
Statins in the treatment of chronic heart failure: Biological and
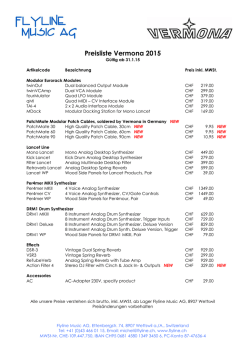
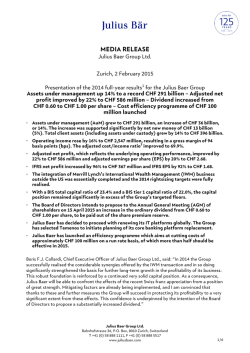
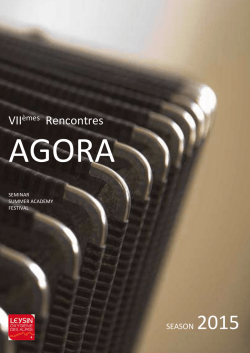
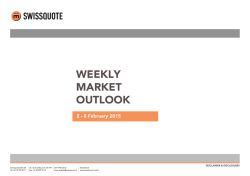
Cardiovascular Research 71 (2006) 443 – 454 www.elsevier.com/locate/cardiores Review Statins in the treatment of chronic heart failure: Biological and clinical considerations Pim van der Harst a,⁎, Adriaan A. Voors a , Wiek H. van Gilst b , Michael Böhm c , Dirk J. van Veldhuisen a a Department of Cardiology, Thoraxcenter, University Medical Center Groningen, University of Groningen, Hanzeplein 1, 9700RB Groningen, The Netherlands b Department of Clinical Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands c Klinik and Poliklinik Innere Medizin III, Universitat des Saarlandes, Homburg, Germany Received 5 February 2006; received in revised form 6 April 2006; accepted 19 April 2006 Available online 27 April 2006 Time for primary review 24 days Patients with increased cholesterol levels are at increased risk to experience cardiovascular events and to die from vascular disease. Statins have been proven to effectively reduce cholesterol levels and subsequently reduce cardiovascular events in patients with coronary artery disease or at increased risk to develop coronary artery disease. However, in patients with chronic heart failure (CHF), not high, but low levels of cholesterol are related to increased mortality. This phenomenon of reverse epidemiology is not unique to CHF, but also exists in other critical diseases and in the elderly in general as well. An important rationale has been provided by the endotoxin hypothesis, which suggests that cholesterol has an important scavenger function regarding harmful endotoxins. Indeed, these lines of evidence predict a harmful effect of statin treatment in patients with CHF. However, statins not only lower cholesterol, but also have been reported to exhibit a plethora of pleiotropic effects, including reduction of inflammation and improvement of endothelial function. In order to reconcile these contradictory lines of evidence, it is necessary to examine the pharmacological mechanisms of effects of statin treatment. Understanding the pharmacology of statin intervention in CHF models and patients may facilitate the development of therapeutic strategies. In this review, we provide an overview of the known associations between serum cholesterol and CHF in human subjects. In addition, we review the available lines of evidence in animal models and humans predicting both harmful and beneficial effects of statin treatment in CHF. We emphasize the importance of additional research specifically in CHF models and patients. © 2006 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: Chronic heart failure; Statins; Cholesterol; HMG-CoA reductase inhibitors The efficacy of 3-hydroxy-3-methylglutaryl co-enzymeA inhibitors, or statins, in reducing morbidity and mortality in patients with documented coronary artery disease (CAD) or those at increased risk of CAD has been overwhelmingly and indisputably demonstrated [1–15]. The result is that statin therapy is the treatment of choice in the primary and secondary prevention of cardiovascular disease for almost every suitable patient. But what if statin treatment has not been initiated? Is it still beneficial to begin statin treatment in ⁎ Corresponding author. Tel.: +31 503612355; Tel./fax: +31 503614391. E-mail address: [email protected] (P. van der Harst). end stage CAD that has resulted in chronic heart failure (CHF)? Or might we do more harm than good? Evidence for statin treatment in patients with established chronic heart failure (CHF) has not been well established and remains a subject of debate [16,17]. CHF patients have been systematically excluded from large clinical statin trials. Although a few smaller, uncontrolled trials do provide some evidence for the use of statins in CHF, there is some reason to think that statins may have harmful effects in patients with CHF. For example, recent data suggests that high cholesterol levels are beneficial in a state of CHF, even when CAD coexists. In this article, the potentially harmful and beneficial 0008-6363/$ - see front matter © 2006 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.cardiores.2006.04.011 Downloaded from by guest on February 6, 2015 Abstract 444 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 effects of statins in CHF patients will be reviewed, both from a pathophysiological and a clinical perspective. 1. Cholesterol in CHF 2. Potentially harmful effects of statin treatment in CHF Potentially harmful effects of statins in CHF are not farfetched. In addition to the observed inverse relationship between cholesterol and survival in CHF, there are other lines of evidence suggesting adverse effects of statins. Most noteworthy are the endotoxin–lipoprotein hypothesis, the coenzyme Q10 (ubiquinone) hypothesis, and the selenoprotein hypothesis. 2.1. Endotoxin lipoprotein hypothesis Rauchhaus et al. were the first to propose that higher levels of cholesterol are beneficial in CHF on the basis of the ability of serum lipoproteins to modulate the inflammatory immune function [41]. CHF patients have increased serum cytokine levels, which might be linked to increased endotoxin levels [42]. Circulating cholesterol- and triglyceride rich lipoproteins are natural nonspecific buffers of endotoxins (Fig. 1). They have the capacity to bind and detoxify bacterial lipopolysaccharides (LPS). LPS are very strong stimulators of the release of inflammatory cytokines from circulating immune competent cells and LPS are an important stimulus of proinflammatory cardio-depressive cytokine production in CHF. For example, LDL receptor deficient mice, with consequently very high plasma cholesterol concentrations are protected against lethal endotoxaemia and severe gramnegative infections [43]. Edematous and severely affected CHF patients show substantial immune activation in parallel with raised LPS plasma concentrations, comparable to patients with sepsis and liver cirrhosis [42]. In CHF patients, episodes of endotoxaemia can occur, and lowering of lipoproteins could adversely effect LPS bioactivity modification [41]. This hypothesis suggests that normal patients Downloaded from by guest on February 6, 2015 Hypercholesterolemia is a well-known risk factor for the development of CAD and long-term morbidity and mortality, at least in middle-aged persons. However, controversial associations have been found in elderly patients and in patients with a wide range of chronic and acute diseases [18– 24]. It seems that with advancing age or in critically diseased patients, the traditional association between elevated cholesterol and increased morbidity and mortality no longer applies. In fact, serum cholesterol levels are inversely correlated with in-hospital mortality in patients with infectious diseases [18,19] as well as acutely ill patients [20], regardless of malnutrition, frailty, inflammation, and comorbidity. In the Framingham study, dyslipidemia initially appeared to be a risk factor for the development of CHF [25]. However, subsequent studies have challenged this finding [26–28]. Importantly, in a more detailed analysis of the same Framingham database, the association between total cholesterol and all-cause mortality was positive at 40 years of age, negligible at 50–70 years, and negative at age 80 years and above [29]. Since both the incidence and prevalence of CHF is increasing steeply with age, the accepted association between cholesterol and CHF might change [30]. Several observational studies have addressed the relationship between serum cholesterol levels and outcome, specifically in CHF patients. In 1998, Vredevoe et al., were the first to report that lower total cholesterol was significantly associated with increased mortality in patients with advanced, idiopathic CHF [31]. This observation has been confirmed in other studies, indicating that both in ischemic and nonischemic CHF, higher cholesterol levels are associated with decreased mortality [32–37]. Based on Receiver Operating Characteristic (ROC) curves analysis, the best cut-off level for total cholesterol in predicting mortality in CHF patients is estimated to be around 4.9–5.2 mmol/L (190–200 mg/dL) [32,35]. Mortality increased 25% for each mmol/L decrease in total cholesterol. This phenomenon of ‘reverse epidemiology’ in CHF has not only been observed for serum cholesterol levels, but also for body mass index and blood pressure [38]. Nevertheless, previously mentioned studies were observational and do not prove causality. Low cholesterol could merely be a consequence of advanced CHF, without a causal role, or high cholesterol could be an indicator of a greater metabolic reserve to deal with the disease [39,40]. Although several studies corrected for general health indicators, like nutritional status, and cachexia, it remains possible that low cholesterol carries a poor prognosis because it is a marker of poor health or a consequence of CHF. Consequently, the association with mortality could be a consequence of inadequate adjustment for other confounding factors. Alternatively, lower mortality among patients with elevated cholesterol could be a consequence of a selection bias. Patients surviving elevated cholesterol could represent a selected subgroup with advantageous genetic or other characteristics that protect them from the harmful effects of high cholesterol. Finally, lower cholesterol might just mark an end-stage disease epiphenomenon, due to reduced hepatic cholesterol synthetic capacity. Any of the aforementioned possibilities do not exclude the possibility that cholesterol may, even in a state of CHF, still be a pro-atherogenetic factor. Further research into the mechanism to explain the inverse associations remains obligatory. Since it has not been established whether low cholesterol is causally involved or is simply a marker, interventions aimed at lowering cholesterol will remain controversial. However, such an association between increased mortality and lipid lowering therapy has as yet not been demonstrated. Although high cholesterol seems advantageous in elderly patients, treatment with statins does not necessarily cause harm in these patients [8,10]. These seemingly contradictory findings might thus be explained by a difference in intrinsicly low cholesterol levels as compared to pharmacologically induced low cholesterol levels. P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 445 with CAD should be treated differently from patients with ischemic CHF. 2.2. Ubiquinone hypothesis The mode of action of statins through the inhibition of mevalonate synthesis, decreases the production of ubiquinone (Coenzyme Q10; Fig. 1). Indeed, in humans, statins have been shown to cause decreased levels of ubiquinone in several studies [44–46]. In the heart, ubiquinone is most abundant and represents an essential component of the mitochondrial respiratory chain. Ubiquinone is involved in the production of ATP and is therefore related to the metabolic demands of cells (Fig. 1) [47–50]. Another fundamental characteristic of ubiquinone is its antioxidant (free radical scavenging) property. By affecting mitochondrial function through ubiquinone, statins might have deleterious effects on skeletal or cardiac muscles. This mechanism is thought to be involved in toxic myopathy, an adverse effect of statins, and might also be relevant in cardiac muscle. This hypothesis is supported by the finding that in CHF patients, deficiencies of ubiquinone have been found frequently, and are more prominent with increasing NYHA class [51]. The reported decrease of ubiquinone with statin treatment, in both animal and human experimental studies, might therefore be harmful in CHF [44–46]. A clinical trial in CHF evaluating the efficacy of ubiquinone as an adjunctive treatment in major adverse cardiovascular events is currently ongoing [52]. 2.3. Selenoprotein hypothesis Reduction of mevalonate results in the reduction of isopentenyl-pyrophosphate (Fig. 1). Selenocysteine-tRNA[Ser]sec (Sec-tRNA) controls the expression of all selenoproteins [53]. However, Sec-tRNA is only functional after essential post-transcriptional modification, one of which is the isopentenylation of adenoseine. Isopentenylation of Sec-tRNA is undertaken by tRNA isopentenyl transferase, which uses isopentenyl pyrophosphate (Fig. 1) as a substrate [54]. The seloprotein hyopthesis postulates that statins interfere with the mevalonate pathway, which interferes with the Downloaded from by guest on February 6, 2015 Fig. 1. The hypothetical effects of statins on Chronic Heart Failure through the intermediates of the mevalonate pathway. HMG-CoA: 3-hydroxy-3methylglutaryl co-enzyme-A; Sec-tRNA: Selenocysteine-tRNA[Ser]sec; Farnesyl-PP: Farnesyl pyrophosphate; t-t GGPP: trans–trans geranylgeranyl diphosphate; ATP: adenosine triphosphate; AT-1 receptor: angiotensin II type 1 receptor; NADPH: nicotinamide adenine dinucleotide phosphate-oxidase; eNOS: endothelial nitric oxide synthase. 446 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 enzyme isopentenylation of Sec-tRNA, and consequently statins prevent its maturation to a functional tRNA molecule [55]. Indeed, a strongly reduced selenoprotein synthesis has already been demonstrated in cell culture after the addition of lovastatin [56]. Considering that individuals with statin-induced myopathy have very similar clinical and pathological features to those with syndromes associated with severe selenoprotein deficiency, the fall in available selenoproteins might be particularly harmfull in CHF [55]. 3. Potential beneficial effects of statin treatment in CHF Besides reduction in cholesterol, statins also influence other isoprenoid intermediates of the cholesterol biosynthetic pathway (Fig. 1). These intermediates are key moieties for posttranslational modification of numerous proteins. Some of these influences are of particular interest in CHF. 3.1. Capillary density and vascular function (Fig. 4A) [75]. This effect of statins on angiogenis is highly dependent on eNOS and is absent in eNOS deficient mice (Fig. 4B) [76]. Recently, the effects of statins on circulating endothelial progenitor cells in humans have been reported [77,78]. These findings might provide another explanation for the possible beneficial effects of statins on capillary density and vascular function in CHF patients. 3.2. Neurohormonal activation The principal neurohormonal systems involved in the pathophysiology of CHF are the renin–angiotensin–aldosteron system and the sympathic system. Therapies aimed at modifying activation of these systems, such as angiotensinconverting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARB), aldosteron inhibitors and beta-blockers have all been proven to be beneficial in the treatment of CHF. However, statins also modify these neurohormonal systems. In humans, high levels of cholesterol are known to increase the expression of angiotensin type 1 receptors, and consequently amplify the biological effects of angiotensin II [79]. In this regard, it is of particular interest that increased expression of cardiac angiotensin type 1 receptors is related to decreased myocardial microvessel density after experimental myocardial infarction [80]. Recently, we have demonstrated that vasoconstrictor responsiveness to angiotensin II can be modified by statin treatment in patients with diseased coronary arteries [81]. Oral treatment with statins inhibits rac1-GTPase activity and reduces angiotensin II induced NADPH oxidase activity, and subsequent oxidative stress, and might therefore be of particular relevance in the ventricles of CHF patients [82]. Additionally, statins can Downloaded from by guest on February 6, 2015 Coronary blood flow reserve is strongly and inversely related to serum cholesterol levels [57,58]. Several studies have indicated that in patients with normal left ventricular function, cholesterol lowering drug therapy can improve coronary blood blow [59,60]. These effects can be observed very quickly after cholesterol lowering, as has been shown by single LDL apheresis, which improved coronary blood flow within 24 h [61]. CHF is characterized by a relative microvascular insufficiency. The increase in myocytes in both thickness and length is not adequately matched by a proportional increase in vasculature. In animal studies, it has been found that the eccentric hypertrophy associated with CHF lacks the compensatory angiogenesis, in contrast to physiological (i.e. exercise or anemia-induced) hypertrophy of the heart [62,63]. Consequently, in patients with increased cholesterol levels and CHF, coronary flow reserve is jeopardized for two reasons (Fig. 2). A recent study from Japan showed that cardiac function in CHF patients was improved after statin treatment in parallel with decreasing inflammation [64]. It is tempting to speculate that an increase in coronary blood flow was responsible for this effect [65]. Furthermore, dysfunction of the endothelium, in both coronary and peripheral arteries, and independently of serum cholesterol has been well documented in patients with CHF [66,67]. Endothelial dysfunction in CHF patients was associated with increased mortality risk [68]. Endothelial dysfunction in CHF is thought to reflect predominantly decreased NO bioavailability (Fig. 3) [69]. Indeed, the effects of statins on eNOS are the basis of the well described favourable effects of statins on endothelial dependent vasomotor function [70–73]. In patients with documented CAD, statins reduced transient myocardial ischemia [74]. Their anti-ischemic properties are thought to be a consequence of protein kinase Akt activation, subsequently promoting collateral growth and increasing capillary density Fig. 2. Three-dimensional bar graph showing hypothetical relation of decreased coronary blood flow reserve (vertical axis) in relation to increasing levels of cholesterol (horizontal axis) and decreasing Left Ventricular Ejection Fraction (LVEF; diagonal axis). Coronary blood flow is reduced in hypercholesterolemia [57,58] and in CHF a relative microvascular insufficiency exists [62,63]. Therefore, in patients with increased cholesterol levels and CHF, coronary flow is jeopardized for two reasons. P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 447 Downloaded from by guest on February 6, 2015 Fig. 3. Simplified schematic overview of the known processes involved in atherosclerosis and the established effects of statin treatment. Fig. 4. (A) Adapted with permission from Kureishi et al. [75]. Alkaline phosphatase staining of the adductor muscle from ischemic limbs showing greater capillary density in statin treated animals (statin = 253 ± 23 capillaries/mm2; control = 163 ± 9 capillaries/mm2); P < 0.01. (B) Adapted with permission from Landmesser et al. [76]. Effect of statin treatment on capillary density in infarct border zone of wild type (WT) and eNOS−/− mice after myocardial infarction (MI). Average number of endothelial cells per high-powered field in border zone for each experimental group is shown, as determined by platelet and endothelial cell adhesion-molecule immunohistochemical staining. 448 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 inhibit VEGF-induced ACE upregulation in endothelial cells [83] and enhance the efficacy of angiotensin receptor blockers [84–87]. Besides the renin–angiotensin system, statins can also modify the sympathetic system. β-Adrenergic receptor stimulation of cardiac myocytes leads to apoptosis. In rats, statins inhibit β-adrenergic receptor activation of Rac1 and consequently inhibit the activation of the mitochondrial death patways and apoptosis [88]. Statin treatment also decreases sympathetic activity and delays the time of onset of cardiac decompensation in pacing-induced dilated cardiomyopathy in dogs [52,53]. 3.3. Left ventricular hypertrophy (LVH) 3.4. Atherosclerosis Statins reduced the progression of coronary atherosclerosis in clinical studies [100,101]. Some studies even demonstrated regression of atherosclerotic plaques with high doses of statins (Fig. 3) [102]. 3.5. Inflammation In patients with CHF, elevated systemic levels of inflammatory parameters have been extensively documented and associated with progression of CHF and death [103– 106]. Several clinical trials have demonstrated the efficacy of statin treatment in reducing C-reactive protein [107,108] and other inflammatory markers (Fig. 3) [109,98]. 3.6. Matrix metalloproteinase (MMPs) Recent studies have documented that activated MMPs play an important role in the development of CHF [110]. In experimental studies, production of MMPs was inhibited by statins [111,112]. Inhibition of MMP attenuated cardiac fibrosis and failure in murine models [113]. The clinical relevance of all of these potentially beneficial effects remains to be established in clinical studies. 4.1. Animal experiments Several animal studies have suggested beneficial effects of statins in the treatment of CHF. Cerivastatin treatment (starting 1 week after myocardial infarction) significantly improved left ventricular systolic and diastolic function in rats with CHF after experimental myocardial infarction [114]. In a murine model of CHF after myocardial infarction, treatment with fluvastatin 6 h after infarction increased survival, without affecting infarct size [115]. Fluvastatin not only attenuated LV dilatation, but also decreased LV enddiastolic pressure and improved LV ejection performance. However, not all studies favoured statin treatment in CHF. In female hamsters with inherited cardiomyopathy, lovastatin treatment significantly reduced median survival time from 89 to 30 days [48]. 4.2. Retrospective clinical studies Several post-hoc subgroup analyses from large clinical trials have been published on the effects of statins in CHF. In the Cholesterol and Recurring Events (CARE) trial pravastatin significantly reduced coronary events in patients with decreased left ventricular ejection fractions (LVEF), although the study excluded symptomatic CHF patients and patients with a LVEF < 25% [4]. In the Evaluation of Losartan in Elderly II (ELITE II) trial, a retrospective analysis suggested that symptomatic CHF patients using statins had decreased mortality compared to patients not on statin therapy [116]. The effects of statins on mortality were independent of treatment with either captopril or losartan. The Scandinavian Simvastatin Survival Study (4S) [2] reported a long-term reduction in the development of CHF in patients with a history of myocardial infarction who were randomized to statin therapy [117]. The PROSPER study evaluated the benefits of pravastatin treatment in an elderly cohort with a high risk of developing cardiovascular disease and stroke [10]. Although PROSPER excluded CHF patients with NYHA III/IV, the pre-specified outcome parameter ‘Heart failure hospitalization’ did not differ between pravastatin treated and placebo treated elderly patients (Table 1). A post-hoc analysis of the Heart Protection Study, involving more than 20,000 patients randomized to simvastatin or placebo treatment, reported a non-significant trend toward fewer CHF deaths due to any cause (70 (0.7%) vs. 86 (0.8%) patients; RR 0.81 [0.59–1.10]; P = 0.2), which was supported by a marginally significant reduction in first hospital admission for worsening CHF or CHF death (354 (3.4%) vs. 405 (3.9%); RR 0.86 [0.75–1.00]; P = 0.05) [118]. An important limitation of the Heart Protection Study data was that the presence of heart failure at study entry was not routinely recorded. A subanalysis of the data from the Prospective Randomized Amlodipine Survival Evaluation (PRAISE) trial was aimed at evaluating associations of statin Downloaded from by guest on February 6, 2015 Small G proteins are the molecular switches regulating cardiac hypertophy and fibrosis. Ras, RhoA and Rac1 are key mediators of the hypertrophic response [89,90]. By blocking the synthesis of mevalonate, statins inhibit farnesylation and geranylgeranylation of Ras, RhoA, and Rac (Fig. 1) [91]. By inhibiting Rac, statins can inhibit angiotensin II induced [92–95] and noradrenalin [96] induced cardiac radical production and hypertrophy. In rat models of cardiac hypertrophy, induced by coarctation of the abdominal aorta, simvastatin treatment reduced the development of LVH [97,98]. Simvastatin was even more potent in its reduction of LVH than captopril treatment [98]. Also, pravastatin reduced left ventricular mass in patients with hypertension and hyperlipidemia, on top of anti-hypertensive treatment [99]. 4. Studies on statin therapy in CHF P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 449 Table 1 Large (> 1000 patients) placebo controlled statin trials and CHF patients Trial acronym, date Number of patients Intervention Prevention CHF patients PMSGCRP, 1993 [1] 4S, 1994 [2] WOSCOPS, 1995 [3] CARE, 1996 [4] 1062 4444 6595 4159 Pravastatin 20 mg Simvastatin 10–40 mg Pravastatin 40 mg Pravastatin 40 mg Primary Secondary Primary Secondary Excluded Excluded Excluded Symptomatic CHF excluded AFCAPS/TexCAPS, 1998 [5] LIPID, 1998 [6] MIRACL, 2001 [7] GREACE, 2002 [11] 6605 Primary Excluded 9014 3086 1600 Lovastatin 20–40 mg Pravastatin 40 mg Atorvastatin 80 mg Atorvastatin 24 mg Secondary Secondary Secondary Symptomatic CHF excluded Excluded NYHA IIIb/IV. NYHA III and IV excluded MRC/HPS, 2002 [8] 20,536 Simvastatin 40 mg Secondary Severe heart failure excluded 1677 5804 Fluvastatin 80 mg Pravastatin 40 mg Excluded LVEF < 30% Excluded NYHA III/IV. CARDS, 2004 [15] 10,355 Pravastatin 20–40 mg Secondary Primary/ Secondary Primary 10,305 Atorvastatin 10 mg Primary Excluded Fluvastatin 40 mg and increased to 80 mg after 2 years Atorvastatin 10 mg Renal transplant Not reported Primary Excluded 2102 2838 therapy with total mortality among 1153 patients with severe heart failure (ejection fraction < 30% and NYHA class IIIB or IV symptoms) of ischemic and nonischemic etiologies [33]. Only 134 patients (12%) used a statin, but in multivariate analysis this was associated with a 62% lower risk of death, which represents a major absolute risk difference. In the Optimal Trial in Myocardial Infarction with the Angiotensin II Antagonist Losartan (OPTIMAAL) [119], the effect of initiating statin treatment in heart failure or left ventricular dysfunction in the acute phase after acute myocardial infarction was studied post-hoc [120]. After adjustment for risk variables before inclusion, statin treatment was associated with a 26.1% decreased mortality. However, the reported protective associations of statin use in CHF do not prove causality, and are susceptible to considerable confounders and biases. First, probably the single largest major confounder in non-statin randomised trials can be found in the patient characteristics associated with the choice of the physician to prescribe a statin. Statin treatment could therefore have represented a selected subgroup. Such characteristics may include ones not registered, thus unknown in the study databases and unadjused for in multivariate analysis, e.g. socioeconomic status, and healthy-heart behaviors. A major potential confounder is that patients with a short life expectation will generally not be treated with statins. In addition, since LVEF 26–40% (n = 706); beneficial effect of statin treatment No information on CHF No difference in new or worsening CHF Reduction development of CHF (n = 11 vs. n = 22). Beneficial effect of statin treatment in patients with NYHA II (n = 118). Non-significant trend toward fewer heart failure deaths due to any cause and marginally significant reduction in first hospital admission for worsening heart failure or heart failure death. [118] No information on CHF No difference in CHF hospitalisation. Excluded cholesterol levels inversely correlate with mortality in CHF patients, (also in the aforementioned studies in patients not using statins [33]) the possibility remains that statin therapy in these patients is simply a marker of higher pre-statin cholesterol levels (often unavailable in study databases), predicting lower baseline risk. Second, some of these CHF studies were conducted at a time when beta-blockers and spironolactone were not generally used in severe heart failure. Third, most of the patients receiving statin treatment at discharge were on statin treatment before inclusion in the study, further complicating this analysis. Finally, although statin therapy seems to reduce new onset heart failure, it could be related to effects on reduction of recurrent myocardial infarction and subsequent CHF, rather than development of CHF without recurrent infarctions. In conclusion, the effect of statin treatment in established CHF has not been definitely addressed by these studies. 4.3. Prospective clinical studies There are limited data on the effects of statins in established CHF. One of the most noteworthy studies has been performed in idiopathic dilated cardiomyopathy. Fiftyone patients were randomly assigned to simvastatin (up to 10 mg/day) or placebo [64]. Using M-mode echocardiograpy with 2D monitoring before and after 14 weeks of treatment, Downloaded from by guest on February 6, 2015 LIPS, 2002 [9] PROSPER, 2002 [10,128] ALLHAT-LLT, 2002 [12] ASCOT-LLA, 2003 [13] ALERT, 2003 [14] Subgroup and secondary analysis 450 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 mortality or cardiovascular hospitalisations. These two studies are complementary in their inclusion of CHF patients and will provide a more definite answer to the question of whether or not we should start statin treatment in patients with established CHF. 5. Conclusion Despite the widespread clinical use of statins for hypercholesterolaemia and prevention of CAD, data are lacking on the effects of statins on clinical outcome in CHF. Theoretical considerations and animal experimental data indicate both beneficial and harmful effects of statins in CHF. In contrast, the currently available small-scale studies and post-hoc analyses suggest a neutral or beneficial effect of statins, but no harmful effects. Currently, two large placebo controlled trials are evaluating the efficacy of statin treatment in CHF [125,126]. Until the results are presented, we are practicing non-evidence based medicine when prescribing statins to CHF patients. Currently, we do prescribe statins to CHF patients of non-ischemic etiology when cholesterol levels need to be treated according to the guidelines (based on non-CHF populations). In CHF patients with coronary heart disease, most physicians also feel more comfortable prescribing statins than withholding them. If statins prove to reduce mortality and morbidity in patients with CHF, future research should be aimed at elucidating the precise mechanism. This is of particular importance since, in CHF, statins cholesterol lowering efficacy might be of secondary importance [127]. Acknowledgements P.v.d.H. is supported by Zon-MW 920-03-236 of The Netherlands Organization for Health Research and Development. D.J. van Veldhuisen is an Established Investigator of the Netherlands Heart Foundation (grant D97-017). We like to thank Maren White for her comments on a previous version of the manuscript. References [1] Effects of pravastatin in patients with serum total cholesterol levels from 5.2 to 7.8 mmol/liter (200 to 300 mg/dl) plus two additional atherosclerotic risk factors. The Pravastatin Multinational Study Group for Cardiac Risk Patients. Am J Cardiol 1993;72:1031–7. [2] Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383–9. [3] Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, Macfarlane PW, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med 1995;333:1301–8. [4] Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med 1996;335:1001–9. [5] Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, et al. Primary prevention of acute coronary events with lovastatin in Downloaded from by guest on February 6, 2015 Node et al. demonstrated improved functional capacity in patients who received simvastatin compared to placebo. In the statin group, 39.1% of patients had an improved functional class and 4.3% deteriorated. In contrast, in the placebo group, 16% of patients improved and 12% deteriorated (P < 0.01 between the groups). The functional improvement was associated with improved left ventricular ejection fraction in the simvastatin group (from 34% to 41%, P < 0.05), but not in the placebo group. Furthermore, plasma concentrations of TNF-a, IL-6 and BNP were significantly lower in simvastatin treated patients. Another prospective, double blind study randomised non-ischemic dilated cardiomyopathy patients to cerivastatin 0.4 mg versus placebo [121]. Quality of life and exercise capacity significantly increased in the statin group, but not in the placebo group. In addition, there was a trend towards increased left ventricular ejection fraction and improved endothelial function. A small study involving few CHF patients demonstrated improvement of reactive hyperaemia, associated with decreased plasma concentrations of components of the thrombosis– fibrinolysis system and inflammation [122,123]. The recently published Treating to New Targets (TNT) study involving 10,001 CAD patients investigated the efficacy of 80 mg versus 10 mg atorvastatin. The TNT study excluded patients with a LVEF < 30%. However, a prespecified secondary outcome of the TNT trials was the incidence of hospitalisation with a primary diagnosis of CHF. A total of 164 (3.3%) of the patients on atorvastatin 10 mg vs. 122 (2.4%) of the patients on atorvastatin 80 mg were hospitalized with a primary diagnosis of CHF; representing a 26% decreased hospitalization rate for congestive heart failure in the high dose statin group (HR 0.74 [0.59–0.94]; P = 0.01) [124]. Thus, in patients with CAD, the TNT trial suggests that the incidence of new onset CHF can be reduced with statin therapy. Despite a considerable amount of circumstantial evidence, so far no large randomised controlled clinical trails have been published on the effects of statins in CHF patients. However, two large clinical trials are currently ongoing [125,126]. The Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA) will enroll about 4950 patients with chronic symptomatic systolic CHF with ischemic etiology [125]. CORONA is an endpoint-driven trial that is expected to last 52 months. The primary outcome is the composite endpoint of cardiovascular death or non-fatal myocardial infarction or non-fatal stroke (time to first event). The GISSI heart failure trial will enrol approximately 7000 patients to be randomised to n-3 polyunsaturated fatty acids or matching placebo and where there is no clear indication for cholesterol-lowering therapy patients will be further randomized to receive rosuvastatin or matching placebo [126]. In contrast to the CORONA trial, the GISSI heart failure trial will enroll patients with both ischemic and non-ischemic heart failure. The GISSI heart failure trial is also event driven and has two co-primary endpoints, namely all-cause mortality and the combined endpoint of all-cause P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 [6] [7] [8] [9] [10] [11] [13] [14] [15] [16] [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] [41] [42] [43] [44] [45] and Death from Coronary Heart Disease in Older Persons. Ann Intern Med 1997;126:753–60. Schatz IJ, Masaki K, Yano K, Chen R, Rodriguez BL, Curb JD. Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: a cohort study. Lancet 2001;358:351–5. Kannel WB. Epidemiology of heart failure. Am Heart J 1991; 121:951–7. Hoffman RM. Modifiable risk factors for incident heart failure in the coronary artery surgery study. Arch Intern Med 1994;154:417–23. Wilhelmsen L. Heart failure in the general population of men— morbidity, risk factors and prognosis. J Intern Med 2001;249:253–61. Coughlin SS. Predictors of mortality from idiopathic dilated cardiomyopathy in 356,222 men screened for the Multiple Risk Factor Intervention Trial. Am J Epidemiol 1994;139:166–72. Kronmal RA. Total serum cholesterol levels and mortality risk as a function of age. A report based on the Framingham data. Arch Intern Med 1993;153:1065–73. Cowie MR. The epidemiology of heart failure. Eur Heart J 1997; 18:208–25. Vredevoe DL, Woo MA, Doering LV, Brecht ML, Hamilton MA, Fonarow GC. Skin test anergy in advanced heart failure secondary to either ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol 1998;82:323–8. Horwich TB, Hamilton MA, Maclellan WR, Fonarow GC. Low serum total cholesterol is associated with marked increase in mortality in advanced heart failure. J Card Fail 2002;8:216–24. Mozaffarian D, Nye R, Levy WC. Statin therapy is associated with lower mortality among patients with severe heart failure. Am J Cardiol 2004;93:1124–9. Rauchhaus M, Koloczek V, Volk H, Kemp M, Niebauer J, Francis DP, et al. Inflammatory cytokines and the possible immunological role for lipoproteins in chronic heart failure. Int J Cardiol 2000; 76:125–33. Rauchhaus M, Clark AL, Doehner W, Davos C, Bolger A, Sharma R, et al. The relationship between cholesterol and survival in patients with chronic heart failure. J Am Coll Cardiol 2003;42:1933–40. Richartz BM, Radovancevic B, Frazier OH, Vaughn WK, Taegtmeyer H. Low serum cholesterol levels predict high perioperative mortality in patients supported by a left-ventricular assist system. Cardiology 1998;89:184–8. Rosolova H, Cech J, Simon J, Spinar J, Jandova R, Widimsky sen J, et al. Short to long term mortality of patients hospitalised with heart failure in the Czech Republic\a report from the EuroHeart Failure Survey. Eur J Heart Fail 2005;7:780–3. Kalantar-Zadeh K, Block G, Horwich T, Fonarow GC. Reverse epidemiology of conventional cardiovascular risk factors in patients with chronic heart failure. J Am Coll Cardiol 2004;43:1439–44. Riley M. Resting energy expenditure in chronic cardiac failure. Clin Sci (Lond) 1991;80:633–9. Anker SD, Chua TP, Ponikowski P, Harrington D, Swan JW, Kox WJ, et al. Hormonal Changes and Catabolic/Anabolic Imbalance in Chronic Heart Failure and Their Importance for Cardiac Cachexia. Circulation 1997;96:526–34. Rauchhaus M, Coats AJS, Anker SD. The endotoxin–lipoprotein hypothesis. Lancet 2000;356:930–3. Niebauer J, Volk HD, Kemp M, Dominguez M, Schumann RR, Rauchhaus M, et al. Endotoxin and immune activation in chronic heart failure: a prospective cohort study. Lancet 1999;353:1838–42. Netea MG, Demacker PNM, Kullberg BJ, Boerman OC, Verschueren I, Stalenhoef AFH, et al. Low-density lipoprotein receptor-deficient mice are protected against lethal endotoxemia and severe gramnegative infections. J Clin Invest 1996;97:1366–72. Rundek T, Naini A, Sacco R, Coates K, DiMauro S. Atorvastatin decreases the coenzyme Q10 level in the blood of patients at risk for cardiovascular disease and stroke. Arch Neurol 2004;61:889–92. Watts GF. Plasma coenzyme Q (ubiquinone) concentrations in patients treated with simvastatin. J Clin Pathol 1993;46:1055–7. Downloaded from by guest on February 6, 2015 [12] men and women with average cholesterol levels: results of AFCAPS/ TexCAPS. JAMA 1998;279:1615–22. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339:1349–57. Schwartz GG, Olsson AG, Ezekowitz MD, Ganz P, Oliver MF, Waters D, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL Study: a randomized controlled trial. JAMA 2001;285:1711–8. MRC/BHF heart protection study of cholesterol lowering with simvastatin in 20536 high-risk individuals: a randomised placebocontrolled trial. Lancet 2002;360:7–22. Serruys PW, de Feyter P, Macaya C, Kokott N, Puel J, Vrolix M, et al. Fluvastatin for prevention of cardiac events following successful first percutaneous coronary intervention: a randomized controlled trial. JAMA 2002;287:3215–22. Shepherd J, Blauw GJ, Murphy MB, Bollen ELEM, Buckley BM, Cobbe SM, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 2002; 360:1623–30. Athyros VG. V. Treatment with atorvastatin to the National Cholesterol Educational Program goal versus ‘usual’ care in secondary coronary heart disease prevention. The GREek Atorvastatin and Coronary-heart-disease Evaluation (GREACE) study. Curr Med Res Opin 2002;18:220–8. The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs. Usual care: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA 2002; 288:2998–3007. Sever PS, Dahlof B, Poulter NR, Wedel H, Beevers G, Caulfield M, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003;361:1149–58. Holdaas H, Fellstrom B, Jardine AG, Holme I, Nyberg G, Fauchald P, et al. Effect of fluvastatin on cardiac outcomes in renal transplant recipients: a multicentre, randomised, placebo-controlled trial. Lancet 2003;361:2024–31. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685–96. Krum H, McMurray JJ. Statins and chronic heart failure: do we need a large-scale outcome trial? J Am Coll Cardiol 2002;39:1567–73. Bohm M, Hjalmarson A, Kjekshus J, Laufs U, McMurray J, Van Veldhuisen DJ. Heart failure and statins—Why do we need a clinical trial? Z Kardiol 2005;94:223–30. Iribarren C. Cohort study of serum total cholesterol and in-hospital incidence of infectious diseases. Epidemiol Infect 1998;121:335–47. Pacelli F. Prognosis in intra-abdominal infections. Multivariate analysis on 604 patients. Arch Surg 1996;131:641–5. Onder G, Landi F, Volpato S, Fellin R, Carbonin P, Gambassi G, et al. Serum cholesterol levels and in-hospital mortality in the elderly. Am J Med 2003;115:265–71. Forette B. Cholesterol as risk factor for mortality in elderly women. Lancet 1989;1:868–70. Weverling-Rijnsburger AWE, Blauw GJ, Lagaay AM, Knook DL, Meinders AE, Westendorp RGJ. Total cholesterol and risk of mortality in the oldest old. Lancet 1997;350:1119–23. Corti MC, Guralnik JM, Salive ME, Harris T, Ferrucci L, Glynn RJ, et al. Clarifying the Direct Relation between Total Cholesterol Levels 451 452 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 [67] Chong AY, Blann AD, Patel J, Freestone B, Hughes E, Lip GY. Endothelial dysfunction and damage in congestive heart failure: relation of flow-mediated dilation to circulating endothelial cells, plasma indexes of endothelial damage, and brain natriuretic peptide. Circulation 2004;110:1794–8. [68] Katz SD, Hryniewicz K, Hriljac I, Balidemaj K, Dimayuga C, Hudaihed A, et al. Vascular endothelial dysfunction and mortality risk in patients with chronic heart failure. Circulation 2005;01. [69] Hornig B, Maier V, Drexler H. Physical training improves endothelial function in patients with chronic heart failure. Circulation 1996;93: 210–4. [70] Rikitake Y, Liao JK. Rho GTPases, statins, and nitric oxide. Circ Res 2005;97:1232–5. [71] Anderson TJ, Meredith IT, Yeung AC, Frei B, Selwyn AP, Ganz P. The effect of cholesterol-lowering and antioxidant therapy on endothelium-dependent coronary vasomotion. N Engl J Med 1995;332:488–93. [72] Treasure CB, Klein JL, Weintraub WS, Talley JD, Stillabower ME, Kosinski AS, et al. Beneficial effects of cholesterol-lowering therapy on the coronary endothelium in patients with coronary artery disease. N Engl J Med 1995;332:481–7. [73] Asselbergs FW, van der Harst P, Jessurun GAJ, Tio RA, van Gilst WH. Clinical impact of vasomotor function assessment and the role of ACE-inhibitors and statins. Vascul Pharmacol 2005;42:125–40. [74] van Boven AJ, Jukema JW, Zwinderman AH, Crijns HJGM, Lie KI, Bruschke AVG. Reduction of transient myocardial ischemia with pravastatin in addition to the conventional treatment in patients with angina pectoris. Circulation 1996;94:1503–5. [75] Kureishi Y, Luo Z, Shiojima I, Bialik A, Fulton D, Lefer DJ, et al. The HMG-CoA reductase inhibitor simvastatin activates the protein kinase Akt and promotes angiogenesis in normocholesterolemic animals. Nat Med 2000;6:1004–10. [76] Landmesser U, Engberding N, Bahlmann FH, Schaefer A, Wiencke A, Heineke A, et al. Statin-induced improvement of endothelial progenitor cell mobilization, myocardial neovascularization, left ventricular function, and survival after experimental myocardial infarction requires endothelial nitric oxide synthase. Circulation 2004;110:1933–9. [77] Llevadot J, Murasawa S, Kureishi Y, Uchida S, Masuda H, Kawamoto A, et al. HMG-CoA reductase inhibitor mobilizes bone marrow-derived endothelial progenitor cells. J Clin Invest 2001; 108:399–405. [78] Vasa M, Fichtlscherer S, Adler K, Aicher A, Martin H, Zeiher AM, et al. Increase in circulating endothelial progenitor cells by statin therapy in patients with stable coronary artery disease. Circulation 2001;103:2885–90. [79] Nickenig G, Baumer AT, Temur Y, Kebben D, Jockenhovel F, Bohm M. Statin-sensitive dysregulated AT1 receptor function and density in hypercholesterolemic men. Circulation 1999;100:2131–4. [80] De Boer RA, Pinto YM, Suurmeijer AJ, Pokharel S, Scholtens E, Humler M, et al. Increased expression of cardiac angiotensin II type 1 (AT(1)) receptors decreases myocardial microvessel density after experimental myocardial infarction. Cardiovasc Res 2003; 57: 434–42. [81] van der Harst P, Wagenaar LJ, Buikema H, Voors AA, Plokker HW, Morshuis WJ, et al. Effect of intensive versus moderate lipid lowering on endothelial function and vascular responsiveness to angiotensin ii in stable coronary artery disease. Am J Cardiol 2005; 96:1361–4. [82] Maack C, Kartes T, Kilter H, Schafers HJ, Nickenig G, Bohm M, et al. Oxygen free radical release in human failing myocardium is associated with increased activity of Rac1-GTPase and represents a target for statin treatment. Circulation 2003;108:1567–74. [83] Saijonmaa O, Nyman T, Stewen P, Fyhrquist F. Atorvastatin completely inhibits VEGF-induced ACE upregulation in human endothelial cells. Am J Physiol Heart Circ Physiol 2004;286: H2096–102. Downloaded from by guest on February 6, 2015 [46] Mortensen SA, Leth A, Agner E, Rohde M. Dose-related decrease of serum coenzyme Q10 during treatment with HMG-CoA reductase inhibitors. Mol Aspects Med 1997;18 Suppl:S137–44. [47] De Pinieux G. Lipid-lowering drugs and mitochondrial function: effects of HMG-CoA reductase inhibitors on serum ubiquinone and blood lactate/pyruvate ratio. Br J Clin Pharmacol 1996; 42:333–7. [48] Marz W, Siekmeier R, Muller HM, Wieland H, Gross W, Olbrich HG. Effects of lovastatin and pravastatin on the survival of hamsters with inherited cardiomyopathy. J Cardiovasc Pharmacol Ther 2000; 5:275–9. [49] de Lorgeril M. Effects of lipid-lowering drugs on left ventricular function and exercise tolerance in dyslipidemic coronary patients. J Cardiovasc Pharmacol 1999;33:473–8. [50] Permanetter B. Ubiquinone (coenzyme Q10) in the long-term treatment of idiopathic dilated cardiomyopathy. Eur Heart J 1992; 13:1528–33. [51] Folkers K. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc Natl Acad Sci U S A 1985;82:901–4. [52] Mortensen SA. Overview on coenzyme Q10 as adjunctive therapy in chronic heart failure. Rationale, design and end-points of “Qsymbio”—a multinational trial. Biofactors 2003;18:79–89. [53] Hatfield DL, Gladyshev VN. How selenium has altered our understanding of the genetic code. Mol Cell Biol 2002;22:3565–76. [54] Dihanich ME, Najarian D, Clark R, Gillman EC, Martin NC, Hopper AK. Isolation and characterization of MOD5, a gene required for isopentenylation of cytoplasmic and mitochondrial tRNAs of Saccharomyces cerevisiae. Mol Cell Biol 1987;7:177–84. [55] Moosmann B, Behl C. Selenoprotein synthesis and side-effects of statins. Lancet 2004;363:892–4. [56] Warner GJ, Berry MJ, Moustafa ME, Carlson BA, Hatfield DL, Faust JR. Inhibition of selenoprotein synthesis by selenocysteine tRNA [Ser]Sec lacking isopentenyladenosine. J Biol Chem 2000; 275:28110–9. [57] Yokoyama I, Ohtake T, Momomura S, Nishikawa J, Sasaki Y, Omata M. Reduced coronary flow reserve in hypercholesterolemic patients without overt coronary stenosis. Circulation 1996;94:3232–8. [58] Kaufmann PA, Gnecchi-Ruscone T, Schafers KP, Luscher TF, Camici PG. Low density lipoprotein cholesterol and coronary microvascular dysfunction in hypercholesterolemia. J Am Coll Cardiol 2000;36: 103–9. [59] Baller D, Notohamiprodjo G, Gleichmann U, Holzinger J, Weise R, Lehmann J. Improvement in coronary flow reserve determined by positron emission tomography after 6 months of cholesterol-lowering therapy in patients with early stages of coronary atherosclerosis. Circulation 1999;99:2871–5. [60] Guethlin M, Kasel AM, Coppenrath K, Ziegler S, Delius W, Schwaiger M. Delayed response of myocardial flow reserve to lipid-lowering therapy with fluvastatin. Circulation 1999;99:475–81. [61] Mellwig KP, Baller D, Gleichmann U, Moll D, Betker S, Weise R, et al. Improvement of coronary vasodilatation capacity through single LDL apheresis. Atherosclerosis 1998;139:173–8. [62] Anversa P, Beghi C, Kikkawa Y, Olivetti G. Myocardial infarction in rats. Infarct size, myocyte hypertrophy, and capillary growth. Circ Res 1986;58:26–37. [63] Anversa P, Ricci R, Olivetti G. Effects of exercise on the capillary vasculature of the rat heart. Circulation 1987;75:I12–8. [64] Node K, Fujita M, Kitakaze M, Hori M, Liao JK. Short-term statin therapy improves cardiac function and symptoms in patients with idiopathic dilated cardiomyopathy. Circulation 2003;108:839–43. [65] van der Harst P, Voors AA, Van Veldhuisen DJ. Short-term statin therapy and cardiac function and symptoms in patients with idiopathic dilated cardiomyopathy. Circulation 2004;109:e34. [66] Treasure CB, Vita JA, Cox DA, Fish RD, Gordon JB, Mudge GH, et al. Endothelium-dependent dilation of the coronary microvasculature is impaired in dilated cardiomyopathy. Circulation 1990;81:772–9. P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 [103] Levine B. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N Engl J Med 1990;323:236–41. [104] Kapadia S. The role of cytokines in the failing human heart. Cardiol Clin 1998;16:645. [105] Blum A, Miller H. Pathophysiological role of cytokines in congestive heart failure. Annu Rev Med 2001;52:15–27. [106] Feldman AM, Combes A, Wagner D, Kadakomi T, Kubota T, You Li Y, et al. The role of tumor necrosis factor in the pathophysiology of heart failure. J Am Coll Cardiol 2000;35:537–44. [107] Ridker PM, Rifai N, Lowenthal SP. Rapid reduction in c-reactive protein with cerivastatin among 785 patients with primary hypercholesterolemia. Circulation 2001;103:1191–3. [108] Ridker PM, Cannon CP, Morrow D, Rifai N, Rose LM, McCabe CH, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005;352:20–8. [109] Holm T, Andreassen AK, Ueland T, Kjekshus J, Froland SS, Kjekshus E, et al., Effect of pravastatin on plasma markers of inflammation and peripheral endothelial function in male heart transplant recipients. Am J Cardiol 2001;87:815–8 [A9]. [110] Spinale FG, Coker ML, Bond BR, Zellner JL. Myocardial matrix degradation and metalloproteinase activation in the failing heart: a potential therapeutic target. Cardiovasc Res 2000;46: 225–38. [111] Bellosta S, Via D, Canavesi M, Pfister P, Fumagalli R, Paoletti R, et al. HMG-CoA reductase inhibitors reduce MMP-9 secretion by macrophages. Arterioscler Thromb Vasc Biol 1998;18:1671–8. [112] Furman C, Copin C, Kandoussi M, Davidson R, Moreau M, McTaggiart F, et al. Rosuvastatin reduces MMP-7 secretion by human monocyte-derived macrophages: potential relevance to atherosclerotic plaque stability. Atherosclerosis 2004;174:93–8. [113] Li YY, Feng YQ, Kadokami T, McTiernan CF, Draviam R, Watkins SC, et al. Myocardial extracellular matrix remodeling in transgenic mice overexpressing tumor necrosis factor alpha can be modulated by anti-tumor necrosis factor alpha therapy. Proc Natl Acad Sci U S A 2000;97:12746–51. [114] Bauersachs J, Galuppo P, Fraccarollo D, Christ M, Ertl G. Improvement of left ventricular remodeling and function by hydroxymethylglutaryl coenzyme a reductase inhibition with cerivastatin in rats with heart failure after myocardial infarction. Circulation 2001;104:982–5. [115] Hayashidani S, Tsutsui H, Shiomi T, Suematsu N, Kinugawa S, Ide T, et al. Fluvastatin, a 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor, attenuates left ventricular remodeling and failure after experimental myocardial infarction. Circulation 2002;105: 868–73. [116] Segal R, Pitt B, Poole-Wilson P, Sharma D, Bradstreet DC, Ikeda LS. Effects of HMG-CoA reductase inhibitors (statins) in patients with heart failure. Eur J Heart Fail 2000;2(Suppl 2):96. [117] Kjekshus J, Pedersen TR, Olsson AG, Faergeman O, Pyorala K. The effects of simvastatin on the incidence of heart failure in patients with coronary heart disease. J Card Fail 1997;3:249–54. [118] The effects of cholesterol lowering with simvastatin on cause-specific mortality and on cancer incidence in 20,536 high-risk people: a randomised placebo-controlled trial [ISRCTN48489393]. BMC Med 2005;3:6. [119] Dickstein K, Kjekshus J. Effects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal trial in myocardial infarction with angiotensin II antagonist losartan. Lancet 2002;360: 752–60. [120] Hognestad A, Dickstein K, Myhre E, Snapinn S, Kjekshus J. Effect of combined statin and beta-blocker treatment on one-year morbidity and mortality after acute myocardial infarction associated with heart failure. Am J Cardiol 2004;93:603–6. [121] Laufs U, Wassmann S, Schackmann S, Heeschen C, Bohm M, Nickenig G. Beneficial effects of statins in patients with non-ischemic heart failure. Z Kardiol 2004;93:103–8. Downloaded from by guest on February 6, 2015 [84] Chen J. Inhibitory effect of candesartan and rosuvastatin on CD40 and MMPs expression in apo-E knockout mice: novel insights into the role of RAS and dyslipidemia in atherogenesis. J Cardiovasc Pharmacol 2004;44:446–52. [85] Horiuchi M, Cui TX, Li Z, Li JM, Nakagami H, Iwai M. Fluvastatin enhances the inhibitory effects of a selective angiotensin II Type 1 receptor blocker, valsartan, on vascular neointimal formation. Circulation 2003;107:106–12. [86] Li Z, Iwai M, Wu L, Liu HW, Chen R, Jinno T, et al. Fluvastatin enhances the inhibitory effects of a selective AT1 receptor blocker, valsartan, on atherosclerosis. Hypertension 2004;44: 758–63. [87] Koh KK, Quon MJ, Han SH, Chung WJ, Ahn JY, Seo YH, et al. Additive beneficial effects of losartan combined with simvastatin in the treatment of hypercholesterolemic, hypertensive patients. Circulation 2004;110:3687–92. [88] Ito M, Adachi T, Pimentel DR, Ido Y, Colucci WS. Statins inhibit {beta}-adrenergic receptor-stimulated apoptosis in adult rat ventricular myocytes via a Rac1-dependent mechanism. Circulation 2004;110:412–8. [89] Sugden PH. Ras, Akt, and mechanotransduction in the cardiac myocyte. Circ Res 2003;93:1179–92. [90] Proud CG. Ras, PI3-kinase and mTOR signaling in cardiac hypertrophy. Cardiovasc Res 2004;63:403–13. [91] Liao JK. Statin therapy for cardiac hypertrophy and heart failure. J Investig Med 2004;52:248–53. [92] Dechend R. Amelioration of angiotensin II-induced cardiac injury by a 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitor. Circulation 2001;104:576–81. [93] Takemoto M, Node K, Nakagami H, Liao Y, Grimm M, Takemoto Y, et al. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest 2001;108:1429–37. [94] Oi S. Lovastatin prevents angiotensin II-induced cardiac hypertrophy in cultured neonatal rat heart cells. Eur J Pharmacol 1999; 376:139–48. [95] Delbosc S, Cristol JP, Descomps B, Mimran A, Jover B. Simvastatin prevents angiotensin II-induced cardiac alteration and oxidative stress. Hypertension 2002;40:142–7. [96] Luo JD, Xie F, Zhang WW, Ma XD, Guan JX, Chen X. Simvastatin inhibits noradrenaline-induced hypertrophy of cultured neonatal rat cardiomyocytes. Br J Pharmacol 2001;132:159–64. [97] Indolfi C, Di Lorenzo E, Perrino C, Stingone AM, Curcio A, Torella D, et al. Hydroxymethylglutaryl coenzyme A reductase inhibitor simvastatin prevents cardiac hypertrophy induced by pressure overload and inhibits p21ras activation. Circulation 2002; 106: 2118–24. [98] Luo JD, Zhang WW, Zhang GP, Guan JX, Chen X. Simvastatin inhibits cardiac hypertrophy and angiotensin-converting enzyme activity in rats with aortic stenosis. Clin Exp Pharmacol Physiol 1999;26:903–8. [99] Su SF, Hsiao CL, Chu CW, Lee BC, Lee TM. Effects of pravastatin on left ventricular mass in patients with hyperlipidemia and essential hypertension. Am J Cardiol 2000;86:514–8. [100] Jukema JW, Bruschke AVG, van Boven AJ, Reiber JHC, Bal ET, Zwinderman AH, et al. Effects of lipid lowering by pravastatin on progression and regression of coronary artery disease in symptomatic men with normal to moderately elevated serum cholesterol levels: the Regression Growth Evaluation Statin Study (REGRESS). Circulation 1995;91:2528–40. [101] Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004;291:1071–80. [102] Lima JA, Desai MY, Steen H, Warren WP, Gautam S, Lai S. Statininduced cholesterol lowering and plaque regression after 6 months of magnetic resonance imaging-monitored therapy. Circulation 2004; 110:2336–41. 453 454 P. van der Harst et al. / Cardiovascular Research 71 (2006) 443–454 [122] Tousoulis D, Antoniades C, Bosinakou E, Kotsopoulou M, Tsioufis C, Tentolouris C, et al. Effects of atorvastatin on reactive hyperaemia and the thrombosis–fibrinolysis system in patients with heart failure. Heart 2005;91:27–31. [123] Tousoulis D, Antoniades C, Bosinakou E, Kotsopoulou M, Pitsavos C, Vlachopoulos C, et al. Effects of atorvastatin on reactive hyperemia and inflammatory process in patients with congestive heart failure. Atherosclerosis 2005;178:359–63. [124] LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425–35. [125] Kjekshus J, Dunselman P, Blideskog M, Eskilson C, Hjalmarson A, McMurray JV, et al. A statin in the treatment of heart failure? Controlled rosuvastatin multinational study in heart failure (CORO- NA): study design and baseline characteristics. Eur J Heart Fail 2005;7:1059–69. [126] Tavazzi L, Tognoni G, Franzosi MG, Latini R, Maggioni AP, Marchioli R, et al. Rationale and design of the GISSI heart failure trial: a large trial to assess the effects of n-3 polyunsaturated fatty acids and rosuvastatin in symptomatic congestive heart failure. Eur J Heart Fail 2004;6:635–41. [127] Landmesser U, Bahlmann F, Mueller M, Spiekermann S, Kirchhoff N, Schulz S, et al. Simvastatin versus ezetimibe: pleiotropic and lipidlowering effects on endothelial function in humans. Circulation 2005;111:2356–63. [128] Shepherd J, Blauw GJ, Murphy MB, Cobbe SM, Bollen ELEM, Buckley BM, et al. The design of a prospective study of pravastatin in the elderly at risk (PROSPER). Am J Cardiol 1999;84:1192–7. Downloaded from by guest on February 6, 2015





© Copyright 2026