
Prognostic Factors in Agnogenic Myeloid Metaplasia: A
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
Prognostic Factors in Agnogenic Myeloid Metaplasia: A Report on 195 Cases
With a New Scoring System
By Brigitte Dupriez, Pierre Morel, Jean L. Demon/, Jean L. Lai, Marc Simon, Isabelle Plantier, and Francis Bauters
We studied the survival of 195 patients with agnogenic myeloid metaplasia (AMM) diagnosed between 1962 and 1992
in an attempt to stratify patients into risk groups. Median
survival was 42 months. Adverse prognosticfactors for survival were age > 60 years, hepatomegaly, weight loss, low
hemoglobin level (Hb), low or very high leukocyte count
(WBC), high percentage of circulating blasts, male sex, and
low platelet count. A new scoring system based on two
adverse prognostic factors, namely Hb e 10 g/dL and WBC
e 4 or >30 x l@/L, was able to separate patients in three
groups with low (0 factor), intermediate (1 factor), and high
(2 factors) risks, associated with a median survival of 93,
26, and 13 months, respectively.An abnormal karyotype (32
cases of 94 tested patients) was associated with a short
survival, especially in the low-risk group (median survival of
50 v 112 months in patients with normal karyotype). The
prognostic factors for acute conversion were WBC > 30 x
10s/L and abnormal karyotype. Thus, hemoglobin level and
leukocyte count provide a simple prognostic model for survival in AMM, and the adverse prognosticvalue of abnormal
karyotype may be related to a higher rate of acute conversion.
0 1996 by The American Society of Hematology.
A
single agent oral chemotherapy (hydroxyurea, 78 cases; busulfan, 12
cases; pipobroman, 10 cases); 27 patients with cytopenias received
androgen; 25 patients underwent splenectomy, usually when other
treatments failed; and 3 elderly patients had splenic irradiation because of surgical contraindication.
Prognostic factors analyzed. The following initial characteristics were analyzed in all patients: age, sex, spleen size, hepatomegaly, weight loss, hemoglobin concentration (Hb), white blood cell
count (WBC), platelet count, percentage of circulating blasts, percentage of immature granulocytes (IG, excluding blasts), reticulocyte
count, and MF staging at BM biopsy. Njoku and Visani scoring
Njoku et a15identified four classes of decreassystems were
ing survival from I to IV, by using Hb level (classes 1 to 11, >10
g/dL; classes I11 and IV, < 10 g/dL) and reticulocyte count (classes
I and IV, <2 %; classes I1 to 111, >2%). Visani et a12 identified
three prognostic subgroups by taking the following adverse prognostic factors into account: Hb < 10 g/dL and percentage of WBC
precursors (blasts, promyelocytes, and myelocytes) > 10%. Low-risk
patients had no adverse prognostic factor, intermediate-risk patients
only had anemia, and high-risk patients had WBC precursors >
lo%, independent of Hb level.
Statistical analysis. All analyses were performed with the statistical application system (SAS) software (SAS Institute Inc, Cary,
NC). The closing date was June 1, 1994. The survival curves were
drawn by the Kaplan-Meier product limit method.” Survival was
measured from diagnosis to death or last follow-up. Progression to
ANLL was defined by the presence of >30% BM blasts or >20%
PB blasts. Statistical comparisons between actuarial survival curves
were based on log rank and Cox tests.
The parameters significant at the .05 level for survival were introduced in a first proportional hazards model regression analysis of
survival (Cox model) with the forward stepwise ~election.’~
The
GNOGENIC MYELOID metaplasia (AMM)is a myeloproliferative disorder characterized by bone marrow
(BM) fibrosis and extramedullary hematopoiesis. Individual
clinical course ranging from 1 to over 30 years has been
reported, with a median survival of approximately 4 years
from diagnosis.’-’ Progressive marrow failure, transformation into acute nonlymphoblastic leukemia (ANLL), and portal hypertension (PHT) are the major causes of death. Several
clinical and biological prognostic parameters have been studied, with varying and sometimes conflicting results, except
for anemia, constantly associated with short survival.’-7In
addition, we previously reported the adverse prognostic
value of abnormal karyotype.6 In this study on 195 AMM
patients, we report a prognostic analysis of survival and
progression to ANLL and PHT.Using multivariate analysis,
we develop a new simple scoring system for clinical use and
confirm the independent prognostic value of cytogenetics.
MATERIALS AND METHODS
Patients. Between January 1962 and December 1992, we diagnosed AMM in 195 patients. All patients fulfilled the polycythemia
vera study group criteria for A M M ,which were splenomegaly, red
cell poikilocytosis, leukoerythroblastosis, absence of monocytosis,
BM fibrosis without any identifiable cause, and absence of Philadelphia chromosome.’ Patients with postpolycythemia myelofibrosis
(MF), acute (malignant) MF, and myelodysplastic syndromes with
MF were excluded?
Hematologic examinations were performed by standard methods:
peripheral blood (PB) and BM May-Griinwald-Giemsastained films.
BM trephine biopsy was performed at diagnosis in all patients and
stained with standard and silver stain for reticulin fibers; three stages
of MF were defined according to the usual classification.”
Cytogenetic analysis was available at diagnosis in 94 of 133 patients diagnosed since 1980 (48.2% of the whole group). Metaphases
were obtained on BM or blood samples, after short-term (24 hours)
culture without stimulation. Chromosomes were analyzed with conventional Giemsa stain and the R banding technique and classified
according to the Intemational System for Cytogenetic Nomenclature.” Any anomaly present in at least three cells was considered
clonal.
Treatment. Treatment was based on age, presence of a poor
performance status, importance of cytopenias, or myeloproliferative
features. More precisely, 34 asymptomatic patients received no treatment and 52 received supportive care only (essentially transfusion).
One hundred nine patients received at least one of the following
therapies: 82 patients with very large or symptomatic splenomegaly
and very high white cell or platelet counts received one or more
81004VOI 88, NO 3 (August 1). 1996: pp 1013-1018
From the Service des Maladies du Sang, the Service de Cytogdndtique, Centre Hospitalier Rdgional et Universitaire de Lille; the
Service d’Hdmatologie Clinique, Centre Hospitalier de Lens; the
Laboratoire, Hdpital Saint Vincent, Lille; The Service d’Hdmtologie Clinique, Centre Hospitalier Gdndral de Valenciennes, France.
Submitted November 27, 1995; accepted March 27, 19%.
Address reprint requests to Brigitte Dupriez, MD, Service d ’ H d m tologie Clinique, Centre Hospitalier Dr Schafier, 62307 Lens
Cedex, France.
The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with 18 U.S.C.section 1734 solely to
indicate this fact.
0 1996 by The American Society of Hematology.
0006-497I/96/8803-0023$3.00/0
1013
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1014
DUPRIEZ ET AL
procedure was stopped when the P for entering an additional factor
was above .05. Using the UNIFORM function of the SAS software,
we randomly divided the 195 patients into a training and a test
subsets containing 130 and 65 cases, respectively. Thus, we could
develop a prognostic index in the training sample and test it in the
other sample. We carried out a second proportional hazards model
regression analysis of survival (Cox model) with the forward stepwise selection in the training sample. Initial characteristics selected
by this multivariate analysis of survival were included in a third
proportional hazards model regression analysis of survival performed in the training sample with the best selection. Thus, only
two variables were selected for inclusion in a scoring system (named
LILLE score). For routine clinical use, we examined a categorized
model with the two selected variables and their optimal cutoff values.
We validated this model in the test sample and in the overall group
of 195 patients with the log-rank test.
Because karyotype was available in only 94 patients, the prognostic value of this variable (normal v abnormal) was assessed separately
by univariate analysis, and a last Cox model was built with the
following covariates: karyotype and LILLE score.
The prognostic factors for time to death from ANLL or PHT were
analyzed by the log-rank test.
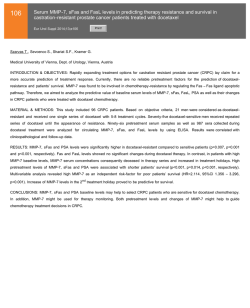
SMR = OIE = I12/20.84 = 5.38
( p < 10-4)
Ob
RESULTS
Initial characteristics and clinical course. There were
105 males and 90 females, with a median age of 65 years
(range 27 to 85). Sixty patients (30.8%) were 5 6 0 years old
and 18 (9.2%) 5 5 0 years. Anemia was present in 139 cases
(71.3%) and Hb < 10 gldL in 44.6%. WBC exceeded 30
X 109/L in 22 cases (11.2%), and 16 patients (8.2%) had
leukopenia. Thrombocytopenia was encountered in 5 1 patients (26.2%) and thrombocytosis in 56 (28.7%). All but 7
patients (3.6%) had immature granulocytes, whereas 104
patients (53.3%) had PB blasts with a percentage 2 5% in
only 19 cases (9.7%). Thirty-two patients (34%) had clonal
chromosomal abnormalities, present either in all cells (19
cases) or coexisting with normal metaphases (13 cases with
a mosaicism): de12Oq (11 cases); dell3q (8 cases); trisomy 8
(4cases); trisomy 21 or add (21) @11) (2 cases); de1(12)(q22)
(2 cases); -Y (2 cases); and several others, accounting for
one case each del(S)(pl4), -12, -17, -18, dup(l)(q32;q44),
der(l7) t(12; 17)(q24;qll), 12, +19, t(13; 17)(q31;q22), t(1;7)
(p31;p22), t(9;21)(p23;qll). Seven subjects exhibited complex
aberrations. Patients with abnormal karyotype presented with
weight loss more frequently than other patients (P = .02). No
other difference in initial characteristics were found.
With a median follow-up of 36 months, the median survival of the 195 patients was 42 months (range 1 to 228).
At the time of the analysis, 148 patients (75.9%) had died,
40 were still alive 16+ to 216+ months from diagnosis, and
7 (3.6%) were lost to follow-up. The actuarial survival rates
at 2 and 5 years were 68% 5 3% and 40% 2 4%, respectively
(Fig 1).
Thirty-three patients (22.3%) died from BM failure (severe anemia, infection, or hemorrhage) without ANLL transformation, 22 patients (14.9%) from ANLL transformation,
16 patients (10.8%) from PHT, 6 patients (4%) from
cachexia, 18 patients (12.2%) from cardiovascular complications, 23 patients (15.5%) from unrelated causes, and 30
patients (20.3%) from unknown causes. Sixteen patients developed and died from PHT during the study period, 12 to
0
U
14
S
Y
M
R
M
S
Fig 1. Overall survival of 196 patients. The standard mortality
ratio t.Chniqu.02' comp8md the mort.lity oburved before January
1, 1991 in the 180 p.tknts d i a g n d befora January 1, 1991, the
date of the last reckoning In France, with the mortality exp.ot.d,
during the Jmibr period of timo, in an age-and sex-matchod population of the Region Nod-Pas-de-Calais in Northern France.
159 months (median 84 months) after diagnosis of AMM.
The actuarial cumulative risk of death from PHT was 7% at 5
years. Twenty-two patients developed and died from ANLL
during the study period, 12 to 136 months (median 36
months) after diagnosis of AMM.The actuarial cumulative
risks of death from leukemic transformation at 1 and 5 years
were 2% and 16%, respectively. Treatment of both complications has only been symptomatic and palliative.
Univariate anafysis of survival prognostic factors {Table
1). Hematologic parameters associated with adverse prognostic significance at the .01 level for both log-rank and Cox
tests were, by decreasing order age > 60 years, hepatomegaly, weight loss, low Hb concentration, low or very high
WBC count, high percentage of circulating blasts, male sex,
low platelet count, and abnormal karyotype.
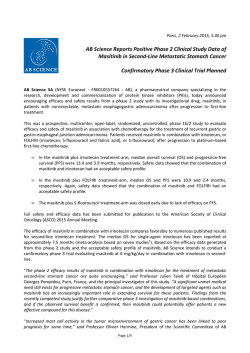
The optimal cutoff value for Hb level was 10 g/a.Both
patients with leukopenia or WBC counts > 30 X 109L
had identical survival (Fig 2). Thus, this variable could be
categorized into two subgroups, namely high-risk patients
with WBC > 30 x 109L or <4 x 10% and low-risk
patients with WBC 4 X lo9& and 5 3 0 X 109L.
The percentage of immature granulocytes, the BM staging,
the spleen size, and the reticulocyte count had no prognostic
value for survival at the .01 level.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1015
PROGNOSIS IN AGNOGENIC MYELOID METAPLASIA
Table 1. Univariate Analysis
Patients
Median Survival
(95% confidence
interval)
66
129
80 (62-1 12)
36 (26-43)
10-4
90
105
64 (47-90)
36 (28-42)
.001
121
74
48 (36-72)
38 (31-49)
.I5
107
88
62 (48-90)
33 (24-37)
10-4
158
37
48 (42-73)
18 (12-33)
10-4
77
97
21
47 (38-59)
38 (30-72)
24 (15-111)
.86
87
108
25 (18-36)
80 (54-96)
10-4
16
158
21
26 (13-48)
48 (38-73)
18 (12-36)
10-4
Fig 2. Survival of 195 patients according to WBC: (0).2 4 x 10'1
L and <30 x IV/L; (+I, <4 x l@/L; and (0I, >30 x lb/L.
51
144
26 (17-48)
48 (38-73)
,002
150
45
49 (42-78)
24 (17-36)
10-4
80
115
59 (43-82)
36 (24-48)
.02
89
64
38 (26-54)
47 (31-79)
.75
62
32
90 (54-112)
36 (27-44)
.003
was available in only 94 patients, this variable was removed
from the subsequent analysis. The Cox proportional hazards
regression method, performed in the overall group of patients
with all significant variables except karyotype, selected six
parameters: Hb level, WBC count, weight loss, age, sex, and
circulating blasts. They are listed in the order entered by the
forward stepwise modeling procedure in Table 2.
A similar forward stepwise regression analysis was performed in the training group of 130 patients. Six variables
were selected: Hb level, WBC count, weight loss, sex, blasts,
and age. Another regression analysis performed with the
best selection in the training sample of patients identified an
No. of
Parameter
Age (yr)
s 60
>60
Sex
Female
Male
Splenomegaly (cm below coastal
margin)
<IO
210
Hepatomegaly
Absent
Present
Weight loss
Absent
Present
BM staging
I
II
111
Hb (e/dL)
<10
210
WBC (xlOa/dL)
<4
4-30
>30
Platelets (xlOg/L)
<150
~150
Circulating blasts (%)
s2
>2
Immature granulocytes (%)
s5
>5
Reticulocytes (xlO*/L)
SI00
>IO0
Karyotype
Normal
Abnormal
P
iili
1
',
0
1)
14
l
d
l
W
R
M
S
m
Table 2. Multivariate Analysis (Stepwise Procedure)
Therapeutic modalities did not influence survival, except
for transfusion; survival of patients who required packed red
cells was shorter than survival of patients who did not (P =
.OOOl). This later correlation was probably related to the
adverse prognostic value of anemia.
As expected, the scoring systems of Njoku and Visani had
a strong prognostic value for survival (P =
However
reticulocytes and WBC precursors (taking into account either
IG alone or IG + blasts and cutoff value of 10% or 15%)
retained no prognostic significance when the analyses were
restricted to the subgroups of patients with a similar Hb level
(< or 210 g/dL).
Multivariate analysis of survival: Development and validation of the scoring system (Table 2). Because karyotype
step
Variable
Entered
Overall population (195 patients)
1
Hb
WBC
2
Weight loss
3
Age
4
Sex
5
Blasts
6
Training set (130 points)
1
Hb
WBC
2
3
Weight loss
4
Sex
Blasts
5
6
Age
Chi-square
P
38.5
40.7
19.0
15.7
11.0
4.8
.0001
.0001
.0001
.0001
.009
.0282
25.9
24.2
13.3
15.1
6.7
6.3
.0001
.OOOl
,0003
.0001
.0094
.0116
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1016
DUPRIEZ ET A1
Table 3. LlLLE Scoring System (For Predicting Survival in AMM)
Adverse prognostic factors
Hb <IO g/dL
WBC <4 or >30 x 109/L
The scoring system (number of adverse prognostic factors)
Factor
No.
Risk Group
Cases (96)
Median
Survival (mo)
0
Low
Intermediate
High
41
45
8
93
26
13
1
2
optimal model including two covariates: Hb level and WBC
count. These two variables and their optimal cutoff values
were included in a categorized Cox model. This model was
nearly as effective (Wald chi-square 45.3) as the continuous
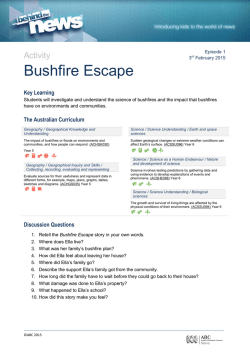
model (Wald chi-square 52.9). We established a numerical
scoring index with the same code system as the categorized
regression model. A scoring system (Table 3)was constructed with the two major variables: Hb and WBC. One
point each was allocated for Hb < 10 g/& and WBC < 4
X 109/L or >30 X 109/L. The total score (addition of the
points for the two variables) separated the patients of the
training group ( P = .OOOl), the test group ( P = .002), and
the overall population into three subgroups. Low-risk patients (score 0; 47% of 195 patients), intermediate-risk patients (score l ; 45% of 195 patients), and high-risk patients
(score 2; 8% of 195 patients) had a median survival of 93,
26, and 13 months, respectively (chi-square 110, P <
(Fig 3).
U-
04 0.i .
01-
j 05 -:
j
4
:
0.4 ;
m
f
Uf
S :
01:
01;
0.0 -
0
11
14
36
M
60
12
M
I
m
Fig 3. Survival of 9
l5 patients according to the score: l+J,
highrisk; (Dl, Intermediate risk; and IO ), low-risk.
I
0.i .
01 M-
0
U
14
36
M
I
I
Z
U
O
I
UONns
Fig 4. Survival of patientsaccording to karyotype: (+), normel
and (OJ,abnormal.
Prognostic value of karyotype. An abnormal karyotype
was also associated witha short survival (P = .003)in
the 94 evaluable patients (Fig 4). Sixty of 94 patients with
evaluable karyotype died: 36 of 62 with normal karyotype
and 24 of 32 with an abnormal one.
When the survival analysis was restricted to the karyotyped patients, the scoring system remained highly significant. Cytogenetics retained prognostic value in the low-risk
group (48 cases); indeed, patients with normal karyotype (33
cases) had a mediansurvival of 112 months, whereas patients
with abnormal karyotype (15 cases) had a median survival
of 50 months ( P = .03) (Fig 5).
Prognostic factors of death from ANU or PHT. Only
two variables were found associated with a short time to
death from ANLL: WBC count > 30 X 109/L( P = .OO01)
and abnormal karyotype ( P = .Ol). Eleven deaths were related to acute conversion in the subgroup of patients with
evaluable karyotype: 4 cases occurred in 36 patients with a
normal karyotype (11%) and 7 cases in 32 patients (25%)
with an abnormal one. There was no more leukemic conversion in the splenectomized patients than in other patients: 4
of 25 splenectomized patients died from ANLL (16%).
Five variables were found associated with a short time to
death from PHT:circulating blasts > 2% ( P = .001), weight
loss ( P = .Ol), WBC count > 3O.lO9/L ( P = .02), hepatomegaly ( P = .03) and spleen z 10 cmunder the costal
margin ( P = .M).
DISCUSSION
Despite of a large heterogeneity in median survival, several attempts have been made to identify clinical and labora-
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1017
PROGNOSIS IN AGNOGENIC MYELOID METAPLASIA
and, more recently, cytogenetic studies and plasma soluble
interleukin-2 receptors. On BM biopsy, decreased marrow
cellularity and higher degree of fibrosis (III > I1 > I) was
considered of adverse prognostic value," as was pattern of
BM aplasia.' Patients with mild hepatic myeloid metaplasia
M(HMM) survived longer than those with marked HMM in a
clinicopathologic study of 22 cases.I4
01 Ferrokinetic studies provided sometimes conflicting results. A lower red cell volume was highly significant but not
a larger plasma volume for Najean et al," and conversely for
Njoku et a15; lower erythroid iron incorporation and higher
hemolysis were also found ~ejorative'~;
and a pattern of
erythroid failure, described as class III by Barosi et al,1*16
usually correlated with BM aplasia, carried a bad prognostic
witha high incidence of acute conversion. However, by
multivariate analysis, only routine clinical and hematologic
parameters retained prognostic value in our series as in others. Varki et a14 identified three risk groups on the basis
of constitutional symptoms, platelet count, and Hb level.
DJ Although most multivariate analyses agreed for the prognostic value of anemia, the other independent prognostic vari01ables remained controversial. Njoku et a15 proposed a score
based on Hb and reticulocyte count. Barosi et a l l built a
0
U
11
X
U
~
R
M
~
prognostic
classification
tree in a series of 137 patients with
age,
Hb
level,
percentage
of immature myeloid cells, and
m
histologic or isotopic BM features. Finally, Visani et a
l'
Fig 5. Survival of patients with low-risk score accordingto karyoidentified three prognostic subgroups by taking into account
type: (+l, normal and (0).
abnormal.
percentage of WBC precursors and Hb concentration. These
scores had strong prognostic value for survival; however,
their prognostic value in the present series was probably
only provided by Hb level. The prognostic index presented in
tory features predicting survival. A short delay (<13 months)
this report based only on two simple hematologic parameters
between first signs and diagnosis,' the presence of constiturecorded at diagnosis (Hb level and WBC count) was able
tional symptoms (fever, night sweats, andor weight loss),'
to divide the patients into three groups withsignificantly
spleen s i ~ e ? ' ~ *liver
' ~ size,' age > 60 years,244.10the
different survival. In contrast with previous reports of progmale sex,'O anemia,'-5.'0"4thrombo~ytopenia,4.'~
reticulocyte
nostic systems, we could validate the present scoring system
count? increased percentage of immature granulocytes, a n d
in a test population.
or of circulating
have all been found to influence
The difference between our results and those of other
survival. In the present study on 195 patients, until now the
published series might be due to the following reasons: the
largest study in A " , the clinical and hematologic features
varying criteria for diagnosis (including or not postpolycyare similar to those reported in other large series. Univariate
themic MF, acute MF, or myelodysplasia with MF), the
analysis confirmed the prognostic value of most previously
large heterogeneity of features and outcome in A " , and
reported factors, especially anemia.'".'0.'4 Thrombocytopenia
the large number of subjects required for the Cox propormoderately affected survival and was not selected in multitional hazard model.
variate analysis, probably because of a correlation with aneWe previously reported the adverse prognostic value of
mia, as previously demonstrated: Reticulocyte count, spleen
abnormal karyotype: first suggested, albeit indirectly, in
size, and BM staging had no prognostic value. To our knowl1982 by Besa et all8 and recently confirmed by Reilly et al.I9
edge, this is the first time that the leukocyte count at diagnoThe adverse prognostic value associated with an abnormal
sis has been shown to be highly significant, for survival,
karyotype among our low-risk patients suggested that the
both in univariate and in multivariate analysis; both leukopepresent scoring system might be improved by cytogenetics.
nia and high leukocytosis (>30 X 109/L)were associated
The insufficient number of patients with available karyotype
with short survival. The percentage of circulating blasts was
at the time of the analysis precluded the selection of this
also significant, but at a lower degree, in multivariate analyparameter in multivariate analysis.
sis, and the percentage of immature granulocytes had only
a moderate significant effect. Previous studies found progFew series reported on the prognostic factors for progresnostic value of immature granulocytes andor blasts,'.3 but
sion to AML. High percentage of WBC precursors was assocomparison is difficult as their definition of WBC precursors
ciated with frequent progression to AML and short survival
included blasts and metamyelocytes.
in twp previous studies." We found that high WBC count
Other prognostic factors have been des~ribed,'.~,'~.'~"~
m'
was associated with more frequent death from acute convercluding BM biopsy, liver biopsy, ferrokinetic parameters,
sion, but high WBC precursors count was not. Patients with
7
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1018
DUPRIEZ ET AL
abnormal karyotype also carried a high risk of progression
to AML, as suggested in our previous report^.^.^ These results
are partially different from those of Reilly et al,I9 who only
demonstrated a shorter survival for patients with abnormal
karyotype and not increased risk of ANLL. Finally, an unexpected high rate of blastic transformation was observed in a
recent study on 7 1 splenectomized patients, without significantly different survival.2o
In conclusion, our study shows that the combination of
Hb level and leukocyte count provides a useful and simple
prognostic model for survival in AMM. In addition, we confirm the adverse prognostic value of abnormal karyotype,
probably related in part to an increased risk of acute conversion. Treatment of A“ is still controversial. Our staging
system could be useful to identify patients with limited life
expectancy, for whom new therapeutic approaches might be
investigated, mainly BM transplantation in younger ones.
REFERENCES
1. Barosi G, Berzuini C, Liberato LN, Costa A, Polino G, Ascari
E: A prognostic classification of myelofibrosis with myeloid metaplasia. Br J Haematol 70:397, 1988
2. Thiele J, Kvasnicka HM, Steinberg T, Zankovich R, Fischer
R, Diehl V: Survival in primary (idiopathic) osteomyelofibrosis, socalled agnogenic myeloid metaplasia. Leuk Lymph 6:389, 1992
3. Visani G, Finelli C, Castelli U, Petti MC, Ricci N. Vianelli N,
Gianni L, Zuffa E, Aloe Spiriti MA, Latagliata R, Pileri S, Magrini
U, Gugliota L, Mona E, Bernasconi C, Mandelli F, Tura S: Myelofibrosis with myeloid metaplasia: Clinical and haematological parameters predicting survival in a series of 133 patients. Br J Haematol
75:4, 1990
4. Varki A, Lottenberg R, Griffith R, Reinhard E: The syndrome
of idiopathic myelofibrosis. A clinico-pathologic review with emphasis on the prognostic variables predicting survival. Medicine
62:353, 1983
5. Njoku OS, Lewis SM, Catovski D, Gordon-Smith EC: Anaemia in myelofibrosis: Its value in prognosis. Br J Haematol 54:79,
1983
6. Demory JL, Dupriez B, Fenaux P, Lai’ JL, Beuscart R, Jouet
JP, Deminatti M, Bauters F: Cytogenetic studies and their prognostic
significance in agnogenic myeloid metaplasia: A report on 47 cases.
Blood 72:855, 1988
7. Dupriez B, Demory JL, Lai JL, Fenaux P, Bauters F, Barosi
G: Prognostic classification of myelofibrosis with myeloid metaplasia. Br J Haematol 73:136, 1989 (letter)
8. Laszlo J: Myeloproliferative disorders (MPD): Myelofibrosis,
myelosclerosis, extramedullary hematopoiesis, undifferentiated
MPD and hemorrhagic thrombocytemia. Semin Hematol4:409, 1975
9. Bearman RM, Pangalis GA, Rappaport H: Acute (“malignant”) myelosclerosis. Cancer 43:279, 1979
10. Chelloul N, BriBreJ, Laval-Jeantet M, Najean Y, Vorhauer W,
Jacquillat C: Prognostic of myeloid metaplasia with myelofibrosis.
Biomedicine 24:272, 1976
11. ISCN: An international system for human cytogenetic nomenclature. Cytogenet Cell Genet 21:309, 1978
12. Kaplan EL, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457, 1958
13. Cox DR: Regression models and lifetables (with discussion).
JR Stat SOC34:187, 1972
14. Pereira A, Bruggera M, Cervantes F,Rozman C: Liver
involvement at diagnosis of primary myelofibrosis. A clinicopathological study of twenty-two cases. Eur J Haematol 40:355, 1988
15. Najean Y, Cacchione R, Castro Malaspina H, Dresch C:
Erythrokinetic studies in myelofibrosis: Their significance for prognosis. Br J Haematol 40205, 1978
16. Barosi G, Cazzola M, Frassoni F, Orlandi E, Stefanelli M:
Erythropoiesis in myelofibrosis with myeloid metaplasia: Recognition of different classes of patients by erythrokinetics. Br J Haematol
48:263, 1981
17. Wang JC, Wang A: Plasma soluble interleukin-2 receptor in
patients with primary myelofibrosis. Br J Haematol 86:380, 1994
18. Besa EC, Nowell PC, Geller NL, Gardner FM: Analysis of
the androgen response of 23 patients with agnogenic myeloid metaplasia. The value of chromosomal studies in predicting response and
survival. Cancer 49:308, 1982
19. Reilly S T , Wilson G, Barnett D, Watmore A, Potter A: Karyotypic and ras gene mutational analysis in idiopathic myelofibrosis.
Br J Haematol 88575, 1994
20. Barosi G, Ambrosetti A, Buratti A, Finelli C, Liberato NL,
Quaglini S, Ricetti MM, Visani G, Tura S, Ascari E: Splenectomy for
patients with myelofibrosis with myeloid metaplasia: Pretreatment
variables and outcome prediction. Leukemia 7:200, 1993
21. Breslow NE, DayNE: The standardized mortality ratio, in
Sen PK Biostatistics (eds): Statistics in Biomedical, Public Health
and Environmental Sciences. New York, NY, North-HollandElsevier Science Publishers BV, 1985, p 55
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1996 88: 1013-1018
Prognostic factors in agnogenic myeloid metaplasia: a report on 195
cases with a new scoring system [see comments]
B Dupriez, P Morel, JL Demory, JL Lai, M Simon, I Plantier and F Bauters
Updated information and services can be found at:
http://www.bloodjournal.org/content/88/3/1013.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.






© Copyright 2026