
Polymerase Chain Reaction Detection of the BCR-ABL
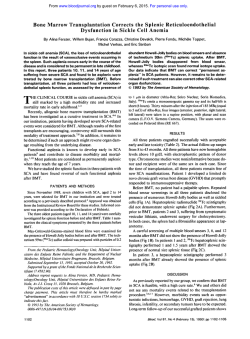
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Polymerase Chain Reaction Detection of the BCR-ABL Fusion Transcript After Allogeneic Marrow Transplantation for Chronic Myeloid Leukemia: Results and Implications in 346 Patients By J.P. Radich, G. Gehly,t T. Gooley, E. Bryant, R.A. Clift, S . Collins, S. Edmands, J. Kirk, A. Lee, P. Kessler, G. Schoch, C.D. Buckner, K.M. Sullivan, F.R. Appelbaum, and E.D. Thomas We studied 346 patients after bone marrow transplantation (BMT) for chronic myeloid leukemia (CML) for the presence of the bcr-ab/ transcript detected by the polymerase chain reaction (PCR) t o understand the frequency and implication periphof a positive test. A total of634 samples of BM andlor eral blood were obtained for PCR analysis between 3 and 192 months after BMT. A positive PCR test at3 months postBMT was not statistically significantly associated with an increased risk of relapse compared with PCR-negative patients. However, a positive PCR assay at 6 months and beyond was highly associated with subsequent relapse. The Kaplan-Meier estimate of relapse for patients testing PCRpositive at 6 t o 12 months was 4290 versus 3% for PCRnegative patients (PC .0001). The Kaplan-Meier estimate of survival at 4 years for the PCR-positive patients was 74% compared with 8340 for the PCR-negative group (P= .002). Multivariable analysis indicated that a PCR-positive result at 6 to 12 months post-BMT, the type of BMT donor (allogeneic matched donor Y mismatched or unrelated), and the prescence of acute GVHD were independent risk factors for subsequent relapse. The relative risk(RR) for relapse for patients PCR-positive at 6 t o 12 months post-BMT was 26.1(95% confidence interval, 8.9 t o 76.1, P < .0001). The outcome of long-term patients(>36 months post-BMT) who testedPCRpositive was much better, as 15 of 59 (2540)tested positive for bcr-ab/, but only one patient relapsed. There was a 91% concordance between PCR tests of simultaneously obtained BM andperipheral blood.These analyses show that the PCR assay of the bcr-ablfusion transcript6 t o 12 months postBMT is an independentpredictorof subsequent relapse which provides an opportunity for early therapeutic intervention. 0 1995 b y The American Society of Hematology. B Philadelphia chromosome (Ph). This technique can identify the bcr-ubl transcript at a dilution of a single Ph-positive cell in a background of I O 5 to 10' normal cells. Although the PCR assay can detect the presence of the bcr-ab1 transcript with exquisite sensitivity, the association of the detection of bcr-ab1 post-BMT and relapse is uncertain."-*' Several studies have examined the association of PCR-positivity post-BMT, but the two largest studies are contradictory in conclusions. Roth et a12' studied 64 patients post-BMT and found that while PCR status early after transplant (< 100 days) did not correlate with relapse, PCR-positivity at later periods did predict relapse. Overall 37 of 64 patients had at least one positive assay, and 13 of these 37 (35%) relapsed. When multiple samples were analyzed for each patient, those with 2 1 PCR-positive assay had a 40% probability of relapse, and those with all PCR-positive assays had 70% risk of relapse. Patients with multiple negative assays did not relapse. Although this study concludes that PCR-positivity at 6 months post-BMT is associated with relapse, the study by Miyamura et al," coincidentally also with 64 patients, suggests that PCR-positivity is not so foreboding. In their study patients were from 2 to 220 weeks from BMT. The analysis divided patients into two groups. Thirty-one patients had at least one negative PCR test, and none of these patients relapsed. In contrast, 33 patients had all PCR tests positive, yetonly 7 relapsed. Moreover, 21 patients had a positive PCR assay greater than 1 yearfrom transplant, withonly two relapses. Thus far, all studies have been too small to evaluate the PCR assay results with other variables known to influence the risk of relapse, such as the phase of disease, the type of allograft, and the presence of GVHD. Does the PCR assay have predictive power even when controlling for these factors, or does it merely recapitulate a known relapse risk? We report here onthe PCR evaluation of 346 CML patients postBMT and the estimate of risk of relapse associated with PCR-positivity for bcr-abl, controlling for other clinical vari- ONE MARROW transplantation (BMT) is the only curative modality for chronic myeloid leukemia (CML), but relapse occurs in 10% to 20%of patients receiving transplants in chronic phase"3 and over 50% of patients receiving transplants in accelerated or blast c r i ~ i s . ' . ~ In. ~addition to phase of disease, other clinical features that may influence the risk of relapse include the type of donor allograft (unmanipulated BM v T-cell-depleted marrow), and the presence or absence of acute or chronic graft-versus-host disease (GVHD), with patients receiving unmanipulated marrow or developing GVHD having a lower risk of relapse than those receiving T-cell-depleted marrow or without GVHD.'."' The ability to identify patients at high risk for relapse postBMT is of considerable interest because it might allow for early interventions, including manipulations of the immunosuppression used to prevent and treat GVHD, the addition of donor leukocytes,*"' or the addition of drugs such as ainterferon.'* The polymerase chain reaction (PCR) can detect CML cells through the amplification of the unique bcr-ab1 fusion mRNA transcript, which is the molecular correlate of the From the Divisions of Clinical Research, Experimental Pathology, and the Program of Molecular Medicine, Fred Hutchinson Cancer Research Center, Seattle, WA. fDeceased. Submitted August 12, 1994; accepted December 19, 1994. Supported by Grants No. CA18029 and CA18221 from the National Cancer Institute. Address reprint requests to Jerry Radich, MD, Fred Hutchinson CancerResearchCenter,C2-023, 1124 Columbia St, Seattle, WA 98104. The publication costsof this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-497//95/8509-0012$3.00/0 2632 Blood, Vol 85, No 9 (May 1). 1995: pp 2632-2638 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. BCR-ABL IN CML POST-BMT abies associated with relapse in multivariable models. We find that a positive PCR assay at 6 to 12 months post-BMT is an independent predictor of relapse after separately controlling for phase of disease, type of donor, and acute and chronic GVHD. We also note that PCR positivity is less common in patients greater than 12 months from transplant and is less strongly associated with relapse. Like allogeneic, related transplants, unrelated donor (URD) transplants are commonly PCR-positive early after transplant but, in contrast, URD patients who are PCR-positive infrequently relapse. MATERIALS AND METHODS Patients. All patients receiving transplants for CML at the Fred Hutchinson Cancer Research Center between 1976 and 1993 were eligible for study. The transplant protocols were approved by the Institutional Review Board. Patients were identified after BMT before their discharge home, or for patients already home, through contact with our Long-Term Follow-Up (LTFW) program. Requests were made to receive both BM and peripheral blood (PB) at 6month intervals. The LTFU staff were unaware of the results of PCR assays. Many patients elected to have samples obtained at their yearly LTFU check at our institution. These BM and PB samples were used to perform cytogenetic evaluations and the PCR assay for the presence of bcr-ab[ mRNA. Transplant regimen. Patients receiving transplants in chronic phase before 1990 received a conditioning regimen of cyclophosphamide (CY) 60 mgkg for 2 days (120 mgkg total) and total body irradiation (TBI) at a dose of 200 cGy for 6 days (1,200 cGy total).’ Since 1990 chronic phase patients were randomized tothe above regimen versus busulfan (BU) 16 mgkg and CY120 Accelerated- and blast-phase patients received a preparative regimen of CY 120 m a g and TB1 of 225 cGy for 7 days (1,575 cGy total).’ Unrelated donor transplant recipients received a preparative regimen of CY 120 m@g and either 1,200 cGy of T B 1 if in chronic phase or 1,320 cGy if in accelerated or blast phase. All patients received GVHD prophylaxis with methotrexate and cyclosporine as previously described.M Sample preparation. RNA isolation from leukocytes from fresh BM and PBsamples was performed by the acid guanidinium thiocyanate-phenol-chloroform method as previously described.” Aliquots from this RNA were used for the detection of bcr-ab1 and the control g 2 microglobulin mRNA (below). Reverse transcription (RT) PCR assay for bcr-abl. We used a two-step, “nested” RTPCR to amplify the chimeric bcr-ab1 mRNA. The nested reaction yields either a 305-bp or a 234-bp PCR product depending on the expression of bcr exon 3. One microgram of total RNA was added to a combination 50 pL RTPCR mix of 25 pmol of oligonucleotides CMLND and CMLNC, 50 mmoVL KCL, 10 mmom TRIS-HCL (pH 9.0). 0.1%Triton X-100 (Sigma, St Louis, MO), 200 pmoVL dioxynucleotides (dNTPs), 1.5 mmol/L MgClz, 1.25 U Taq polymerase (Amplitaq; Perkin Elmer Cetus, Nonvalk, CT), 10 U RNAsin, 7.5 U AMV RT (Boehringer Mannheim, Indianapolis, IN), and DEPC H20. This reaction mixture was incubated for 30 minutes at 42”C, brought to 95°C for 5 minutes, and then amplified for 40 cycles of 94°C for 30 seconds, 55°C for 1 minute, and 72°C for 1 minute followed by a final elongation step at 72’C for 7 minutes, using an Omigene thermocycler (Hybaid, Ltd, Woodbridge, NJ). Five microliters of this first reaction was transferred to a 45-pL second reaction mixture containing fresh PCR ingredients of25pmol oligonucleotides CMLNA and CMLNB, 500 mmoVL KCl, 10 moVL TRIS-HCL (pH 9.0), 0.1% Triton X-100, 1 mmol/ L dNTPs, 1.5 mmol/L MgC12, 1.5 U Taq polymerase, and DEPC 2633 HzO. The tubes were placed into a preheated (65°C) thermocycler, and after an initial denaturation step of 95°C for 5 minutes, 40 cycles of amplification at94°C for 30 seconds, 55°C for 1 minute, and 72°C for 1 minute followed by a final elongation step at 72°C for 7 minutes was performed. After amplification 15 pL of the final PCR product was electrophoresed through ethidium-bromide-stained 2% agarose gel and photographed. For all PCR reactions a dilution of K562 RNA into the Phnegative cell line HL60 RNA served as a positive control. Negative controls included both a no-RNA PCR mix (“blank”) and HL60 RNA. A separate amplification of p2 microglobulin was used as a control ofRNA integrity andwas performed as previously described.% Precautions to eliminate PCR carryover contamination included separate rooms for pre-PCR and amplification procedures, filtercontaining disposable pipette tips, and no-nucleic acid PCR reactions as negative control in all PCR amplification reactions.’* Using these precautions we had an approximately 2% incidence of false positive assays, defined as a positive PCR result in the no-RNA or HL60 RNA reactions. In these instances all samples run in the amplification “batch” (usually 10 samples) was repeated. The nucleotide sequences of the PCR primers used in bcr-ab1 amplification were: CMLNA 5’-TGGAGCTGCAGATGCTGACCAACTCG-3’; CMLNB 5“ATCTCCACTGGCCACAAAATCATACA-3’; CMLNC 5“GAAGTGTTTCAGAAGClTCTCC-3’; CMLND 5”TGATTATAGCCTAAGACCCGGA-3’. Definition of positive and negative PCR assays. The PCR assays were performed without knowledge of the patient’s cytogenetic results or hematologic remission status. A positive PCR test required a correct-size bcr-ab1 PCR product as well as negative “blank” and HL60 amplifications. A negative assay required the absence of a bcr-ab1 PCR product as well as no amplification of the “blank” and HL60-negative controls, successful amplification ofthe diluted K562-positive control, and a successful p2 microglobulin PCR amplification. If a positive or negative control did not amplify as expected, the entire panel of patient samples done in that amplification “batch” was discarded and repeated. Definitions of outcomes and statistical methods. In this study we defined relapse by both hematologic and cytogenetic criteria. Cytogenetic relapse was defined as 2 5 metaphases positive for the Ph chromosome atany point in time or the presence ofanyPh chromosomes on two successive cytogenetic evaluations at least 6 months apart. Patients were classified as being PCR-positive or -negative at the time interval of sampling. Relapse and survival rates for patients appropriately classified at the stated time intervals were estimated by the method of Kaplan and Meier.33For the endpoint of relapse patients who died without relapse were censored at the time of death. The hazard rates of relapse and survival for patients classified as PCR-positive and PCR-negative at specific time intervals were compared using the log-rank test.’4 Multivariable analyses were performed by fitting Cox regression models and considering the data to be left truncated. This allowed the variable entry times onto study to be ac~ommodated.’~ PCR status was considered as a time-dependent covariate in these models. If a patient had PCR results that were positive concurrently with a sample which showed hematologic or cytogenetic relapse, then such a patient was classified according to the PCR status at the last test before relapse. For example, a patient with a negative PCR assay at 6 months who at 12 months was FCR-positive for bcr-ab1 with cytogenetics positive for the Ph chromosome is regarded in this analysis as a patient who relapsed with a negative PCR assay at 6 months. Patients were excluded from statistical analyses if (1) they had evidence of hematologic or cytogenetic relapse simultaineously to, From www.bloodjournal.org by guest on February 6, 2015. For personal use only. RADICHET AL 2634 Table 1. Patient Characteristics N = 346 Sex: 148 F1198 M Age: Median 36 (range 2-60) BMTtype: Allogeneic related Unrelated Twin Phase: Chronic Accelerated Blast 2nd chronic 501 .- p<0.0001 A5 240 96 10 262 56 16 12 (69%) (28%) (3%) (76%) 115%) (6%) (3%) 40 35 g 30 0) L 25 22 20 15 10 or before. their first PCR assay: or (2) they received a second transplant before their first PCR assay. 5 0 6-12 m 3m RESULTS Patient characteristics. The clinical characteristics of the 346 patients included in these analyses are shown in Table 1. Six hundred thirty-four samples of PB and/or BM were successfully analyzed by PCR; in 15 other samples RNA did not amplify from the PB and BM. One hundred sixty-two patients had one PCR test performed, and 184 had two or more tests performed. Eighty-two patients had their first PCR sample at 3 months post-BMT, 146 patients at 6 to 12 months, 83 patients at 12 months to 3 years, and 35 patients at greater than 3 years post-BMT. The total number of patients tested in each interval after BMT, categorized by type of donor and phase of disease, is shown in Table 2. The median follow-up for all patients from the time of first PCR assay to either relapse or last contact is 16 months (range, 1 to 47 months). PCR-pnsitivih~and the risk qf srrbsequent relapse. The percentage of patients testing positive for hcr-ah1 by the PCR assay at 3 months, 6 to I2 months, > 12 months to 36 months, and >36 months, and the Kaplan-Meier estimates of relapse for those testing PCR-positive versus PCR-negative are shown in Fig 1. Thirty-two patients were subsequently excluded from these analyses because they relapsed >36 m ~12-36 m Interval from BMT Fig 1. The percentage of patients testing PCR-positive and the Kaplan-Meier estimate of relapse associated with a PCR-positiveand PCR-negativetest, defined by time from BMT. The x axis represents the time interval from BMT, whereas the y axis is percentage. ( W The percentage of patients testing PCR-positiveat each time interval. (0) The Kaplan-Meier estimate of relapse for PCR-positive patients tested in the designated time interval from BMT. (R) The estimate of relapse associated with a negative PCR-test in the time interval. The P values compare the risk of relapse for patients PCR-positive before or at the time of their first PCR test. Forty-five percent (35/77) of patients tested at 3 months post-BMT were PCRpositive, and their Kaplan-Meier estimate of relapse at 3.5 years is 32%. whereas the Kaplan-Meier estimate of relapse of those patients PCR-negative at 3 months is 24% ( P = .27). The percentage of patients PCR-positive at 6 to 12 months was 26%. The Kaplan-Meier relapse estimates for patients testing positive for hcr-ah1 at 6 to 12 monthsis shown in Fig 2. Forthe 38 patients testing PCR-positive, the Kaplan-Meier estimate of relapse at 4.5 years is 42%, compared with 3% for the 112 PCR-negative patients (P < Table 2. Patients TestingPCR-Positive and Time FromTransplant 0.5. 6-12 Variable rnos Related URD Twin Chronic Accelerated Blast 2nd chronic 301151 Total 381150 3 rnos 23/49 12/28 010 22/51 5115 516 315 35177 221103 14/42 215 281124 9/20 115 011 >12. <36 rnos 251110 4/39 112 251121 4/22 113 0/5 >36 rnos o) 14/45 v) 017 - 016 0.4- a 0 0, E 0.3. 0 12/49 216 011 011 14/58 The number of patients testing PCR-positive (numerator) and the total number of patients tested (denominator) in the s 3 months, >3 to s 1 2 months, > l 2 to s 3 6 months, and >36 months post-BMT is shown in each cell of the table. The first three rows categorizes the patients by the type ofdonor; the next four rowscategorizes patients by the phase of disease. Patients who had tests in more than one interval are included in the counts of each interval. 0 1 2 3 4 5 Years ofter BMT Fig 2. The Kaplan-Meier estimates of relapse for patients testing PCR-positive (N = 38)at 6 t o 12 months compared with patients who were PCR-negative(N = 112) for bcr-ablmRNA. Tick marks represent patients alive and still atrisk of relapse. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2635 BCR-ABL IN CML POST-BMT n 5617 0/20 5546 0120 5177 0/31 5152 0135 5026 4872 n OD0 * I m0 * W 0 5045 0120 n W20 W20 0120 o m 0120 0 0 8 . 8 OD0 0/120112 0/20 0120 * 019 8 0 OR0 0120 0 0120 0 0 - o m 0/20 0120 8 W 0120 4698 0 0120 8 8 I 0120 4862 0/20 0 m 0120 m 0 Fig 3. Follow-up of nine patients who had their first PCR-positive assay greater than 36 months post-BMT. IO) A PCR-negative test; ( 8 )a PCR-positive assay.Below the PCR result is a numericalfraction ofPhchromosome positive metaphasesltotal metaphases from a concurrent cytogenetic exam. ”-“ Indicates that a cytogenetic sample was not received. “I“ indicatesthat thesample yielded an inadequate cytogenetic preparation for evaluation. .mol).The median time from PCR-positivity to relapse was 7 months (range, 1.5 to 12 months). A separate Kaplan- Meier estimation was performed for just the allogeneic-related transplants. Ninety-eight patients were tested, and 20 were PCR-positive. The Kaplan-Meier estimate of relapse associated with a PCR-positive test at 6 to 12 months postBMT was 62%, compared with 3% for PCR-negative patients (P < .mol). Thirty of 151 patients (20%)tested from 12 to 36 months post-BMT were PCR-positive. Five of the PCR-positive and one of the PCR-negative patients have relapsed (KaplanMeier estimates of relapse 25% v l%, P < .OOOl). The median time from PCR-positivity to relapse was 7 months (range, 0.5 to 20 months). The median follow-up of the patients who tested PCR-positive but have not relapsed by June 1, 1994 is 28 months from the first PCR-positive assay. Fifteen of 58 patients (25%)tested greater than 36months post-BMT tested PCR-positive, and one relapsed. No PCRnegative patient relapsed. The median follow-up of these patients from their first PCR-positive test to present time is 22 months. Nine patients had their first positive PCR assay detected greater than 36 months post-BMT, and none have relapsed (Fig 3). The latest finding of a new positive PCR assay following a previous negative PCR was at 48 months (unique patient number [UPN] 5026, Fig 3). We also examined the effect of serial PCR testing among 184 patients with 2 2 PCR tests.For patients with all positive PCR tests, the Kaplan-Meier estimate of relapse is 78%. For patients with all negative PCR tests, the Kaplan-Meier estimate of relapse is 3%. For patients with both PCR-positive and PCR-negative tests, the relapse estimate is 22% (P < .0001). PCR-positivity in URDpatients. Because of the observation that URD BMT recipients have a lower relapse rate than allogeneic-related transplant recipientsz6.*’ we performed a separate statistical analysis on the 96 patients receiving an URD BMT. Twelve of 28 (43%) URD patients were PCRpositive at 3 months, and 4 relapsed, compared with one relapse in the 16 PCR-negative patients ( P = .lo, Fisher’s exact test). Fourteen of 42 (33%) URD patients tested 6 to 12 months post-BMT were PCR-positive, and 2 relapsed, compared with no relapses in the 28 PCR-negative patients (Kaplan-Meier estimate of relapse 18% v 0%, respectively, P = .11). Multivariableanalyses of MRDandrelapse. Clinical features potentially associated with relapse were added individually to PCR status at 6 or 12 months in multivariable analyses testing the association between relapse and PCR status along with various individual clinical variables (Table 3). These clinical variables included the HLA matching status of the donor (twin or matched v URD or mismatched), phase of disease at BMT (chronic phase v accelerated or blast phase), the presence or absence of acute (grade 2 11) and chronic GVHD after BMT, and the use of a TBI-containing preparative regimen. Because of the relatively small number of relapses, it was feasible to include only two covariates in any given model (PCR status plus one clinical variable). PCR-positivity alone was associated with a 26fold risk of relapse. Match status and acute GVHD were independently significantly associated with relapse. Patients who received an allogeneic matched transplant had a relative risk (m) of relapse of 5.1 compared withURD or mismatched transplant recipients, and patients with acute GVHD grades 0 or I had anRRof relapse of 0.4 compared to patients with grades 2 11. However, these variables did not influence the strength of the risk associated with a PCRpositive assay in either multivariable model. The phase of disease and the chronic GVHD status did not contribute to the risk of relapse independent of a PCR-positive assay. Table 3. Multivariate Analysis of Risk of Relapse for Patients Tested at 6 or 12 Months Post-BMT Variable PValue PCR-positive 26.1 PCR-positive match’ and 5.1 PCR-positive phaset and PCR-positive and PCR-positive and PCR-positive and cGVHDS 0.6 aGVHD§ TB111 0.6 <.0001 29.3 <.0001 ,003 <,000 24.81 .43 <.0001 24.9 .30 <.0001 30.9 0.4 .o 1 <.0001 .20 RR 0.7 26.1 95% Cl 8.9-76.1 10.0-86.4 1.8-15.1 8.4-73.0 0.3- 1.7 8.5-73.0 0.2-1.9 10.4-91.5 0.2-0.8 9.0-76.2 0.3-1.3 Relative risks (RR) of relapse were estimated by placing the PCR status (positive v negative) by itself into a multivariable model and then adding an individual covariate to the model. Thus an RR > 1 reflects a elevated risk of relapse associatedwith the presence of the covariates defined as: (*), allogeneic matched related transplant v mismatched orURD; (t),chronic phase vaccelerated,blast, or second chronic phase; (*), presence v absence of chronic GVHD; (§l, acute GVHD grades 2 II vgrades 0-1; and (11). use of a TBI-containing preparative regimen v chemotherapy only. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2636 RADICH ET AL The same clinical variables along with the PCR status entered into a multivariable model in a step-up fashion, using all patients studied over all time intervals after transplantation. The RRof PCR-positivity was 30 ( P < .000l), and the only other variable entering the model was the HLA match (RR = 5.6, P = .016). A separate analysis was performed on the 216 patients who received an allogeneic-related transplant in chronic phase. A step-up regression analysis was also performed in this group, with the variables of PCRand GVHD status. PCR status was the only variable that entered the model, with anRRof18 ( P < ,0001). Neither acute nor chronic GVHD entered the model. The correlation of blood and BM samples. PB and BM samples obtained on the same day post-BMT were evaluated on S 14 samples. Concordance between the PB and BM PCR result occurred in 468 samples (91%). Discordance with BM PCR-positivity and peripheral blood PCR-negativity occurred in 6.5% of tests, whereas a negative BM PCR assay with a positive PB assay occurred in 2.5% of tests. DISCUSSION Although the presence of the bcr-ab1 chimeric mRNA has been studied in CML patients previously, the predictive il. .')actof a positive PCR, especially in light of clinical variat es associated with relapse, has been unclear. Does the PCR detection of bcr-ab1predict relapse even when controlling for factors such as GVHD and phase of disease? The present study of 346 patients allowed usto evaluate the predictive power of the PCR in light of other clinical variables as well as examine the significance of the PCR assay at different time points after BMT. We found that a single PCR assay positive for the bcr-ab1 chimeric mRNA was associated with a high risk of subsequent relapse. The PCR assay discriminated best at 6 to 12 months post-BMT, when patients who were PCR-positive experienced a 42% risk of relapse, compared with only 3% for those PCR-negative. Moreover, the PCR assay was the strongest predictor of relapse and remained highly associated with relapse in multivariable models when adjusted for other clinical variables associated with relapse in CML. In the multivariable model of all patients PCR-positivity carried an RR = 30, whereas in the subgroup of those receiving an allogeneic, matched transplant while in chronic phase, the RR = 18. In patients sampled greater than 36 months after BMT,andinURD transplants, a PCR-positive test was not strongly associated with relapse. It should be emphasized that these data do not meanthat clinical variables such as phase of disease are unimportant in describing relapse risk, but instead indicate that PCR-positivity is in itselfa strong independent predictor of relapse. Our finding of a 42% Kaplan-Meier estimate of relapse in patients with PCR-positivity for bcr-ab1 at 6 to 12 months post-BMT is in agreement with the study by Roth et al.23 Moreover, we found a similar influence of multiple PCR testing on predicting relapse, with a 78% estimate of relapse for patients with two or more positive PCR tests, a 22% risk for patients with only one positive test, and a 3% risk for patients with repetitive PCR-negative assays. However, we have chosen to emphasize the predictive power of a single test, thus avoiding potential biases associated with multiple testing, such as controlling for patients who either did not receive subsequent testing for a variety of reasons or who received testing at a different interval. We found that IS of S8 patients who were studied greater than 36 months post-BMT had at least one PCR-positive test. Nine of these 14 had their first PCRtest become positive at greater than 36 months after at least one negative PCR test (Fig 3). However, with a median follow-up since first PCR-positivity of nearly 2 years none of these long-term patients has relapsed. These data suggest that PCR-positivity in these long-term patients is associated with a lower risk of relapse, or predicts a considerably slower tempo of relapse, than PCR-positivity at 6 to 12 months post-BMT. This interesting trend is most clearly demonstrated in Fig 1, which shows that the relapse risk associated with a PCR-positive assay steadily decreases from 42% at 6 to 12 months to less than 10% for those patients testing positive at greater than 36 months after BMT. These data suggest that CML may be a heterogeneous disease which may be more or less aggressive. Early PCR-positivity (6 or 12 months post-BMT) may delineate a group of patients with more aggressive disease in whichthetempoof PCR-positivity to relapse is relatively quick. In contrast, patients who become PCR-positive late after BMT may have more indolent disease, which may relapse at a slower pace after PCR-positivity, if at all. Thus, although patients PCR-positive at 6 or 12 months the mGdianof first PCR-positive test to relapse was 7 months, for patients PCR positive at greater than 36 months postBMT, the median follow-up from time of first PCR-positive test to last contact is 22 months. Previously the most extensive investigation of long-term CML patients was reported by Guerrasio et aI,** who tested 27 patients at greater than 36 months post-BMT. Five of those 27 patients had at least one PCR-positive test. One had no subsequent test, one had a subsequent PCR-positive assay, and the remaining three reverted to PCR-negativity. None of the five patients relapsed. These data combined with our experience suggest that PCR-positivity in long-term patients may not carry so high a risk of relapse compared with those patients testing positive sooner after BMT. Further follow-up willbeimportant to see if these long-term PCR-positive patients are truly unlikely to relapse, or merely relapse at a slower rate than those patients with early PCR-positive tests. We were interested in separately evaluating patients receiving an URD transplant because these patients experience relapse rates less than half of that of allogeneic, related transplants for CML.36.37 Interestingly, these patients have a similar rate of PCR-positivity to the aggregate CML group at 3 months and 6 to 12 months. The difference in the URD experience is that the Kaplan-Meier estimateof relapse associated witha positive PCR assay is relatively low, only 18%. There are few reports with which to c 'mpare this experience. Cross et ai" report on 15 URD recipients, IO of whom were PCR-positive at some time during the post-BMT course. They report only one cytogenetic relapse in this group. The low progression to relapse in PCR-positive patients parallels the low risk of relapse experienced in all URD transplants for CML, and may be related to From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2637 BCR-ABL IN CML POST-B'MT the graft-versus-leukemia effect.&' Thus, the common occurrence of PCR-positivity early after transplantation implies that the preparative regimen frequently does not completely eliminate the leukemic cells and that the subsequent lower relapse rates in the URD recipients revolves around the itnmunomodulatory effect associated with GVHD. Although our findings contrastwithseveralstudies which suggest that PCR-positivity after BMT is not associated with a dramatic increase of relapse risk,14.1','9.25.29 most studies, including our own, agree that persistently negative PCR assays from 6 to 12 months after BMT place the patient in a low-risk category. In our study, a negative PCR test at 6 to 12 months post-BMT was associated with only a 3% Kaplan-Meier estimate of relapse. At longer intervals from transplant, the predictive power of a negative exam was even more dramatic, as no patient with a negative test after 12 months has relapsed, with a median follow-up of 19 months. Taken together, all studies agree that a negative PCR test is associated with a very low risk of relapse. However, the implications of an early positive test arelessclear.This may becausedlargely by the sundry differences between studies both in variables related to therapy (eg,thecomposition of thecohortin regard to phases of disease, unmanipulated v T-cell-depletedmarrow,preparativeregimens,andimmunosuppression regimen), and to PCR testing (eg, PCR test assay conditions and sensitivity, frequency and time points of testing, and rigor of cytogenetic testing). Our study has practical implications for the study and treatment of CML patients post-BMT. First, there was a median of approximately 6 months from PCR-positivity to subsequent relapse, long enough to launch intervention trials. Therapeutic approaches include the reduction in the amount of immunosuppression given to prevent GVHD, the use of a interferon," or the administration of donor buffy coat infusions."" Secondly, the high concordance between results obtained from PB and BM shows that PB can be used for monitoring. Thirdly, the PCR test has less predictive value in long-term patients and URD recipients who may not benefit from routine testing for bcr-abl. Recently studies using a semi-quantitative or competitive PCR assay for the bcr-abl fusion mRNA24.26 have suggested that a progressive increase in bcr-ab2 copy number can be used to identify those patients who will relapse from those who will not. Validation of these data may not improve on the predictive power of a negative PCR test but could improve the predictive power of a positive test. However, caution may be required to interpret quantitative results from center to center for reasons involving both center-specific treatment and patient population as well as methods of sampling and PCR testing. In summary, the PCR assay appears to discriminate between patients at a very low risk of relapse and those at a higher risk of relapse. The predictive power of the PCR assay appears independent of other relapse risk factors. Our data indicate that the PCR test is of greatest predictive value when performed at 6 to 12 months after BMT in allogeneicrelated donor recipients. PCR testing makes possible early intervention to avert relapse. REFERENCES 1. Thomas ED, Clift A, Fefer A, Appelbaum FR, Beatty P, Bensinger WI, Buckner D, Cheever MA, Deeg HG, Doney K,Flournoy N, Greenberg P, Hansen J, Martin P, McGuffin R, Ramberg R, Sanders JE, Singer J, Stewart P, Storb R, Sullivan K, Weiden PL, Witherspoon R: Marrow transplantation for the treatment of chronic myelogenous leukemia. Ann Intern Med 104:155, 1986 2. Goldman JM, Gale RP, Horowitz MM, Biggs JC, Champlin RE, Gluckman E, Hoffman RG, Jacobsen SJ, Marmont AM, McGlave PB, Messner HA, Rimm AA, Rozman C, Speck B, Tura S, Weiner RN, Bortin MM: Bone marrow transplantation for chronic myloid leukemia in chronic phase: Increased rate of relapse associated with T-cell depletion. AM Intern Med 108:806, 1988 3. Marks DI, Hughes TP, Szydlo R, Kelly S, Cullis JO,Schwarer AP, Mackinnon S, Apperley J, Barrett J, Hows JM, Goldman JM: HLA-identical sibling donor marrow transplantation for chronic myeloid leukaemia in first chronic phase: Influence of GVHD prophylaxis on outcome. Br J Haematol 81:383, 1992 4. Martin PJ, Clift RA, Fisher LD, Buckner CD, Hansen J, Appelbaum FR, DoneyKC, Sullivan KM, Witherspoon RP, Storb R, Thomas ED: HLA-identical marrow transplantation during accelerated-phase chronic myelogenous leukemia: Analysis of survival and remission duration. Blood 72:1978, 1988 5 . Clift RA, Buckner CD, Thomas ED, Bensinger WI, Bowden R, Bryant E, Deeg HJ, Doney KC, Fisher LD, Hansen JA, Martin P, McDonald GB, Sander JE, Schoch G, Singer J, Storb R, Sullivan KM, Witherspoon RP, Appelbaum FR: Marrow transplantation for chronic myeloid leukemia. A randomized study comparing cyclophosphamide and total body irradiation with busulfan and cyclophosphamide. Blood 84:2036, 1994 6. Sullivan KM, Weiden PL, Storb R, Witherspoon RP, Fefer A, Fisher L, Buckner CD, Anasetti C, Appelbaum FR, Badger C, Beatty P, Bensinger W, Berenson R, Bigelow C, Cheever MA, Clift R, Deeg HJ, Doney K, Greenberg P, Hansen JA, Hill R, Loughran T, Martin P, Neiman P, Petersen FB, Sanders J, Singer J, Stewart P, Thomas ED: Influence of acute and chronic graft-versus-host disease on relapse and survival after bonemarrow transplantation from HLA-identical siblings as treatment of acute and chronic leukemia. Blood 73:1720, 1989 7. Horowitz MM, Gale RP, Sonde1 PM, Goldman JM, Kersey J, Kolb H-J, Rimm AA, Ringden 0, Rozman C, Speck B, Truitt RL, Zwaan FE, Bortin MM: Graft-versus-leukemia reactions after bone marrow transplantation. Blood 75:555, 1990 8. Kolb HJ, Mittermuller J, Clemm Ch, Holler E, Ledderose G , Brehm G, Heim M, Wilmanns W: Donor leukocyte transfusions for treatment of recurrent chronic myelogenous leukemia in marrow transplant patients. Blood 76:2464, 1990 9. Cullis JO, Jiang YZ, Schwarer AP, Hughes TP, Barrett AJ, Goldman JM: Donor leukocyte infusions for chronic myeloid leukemia in relapse after allogeneic bone marrow transplantation. Blood 79:1379, 1992 IO. Drogyski WR, Keever CA, Roth MS, Koethe S, Hanson G, McFadden P, Gotttschall JL, Ash RC, van Tuinen P, Horowitz, Flomenberg N: Salvage immunotherapy using donor leukocyte infusions as treatment for relapsed chronic myelogenous leukemia after allogeneic bone marrow transplantation: Efficacy and toxicity of a defined T-cell dose. Blood 82:2310, 1993 1 l . Szer J, Grigg AP, Phillips CL, Sheridan WP: Donor leukocyte infusions after chemotherapy for patients relapsing with acute leukaemia following allogeneic BMT. Bone Marrow Transplant 11:109, 1993 12. Higano CS, Raskind WH, Singer JW: Use of alpha interferon for the treatment of relapse of chronic myelogenous leukemia in chronic phase after allogeneic bone marrow transplant. Blood 80:1437, 1992 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2638 13. Morgan GJ, Janssen JWG, Guo AP, Wiedemann LM, Hughes T, Gow J, Goldman JM, Bartram C R Polymerase chain reaction for detection of residual leukaemia. Lancet 1:928, 1989 14. Gabert 3, Lafage M, Maraninichi D, Thuret I, Carcassonne Y, Mannoni P Detection of residual bcr/abl translocation by polymerase chain reaction in chronic myeloid leukaemia patients after bone-marrow transplantation. Lancet 2.1 125, 1989 15. Martiat P, Maisin D, Philippe MK, Ferrant A, Michaux JL, Cassiman JJ, Van den Berghe H: Detection of residual BCWABL transcripts in chronic myeloid leukaemia patients in complete remission using the polymerase chain reaction and nested primers. Br .l Haematol 75:355, 1990 16. Kohler S, Galili N, Sclar JL, Donlon TA, Blume KG, Cleary ML: Expression of bcr-ab1 fusion transcripts following bone marrow transplantation for Philadelphia chromosome-positive leukemia. Leukemia 4 5 4 1, 1990 17. Sawyers CL, Timson L, Kawasaki ES, Clark SS, Witte ON, Champlin R: Molecular relapse in chronic myelogenous leukemia patients after bone marrow transplantation detected by the polymerase chain reaction. Proc Natl Acad Sci USA 87563, 1990 18. Delfau MH, Kerckaert JP, d’Hooghe MC, Fenausx P, Lai JL, Jouet JP, Grandchamp B: Detection of minimal residual disease in chronic myeloid leukemia patients after bone marrow transplantation by polymerase chain reaction. Leukemia 4: 1, 1990 19. Snyder DS, Rossi JJ, Wang JL, Sniecinski U, Slovak ML, Wallace RB, Forman SJ: Persistence ofbcr-ab1 gene expression following bone marrow transplantation for chronic myelogenous leukemia in chronic phase. Transplantation 51:103, 1991 20. Delage R, Soiffer RJ, Dear K, Ritz J: Clinical significance of BCR-ABL gene rearrangement detected by polymerase chain reaction after allogeneic bone marrow transplantation in chronic myelogenous leukemia. Blood 78:2759, 1991 21. Hughes TP, Morgan GJ, Martiat P, Goldman JM: Detection of residual leukemia after bone marrow transplantation for chronic myeloid leukemia: Role of polymerase chain reaction in predicting relapse. Blood 77:874, 1991 22. Guerrasio A, Martinelli G, Saglio G, Rosso C, Zacaria A, Rosti G, Testoni N, Ambrosetti A, Izzi T, Sessargeo M, Frassoni F, Gasparini P, Chiamenti A, Di Bartolomeo P, Pignatti PF: Minimal residual disease status in transplanted chronic myelogenous leukaemia patients; low incidence of polymerase chain reaction positive cases among 48 long disease free subjects who received unmanipulated allogeneic bone marrow transplantation. Leukemia 6507, 1992 23. Roth MS, Antin JH, Ash R, Valeri TH, Gotlieb M, Silver SM, Ginsburg D: Prognostic significance of Philadelphia chromosomepositive cells detected by the polymerase chain reaction after allogeneic bone marrow transplant for chronic myeloid leukemia. Blood 791276, 1992 24. Thompson JD, Brodsky I, Yunis JJ: Molecular quantification of residual disease in chronic myelogenous leukemia after bone marrow transplantation. Blood 79: 1629, 1992 25. Lee M, Khouri I, Champlin R, Kanarjian H, Talpaz M, TrujilloJ, Freireich E, Deisseroth A, Stass S: Detection of minimal residual disease by polymerase chain reaction of bcr/abl transcripts in RADICH ET AL chronic myelogenous leukaemia following allogeneic bone marrow transplantation. Br J Haematol 82:708, 1992 26. Cross NCP, Feng L, Chase A, Bungey J, Hughes TP, Goldman JM: Competitive polymerase chain reaction to estimate the number of bcr-ab1 transcripts in chronic myeloid leukemia patients after bone marrow transplant. Blood 82:1929, 1993 27. Cross NCP, Hughes TP, Lin F, O’Shea P, Bungey .I, Marks DI, Ferrant A, Martiat P, Goldman JM: Minimal residual disease after allogeneic bone marrow transplantation for chronic myeloid leukaemia in first chronic phase: Correlations with acute graft-versus-host disease and relapse. Br J Haematol 84:67. 1993 28. Arnold R, Janssen JWG, Heinze B, Bunjes D, Hertenstein B, Wiesneth M,Kubanek B, HeimpelH, Bartram CR: Influence of graft-versus-host disease on eradication of minimal residual leukemia detected by polymerase chain reaction in chronic myeloid leukemia patients after bone marrow transplantation. Leukemia 7:747, 1993 29. Miyamura K, Tahara T, Tanimoto M, Morishita Y, Kawashima K, Morishima Y, Saito H, Tsuzuki S, Takeyama K, Kodera Y, Matsuyama K, Hirabayashi N, YamadaH, Naito K,Imai K, Sakamaki H, Asai 0, Miqutani S: Long peristent bcr-ab1 positive transcript detected by polymerase chain reaction after marrow transplant for chronic myelogeous leukemia without clinical relapse: A study of 64 patients. Blood 81:1089, 1993 30. Storb R, Deeg HJ, Whitehead J, Appelbaum F, Beatty P, Bensinger W, Buckner CD, Clift R, Doney K, Farewell V, Hansen J, Hill R, Lum L, Martin P, McGuffinR, Sanders J, Stewart P, Sullivan K, Witherspoon R, Yee G, Thomas ED: Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med 313:729, 1986 31. GehlyGB, Bryant EM, Lee AM,KiddPG, Thomas ED: Chimeric BCR-ab1 messenger RNA as a marker for minimal residual disease in patients transplanted for Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood 78:458, 1991 32. Kwok S, Higushi R: Avoiding false positives with PCR. Nature 339:237, 1989 33. Kaplan EI, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457, 1958 34. Kalbfleish JD, Prentice RI: The Statistical Analysis of Failure Time Data. New York, NY, Wiley, 1980 35. Cox DR, Oakes D: Analysis of Survival Data. London, UK, Chapman and Hall, 1984 36. McGlave P, Bartsch G, Anasetti C, Ash R, Beatty P, Gajewski J, Kernan NA: Unrelated donor marrow transplantation therapy for chronic myelogenous leukemia: Initial experience of the National Marrow Donor Program. Blood 81543, 1993 37. Drobyski WR, Ash RC, Casper JT, McAuliffe T, Horowitz MM, Lawton C, Keever C, Baxter-Lowe LA, Camitta B, Garbrecht F, Pietyga D, Hansen R, Chitambar CR, Anderson T, Flomenberg N: Effect of T-cell depletion as graft-versus-host disease prophylaxis on engraftment, relapse, and disease-free survival in unrelated marrow transplantation for chronic myelogenous leukemia. Blood 83:1980, 1994 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1995 85: 2632-2638 Polymerase chain reaction detection of the BCR-ABL fusion transcript after allogeneic marrow transplantation for chronic myeloid leukemia: results and implications in 346 patients JP Radich, G Gehly, T Gooley, E Bryant, RA Clift, S Collins, S Edmands, J Kirk, A Lee and P Kessler Updated information and services can be found at: http://www.bloodjournal.org/content/85/9/2632.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.







© Copyright 2026