radiochromic film for routine measurements. INTRODUCTION Apart from performing these tests, I observed the treatment of a patient with an arteriovenous malformation from fixation of the stereotactic frame, through angiography, CT-scanning, image fusion, target delineation, treatment planning and treatment delivery. I also participated in quality control measurements using electronic portal imaging devices (EPID). On my final day in The Netherlands it was arranged for me to visit the Utrecht Medical Centre where I had the opportunity to see the radiotherapy department and discuss my research with members of their physics team who have similar interests. Finally, I would like to take this opportunity to convey my gratitude and appreciation to all the people at the VUmc, who, apart from making me feel welcome during my stay, took the time to discuss with me and help me out in any way EORTC-ROG MEETING they could. Special thanks to Johan Cuijpers, Stan Heukelom, Leo Van Battum, Mustafa Zahir, Wenze Van Klink, Omar Bohoudi and Ingrid Kuijper. Alexis Dimitriadis Radiotherapy Dosimetrist St. Luke’s Cancer Centre Royal Surrey County Hospital Guildford, UK [email protected] Postgraduate Researcher Advance Technology Institute University of Surrey Guildford, UK [email protected] ESTRO YOUNG TASK FORCE MOBILITY REPORT BASIC CLINICAL RADIOBIOLOGY 2015 ESTRO SCHOOL LIVE COURSE 7 - 11 March 2015 | Brussels, Belgium BIOLOGY TOPICS · The basic mechanisms of cell death/ survival and the radiation response of tumours and normal tissues. · Formulas of tissue tolerance · The biological basis for current approaches to the improvement of radiotherapy including novel fractionation schemes, retreatment, IMRT, modification of hypoxia, hadron therapy, combined radiotherapy/chemotherapy and biological modifiers of tumour and normal tissue effects. www.estro.org/school > WWW.ESTRO.ORG HEALTH ECONOMICS INTRODUCTION REIMBURSEMENT HEALTH ECONOMICS “The burgeoning cost of health care is a concern in almost every jurisdiction and particularly in the United States where it currently consumes close to 18% of GDP” “Every health care system is shaped by its reimbursement design”. This is the opening sentence of a recently published paper by Cox and colleagues1. The burgeoning cost of health care is a concern in almost every jurisdiction and particularly in the United States where it currently consumes close to 18% of GDP. It has long been recognised that even if the current yearly expenditures on health care are sustainable, the rates of increase seen over the last two decades are not. The authors of this paper discuss this issue against the background of health care reform in the US, which, particularly in the light of “Obamacare” (Affordable Health Care for America Act), is the subject of considerable debate. The authors are medical oncologists who might see the world differently from the radiation community where infrequent large capital items are required as opposed to more frequent but often expensive drug regimens. YOLANDE LIEVENS PETER DUNSCOMBE Yolande Lievens, Peter Dunscombe and Madelon Pijls MADELON PIJLS INTRODUCTION REIMBURSEMENT HEALTH ECONOMICS REIMBURSEMENT PETER DUNSCOMBE INTRODUCTION Funding of radiotherapy, and other health care activities, can be provided in the form of a global budget for a programme or department. Global budgets are loosely coupled to workload, although frequently involve a time lag between volume/complexity increases and the release (or not) of additional funding. A reimbursement system, on the other hand, is a funding mechanism which attempts to directly reflect the volume of activities, including complexity, in somewhat closer to real time. While there is a spectrum of reimbursement models, the extremes are fee-forservice (FFS) and capitation. In their simplest forms, FFS requires every patient-related activity to be identified and billed and capitation provides reimbursement per patient irrespective of complexity and the details of the activities performed. FFS is obviously costly to administer and has a tendency to drive more expensive billable activities, while capitation could lead to treatments that may be sub-optimal in order to keep total costs within the reimbursement limit. The challenge of designing a reimbursement system is to provide the best outcome, in all its dimensions, for patients while controlling costs: i.e. providing value. The authors of the paper under discussion [1], and many others, see some form of bundling or episode payment as a (partial) solution to the current dilemma. Bundling means reimbursement on the basis of expected costs for a clinically-defined episode of care for a set period of time, perhaps from 30 days to a year. Failure to provide a quality service would presumably result in more remedial interventions, such as hospitalisation, the cost of which would have to be covered within the previously negotiated bundle reimbursement, thus promoting quality medicine in some sense. Some form of bundling could also serve to break down the silo mentality encountered in much of medicine, as all the service providers would share the same pot of money and be jointly accountable for the patient outcome. The authors make several arguments for reform of the FFS system. To make FFS workable at all, only certain activities can be identified for reimbursement within the fee schedule. All the other activities, such as phone calls to the patient and informal discussions with colleagues, have to be covered by the “overhead” on the billable service. The authors see this as a shortcoming that has a major impact on the movement towards personalised medicine. Personalised medicine, in their interpretation, includes questioning huge databases and looking for successful treatments for patients with similar profiles to the patient of interest. With no reimbursement for learning the skills and taking the time to personalise medicine, it’s unlikely to be widely adopted. Lack of transparency is another negative aspect of the current FFS system that the authors cite. By transparency, the authors mean knowing both the costs and the benefit or value of a service. Only armed with such information can informed judgements be made on the allocation of scarce resources. With the piecemeal billing of the FFS approach to reimbursement, the actual cost of REIMBURSEMENT an episode of care to a patient will be variable, depending on what diagnostic and therapeutic activities are actually performed for that particular patient, and difficult to quantify as overhead and ancillary support services are somehow incorporated into the billing codes. While methods for calculating the benefit of an intervention, in QALYs or some other metric, are still the subject of debate, in principle it should be possible to get a reasonable handle on costs if an appropriate alternative to FFS were to be implemented. Next, the authors discuss the issue of palliative care. They stress the importance of palliative care, which, for them, starts with a conversation about the goals of treatment and prognosis, and point out that a one-size-fits-all approach may not be appropriate in this context. They then float the idea of “time-based billing” which sounds a lot like fee for service. The main message in this section of the paper seems to be that while palliative care, by any definition, has assumed greater importance in recent years, reimbursement schemes have yet to acknowledge the resource implications. The paper concludes with a description of an initiative by one of the authors, Dr McAneny. She has been promoting the value to the patient of moving as much patient care as possible out of the hospital into the physician’s office, which is cheaper, more acceptable to the patient but, apparently, not adequately reimbursed by the current US FFS system. The implication here is INTRODUCTION that a new payment model should include the full spectrum of services from financial counselling to symptom management to be delivered in a community practice. This paper obviously has a US (and medical oncology) flavour but issues surrounding reimbursement are of concern in every health care jurisdiction. Strategies for containing costs whilst meeting patients’ increasing expectations of quality care should be formulated by the radiation community before key decisions are taken out of our hands to the possible detriment of the patient population we serve. The ESTRO-HERO project has accumulated data on reimbursement systems for radiotherapy in the European countries. Such information will fuel this important discussion and hopefully will support the development of reimbursement strategies that promote the highest quality and most cost-effective care for the radiotherapy patient, in each individual European country. Peter Dunscombe University of Calgary, Calgary, Alberta, Canada REFERENCE 1. Cox, J.V., Ward, J.C, Hornberger, J. C., Temel, J.S. and McAneny, B. L. Community Oncology in an Era of Payment Reform 2014 ASCO Educational Book asco.org/ edbook REIMBURSEMENT INSTITUTIONAL MEMBERSHIP INTRODUCTION THE LAUSANNE UNIVERSITY HOSPITAL INSTITUTIONAL MEMBERSHIP INSTITUTIONAL ESTRO MEMBERSHIP BECOME AN INSTITUTIONAL MEMBER The possibility of signing up groups of five people represents a very interesting economical opportunity, whilst benefitting from all regular membership advantages as well as a few extra advantages created just for your institute. The packages include various membership types and a minimum of thee disciplines need to be represented. Detailed information can be found on the website: www.estro.org The Institutional membership category has been especially designed for European hospitals, clinics or other institutions that seek to continuously develop and support their radiotherapy and oncology professionals. In this Corner we invite our institutional members to provide you and us with some feedback on their experience and institute. This month we have invited Jean Bourhis, Chair of the Radiation Oncology Department of the Lausanne University Hospital in Switzerland to introduce his institute. Contact: [email protected] INTRODUCTION THE LAUSANNE UNIVERSITY HOSPITAL INSTITUTIONAL MEMBERSHIP THE LAUSANNE UNIVERSITY HOSPITAL Lausanne, Switzerland Number of ESTRO institutional members: 40 Spokesperson: Professor Jean Bourhis, Chair of the Radiation Oncology Department www.chuv.ch/radio-oncologie for medical physics: www.chuv.ch/ira Radiation Oncology / Biology and Medical Physics at Lausanne University Hospital How would you describe the radiation oncology department of your institute? JEAN BOURHIS INTRODUCTION The Radiation Oncology Department of the Lausanne Cancer Centre treats a little over 1,000 new patients per year and has 15 medical staff (junior and senior) 20 RTTs, two nurses and 12 physicists (junior and senior, under the leadership of Dr Raphaël Moeckli), and five biologists (under the leadership of Dr. Marie-Catherine Vozenin). A majority of us (40) are ESTRO members through the institutional membership. What are the main areas of specialisation in your department? The Radiation Oncology Department is very well integrated in the newly created Lausanne Cancer Centre, where the development of synergies between the sub-specialities of oncology is a major priority. The Radiation Oncology Department is in charge of treating all types of tumours and some clinical areas are very strong due to excellent connections with our surgical colleagues, such as lung, head and neck, sarcoma, brain/spine and gynaecology. THE LAUSANNE UNIVERSITY HOSPITAL What are the main achievements so far and the main challenges on your daily work and for the future? 3D conformal radiotherapy is no longer used in our institute and has been replaced by either IMRT/ IGRT, 4D-RT or SBRT for all our patients. SBRT is used increasingly in the context of metastatic patients, due to its excellent cure rate potential with minimal, if any side effects. All this can be provided to our patients through a CyberKnife, two Tomotherapies (along with a strong partnership with Accuray) a Gammaknife and a Synergy (Elekta). Brachytherapy is still used for some cases. PET-CT or 4D PET-CT are used for planification purposes for many of our patients. We have recently launched under the same umbrella and under the direction of Dr. Marie-Catherine Vozenin two radiobiological laboratories: one is dedicated to functional imaging and adaptive radiotherapy (with micro-PET and X-Rad 225 Cx 3D irradiator), and the other one is focused on new therapeutics and the combination of radiation therapy with molecular targeted drugs or immunotherapy (in collaboration with the Lausanne branch of the Ludwig Institute). Is your department currently undertaking some studies or clinical trials that you would like to share with the ESTRO community? We would be delighted to share with other centres in the ESTRO community some of our current clinical research programmes. These are focused INTRODUCTION on SBRT (ex: dose escalation, five fractions in prostate cancers, or generating EBM level 1 on SBRT in oligo-metastatic patients) or SBRT combined with various types of immuno-stimulation. Functional imaging and adaptive radiotherapy are also important avenues for potential collaboration (we have easy access to many types of tracers). Along with the Swiss Institute of Bioinformatics, we have launched a programme to design new drugable molecules that could be of interest for combinatory approaches and that are first tested in our lab, and later transferred in patients. We have also created some innovations that are about to be shared with the ESTRO community, for example the “supergating”, which can fully control lung motion (Dr Peguret/Professor Ozsahin). Other examples will follow relatively soon, for example we are testing a totally new and promising radiation therapy prototype... Stay tuned! What attracted you to apply for an institutional membership and why is it important for your institute that its staff members are part of ESTRO? The newly created radiobiology team under the leadership of Dr. Marie-Catherine Vozenin (centre of the picture) In your opinion, what additional benefits would be useful as part of the institutional membership package? This is an excellent initiative created in 2013, and we have a very positive view on it. Congratulations to Vincenzo Valentini (ESTRO past President), Alessandro Cortese (ESTRO CEO), Dirk Verellen (ESTRO membership officer) and the ESTRO Board who promoted it. What a strange question! ESTRO is “The” European Radiation Oncology Society . . . Could we imagine radiation oncology in Europe without a strong ESTRO . . . and not being part of it? The institutional membership is probably the easiest and most practical way to bring most of our department within the ESTRO network. THE LAUSANNE UNIVERSITY HOSPITAL NATIONAL SOCIETIES INTRODUCTION SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES NATIONAL SOCIETIES Welcome to another issue of the National Societies Committee (NSC) Corner. In this issue, the NSC presents a critical summary of results from a survey on the relationship of ESTRO with the national societies (NS). “National societies on the role of ESTRO and the National Societies Committee: on the right path …” These results are part of a broader survey performed by Joana Poggemann in June 2014 as a case study for her International Business Bachelor thesis on “Value creation in non-profit organisations: a stakeholder approach” during her internship at ESTRO. PANAGIOTIS PAPAGIANNIS We would like to thank Joana, as well as NS representatives that responded, once more for the opportunity to refine the NSC role and road map. Panagiotis Papagiannis Member of the ESTRO national societies committee Medical School, University of Athens Athens, Greece If your national society would like to share views on these topics, please contact the National Societies Committee via Chiara Gasparotto: [email protected] INTRODUCTION Read about the Belgian national societies for radiation therapists in the RTT Corner on p 56> SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES NATIONAL SOCIETIES ESTRO is a strategic partner: 24.56% SUMMARY OF RESULTS FROM A SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES (NS) PANAGIOTIS PAPAGIANNIS INTRODUCTION ESTRO is a partner: 24.56% ESTRO is important to us as one of our external points of reference: 47.37% ESTRO is not important to us: 1.75% Other: 1.75% Fig 1. Replies to the survey question: Describe the relationship you have with ESTRO The degree of participation is an immediate and unambiguous indicator. The response rate for this survey was 45%. This is typical for NS responses to questionnaire-based surveys. While adequate, this figure certainly implies that there is room for improvement. Especially considering that, while NS involvement is strong in annual meetings, it has been quite weak so far in terms of contributing or stimulating discussion in this Corner. So the NSC would like to take the opportunity to stress the importance of a two-way communication once more. The NS deem their relationship with ESTRO to be important. A closed-form question asking the NS to define their relationship with ESTRO was included in the questionnaire and replies indicate that ESTRO serves mainly as one of the NS’s external points of reference, rather than a partner (fig 1). The non-exclusiveness of ESTRO in this regard is understood in view of the currently available means for swift and effortless information gathering. The NS also acknowledge ESTRO as a provider of education and technology support, as well as a force in acting towards international integration. The positive response to the question of whether NS members feel included in ESTRO was an overwhelming 89.5%. This, however, is SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES by strengthening the communication and cooperation with the NS. This need is also supported by the fact that ESTRO communicates with the NS more frequently than they do with ESTRO. No: 4% Yes: 96% Fig. 2a. Replies to the survey question: Is the information provided by ESTRO sufficient? > Education and Training, especially grant possibilities > Events and Congresses > Oncopolicy, standards and regulations > Research, developments, updates on new techniques A selection of the open comments to the question: On what matters would you like to be informed? explained to a certain degree by the fact that most NS members are also ESTRO members as individuals. According to the constructive comments accompanying negative responses, the NS are more readily accessible than ESTRO and also better accommodate issues associated with daily practice. The latter is a field where the NSC is called to act upon INTRODUCTION Undoubtedly, the information provided by ESTRO is deemed sufficient by the NS (fig 2a). Most importantly, the NSC ranks high in the list of information channels on ESTRO matters, following the ESTRO office, newsletter and website (fig 2b). The list of topics on which NS prefer to be informed about, mirrors the NS expectations from ESTRO, as well as the main points of the NSC agenda. The latter focuses on: communication (newsletter Corner, annual meetings, support of HERO and results dissemination to NS), education (NS feedback on annual planning, promoting/improving attendance, links with other European education and training initiatives), support of young members (promoting the establishment and cooperation of young societies within NS), continuing personal and professional development (core curricula, professional standards, training harmonisation, link to ACROP and oncopolicy), and quality. While a rewarding 83% believes that the introduction of the NSC has improved the communication between ESTRO and the NS, only 69% of the NS feel better integrated within ESTRO after the committee’s introduction. This is interpreted as a clear need for further communicating the NSC agenda and advancing the pace at which it is realised. According to replies to a closed question on the NS’s organisational goals, the NS’s priorities are the development of high quality standards, fostering adoption of standards of care, and science dissemination (fig 3). Survey results also indicate the strong belief of NS that information exchange at the European level is necessary to facilitate health research in radiotherapy and oncology as well as to support lobbying activities (fig 4). It is worth noting that NS share the belief that health care is not a national issue, and this is also evident in the balance between the perceived importance of lobbying at national and international levels. 0 10 20 30 40 50 National Societies Committee/ NSC contact person ESTRO Office ESTRO Website ESTRO Newsletter ESTRO Flash Other Fig. 2b. Collection of the open replies to the question: Who informs you on ESTRO matters? SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES NATIONAL SOCIETIES PRIORITIES It does not fit to our goals. (1) It is important but it It is one of our most is not one of our preimportant goals. (3) eminent goals. (2) Σ % Σ % Σ % Ø ± Dissemination of science 1x 1,92 20x 38,46 31x 59,62 2,58 0,54 Development of high quality standards - - 7x 13,46 45x 86,54 2,87 0,34 Foster adoption of standards of care - - 15x 28,85 37x 71,15 2,71 0,46 Health and economics 4x 7,69 36x 69,23 12x 23,08 2,15 0,54 Dissemination and adoption of European Core Curricula 2x 3,85 25x 48,08 25x 48,08 2,44 0,57 EU policy monitoring and intelligence gathering 5x 9,62 29x 55,77 18x 34,62 2,55 0,62 This corroborates the currently favoured action plan wherein information is provided from ESTRO to NS for them to act at a national level, and collected by ESTRO from NS to lobby in the interest of the radiation oncology field at an international level. Fig. 3. Replies to the survey question: Please rate if your organisational goals correspond to the following. NECESSITY OF INFORMATION EXCHANGE Because it facilitates lobbying activities on a European Level Because it enables health research in radiotherapy and oncology Does not make sense as health care is a national issue Is too much of an effort 0% 5% 10% 15% 20% 25% 30% 35% Continuous development and improvement of RT: 18% Expectations arising from ESTROs position in Oncopolicy on EU level More acces to resources and support: 24% More visibility and activity within ESTRO: 12% Other 0 10 20 30 40 50 Fig.4. Replies to the survey question: Exchange of data, databases, guidelines and best practices at European Level is necessary... (more than one answer is possible) INTRODUCTION A strong dialogue: 32% Fig. 5. Collection of the open replies to the question: What do you expect from the collaboration with ESTRO? SURVEY ON THE RELATIONSHIP OF ESTRO WITH THE NATIONAL SOCIETIES ESTRO CONFERENCES INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ESTRO CONFERENCES “It appears that the need to build bridges between disciplines is a concept that many of you have found appealing and useful” A NEW YEAR WITH A PROMISING CONGRESS IN VIEW… We are very pleased to announce that 1,637 abstracts have been submitted for the 3rd ESTRO Forum – a record for this congress. It appears that the need to build bridges between disciplines is a concept that many of you have found appealing and useful. There are a lot of radiation oncology events to look forward to in the first part of 2015. In the following pages, we introduce the next Wolfsberg meeting; this meeting, initiated in 1997 and organised in scientific collaboration with ESTRO, brings together both experienced as well as young basic and clinical scientists from radiobiology and radiation oncology disciplines to discuss the newest developments in molecular radiation biology oncology. Do not miss the call for applications for the Varian - Juliana Denekamp award. The next head and neck oncology event that should not be missed in early 2015 is ICHNO, the multidisciplinary conference co-organised by ESTRO, European Head and Neck Society (EHNS) and European Society for Medical Oncology (ESMO). We hope to see you in Nice next month. AGOSTINO BARRASSO ESTRO Congress manager ERALDA AZIZAJ ESTRO Programme manager Finally, we report on some of the 2014 conferences: EMUC in Lisbon, with a report from the ESTRO representatives on the scientific committee, as well as the view from an ESTRO member; and the EHNS conference in Liverpool. The latter is the opportunity to give an update on the “Make sense” campaign, to raise awareness on head and neck cancer among the general public and the healthcare community in Europe. We wish you an excellent 2015. Agostino Barrasso and Eralda Azizaj INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ESTRO CONFERENCES FOCUS ON NEXT ESTRO CONGRESSES 14TH INTERNATIONAL WOLFSBERG MEETING 3RD ESTRO FORUM 24 - 28 April 2015 Barcelona, Spain 20 - 22 June 2015 Ermatingen, Switzerland 5TH ICHNO International Conference on Innovative Approaches in Head and Neck Oncology 12 - 14 February 2015 Nice, France INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES EUROPEAN CANCER CONGRESS 25 - 29 September 2015 Vienna, Austria FOCUS ON PAST ESTRO CONGRESSES CLINICAL 24 - 28 April 2015 Barcelona, Spain PHYSICS BRACHYTHERAPY RADIOBIOLOGY RTT INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 3rd ESTRO Forum ESTRO CONFERENCES FIVE MEETINGS WITH OUTSTANDING SCIENTIFIC PROGRAMME 3rd ESTRO Forum 24 - 28 April 2015 Barcelona, Spain The 3rd ESTRO Forum will provide a wonderful opportunity to explore innovations and the latest advances in radiation oncology. Five meetings, each offering an outstanding scientific programme, will be hosted in parallel under its umbrella: • Clinical and translational meeting • Biennial physics meeting • GEC-ESTRO-ISIORT meeting • RTT meeting • PREVENT and TARGET meetings Placing interdisciplinarity under the spotlight, clinicians, physicists, brachytherapists, radiobiologists and radiation therapists (RTTs) will also find, in addition to the five meetings, a broad range of interdisciplinary sessions in which they can participate to explore topics of interest to all. ABSTRACTS IN FIGURES 1,637 abstracts submitted, an increase of 39% compared to the 2nd ESTRO Forum in 2013. The number of abstracts submitted per track is in the table below. IMPORTANT DATES Late registration deadline: 24 March 2015 Desk registration: from 25 March 2015 INTRODUCTION 2015 - Clinical and translational meeting 594 2015 - Biennial physics meeting 2015 - RTT meeting 2015 - GEC-ESTRO 2015 - ISIORT meeting 2015 - PREVENT & TARGET meeting 2015 - 3rd ESTRO Forum TOTAL 630 197 133 31 52 1637 FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 3rd ESTRO Forum ESTRO CONFERENCES Clinical and translational meeting HIGHLIGHT TOPICS We can expect a broad range of science during these five days. Below is an overview of the topics for each meeting. • Palliative care, including a report of the consensus meeting • Individualisation: to the cancer or to the patient? •Lung cancer: how radiation therapy can improve the outcome of SCLC •Lung cancer, NSCLC: treatment intensification and individualisation •Regional radiation therapy in breast cancer •Breast cancer: technical issues for the clinician •HPV and cancer: impact on radiation therapy •Management of HPV-negative head and neck cancer •Organ sparing in bladder cancer •Imaging for radiation therapy in prostate cancer •Sequence of radiation and systemic therapy in rectal cancer. Physics meeting •From 4D imaging to 4D delivery •MR-only workflow in external-beam radiotherapy •Proton therapy practical and advances •Radiobiology on particle therapy •Risks of hypo-fractionation •Planning strategies for SBRT INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES •Innovations in functional imaging for radiotherapy •Imaging to predict toxicity and tumour control •Molecular radionuclide therapy and external beam radiotherapy •Secondary cancer: measuring / estimating organ doses and models of prediction •Clinical and genetic factors in dose-volume models of side-effects •Geometric uncertainties •Overview of recent detectors •Detector response in small photon fields •Nanodosimetry •Treatment planning improvements •Application of Monte Carlo methods in radiation treatment planning •Role, clinical application and validation of deformable image registration and dose mapping tools •Low and medium energy radiotherapy •Research in the field of medical physics •Have we reached the technology edge in radiation therapy? GEC-ESTRO-ISIORT meeting •State-of-the-art breast brachytherapy •QA of treatment planning and delivery in image-guided brachytherapy FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 3rd ESTRO Forum •Clinical outcome of 4D brachytherapy in cervix cancer •Role of brachytherapy and contact X-ray in rectal cancer •Focused and focal therapy via brachytherapy in prostate cancer. •Immunotherapy and radiotherapy •Tumour metabolism and radioresistance •High-throughput biological screens and translation to new targets •New targets and evaluation in model systems and early trials. PREVENT Meeting RTT meeting Prediction, Recognition, EValuation, and Eradication of Normal Tissue effects of radiotherapy •Creating uncomplicated cures in oncology – a paradigm shift •Combination therapy and new mechanisms regulating toxicity in the gut •Combination therapy and new mechanisms regulating toxicity in the heart •Biomarkers of normal tissue toxicity •Evaluating toxicity of targeted agents •Targeted therapy, stem cells, and normal tissue toxicity. TARGET Meeting Targeted therapy and personalised medicine in radiation oncology •Challenges of combining targeted therapy with radiotherapy •Using imaging to assess biomarkers of biological response INTRODUCTION •Advanced technology assessment and health economics •Adaptive radiation therapy •Future of radiation oncology. •IGRT, margin calculation and minimising treatment volumes •Advanced treatment planning techniques •A site-specific symposium on breast cancer •Proton therapy •MRI imaging throughout the treatment chain. Interdisciplinary track •Tumour biology for treatment planning and response evaluation •Paediatrics •Elderly •Psycho-social aspects of radiation therapy •Databases and data-mining •Risk management •Stereotactic ablative radiotherapy •Re-irradiation, including a session on hyperthermia •Particle therapy FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 3rd ESTRO Forum ESTRO CONFERENCES HIGHLIGHTS OF SESSIONS The chairs of the five meetings have selected for you some topics, sessions and speakers that are not to be missed… Clinical and translational meeting Physics meeting Saturday 25 April 2015 | 16.45 Symposium on patient individualisation versus cancer individualisation Patient perspective of quality. patient-reported outcomes versus physician reported outcomes Kathrin Kirchheiner (AT) Saturday 25 April | 8.45-10.00 Symposium on MR-only workflow in external-beam radiotherapy Full integration of MRI in the work flow of external-beam radiotherapy Lars Olsson (SE) Monday 27 April 2015 | 8.00-8.40 Teaching lecture on regional nodes radiotherapy in early breast cancer Brigitte Offersen (DK) speaker Saturday 25 April | 8.45-10.00 Symposium on proton therapy Current developments in proton and ion beam production and delivery Oliver Jäkel (DE) Monday 27 April 2015 | 14.45 Symposium on HPV and cancer and radiotherapy (Head and neck, cervix, vulva, anal) How come that HPV status has an effect on radiotherapy and is it true for all tumour entities? Marie-Catherine Vozenin (CH) Sunday 26 April | 8.45-10.00 Symposium on nanodosimetry Requirements for multiscale models of radiation action – activities in EU projects nano-IBCT and BioQuaRT Hans Rabus (DE) Tuesday 28 April 2015 | 9.15-10.30 Symposium on prostate: use of imaging for treatment planning Local or focal dose prescription Barbara Jereczek-Fossa (IT) INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 3rd ESTRO Forum GEC-ESTRO-ISIORT meeting Saturday 25 April | 14:45-16:15 Symposium on clinical outcome of image guided brachytherapy in cervical cancer Clinical impact of IGABT in cervical cancer Richard Pötter (AT) Sunday 26 April | 8:45-10:00 Symposium on role of brachytherapy and contact X-ray in the treatment of rectal cancer Role of contact x-ray brachytherapy (CXB) for rectal cancer: current status and Challenges Jean-Pierre Gérard (FR) Sunday 26 April | 8:45-10:00 Symposium on focused and focal therapy via brachytherapy in prostate cancer Focal boosts: the best of both worlds? Roberto Alonzi (UK) PREVENT and TARGET meeting Saturday 25 April | 14.45 Symposium around organs / combination therapy: heart Ischemic heart disease after radioptherapy Sarah Darby (UK) Monday 27 April 2015 | 8.45 Symposium on biomarkers - using imaging to assess biology Imaging biology in the cancer patient Kevin Brindle (UK) Monday, 27 April 2015 | 14.45 Symposium on immunotherapy and radiotherapy Radio-immunotherapy of cancer: therapeutic efficacy, underlying mechanisms and potential applications Jacques Neefjes (NL) RTT meeting BREAST Sunday 26 April | 8.00-08.40 Teaching lecture on current overview of radiotherapy for breast cancer Philip Poortmans (NL) Sunday 26 April | 8.45-10.00 Symposium on current issues in breast radiotherapy The symposium will include a presentation on psychosocial aspects of breast cancer from a patient's point of view Carmen Boronat (ES) PROTON THERAPY Monday 27 April | 8.00-08.40 Teaching lecture on introduction to proton therapy Håkan Nyström (SE) Monday 27 April | 8.45-10.00 Symposium on proton therapy, from rationale to planning and delivery Treatment planning for proton therapy – a challenge for the whole team I. Kristensen (SE) INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES International Conference on innovative approaches in HEAD & NECK ONCOLOGY 12 - 14 February 2015 Nice, France INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 5th ICHNO ESTRO CONFERENCES KEYNOTE LECTURES 5th ICHNO 12 - 14 February 2015 Nice, France Jointly organised by ESTRO, the European Head and Neck Society (EHNS) and the European Society of Medical Oncology (ESMO), the biennial international conference will focus on multidisciplinarity and innovation in the treatment of head and neck cancers. Of special interest are the sessions on randomised trials, the debates and also the sessions mimicking a tumour board. Thursday 12 February 2015 | 13.15-13:45 The evolving role of surgery in the treatment of head and neck cancer Randal Weber (USA) Prof Randal S. Weber Chair of the Department of Head and Neck Surgery University of Texas MD Anderson Cancer Center Houston, USA Randal S. Weber, M.D., F.A.C.S., is a renowned surgeon and expert in the treatment of patients with head and neck cancer. He is Chairman of the Department of Head and Neck Surgery, with a joint appointment as Professor, Department of Radiation Oncology, at The University of Texas MD Anderson Cancer Center in Houston, Texas. He is the recipient of the John Brooks Williams and Elizabeth Williams Distinguished University Chair in Cancer Medicine. A leader in healthcare INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES initiatives to improve cancer care, Dr Weber has been instrumental in the establishment of performance-driven processes and evidence-based medicine for patients with head and neck cancer. He is active in clinical research investigating various head and neck cancers and is a pioneer in the use of organ-sparing oncologic techniques. Highly sought after for his expertise and professional insights, Dr Weber has been the guest lecturer and visiting professor on more than 80 occasions in the United States and internationally and has led numerous courses and seminars. Dr Weber was honored as the Hayes Martin Lecturer and recipient of the Distinguished Service Award at the April 2011 meeting of the American Head and Neck Society. He has served as President of the Society of University Otolaryngologists–Head and Neck Surgeons, the American Radium FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 5th ICHNO Thursday 12 February 2015 | 13:45-14:15 Novel opportunities in cancer immunotherapy George Coukos (CH) Society, and the American Head and Neck Society. He is currently a Director and President-elect of the American Board of Otolaryngology and past Chair of the Head and Neck Surgery Committee of the Radiation Therapy Oncology Group. Dr Weber is a prolific author whose works include scientific articles, book chapters, and textbooks. He is the immediate past Editor in Chief of Head & Neck: Journal for the Sciences and Specialties of the Head and Neck, is an Associate Editor for Annals of Surgical Oncology, and serves on the editorial boards of American Journal of Rhinology; Clinical Medicine Insights: Ear, Nose and Throat; and Head & Neck. INTRODUCTION Prof George Coukos Head of the Ludwig Institute for Cancer Research at the University of Lausanne Director of the Swiss Cancer Center Lausanne, Switzerland George Coukos obtained his MD in 1986 at the University of Modena and his PhD in 1991 at the University of Patras. He completed training in obstetrics and gynaecology at the University of Modena in 1991. He did a post-doc at the University of Pennsylvania in Philadelphia, USA, in cell biology (1991-1994), and he completed residency training in obstetrics and gynaecology (1994-1997) and fellowship training in gynaecologic oncology (1997-2000) at the University of Pennsylvania. In 2000 he became Assistant Professor at the University of Pennsylvania. He became Associate Professor in 2006 and Full Professor in 2010. In 2007, George Coukos founded and directed the Ovarian Cancer Research Center at the University of Pennsylvania, and served as Associate Director of the Division of Gynecologic Oncology. He relocated to FOCUS ON NEXT ESTRO CONGRESSES Switzerland in 2012, to become Director of the new Department of Oncology at the University Hospital of Lausanne (CHUV-UNIL) in 2013. He is also the head of the Ludwig Institute for Cancer Research at the University of Lausanne (LICR@UNIL) and Director of the Swiss Cancer Centre, Lausanne. Prof. Coukos is interested in elucidating fundamental mechanisms in the tumour microenvironment (TME) that determine the fate of antitumour immunity, focusing on the study of the deregulation of tumour-infiltrating lymphocytes (TILs). These studies are expected to yield novel pharmacologic approaches to restore antitumour immunity as well as novel methodologies to select and expand TILs for adoptive therapy. He is also involved in the study of the tumour vasculature as a barrier to effective T cell infiltration in many tumours, but also as a potential target for therapy. Prof. Coukos is pursuing T cell engineering approaches as a means of addressing the deregulation of T cells in the TME, and redirecting them against relevant tumour targets, including the vasculature, with the ultimate goal of translating basic discovery to the clinic. FOCUS ON PAST ESTRO CONGRESSES ESTRO 29 April - 3 May 2016 Turin, Italy INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 14th International Wolfsberg Meeting ESTRO CONFERENCES 14TH INTERNATIONAL WOLFSBERG MEETING on Molecular Radiation Biology/Oncology 20 - 22 June 2015 Wolfsberg Conference Centre Ermatingen (Lake Constance), Switzerland In collaboration with ESTRO The International Wolfsberg Meeting started in 1997 and has been organised since 2005 in collaboration with ESTRO. The meeting brings together both experienced, as well as young, basic and clinical scientists in the disciplines of molecular and cell biology, tumour and normal tissue biology, radiobiology and radiation oncology, to discuss the newest developments that are most likely to have the greatest impact on the development of future treatment strategies in radiation oncology. Topics to be discussed: DNA repair and radiation-induced signalling cascades; molecular and micro-environmental aspects of tumour and radiation biology; biomarkers and targeting strategies for radiation oncology. Keynote speakers invited: IMPORTANT DATE Abstract submission deadline: 26 January 2015 INTRODUCTION Randall J. Kimple, Madison (USA), Ira-Ida Skvortsova (Innsbruck, Austria), Karen E. Knudsen (Philadelphia, USA), Amato J. Giaccia (Stanford, USA), Michele De Palma (Lausanne, Switzerland), Lars Zender (Tübingen, Germany), and Dan G. Duda (Boston, USA). More information: www.wolfsberg-meeting.com Contact: [email protected] FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES 14th International Wolfsberg Meeting VARIAN-JULIANA DENEKAMP AWARD 2015 Call for applications The VARIAN-Juliana Denekamp Award, established in 2005 by ESTRO, honours the great and dearly-missed European radiobiologist Professor Dr Juliana Denekamp. This award is sponsored by VARIAN Medical Systems, Switzerland. In concordance with the outstanding scientific achievements of Prof Denekamp and her enthusiasm for promoting young talent, the award will be given to young scientists (junior radiobiologists/radiotherapists) who, at a very early stage in their career, have demonstrated excellence and passion for biologically-driven cancer research relevant to radiation oncology, and who are likely to assume a scientific leadership role in this field in the future. Born in 1943, Prof Denekamp grew up in south Wales, UK. She studied zoology and botany at the University of London and received her PhD at the Royal Postgraduate Medical School, Hammersmith Hospital, London, in 1968. Prof Denekamp was a leading international scientist in radiation biology applied to radiotherapy, a field now called translational research in radiation oncology. Between 1988 and 1994 she was director of the Gray Laboratory, UK. Thereafter, she was appointed as INTRODUCTION a Professor of Translational Research at the Umea University, Sweden, a position that she filled very actively both as researcher and teacher until her much too early death in June 2001. The VARIAN-Juliana Denekamp Award is a single prize of €2,500 which is awarded on the occasion of the International Wolfsberg Meeting on Molecular Radiation Biology/Oncology in collaboration with ESTRO in uneven years. In 2015, the award will be presented during the 14th International Wolfsberg Meeting to be held at Wolfsberg Castle from 20-22 June 2015. Criteria for eligibility are: • Candidates should be ESTRO members. • Candidates should be no older than 36. Exceptions will be made for female applicants who have interrupted their research for pregnancy/ maternity reasons – in this case the maximum age is fixed at 40. • Candidates should have published at least two to three, first author, high-quality publications on a particular topic in the field of biologically-driven cancer research relevant for radiation oncology. FOCUS ON NEXT ESTRO CONGRESSES Candidates should submit a curriculum vitae, including a list of publications and the two or three articles published on one particular topic. If the articles were not published in English, an English summary (max two pages) should be submitted. Deadline for application is 16 February 2015 Applications should be addressed to: Eralda Azizaj ESTRO Scientific Programme Manager ESTRO Office Rue Martin V 40 1200 Brussels, Belgium Tel: +32 2 775 93 40 Fax: +32 2 779 54 94 E-mail: [email protected] FOCUS ON PAST ESTRO CONGRESSES INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON NEXT ESTRO CONGRESSES European Cancer Congress ESTRO CONFERENCES 18th ECCO - 40th ESMO EUROPEAN CANCER CONGRESS The European Cancer Congress will combine the efforts of all partner organisations to continue positioning multidisciplinarity as the way forward for improving the prevention, diagnosis, treatment and care of cancer patients – placing the patient at the heart of all our efforts and discussions. KEY DATES Reinforcing Multidisciplinarity • 26 January 2015: Abstract submission opens 25 - 29 September 2015 Vienna, Austria • 28 April 2015: Abstract submission deadline In collaboration with ESTRO • 7 April 2015: Early rate registration deadline • 29 April 2015: Fellowship grant application deadline • 22 July 2015: Late breaking abstract submission opens • 4 August 2015: Regular rate registration deadline • 5 August 2015: Late breaking abstract submission deadline • 18 September 2015: Late rate registration deadline More information: www.europeancancercongress.org/en > Registration: www.europeancancercongress.org/Registration > INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ESTRO CONFERENCES INTRODUCTION FOCUS ON PAST ESTRO CONGRESSES EMUC ECHNO 2014 13 - 16 November 2014 Lisbon, Portugal 24 - 26 April 2014 Liverpool, UK FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES EMUC ESTRO CONFERENCES REPORT BY THE ESTRO REPRESENTATIVES ON THE SCIENTIFIC COMMITTEE EMUC 6th European Multidisciplinary Meeting on Urological Cancers 13 - 16 November 2014 Lisbon, Portugal MARCO VAN VULPEN INTRODUCTION VINCENT KHOO The sixth European Multidisciplinary Meeting on Urological Cancers (EMUC) took place in Lisbon from 13-16 November 2014. More than 1,300 professionals from all over the world, involved in the management of urological cancers, gathered to discuss recent achievements in the field. The number of participants had increased by more than 50% since the previous year’s EMUC in Marseille, as the EMUC meeting seems to be increasingly appreciated. This increase can probably be explained by the growing need for a multidisciplinary approach in urological cancer FOCUS ON NEXT ESTRO CONGRESSES care. The attendees consisted of a broad range of professionals: urologists (approximately 50%), radiation oncologists (20%), medical oncologists (20%), radiologists, pathologists, trainees, physician assistants and other professions (10%). The faculty represented the major societies involved in urological cancers: ESTRO, EAU, ESMO, ESUP, ESUR and ESUI. The conference was entitled “Multidisciplinary Consensus on the Management of Urological Malignancies”. Around 200 abstract were FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES EMUC presented during oral sessions or displayed as posters. The format featured state-of-the art lectures, practice-oriented case discussions with voting and debates over the most controversial aspects in everyday clinical practice. The facility to text questions and comments to the faculty by keypad enabled real-time interaction with the audience. Further, there were several voting rounds, before and after presentations, which in some cases resulted in changed opinions. These interactions provided a better understanding of each other’s perspectives. Several sessions were of great interest to the radiation oncology community. Albert Bossi had a very interesting presentation on the high level of quality control in radiotherapy. In the bladder cancer management section, Robert Huddart discussed the options for bladder preservation. This was concluded generally to be a very promising treatment option, which should be considered more in clinical practice. In the session on the “best of journals, radiotherapy part”, David Dearnaley’s Lancet Oncology paper on the survival outcome of the MRC RT01 randomised trial on dose escalation was discussed, together with the forthcoming results of the ConcepT trial, a randomised trial between active surveillance, radical prostatectomy and external beam radiotherapy. INTRODUCTION In localised kidney cancer, Gert de Meerleer debated the pros and cons of using radiotherapy as a kidney-sparing approach. At the end of this session several attendees changed their opinion to considering SBRT as a future option to treat small renal masses. Riccardo Valdagni gave an overview on the possibilities for predicting and preventing radiation-induced toxicity. Marco van Vulpen discussed the possibilities and pitfalls of performing (focal) salvage after a previous radiotherapy treatment in prostate cancer and addressed the need for a multidisciplinary approach in this topic. In the section on very high-risk prostate cancer, Ofer Yossepowitch discussed the current standard of the combination of external beam radiotherapy and hormonal treatment. Also, the role of radiotherapy in penile cancer and testicular cancer was discussed during the conference. All speakers pleaded for the more direct involvement of radiation oncologists in multidisciplinary decision-making for patients. Translational and basic science topics were also addressed during the various sessions of the meeting. A Hands-On-Training (HOT) session was presented by Carl Salambier on prostate delineation using CT and MRI. By using the ESTRO FAL- FOCUS ON NEXT ESTRO CONGRESSES CON software, prostate examples were delineated online and discussed in a lively fashion by the group. The next EMUC meeting will take place in Barcelona, Spain, from 12-15 November 2015. This meeting promises to review developments in management of the fast-changing practice of urological cancers. These developments are only possible as part of a multidisciplinary approach. This is evolving and gaining strength year by year in EMUC in an interactive way... So please block your agenda for the 7th EMUC in Barcelona. Marco van Vulpen Radiation oncologist UMC Utrecht Utrecht, The Netherlands Vincent Khoo Clinical oncologist Royal Marsden Hospital, London, UK In collaboration with Philip Poortmans ESTRO President FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES EMUC ESTRO CONFERENCES REPORT BY A PARTICIPANT AND ESTRO MEMBER EMUC 6th European Multidisciplinary Meeting on Urological Cancers 13 - 16 November 2014 Lisbon, Portugal For radiation oncologists with a specific interest in urological cancer, the yearly European Multidisciplinary Meeting on Urological Cancers (EMUC) has become an obligatory event. The sixth meeting took place in Lisbon this year and confirmed the truly multidisciplinary aspect of the conference. PIET DIRIX INTRODUCTION On Thursday 13 November, the 3rd EAU Section of Urological Imaging (ESUI) meeting preced- FOCUS ON NEXT ESTRO CONGRESSES ed the actual EMUC conference, but also had some interesting topics for radiation oncologists. Of particular interest was the joint session with the European Association of Nuclear Medicine (EANM) on new PET tracers. The growing enthusiasm for 68Gallium-labelled Prostate-specific Membrane Antigen (PSMA) was noteworthy and could have implications for staging and especially re-staging of prostate cancer patients. This was also reflected in the oral presentations, two of FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES EMUC which dealt with this particular subject. Tobias Maurer and colleagues from München deservedly won the best poster award with their abstract on 68Ga-PSMA PET-MRI for pre-operative lymph node staging in intermediate and high-risk prostate cancer patients, which could also inform individualised treatment planning. The following session on multiparametric MRI for prostate cancer management was, although not particularly geared towards radiation oncologists, highly informative. EMUC 2014 itself got off to an extremely promising start with a very interesting (and well-attended) session on management of progressive disease. Jelle Barentsz suggested that multiparametric MRI, particularly using dynamic-contrast enhancement sequences, could detect local recurrence after surgery even at very low PSA levels and could help guide focal salvage radiotherapy. For lymph node staging, current imaging modalities (both MRI and Choline PET-CT) remain rather unsatisfactory. Again, the particular promise of 68Ga-PSMA PET-CT (or indeed PET-MRI) and Ferumoxtran-10 ultrasmall superparamagnetic iron oxide-enhanced (USPIO) MRI was stated, although there remain some regulatory issues with general USPIO usage. Marco Van Vulpen clearly described how local progression INTRODUCTION after primary radiotherapy can be salvaged with brachytherapy or other focal treatment options, but stressed the need for increased quality (assurance). Steven Joniau had a particularly interesting talk on salvage surgery, suggesting that in the case of an isolated pelvic recurrence, a broad template resection should be preferred over a limited resection of gross disease only. This suggests that there could be a role for elective radiotherapy, rather than focal treatment only, in those cases as well. The last speaker of the session, Gerhardt Attard, addressed what is arguably the most controversial topic in the management of progressive prostate cancer: the timing of the different systemic treatment options. The second session of the day dealt with adjuvant treatment in stage I testicular cancer (chemotherapy vs. surveillance), followed by a very stimulating talk on checkpoint inhibition by Joaquim Bellmunt. In particular, the combination of anti-CTLA-4 or PD-(L)1 with radiotherapy is very exciting, although early results in prostate cancer appear somewhat disappointing. In the afternoon, Robert Huddart made a strong case for bladder preservation as a sensible and clinically viable alternative to radical cystectomy. On Saturday morning, there was a Hands-OnTraining (HOT) on prostate delineation using FOCUS ON NEXT ESTRO CONGRESSES CT and MRI, presented by Carl Salembier, Marco Van Vulpen, and Vincent Khoo. By using the ESTRO FALCON software, a prostate cancer case was delineated online and discussed afterwards. This was an extremely interesting workshop where many “tips and tricks” were shared by true experts in the field, which apparently resulted in decreased inter-observer variability between the start and the end of the session. In a parallel session, Gert De Meerleer elaborated on his recent Lancet Oncology paper and made the case for stereotactic body radiotherapy in the management of renal cell carcinoma, both in primary settings and in treatment of oligometastatic disease. In the afternoon, there were interesting sessions on the value of quality assurance (QA) in clinical practice and how radiotherapy has led this field from the outset. This was closely followed by a session on the prevention of treatment-related toxicity based on knowledge from dose constraints derived through the QA process. The conference ended on a high note with an exceedingly interesting session on high-risk prostate cancer. Ofer Yossepowitch made the case for surgery as a potential option for such patients, but Alberto Bossi very eloquently stressed the risks with such an approach. Bertrand Tombal summed up the rationale for radiotherapy on FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES EMUC the prostate in metastatic patients, which is currently being investigated in the PEACE-1 (EORTC 1201) and STAMPEDE trials. EMUC 2015 7th European Multidisciplinary Meeting on Urological Cancers In conclusion, I would really recommend this conference to any radiation oncologist with an interest in uro-oncology. Even the sessions not directly discussing radiation oncology topics will increase your general understanding of these cancers and will ultimately improve both clinical decision-making as well as communication with the other specialties. In that regard, EMUC was also an excellent opportunity for networking and getting to know imaging specialists, urologist, and clinical oncologists in the wonderful setting of Lisbon. Barcelona, Spain 12-15 November 2015 www.emuc15.org Piet Dirix Radiation oncologist Iridium Cancer Network University Hospital Antwerp Antwerp, Belgium INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ECHNO 2014 ESTRO CONFERENCES REPORT BY RENÉ LEEMANS President of EHNS Co-Chair of ICHNO ECHNO 2014 6th European Conference on Head and Neck Oncology 24 - 26 April 2014 Liverpool, UK RENÉ LEEMANS INTRODUCTION ECHNO, the biennial congress of the European Head and Neck Society (EHNS), has become a leading forum for presenting the latest and most innovative research, both basic and clinical, in the field of head and neck oncology in Europe. The 2014 meeting, organised jointly by the British Association of Head and Neck Oncologists (BAHNO) and EHNS under the leadership of James Brown, certainly met every expectation, honouring its motto: a singular event, a multidisciplinary approach. Emphasis was placed on addressing the need for a multidisciplinary approach to facilitate cooperation between the various clinical and research specialties involved in the management of head and neck cancer. ECHNO 2014 presented the latest research and techniques in the ongoing effort to improve the lives of patients everywhere. The stellar scientific programme featured experts from around the world, who facilitated stimulating debates about the most controversial topics in proton therapy, robotics and transoral laser, and many others. A total of 900 participants, 54 speakers and 73 exhibitors attended ECHNO 2014 in the city of the “Yellow Submarine”. There were special sessions on the question of whether surgery is still FOCUS ON NEXT ESTRO CONGRESSES the best treatment of oral cavity cancer, on the future of clinical trials, on basic science, and the influence of hypoxia in head and neck cancer. The programme was supplemented by several pre-congress courses. Prizes were awarded for best oral presentation and poster, as well as for best young clinician and young scientist. During the congress, four special recognition awards for outstanding services to EHNS were presented to the former President, Jean Louis Lefebvre, and three former officers, Patrick Bradley, Jan Olofsson and Dominique Chevalier. Under the newly elected board, EHNS will continue to bring together medical experts from many disciplines, including: head and neck cancer specialists, oral and plastic surgeons, radiation therapists, medical oncologists, imaging specialists and pathologists. The society also brings together other stakeholders, including: speech therapists, cancer nurses, psychologists, physiotherapists, dieticians, social workers, basic scientists and patient organisations involved in any aspect of head and neck oncology. We hope to welcome you to the 7th ECHNO to be held in Istanbul from 28-30 April 2016, under the leadership of Sefik Hosal, for a stimulating programme covering the various aspects of FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ECHNO 2014 head and neck oncology with special emphasis on larynx, skin and melanoma, nasopharyngeal cancer, supportive care, and oral cancer, taking advantage of new technologies and state-of-theart basic research, accompanied by a more than fitting social programme. In the meantime, we look forward to welcoming you to ICHNO in February in Nice. René Leemans President of EHNS Co-Chair of ICHNO INTRODUCTION FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES ECHNO 2014 2ND MAKE SENSE CAMPAIGN European Head & Neck cancer awareness week 22 - 26 September 2014 The 2014 Make Sense campaign called for action to drive change for head and neck cancer patients in Europe. There is little awareness of head and neck cancer among the general public and the healthcare community in Europe, resulting in the majority of diagnosed cases being late stage. Consequently, treatment outcomes for patients are poor and chances of survival are significantly reduced. Head and neck cancer is the sixth most common type of cancer in Europe and its incidence is on the rise. In 2012 alone, more than 150,000 new patients were diagnosed. Despite major advances in the treatment of head and neck cancer over the past three decades, patient outcomes remain disappointingly unchanged. Earlier diagnosis and referral to specialised healthcare professionals can have a major impact on improving the outcomes for head and neck cancer patients across Europe. INTRODUCTION To drive change for head and neck cancer patients in Europe, the European Parliament, in partnership with the EHNS and the European Cancer Patient Coalition (ECPC) has set out the following action points and calls on the European Commission to: ing treatment and care to ensure best possible health outcomes 6. Encourage further research on head and neck cancer to ensure better prevention strategies, treatment options and, ultimately, outcomes, for all patients. 1. Actively engage in awareness campaigns on disease prevention and highlight the signs and symptoms of head and neck cancer 2. Support early diagnosis and referral to qualified healthcare professionals 3. Support a multidisciplinary treatment approach for head and neck cancer, by integrating experts across disciplines 4. Provide guidelines at EU level to ensure that all European citizens have equal access to the best available treatment, and support the dissemination of best practices in disease management across EU member states 5. Promote patient rehabilitation programmes to drive engagement and adherence to ongo- www.makesensecampaign.eu FOCUS ON NEXT ESTRO CONGRESSES FOCUS ON PAST ESTRO CONGRESSES CALENDAR OF EVENTS 2015 FEBRUARY 5 - 6 February RUSSCO breast cancer conference Moscow, Russia ESTRO recommended event 5 - 7 February EACR Conference Series 2015 Radiation Biology and Cancer: From Molecular Responses to the Clinic Essen, Germany ESTRO recommended event www.eacr.org/radiationbiology2015/ > hb 12 - 14 February 5th ICHNO Nice, France ESTRO, ESMO and EHNS joint event www.estro.org/congresses-meetings/ items/5th-ichno > hb 12 - 14 March Advanced prostate cancer consensus conference 2015 St. Gallen, Switzerland ESTRO recommended event www.prostatecancerconsensus.org/ > 22 - 26 March Radiobiology & radiobiological modelling in radiotherapy course Port Sunlight, Wirral, UK ESTRO supported course www.estro.org/binaries/content/assets/estro/ school/supported-courses/ccc_rblgy_flyer_2015.pdf > 27 - 28 March Trends in Central Nervous System Malignancies EORTC-EANO-ESMO Conference Istanbul, Turkey ESTRO endorsed event MARCH 6 - 7 March Perspectives in Lung cancer Turin, Italy ESTRO endorsed event imedex.com/lung-cancer-congress-europe/ > www.ecco-org.eu/EEE2015 > 2015 APRIL 29 April - 1 May EMSOS 28th Annual meeting of the European Musculo-Skeletal Oncology Society 14 - 15 April 5th European Lung Cancer Conference (ELCC) Geneva, Switzerland Athens, Greece In collaboration with ESTRO ESTRO endorsed event www.emsos.org > hb www.esmo.org/Conferences/ELCC-2015-LungCancer > 20 - 22 April 10th International Conference on Carbonic Anhydrases MAY 8 - 9 May Modern Radiation For Lymphoma New York, USA Maastricht, The Netherlands ESTRO recommended event ESTRO endorsed event www.carbonicanhydrasemaastricht.info/ > hb 24 - 28 April 3rd ESTRO Forum www.mskcc.org/events/cme/modern-radiation-lymphoma-updated-role-and-new-rules/ form > http ESTRO interdisciplinary congress 18 - 22 May 25th Advanced Multichannel Teaching Course www.estro.org/congresses-meetings/ items/3rd-estro-forum > hb ESTRO endorsed event Barcelona, Spain Rome, Italy 2015 25 - 29 May 15th International Congress of Radiation Research (ICRR 2015) Kyoto, Japan In collaboration with ESTRO www.congre.co.jp/icrr2015/ > http SEPTEMBER 18 18th ECCO - 40th ESMO European Cancer Congress Reinforcing multidisciplinarity VIENNA, AUSTRIA, 25 - 29 SEPTEMBER 2015 25 - 29 September European Cancer Congress 2015 (ECC2015) Vienna, Austria www.ecco-org.eu/Events/ECC2015.aspx > 35 SIOP SIOP Europe the European Society for Paediatric Oncology www.ecco-org.eu NOVEMBER JUNE 20 - 22 June Wolfsberg Meeting Wolfsberg, Switzerland In collaboration with ESTRO www.wolfsberg-meeting.com/ > JULY 26-30 July World Congress on Larynx Cancer Cairns, Australia ESTRO endorsed event www.wclc2015.org/home/ > 12 - 15 November EMUC 7th European Multidisciplinary Meeting on Urological Cancers Barcelona, Spain Joint EAU, ESTRO and ESMO conference 2016 APRIL 29 April - 04 May ESTRO 35 Turin, Italy ESTRO congress CREDITS ESTRO Bimonthly newsletter N° 98 | January - February 2015 European Society for Radiotherapy & Oncology OFFICERS President: Philip Poortmans President-elect: Yolande Lievens Past-president: Vincenzo Valentini EDITOR Cécile Hardon-Villard EDITORIAL ADVISERS Joanna Kazmierska and Ludvig Muren (ESTRO Board Members) Emma Mason and Mary Rice GRAPHIC DESIGN Daneel Bogaerts Published every two months and distributed by the European Society for Radiotherapy & Oncology. DEADLINES FOR SUBMISSION OF ARTICLES IN 2014 AND 2015 May/June 2015 Issue > 2 March 2015 July/August 2015 Issue > 4 May 2015 Sept./Oct. 2015 Issue > 1 July 2015 Nov./Dec. 2015 Issue > 1 September 2015 For permission to reprint articles please contact the editor. If you want to submit articles for publication, please contact the editor: [email protected] For advertising, please contact: [email protected] Opinions expressed in the ESTRO newsletter do not necessary reflect those of the Society or of its officers.


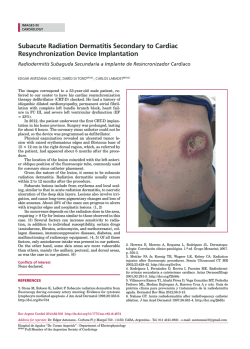

© Copyright 2026