
lam5m111 louisiana medicaid management information system
LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 1 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------001 002 003 004 005 006 007 008 009 010 011 012 013 014 015 016 017 018 019 020 021 022 023 024 025 026 027 028 029 030 031 032 033 034 035 036 037 038 039 040 041 042 043 044 045 046 047 19:11:13 INVALID CLM TYP MOD INVALID PROVIDER NO RECIPIENT # INVALID INVALID OPERATOR CDE INVAL SERV FROM DATE INVAL SERV THRU DATE SERV THRU LT SERV FM SERV FRM GT ENTR DTE SERV THR GT ENTR DTE INV PRIOR AUTH DATE INVALID TPL INDICATR ORG CLM W/ADJ/VD CDE ORG CLM W ADJ/VD ICN IMM COMPL MISS/INVLD INVALID ACCIDENT IND INVALID ACCID IND INVALID EPSDT IND INVALID PRIM DIAGNOS INVALID SECOND DIAG INVAL/MISS DIAG CODE INVALID FORMER REFNO INVALID BILLED CHRGS INV PARTIAL RECIP INV BILLING PROV NO IMM NOT COMP RSN MIS INVALID TOT DOC CHG PROC NEEDS DOCUMENT. INVAL/MISS PROC CODE SERV MORE THAN 12 MO SERV THRU DT TOO OLD NOT EMC ELIGIBLE EOB/CARR.CD MISMATCH NEED EOB-CARR/RECIP. 22 MOD.NOT JUSTIFIED REBILL CORRECT HCPC SUB VOID,REBILL ANES MEDICARE ADJUSTMENT 99297-52 NICU REDUCE MOD.NOT USED FOR CLM INV ADMISSION DATE ADMIT DTE GT SERV FM INVALID UB92 BILL CD INV ATTENDING PHYS INV NATURE OF ADMIT INV PATIENT STATUS INV PATIENT STAT DTE PAT STAT DTE GT THRU INVALID CLAIM TYPE MODIFIER PROVIDER NUMBER MISSING OR NOT NUMERIC RECIPIENT NUMBER INVALID OR LESS THAN 13 DIGITS OPERATOR CODE MISSING SERVICE FROM DATE MISSING/INVALID INVALID OR MISSING THRU DATE SERVICE THRU DATE LESS THAN SERVICE FROM DATE SERVICE FROM DATE LATER THAN DATE PROCESSED SERVICE THRU DATE GREATER THAN DATE OF ENTRY PRIOR AUTHORIZATION DATE NOT NUMERIC TPL INDICATOR NOT Y, N, OR SPACE ORIGINAL CLAIM WITH AN ADJUSTMENT OR VOID REASON CODE ORIGINAL CLAIM WITH AN ADJUSTMENT OR VOID ICN IMMUN COMPLETE AND CURRENT FOR THIS AGE PATIENT MISSING ACCIDENT INDICATOR MUST BE Y,N,SPACE ACCIDENT INDICATOR NOT Y, N OR SPACE EPSDT INDICATOR NOT Y, N, OR SPACE PRIMARY DIAGNOSIS AS CODED NOT ON FILE SECONDARY DIAGNOSIS INVALID INVALID OR MISSING DIAGNOSIS CODE FORMER REFERENCE NUMBER MISSING OR INVALID BILLED CHARGES MISSING OR NOT NUMERIC RECIPIENT NAME IS MISSING BILLING PROVIDER NUMBER NOT NUMERIC IMMUN NOT COMPLETE AND CURRENT REASON CODE MISSING TOTAL DOCUMENT CHARGE MISSING OR NOT NUMERIC PROCEDURE CODE NOT SUBSTANTIATED BY DOCUMENT INVALID OR MISSING PROCEDURE CODE SERVICE MORE THAN 12 MONTHS OLD SERV THRU DATE MORE THAN TWO YEARS OLD PROVIDER NOT APPROVED FOR EMC BY STATE OFS EOB(S) ATTACHED/CARRIER CODE DOES NOT MATCH NEED EOB FOR EACH CARRIER INDICATED ON RESOURCE FILE 22 MOD.SERVICES NOT JUSTIFIED/PAID AT UNMODIFIED RATE ASC,OP FAC/PHYS.BILLED DIFF CODE;REBILL CORRECT HCPC SUBMIT VOID THEN REBILL ANESTHESIA MEDICARE ADJUSTMENT/VOID,ADJUST OR ADJUST MEDICARE CLAI 99297-52 NICU PAID AT REDUCED RATE MODIFIER NOT USED TO PROCESS CLAIM ADMISSION DATE MISSING OR INVALID ADMISSION DATE GREATER THAN SERVICE FROM DATE INVALID UB92 TYPE BILL CODE ATTENDING PHYSICIAN NUMBER NOT NUMERIC NATURE OF ADMISSION MISSING OR INVALID PATIENT STATUS CODE INVALID OR MISSING PATIENT STATUS DATE MISSING OR INVALID PATIENT STATUS DATE GREATER THAN THRU DATE CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 3 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 3 2 3 3 3 1 1 3 2 3 1 3 2 2 2 2 2 2 2 2 2 16 16 31 133 16 16 16 110 16 133 16 16 16 133 16 16 133 16 16 16 16 16 16 16 133 16 150 16 29 29 95 251 251 150 16 59 252 150 4 16 16 16 16 16 16 16 16 N34 N77 M52 M59 MA31 MA31 MA92 MA30 MA30 N305 N305 MA63 M64 MA63 M47 M79 MA36 N257 M54 M51 N4 N4 M20 N4 N519 MA40 MA40 MA30 N290 MA41 MA43 M59 M59 021 021 021 021 021 021 021 021 021 252 021 021 021 021 365 365 021 254 021 255 464 178 021 021 021 178 294 454 263 187 496 286 286 047 454 001 101 628 453 189 187 228 132 231 021 021 021 NCCI = CODE USED FOR NCCI ONLY. 153 153 055 188 188 188 188 188 361 521 584 331 564 564 488 504 153 331 564 287 431 387 387 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 2 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------048 049 050 051 052 053 054 055 056 057 058 059 060 061 062 063 064 065 066 067 068 069 070 071 072 073 074 075 076 077 078 079 080 081 082 083 084 085 086 087 088 089 090 091 092 093 094 19:11:13 INVALID/MISS PROC INV/CONFLIC SURG DTE INV BLOOD NOT REPL INV BLOOD/PINT CHG >12 MONTH QTY LIMIT INV ACCOMODATION DAY CONDITION NOT PAYABL INV ACCOM/ANCILL CHG INV ANCILLARY CHARGE WERE SUSP COND -MISS SUSP COND DISCRPANCY SUSP COND MISSNG/REQ INVALID COVERED DAYS INVALID PSRO DATE INVALID APPROVED DYS INVALID TOTAL CHARGE INVALID NET AMOUNT INVLD SIGNATURE IND CLIN PRE-AUTH REQ'D INVALID NON-COVERED INV POINT ORIGIN INV OCCUR DATE PSRO/UR CLAIM DENIED INV STMT COVERS FROM INV STMT COVER THRU STMT FRM LT SERV FRM STMT THRU GT SRV THR INVALID TYPE SERVICE INV DME PA AMOUNT ATTEND MUST=BILLING RESUB W/ DOCUMENTS FOUND NO PSRO CODE INVALID LAB INDICATR INVALID STATUS DATE INVALID STATUS CODE INVALID SERVICE CODE INVALID TREAT PLACE INVALID UNITS/VISITS PEND FOR RECYCLE MISSINVAL COINS DAY INVALID ORIGIN CODE M/I INCENTIVE AMOUNT REF PROV NO. NOF PROC NOT COV BY FP INVLD/MISSNG MODIFR REVENUE CODE MISSING MISSING PINTS BLOOD INVALID OR MISSING PROCEDURE CODE INVALID/CONFLICT SURGICAL DATE BLOOD NOT REPLACED AMOUNT INVALID BLOOD CHARGE PER PINT INVALID > 12 MONTH QTY LIMIT MD FAX OVERRIDE FORM 866-797-2329 ACCOMODATION DAYS MISSING OR INVALID PROVIDER PREVENTABLE CONDITION NOT PAYABLE ACCOMODATION/ANCILLARY CHARGE MISSING OR INVALID ANCILLARY CHARGE INVALID WERE THERE SUSPECTED CONDITIONS-MISSING WERE THERE SUSPECTED CONDITIONS IS NO BUT COND EXISTS SUSPECTED CONDITIONS ARE MISSING AND REQUIRED COVERED HOSPITAL DAYS NOT NUMERIC OR MISSING A PSRO DATE IS NOT A VALID DATE THE APPROVED STAY DAYS IS NOT NUMERIC THE TOTAL HOSPITAL CHARGE IS NOT NUMERIC THE NET BILLED AMOUNT IS NOT NUMERIC THE SIGNATURE INDICATOR MUST BE Y, N, OR BLANK CLINICAL PRE-AUTH REQUIRED MD FAX FORM TO 866-797-2329 NON COVERED HOSP DAYS NOT NUMERIC OR MISSING INVALID POINT OF ORIGIN INVALID OCCURRENCE DATE PSRO/ UR CLAIM DENIED STATEMENT COVERS FROM DATE INVALID STATEMENT COVERS THRU DATE INVALID STATEMENT COVERS FROM DATE LESS THAN SERVICE FROM DATE STATEMENT COVERS THRU DATE IS GREATER THAN SERVICE THRU TYPE SERVICE FOR AMBULANCE MUST BE 3 OR 9 PRIOR AUTHORIZATION AMOUNT NOT NUMERIC ATTENDING PROV MUST EQUAL BILLING RESUB W/ DOCUMNTS CALL 800-473-2783 PSRO CODE MISSING OR INVALID LABORATORY INDICATOR MUST BE Y, N, OR BLANK INVALID OR MISSING PATIENT STATUS DATE INVALID PATIENT STATUS CODE INVALID SERVICE CODE INVALID OR MISSING PLACE OF TREATMENT INVALID OR MISSING UNITS, VISITS, AND STUDIES CLAIM PENDED FOR FUTURE RECYCLE MISSING OR INVALID COINSURANCE DAYS INVALID ORIGIN CODE MISSING/INVALID INCENTIVE AMOUNT REFERRING PROVIDER NUMBER NOT ON FILE PROCEDURE IS NOT COVERED BY THE FAMILY PLANNING PROGRAM INVALID OR MISSING MODIFIER REVENUE CODE MISSING/INVALID MISSING PINTS BLOOD CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 3 2 3 2 2 2 2 2 2 3 2 2 2 3 2 2 2 2 2 2 1 2 2 2 2 2 2 2 2 2 2 3 2 2 2 16 16 133 133 198 16 233 16 16 133 133 133 16 133 16 133 16 16 197 16 16 16 50 16 16 16 16 133 16 16 252 16 133 16 16 16 16 16 133 16 16 16 16 96 4 16 16 M51 N301 N351 M53 M79 M79 MA32 MA32 M54 MA75 MA33 MA42 M46 N10 M52 M59 M52 M59 N54 N77 N29 M44 M59 MA43 M51 M77 M53 M53 MA42 N190 N286 N30 N519 M50 M53 021 021 021 021 476 744 178 178 021 021 021 456 021 456 021 178 117 021 229 719 084 188 188 021 021 021 048 132 287 048 473 021 001 455 249 476 020 476 021 021 132 227 453 455 235 NCCI = CODE USED FOR NCCI ONLY. 454 666 236 235 431 431 431 142 178 457 188 188 250 387 021 266 402 178 626 084 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 3 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------095 096 097 098 099 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 19:11:13 FROM THRU NOT EQUAL REVENUE CHG MISSING NON-COVCHG > BILLCHG BILL-CODE-REQ-MC-CHG DME COVERAGE ONLY PROC CD MUST 5 DIGIT NDC PRICE MISSING INVALID SURFACE INV TOOTH/CAVITY CDE INDICTR/CPT CONFLICT REF MUST BE MGR BILL PRV NOT PCP PARTIAL HOSP NOT PAY PRV TYPE AGE RESTRIC NOT HCBS LOCKED IN REBILL OB/ABORT D&C CHANGING AGAIN AUTH.PORT X-RAY ONE ER CDE PER VISIT INV/MISSING HCPCS HCPC CD NOT ON FILE DEFRA REDUCTION MAX:2DAYS TRSFR MHIS HOSP LIMITED TO EMER INVEST,EXPER,OR NOT QTY INVALID/MISSING MISS OR INV PRESCRIB INVALID RX DATE RX > SERVICE DATE INVALID DAYS SUPPLY PRESCRIP NO MISSING INVALID REFILL CODE MISSING NDC INVALID MAC INDICATR PRESCRIB PROV NPI NO DENY PROV. 9999999 PRIMARY DX NOF SECONDARY DX NOF BH XOVER SENT TO SMO ENC DENIED BY PLAN PATIENT NOT COVERED NO ELIG SERVICE PAID MEDICARE REPLACEMENT REBILL W/ALL DETAILS REBILL W/APPROP CODE THERAPEUTIC DUP-MD REFILL OVR 12 MONTHS CONDITION CODE 40 FROM THRU NOT EQUAL REVENUE CHARGE MISSING OR INVALID NON-COVERED CHARGES EXCEED BILLED CHARGES BILL CLASS 2 REQUIRES MEDICARE ALLOWED AMOUNT IN LOC#54 ITEM COVERED UNDER DURABLE MED EQUIP. PROG ONLY PROCEDURE CODE MUST BE 5 NUMERIC CHARACTERS NDC PRICE MISSING, CALL MYERS&STAUFFER @ 1-800-591-1183 INVALID TOOTH SURFACE CODE INVALID TOOTH CODE/ORAL CAVITY DESIGNATOR INDICATOR 3 INVALID WITH CPT CODES-PCP REFERRAL REQ REFERRING MUST BE CASE MANAGER BILLING PROVIDER NOT PCP OR SERVICE NOT AUTHOR BY PCP PARTIAL HOSP NOT PAYABLE FOR MEDICAID ONLY PROV TYPE SERVICES NOT COVERED FOR RECIPIENT THIS AGE NOT HCBS LOCKED IN REBILL OB OR ABORTION D & C CPT CODE WITH REPORTS THIS IS A CHANGED ERROR NO DOCUMENT/EDIT OVERRIEDE PORT. X-RAY ONLY ONE ER REVENUE (450/459) CODE PER VISIT INVALID OR MISSING HCPCS HCPC CODE NOT ON FILE PAYMENT REDUCED TO MEDICARE MAXIMUM MAXIMUM OF 2 DAYS ALLOWED TO TRANSFER MHISA PATIENTS HOSP LIMITED TO EMERG CARE & TRANSFER OF MHISA PATIENTS NOT COVERED-IS INVESTIG.,EXPERI.OR NOT MED.NECESSARY QUANTITY INVALID/MISSING A PRESCRIBING PHYSICIAN NPI OR MEDICAID ID REQUIRED RX DATE MISSING OR INVALID RX DATE WAS AFTER DATE FILLED DAYS SUPPLY MISSING,NOT NUMERIC, OR ZERO PRESCRIPTION NUMBER MISSING REFILL CODE MISSING, NOT NUMERIC, OR GREATER THAN 5 NDC CODE MISSING OR INCORRECT. THE MAC OVERRIDE INDICATOR MUST BE A 'C' PRESCRIBING PROV NPI MISSING/NOT ON FILE ALL PROVIDERS 9999999 TO BE DENY. PRIMARY DIAGNOSIS NOT ON FILE SECONDARY DIAGNOSIS NOT ON FILE BEHAVIORAL HEALTH CROSSOVER SENT TO SMO(MAGELLAN) DENIED ENCOUNTER SUBMITTED BY PLAN PATIENT NOT COVERED FOR PHARMACY SERVICE NO ELIGIBLE SERVICE PAID - ENCOUNTER DENIED MEDICARE REPLACEMENT; SUBMIT HARDCOPY ADJ OR VOID CLAIM ADJUNCT CD RPTD AS ONLY DETAIL LNE: REBILL W/ALL DETAIL ONE ADJUNCT CODE ALLOWED PER DDS: REBILL W/APPROP CODE THERAPEUTIC DUPLICATION-DIFFERENT PRESCRIBER REFILL NOT FILLED WITHIN 12 MONTHS CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 3 2 2 2 2 2 3 3 3 3 3 1 3 3 3 2 2 3 3 3 3 2 2 2 3 2 2 2 2 2 2 2 2 4 3 3 2 1 2 2 1 3 16 16 133 16 50 16 16 16 16 16 183 242 171 96 26 252 96 119 119 16 16 119 119 170 55 16 16 16 174 16 16 133 16 16 16 16 16 16 24 109 96 16 252 16 16 251 176 M52 M79 MA04 N180 M51 N65 N75 N37 N56 N450 N428 N30 N52 N29 N10 N435 N362 M20 N65 N45 N362 N95 M53 N31 N57 M53 N388 M119 M62 N257 N257 MA63 M64 N36 N30 N657 N4 N56 N56 MA81 N592 188 178 178 178 096 454 021 240 244 481 048 093 258 158 097 454 21 294 455 454 454 655 456 231 287 476 132 214 187 021 021 021 218 021 020 132 254 255 107 021 059 021 021 263 NCCI = CODE USED FOR NCCI ONLY. 249 325 221 219 216 381 562 538 519 306 453 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 4 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------142 143 144 145 146 147 148 149 150 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170 171 172 173 174 175 176 177 178 179 180 181 182 183 184 185 186 187 188 19:11:13 BILL PROV NPI NOF SERV PROV NPI NOF REF/PCP PROV NPI NOF BILL PROV NPI NO MAT SER PROV NPI NO MATC REF/PCP NPI NO MATCH 9F REF AUTH MISSING DESI-NOT PAYABLE LTC CERT DTE BAD MIXED ICD CODE SETS INV ICD CODE ON DOS QTY EXCEEDS MAX SITE # INVALD OR NOF REF MISS/REQ-MEDICAL REF MISS/REQ-VISION EXCEEDS LIMIT OF 8 REF MISS/REQ-HEARING LTC PROV NOT MATCHED PRECERT NOT ON FILE HOSP STAY REQ PRECRT PRECERT NOT APPROVED DOS NOT PRECERT COVD CLAIM > PRECERT LOS SURG REQUIRES PRECRT CLM RECIP NO MATCH CLM PROV ID NO MATCH DENY SPANDATE/UVS >1 DAYS CUT TO PRECERT PRECERT REVIEW NO PRECERT RESUB DOC CLM/PA DTE MUST MTCH LON/LOC NOT MATCHED RECIP NOT XREF CHARGES MISSING INVALID DEDUCTIBLE POST-OP XRAY REQUIRE INVALID BLOOD DEDUCT REF MISS/REQ-DENTAL INVALID ADMIT DATE INVALID COVERED DAYS PROC/CLAIM TYP CONFL SURGERY PROC NOF REF MISS/REQ-NUTRITN REQ NONCOVRD CHARGES USE CORRECT MODIFIER RECIP NOT ENROLL BYU TRIP CANC BY DISPTCH BILLING PROVIDER NPI MISSING/NOT ON FILE SERVING PROVIDER NPI MISSING/NOT ON FILE REF OR PCP PROVIDER NPI MISSING/NOT ON FILE BILLING PROVIDER NPI MISMATCH SERVICING PROVIDER NPI MISMATCH REFERRING/PCP NPI MISMATCH 9F REFERENCE AUTHORIZATION MISSING IN LOOP 2300 DESI INEFFECTIVE-NOT PAYABLE LTC CERTIFICATION DATE INVALID OR MISSING CLAIM CONTAIN MIXED ICD CODE SETS INVALID ICD CODE SET FOR CLAIM DATES OF SERVICE QUANTITY EXCEEDS MAX MD FAX OVERRIDE FOR 866-797-2329 SITE NUMBER INVALID OR NOT ON FILE REFERRAL MISSING AND REQUIRED FOR MEDICAL REFERRAL MISSING AND REQUIRED FOR VISION EXCEEDS LIMIT OF 8 CO-INS DAYS REFERRAL MISSING AND REQUIRED FOR HEARING LTC PROV NOT MATCHED PRECERT NUMBER NOT ON FILE HOSP STAY REQUIRES PRECERTIFICATION PRECERT HAS NOT BEEN APPROVED CLAIM DOS NOT PRECERT COVERED CLAIM EXCEEDS PRECERT AUTHORIZED DAYS SURGERY REQUIRES PRECERTIFICATION CLAIM RECIP ID DOES NOT MATCH ID ON PRECERT FILE CLAIM PROVIDER ID DOES NOT MATCH ID ON PRECERT FILE SPANDATE OR UVS>1 WILL DENY-BILL LA ST TX DATE AND UVS= DAYS CUTBACK TO PRECERT APPROVED DAYS PRECERT REVIEW NO HOSP PRECERT ON FILE RESUB WITH DOCUMENTATION CLAIM DATES MUST MATCH PRIOR AUTHORIZATION DATES LEVEL OF NEED / LEVEL OF CARE NOT MATCHED NO MEDICAID ID FOUND FOR MEDICARE ID NO CHARGES/COINS/DEDUCT GIVEN THE DEDUCTIBLE FIGURE MUST BE NUMERIC POST-OP XRAY REPORT REQUIRED SEND TO DENTAL PA UNIT THE BLOOD DEDUCTIBLE FIGURE MUST BE NUMERIC REFERRAL MISSING AND REQUIRED FOR DENTAL THE ADMISSION DATE WAS NOT A VALID DATE THE COVERED DAYS WAS NOT A VALID NUMERIC AMOUNT PROCEDURE CLAIM TYPE CONFLICT SURGICAL PROCEDURE NOT ON FILE REFERRAL MISSING AND REQUIRED FOR NUTRITIONAL NON-COVERED CHARGES REQUIRED OR USED FOR PAYMENT CRNA'S MUST BILL CORRECT MODIFIER RECIPIENT NOT ENROLLED WITH BYU HEALTH PLAN TRIP CANCELED BY DISPATCH (CLAIM VOIDED) CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 2 2 2 2 3 3 2 2 2 2 3 3 3 3 2 2 2 3 2 3 2 2 2 3 3 N257 N290 N286 N257 N290 N286 M62 N448 N351 N657 M76 N378 M77 2 2 2 3 2 2 3 2 3 2 2 3 2 3 16 16 16 16 16 16 16 96 96 16 146 16 16 165 165 119 165 16 15 15 39 16 198 15 16 16 59 198 133 15 15 16 31 16 16 96 16 165 16 16 5 16 165 2 3 3 4 243 115 N517 N130 N362 N257 N517 N517 N54 N54 N517 N54 N54 N54 N517 N517 M50 M54 N480 N435 M49 MA40 MA32 M51 562 562 562 020 020 020 020 218 021 21 21 021 048 048 483 048 021 252 252 084 084 258 084 084 084 465 258 046 252 084 021 162 178 021 123 021 048 189 456 275 227 048 562 562 562 562 220 580 255 255 187 138 153 649 258 098 037 453 093 294 337 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 5 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------189 190 191 192 193 194 195 196 197 198 199 200 201 202 203 204 205 206 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223 224 225 226 227 228 229 230 231 232 233 234 235 19:11:13 SHARED PLAN DOC MISS PA NO NOT ON FILE PROC REQUIRES PA PA NOT APPROVED DOS NOT COVERED/PA CLAIM OVER PA LIMITS NEED SPANNING DOS PA RECIP NQ CLM RECI PA PROV NQ CLM PROV PA PROC/NDC NE CLM TRIP CANCELED NONPAY PROV/ATTEND NOF PROVIDER NOT ELIG PROV CLAIM TYP CONFL PROVIDER ON REVIEW GRP NOT ON INDIV REC NOT IN GROUP ON DOS BILL PROV NOT ON FIL BILL PROV NOT ELIG PRESCRIB PROV ONLY GRP MST BILL FOR PRV PROV PROC CONFLICT DOS LESS THAN DOB PROV MUST BE INDIV PROVIDER NOT COVERED PROV ALLOW 1 PROC/CM RECIPIENT NOT ON FIL RECIPIENT NOT ELIG RECIP NAME MISMATCH LOCK IN RECIPIENT EPSDT REFER OVER 21 SPD DOWN NOT MED NDY GEN ASST - NOT COVRD SVC OVERLAPS REC ELI RECYC RECIP N/O FILE INVALID BIRTHDATE P.E. - NOT COVERED INV SURGERY MODIFIER POSSIBLE 707 PEND POSSIBLE 713 PEND POSSIBLE 714 PEND PROC REVIEW NDC NOT ON P/F FILE PROCEDURE CODE NOF P/F DATE RESTRICTION P/F AGE RESTRICTION P/F SEX RESTRICTION BYU SHARED PLAN DID NOT SUBMIT DOCUMENTATION TO MOLINA PA NUMBER NOT ON FILE PROCEDURE REQUIRES PRIOR AUTHORIZATION PA HAS NOT BEEN APPROVED DATE ON CLAIM NOT COVERED BY PA CLAIM EXCEEDS PRIOR AUTHORIZED LIMITS MUST HAVE SPANNING DOS IF BILLING FOR TOTAL AUTH AMOUNT CLAIM RECIPIENT ID DOES NOT MATCH ID ON PRIOR AUTH FILE PA PROVIDER ID NOT SAME AS CLAIM PROVIDER ID PA PROCEDURE/NDC NOT EQ CLAIM PROCEDURE/NDC TRIP CANCELED NON PAYABLE PROVIDER/ATTENDING PROVIDER NOT ON FILE PROVIDER NOT ELIGIBLE ON DATES OF SERVICE PROVIDER CANNOT SUBMIT THIS TYPE CLAIM PROVIDER ON REVIEW BILLING PROV NOT ON ATTENDING PROV RECORD ON DOS ATTENDING PROV NOT IN GROUP ON DATE OF SERV BILLING PROVIDER NOT ON FILE BILLING PROVIDER INELIGIBLE ON DATE OF SERV PRESCRIBER ONLY-CALL 1-800-473-2783 FOR INFO GROUP MUST BILL FOR PROVIDER PROVIDER NOT CERTIFIED FOR THIS PROCEDURE DATE OF SERVICE LESS THAN DATE OF BIRTH ATTENDING PROVIDER MUST BE INDIVIDUAL PROVIDER NOT COVERED FOR SERVICES RENDERED BY MEDICAID PROVIDER ALLOWED 1 SERVICE PER RECIPIENT PER DAY RECIPIENT NOT ON FILE RECIPIENT NOT ELIGIBLE ON DATE OF SERVICE NAME AND/OR NUMBER ON CLAIM DOES NOT MATCH FILE RECORD RECIPIENT IS MD, PHARM RESTRICTED-MD INVALID EPSDT REFERRAL FOR RECIPIENT OVER 21 SPEND DOWN AMOUNT NOT MED NEEDY STATE ONLY ASSISTANCE - SERVICE NOT COVERED RECIPIENT INELIGIBLE ON ONE OR MORE SERVICE DATE(S) RECYCLED RECIPIENT NOT 0N FILE INVALID BIRTHDATE ON RECIPIENT FILE CLAIM NOT COVERED FOR PRESUM ELIG RECIP COMPONENTS OF SURGERY PAID ONLY TO TEACHING FACILITIES CLAIM IN PROCESS CLAIM IN PROCESS CLAIM IN PROCESS PROC REQUIRES REVIEW NDC CODE NOT ON FILE PROCEDURE/TYPE OF SERVICE NOT COVERED BY PROGRAM PROCEDURE/NDC NOT COVERED FOR SERVICE DATE GIVEN P/F AGE RESTRICTION P/F SEX RESTRICTION CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 1 2 2 3 2 3 2 2 2 2 3 2 3 3 3 3 2 3 3 3 3 2 3 3 3 3 3 2 3 3 3 3 3 3 2 3 3 2 2 2 3 3 148 15 15 39 16 198 15 15 15 15 115 16 B7 170 133 96 96 16 B7 96 96 8 14 96 B7 119 31 27 140 184 96 177 96 96 31 16 96 171 133 133 133 133 16 16 16 6 7 N706 N517 N517 N54 N54 N517 N517 N517 N517 N289 N570 N95 N55 N55 N257 N570 N95 N55 N95 N55 N570 N362 N30 N30 N30 N30 N329 N30 N428 M119 N56 N56 N129 N517 132 252 454 084 084 252 252 084 084 084 294 132 109 132 049 026 677 026 109 109 026 132 158 132 109 483 026 109 030 085 001 006 109 109 026 158 097 109 001 419 419 046 218 454 454 475 474 NCCI = CODE USED FOR NCCI ONLY. 276 258 337 048 564 585 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 6 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------236 237 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266 267 268 269 270 271 272 273 274 275 276 277 278 279 280 281 282 19:11:13 P/F PLACE RESTRICT P/F PROV SPEC RESTRT INV PAC CALL HELP DK PRICE MISSING ON P/F PRICE MISSING ON U/C CLAIM IN PROCESS INPUT SPENDDOWN AMT POT NOT ICF-I OR II PROV RATE NOF INVAL PROC TOS TRANS STAND BY NEC. O.P.AUTH. EXT. NEED DELETED,BILL CURR CD SURG REQ MED REV DIAG/PROC REQ REVIEW DENY FOR DIAGNOSIS DIAGNOSIS NOT ON FIL DIAG DATE RESTRICT DIAG AGE RESTRICTION DIAG SEX RESTRICTION DIAG PROC RESTRICT PAS-LOS 90TH EQ ZERO SPAN DATES/QUANT DIF ANESTH REQ REVIEW ANESTHESIA UNITS NOF INPUT M-CARE PD AMT. ADJ-REQUIRES-REVIEW PROCEDURE-AGE-RESTRT PA-01 REQUIRES REVIE SURG REQUIRES PA-0 INVALID AMB SURG REV REQ-ICD9-SURGICAL-CD INVALID-TREATMENT-PL ANES.CPT N/C-M'AID CLAIM OVER 90 DAYS SER HOSPICE RELATED CLAIM OVER 1 YEAR TPL/PRIVATE POSSIBLE TPL RECIP MEDICARE ELIG HIGH VARIANCE ERROR LOW VARIANCE ERROR RECIP ELIG MEDICARE PROF COMP INVLD POT MANUAL PRICE REQ VISIT INC. SURG CHGS PRE-OP INC IN SURG. P/F PLACE RESTRICTION P/F PROVIDER SPECIALTY RESTRICTION INVALD PAC VS DOS / CALL HELP DESK PRICE MISSING FOR DATE OF SERVICE ON P/F CALL HELP DESK U AND C FILE - NO VALID PRICE FOR DOS CLAIM HELD FOR PRE-PAYMENT REVIEW 110-MNP REQUIRED FOR RECIP LIABILITY AMOUNT PLACE OF TREATMENT MUST BE ICF-I OR ICF-II PROVIDER FILE DOES NOT CONTAIN VALID RATE FOR DOS INVALID PROCEDURE TOS FOR TRANSPORTATION PROLONGED ATTENDANCE BILLED;PENDED FOR REVIEW FOUND NO DOC/EDIT OVERRIDE CODE OUTPATIENT EXTENSION DELETED,BILL CURRENT CODE SURGERY REQUIRES REVIEW FOR ATTACHMENTS DIAGNOSIS/PROCEDURE REQUIRES REVIEW PROCEDURE DENIED NOT JUSTIFIED BY DIAGNOSIS DIAGNOSIS NOT ON FILE DIAG DATE RESTRICTION DIAGNOSIS AGE RESTRICTION DIAG SEX RESTRICTION DIAGNOSIS/PROCEDURE RESTRICTION DX CODE REQUIRES 5TH DIGIT TO CALCULATE PAS DAYS DIFFERENCE BETWEEN SERVICE DATES AND QUANT ANESTHESIA UNITS/MINUTES REQUIRE MED REVIEW ANESTHESIA BASE UNITS ARE NOT ON FILE INSERT PROVIDER PAID AMOUNT BY MEDICARE PROVIDER'S ADJUSTMENTS ON REVIEW PROCEDURE ALLOWED FOR RECIP 0-30 DAYS OLD PA-01 FORM REQUIRES REVIEW FOR VALIDITY SURGERY DONE AS IP REQUIRES VALID PA-01 FORM REV CODE INVALID FOR AMBULATORY SURG PROC. REVENUE CODE 490 REQUIRES VALID ICD9 SURGICAL PROCEDURE TREATMENT PLACE IS INCORRECT ANES.CPT NOT COVERED FOR MEDICAID ONLY-BILL SURG+MOD. CLAIM EXCEEDS 90 DAY FILING LIMIT (PHARMACY) HOSPICE RELATED/SUB BILL TO HOSPICE 30 DAYS TO APPEAL CLAIM EXCEEDS 1 YEAR FILING LIMIT 3RD PARTY CARRIER CODE MISSING-REFER TO CARRIER CD.LIST POSSIBLE THIRD PARTY LIABILITY RECIPIENT IS MEDICARE ELIGIBLE HIGH VARIANCE ERROR LOW VARIANCE ERROR RECIPIENT POSSIBLY ELIGIBLE FOR MEDICARE INVALID PLACE OF TREATMENT FOR PROF COMP MANUAL PRICING REQUIRED/HARD COPY BILL OFFICE VISIT CONS. BILLED SEP. FROM SURG FEE PRE-OP INCLUDED IN TOTAL SURGICAL FEE CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 3 2 2 2 2 3 3 2 3 2 3 2 2 2 3 3 2 2 2 2 3 1 2 2 2 2 3 3 3 2 3 3 3 3 3 4 4 5 96 16 16 16 133 16 5 B7 16 133 119 16 133 133 11 16 16 9 10 11 16 16 133 16 16 133 6 133 252 16 16 16 16 29 29 29 16 22 22 96 133 22 5 133 97 97 M77 N95 N65 N65 N65 N58 M77 N570 N56 N435 M20 MA63 M76 N517 N517 M76 M53 M53 MA92 N129 N29 M50 M51 M77 N34 MA92 N372 M77 N390 M144 249 145 021 021 066 046 294 249 001 250 001 021 001 046 046 255 255 255 255 086 255 255 476 046 476 001 046 475 046 252 455 001 249 454 187 187 187 286 171 171 178 178 085 249 046 001 001 NCCI = CODE USED FOR NCCI ONLY. 402 490 402 490 450 499 674 655 666 666 526 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 7 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------283 284 285 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 19:11:13 SALES TAX NOT ON CLM MANUAL PRICE GR BILL PAYMENT GR BILLED CH REF MISS/REQ-DEVELOP PAT LIAB EXCEEDS CHG PROC/DESC CONFLICT INV DENY FOR PROV NO TPL RESOURCE REQ EOB FOUND MULT RESOURCES FOUND NO TPL AMOUNT RECYC RECI INELG DOS RECYC RECIP NOF RECIP RECYC 3 TIMES. CAR-CODE REQ REVIEW BANKRUPT.FILE W/CARR INVALID PROC CODE PROC/DRUG NOTCOVERED CLAIM SPANS FISCL YR ADMISN MUST BE EMER REF MISS/REQ-AB/NEGL HOSPICE DAYS > 5 RECIP NOT IN DBP INV BABY/MTHR PROC INV BABY ADMISSION SURG PROC MISSING REF MISS/REQ-PSY/SOC SURG DATE MISSING SURG DTE LT SRV FROM C-II EXPIRED 90 DAYS REF MISS/REQ-SPEECH SUBMIT TO FI SUSP CON MIS/REQ-RF1 NEGATIVE TPL AMT NOT COV DAYS NE ACCOM STMT DTE/ACCOM CONFL SUSP CON MIS/REQ-RF2 SUSP CON MIS/REQ-RF3 REF ASST MIS/REQ-RF1 PSRO FROM LT ST FROM CLAIM OVER 180 DAYS REF ASST MIS/REQ-RF2 REF ASST MIS/REQ-RF3 EXCEEDS MAX DAILY APP DATE MIS/REQ-RF1 ADJ > ORIG COV'D DYS NH/ICF NOT COVERED CLIA NOT CERT DOS SALES TAXES NOT PRESENT ON RX CLAIM WITH TPL MANUAL PRICE EXCEEDS BILLED CHARGES PAYMENT EXCEEDS BILLED CHARGES/REQUIRES REVIEW REFERRAL MISSING AND REQUIRED FOR DEVELOPMENTAL PATIENT LIABILITY EXCEEDS BILLED CHARGES PROCEDURE CODE/DESCRIPTION CONFLICT INVALID PROVIDER NUMBER WHEN DENY APPLIED NO EOB ATTACHED FOR RECIP WITH OTHER RESOURCE INDICATED CLAIM REQUIRES REVIEW FOR MULTIPLE TPL RESOURCES NO TPL AMOUNT INDICATED ON CLAIM/REQUIRES REVIEW RECYCLED RECIPIENT INELIG ON DOS RECIPIENT NOT ON FILE RECYCLED 3 TIMES RECIPIENT INELIGIBLE RECYCLED THREE TIMES CARRIER CODE REQUIRES REVIEW/POSS NO MATCH DECLARED BANKRUPTCY.FILE W/CARRIER FOR POSSIBLE PMTS. INVALID PROCEDURE CODE FOR DATE-OF-SERVICE PROC/DRUG NOT COVERED BY MEDICAID CLAIM SPANS FISCAL YEAR EMERGENCY ACCESS HOSP - NATURE OF ADMISN MUST BE EMER REFERRAL MISSING AND REQUIRED FOR ABUSE/NEGLECT INPATIENT RESPITE DAYS GREATER THAN FIVE RECIPIENT EXCLUDED FROM DBP BABY AND MOTHER - SURGICAL PROCEDURE MUST BE DELIVERY BABY ONLY / PENDING FOR REVIEW. SURGICAL PROCEDURE MISSING REFERRAL MISSING AND REQUIRED FOR PSYCHOLOGICAL/SOCIAL DATE OF SURGERY MISSING DATE OF SURGERY LESS THAN SERVICE FROM DATE C-II EXPIRED-GREATER THAN 90 DAYS REFERRAL MISSING AND REQUIRED FOR SPEECH/LANGUAGE SUBMIT CLAIM TO FISCAL INTERMEDIARY,NOT BYU OR LBHP PLN SUSPECTED CONDITION MISSING AND REQUIRED FOR REFERRAL 1 NEGATIVE TPL AMOUNT NOT ALLOWED COVERED DAYS DO NOT EQUAL ACCOMODATION DAYS STATEMENT DATES CONFLICT WITH ACCOMODATION DAYS SUSPECTED CONDITION MISSING AND REQUIRED FOR REFERRAL 2 SUSPECTED CONDITION MISSING REQUIRED FOR REFERRAL 3 REFERRAL ASSISTANCE MISSING AND REQUIRED FOR REFERRAL 1 PSRO FROM DATE LESS THAN STATEMENT FROM DATE CLAIMS EXCEEDS 180 DAY FILING LIMIT REFERRAL ASSISTANCE MISSING AND REQUIRED FOR REFERRAL 2 REFERRAL ASSISTANCE MISSING AND REQUIRED FOR REFERRAL 3 EXCEEDS MAX DAILY DOSE MD FAX OVERRIDE FORM866-797-2329 APPOINTMENT DATE MISSING AND REQUIRED FOR REFERRAL #1 ADJUSTED COVERED DAYS > ORIGINAL COVERED DAYS NOT COVERED FOR RECIPIENT IN NH/ICF CLIA # DOES NOT COVER DATE OF SERVICE CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 3 3 2 2 2 3 3 3 3 2 3 2 3 2 3 2 2 3 2 2 3 3 3 3 2 2 2 3 3 3 2 3 3 3 2 3 3 3 3 16 16 16 165 178 16 16 16 133 133 27 31 27 133 22 16 96 133 16 165 16 243 16 133 16 165 16 16 176 165 96 165 15 16 16 165 165 165 16 29 165 165 16 165 198 96 B23 M54 M49 M49 M51 N77 MA04 N30 N30 N56 N643 MA41 MA31 N130 N56 M51 MA31 MA31 N592 N52 N517 MA32 M53 N300 046 178 048 106 306 132 285 052 052 109 026 109 046 001 454 454 046 231 048 021 483 093 626 666 046 021 666 048 187 187 048 487 048 456 188 048 048 048 021 142 187 048 048 N378 N54 M97 048 225 258 107 630 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 8 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350 351 352 353 354 355 356 357 358 359 360 361 362 363 364 365 366 367 368 369 370 371 372 373 374 375 376 19:11:13 QMB NOT MED. ELIG. ABORTION JUST STERILIZATION < 21 AUTH MINOR UNM MO CONSENT 30/180 DAYS SERVICE LIMIT REVIEW AB REQUIRES REVIEW CONSENT FORM REVIEW HYSTER REQ REVIEW OCCUR DATES CONFLICT SPAN DAYS CONFLICT DENY TO BE REBILLED PSRO DATES MISSING APP DATE MIS/REQ RF2 MUST SPLIT BILL INV ZERO BILLED DAYS NOT USED - AVAILABLE EXCEEDS MAX-23 DAYS S/C EXCDS 80% C-CARE INVALID TYPE CASE LTC SNF/DTE ERR SPAN DATE INVALID INV LTC CERT DATE SRV DTE PRIOR CERTIF NOT USED - AVAILABLE NO 51 NH TOT/LOC DAYS CONFL LTC DAYS/DATES CONFL INVLD RATE FOR LOC APP DATE MIS/REQ-RF3 PROV CERT DATE ERROR RECIP EXCD HM/LV DYS SND PLAN PROOF STERL OFS 24 NOT ON FILE RECIP INELIG/DECEASE ANESTH REP REQ SEND OP&PATH REPORT ADJ. DENY REF REAS MIS/REQ-RF1 SUBMIT TO DBPM UNABLE TO CALCU COS TIMELY FILING REVIEW INVALID LEAVE CODE INVALID LEAVE DATE INSUFFICIENT DATA PT STAT REQ HOSP LVE ADJ DAYS CONFL HIST QMB NOT MEDICAID ELIGIBLE DOES NOT MEET PROGRAM CRITERIA FOR ABORTION STERILIZATION IS NOT COVERED FOR RECIPIENT UNDER 21 FOUND NO DOCUMENT/OVERRIDE CODE MINOR UNM MOTHER/UNBORN CONSENT MUST BE AT LEAST 30 BUT NO MORE THAN 180 DAYS ATTACHMENT REVIEW SERVICE LIMITS ABORTION REQUIRES REVIEW STERILIZATION OFS FORM 96 REQUIRES REVIEW ACKNOWLEDGEMENT REQUIRES REVIEW OCCUR CODES/DATES CONFLICT SPAN DAYS/NON COVERED DAYS CONFLICT DENY TO BE REBILLED TO MEDICARE PSRO DATES MISSING - DATE PRIOR TO 070183 APPOINTMENT DATE MISSING AND REQUIRED FOR REFERRAL #2 SPAN FROM & THRU DATES CONFLICT MUST SPLIT BILL DAYS ZERO, PATIENT STATUS NOT 9 NOT USED - AVAILABLE EXCEEDS MAXIMUM MONTHLY DAYS SERVICE CHARGE EXCEEDS 80% OF COMPARABLE CARE RECIPIENT NOT COVERED FOR THIS SERVICE LTC SNF THRU DATE IN ERROR SPAN DATE NOT ALLOWED MUST BILL PER DAY LTC CERTIFICATION DATE INVALID SERVICE DATE IS PRIOR TO LTC CERTIFICATION DATE NOT USED - AVAILABLE NO 51 NH ATTACHED OR ADMIT CODE MUST BE A '6' TO-DAY / TOT-DAYS / STATUS CONFLICT LTC LOC DAYS CONFLICT WITH LTC LOC FROM AND THRU DATES NO VALID RATE WAS FOUND FOR LTC LEVEL OF CARE APPOINTMENT DATE MISSING AND REQUIRED FOR REFERRAL #3 PROVIDER CERTIFICATION EXPIRED AS OF DOS RECIPIENT HAS USED THE MAXIMUM HOME LEAVE DAYS OF 25 HYSTERECTOMY REQUIRES PROOF OF PRIOR STERILE TO PLAN OFS 24 NOT ON FILE RECIPIENT INELIGIBLE/DECEASED ANESTHESIOLOGY REPORT REQUESTED SEND BOTH OPERATIVE AND PATHOLOGY REPORT ADJUSTMENT DENIED/ORIG CLAIM PAID CORRECTLY REASON FOR REFERRAL MISSING AND REQUIRED FOR REFERRAL 1 SUBMIT TO DENTAL BENEFITS PLAN CLAIM IN PROCESS ATTACHMENT REQUIRES REVIEW/FILING DEADLINE ABSENT DAY TYPE MUST BE AN A OR B ABSENT DAY AND/OR TOTAL DAYS CONFLICT UNABLE TO PROCESS/REBILL/ATTENTION P.MISNER PT STATUS CODE 1 REQUIRES HOSPITAL ABSENT DAYS ADJUSTMENT DAYS CONFLICT WITH HISTORY DAYS CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 3 3 1 1 2 2 3 2 3 2 2 1 3 3 3 2 2 2 2 1 1 2 2 2 3 3 3 1 3 2 1 1 3 3 3 3 2 2 2 31 B5 6 252 251 133 133 133 133 16 16 22 16 165 16 16 252 119 96 96 16 16 16 16 252 252 16 16 16 165 B7 119 252 96 13 252 252 B13 165 166 133 29 133 133 16 16 16 N129 N29 N28 M46 MA33 N299 N300 M53 M29 N362 N372 N30 M59 N63 N322 M52 M29 N473 M53 M53 N65 N570 N362 M29 N194 N29 M29 MA130 M46 M53 109 046 475 475 187 046 046 046 046 719 457 116 021 142 048 722 258 483 178 107 021 187 021 187 408 187 021 476 188 021 048 187 483 298 021 109 304 298 021 048 132 021 046 021 021 021 258 021 NCCI = CODE USED FOR NCCI ONLY. 408 499 580 101 041 258 258 287 258 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 9 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------377 378 379 380 381 382 383 384 385 386 387 388 389 390 391 392 393 394 395 396 397 398 399 400 401 402 403 404 405 406 407 408 409 410 411 412 413 414 415 416 417 418 419 420 421 422 423 19:11:13 PAYABLE QMB RECIP NO MEDICARE PAID DTE HOME LEAVE DAY REDUC AMBULANCE-REQ-ATTACH LTC-MED-LOA-OVER-10 HOSPICE MUST BILL SERV. IN MED SCREEN. NOT COVERED NH RESID NOT COVERED NH RESID NOT PAY W/CLIA CERT CLIA # NOT ON FILE RECIP NOT COVER,DRUG LOCK-IN RECIPIENT SERV, MAX 1 PER MO LTC LV DAYS OVER MAX ICF-MR LV OVER MAX NOT USED - AVAILABLE REHAB CTR SRV NOT CO HOSP LEAVE DAYS > 7 HOME LEAVE DAYS > 15 CLAIM-NEEDS-80-MOD NOT USED - AVAILABLE REF REAS MIS/REQ-RF2 REFER PHYSICIAN REQD CONCURRENT CARE NO SERV EXCEEDS MAX MULTIPLE SURGERY PMPM RECOUP FOR DOD OUTSIDE LAB NOT COVD EXCEEDS 3 TREATMENTS NONEMER TRANS REQ PA NON-EMER MLS GR 400 PMPM RECOUP - LAHIPP ENC PREFIX ERROR REF NAME MIS/REQ-RF1 REF NAME MIS/REQ-RF2 DME REQUIRES PA ENC PLAN PMT DT ERR PA AMOUNT GR LEVEL3 ENC RCV DT ERROR ENC INT PMT ERROR PMPM RECOUP - DOC OFS REV PA DT GT DOS SPECIALTY RESTRICTED NOT USED - AVAILABLE NEW PRESC OVER 12 MO ONE H.HLTH AIDE/DAY PAYABLE ONLY FOR QMB RECIP MEDICARE PAYMENT DATE IS MISSING OR INVALID HOME LEAVE DAYS REDUCED TO ONE/HALF PER DIEM CLAIM REQUIRES MD CERTIFICATION ATTACHED AFTER 2/14/87 LTC LEAVE DAYS EXCEED LIMIT - 10 PER HOSPITAL STAY HOSPICE CLIENT -ONLY HOSPICE PROVIDER CAN BILL SERVICE INCLUDED IN MED SCREENING NOT COVERED FOR NURSING HOME RESIDENT DIABETIC SUPPLIES NOT COVERED FOR LTC RECIPIENT NOT PAYABLE WITH CLIA CERT TYPE NO CLIA # ON OUR FILE RECIPIENT NOT COVERED FOR THIS DRUG RECIP IS MD,PHARM RESTRICTED-PHARMACY INVALID SERVICE EXCEEDS MAXIMUM ALLOWABLE OF 1 PER MONTH LTC HOSP LEAVE DAYS IN EXCESS OF MAXIMUM-5-BUDGET CUT ICF-MR HOME LEAVE IN EXCESS OF MAXIMUM 22/30 BUDGET CUT NOT USED - AVAILABLE REHAB CENTER SERVICES NOT COVERED-NURSING HOME RESIDENT HOSPITAL LEAVE DAYS EXCEED 7 HOME LEAVE DAYS EXCEED 15 APPEARS TO BE ASSISTANT--REBILL WITH 80 MODIFIER NOT USED - AVAILABLE REASON FOR REFERRAL MISSING AND REQUIRED FOR REFERRAL 2 REFERRING/ATTENDING PHYSICIAN REQUIRED CONCURRENT CARE IS NOT COVERED BY THE PROGRAM NUMBER OF SERVICES EXCEEDS STATE MAX/ CUTBACK APPLIED MULTIPLE SURGERY - PENDED FOR MANUAL PRICING PMPM RECOVERY FOR DECEASED MEMBERS BASED ON DATEOFDEATH OUTSIDE LABORATORY SERVICES NOT COVERED EXCEEDS THREE CHIRO TREATMENTS SAME DAY NON-EMER TRANSPORTATION REQUIRES PRIOR AUTHORIZATION NON-EMER MILES EXCEED 400-STATE AUTHO REQUIRED PMPM RECOVERY FOR LAHIPP ELIGIBLES LICN PREFIX ON ENCOUNTER IS MISSING OR INVALID REFERRED TO NAME IS MISSING AND REQUIRED FOR REFERRAL 1 REFERRED TO NAME MISSING AND REQUIRED FOR REFERRAL #2 DME REQUIRES PRIOR AUTHORIZATION PLAN PAYMENT DATE ON ENCOUNTER IS MISSING OR INVALID PRIOR AUTHORIZED AMOUNT GREATER THAN LEVEL 3 CHARGE PLAN RECEIVE DATE ON ENCOUNTER IS MISSING OR INVALID INTEREST PAYMENT ON PLAN ENCOUNTER IS INVALID PMPM RECOVERY FOR INCARCERATED MEMBERS OFS TO REVIEW-PA DATE GREATER THAN SERVICE DATE PROVIDER IS RESTRICTED TO DESIGNATED PROCEDURES PER OFS NOT USED - AVAILABLE NEW PRESCRIPTION NOT FILLED WITHIN 12 MO OF DATE PRESC ONLY ONE HOME HEALTH AIDE VISIT ALLOWED PER DAY CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 2 3 1 3 3 4 3 3 3 2 3 3 3 3 3 96 16 96 252 96 B9 97 96 96 B23 16 96 185 119 96 96 N30 MA04 N59 M60 N43 3 3 3 2 2 3 2 3 3 3 3 3 3 2 2 3 1 3 3 2 2 96 96 96 4 16 165 16 B14 119 59 256 5 119 15 15 256 251 165 165 15 16 133 251 16 256 133 170 96 176 119 N174 N43 N43 N517 N56 1 2 3 3 3 3 3 N390 N174 N174 MA120 N30 M86 N43 N43 N286 M86 N362 M77 M86 N517 N517 N464 N517 N480 N446 M49 N95 N54 N592 M86 590 286 187 337 483 487 103 091 091 373 630 026 630 084 155 483 483 483 088 483 483 453 048 132 483 483 046 187 179 483 252 267 187 048 048 048 252 048 048 628 048 048 187 046 025 263 483 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 10 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------424 425 426 427 428 429 430 431 432 433 434 435 436 437 438 439 440 441 442 443 444 445 446 447 448 449 450 451 452 453 454 455 456 457 458 459 460 461 462 463 464 465 466 467 468 469 470 19:11:13 NOT PROV OF RECORD NOT USED - AVAILABLE BILL HR CD PRE 15MIN PSYCH SERV NOT COVER ADMIN.PEND NOT PAY FOR MED NEED MOD NOT NEEDED-RESUB M/I PROF SERV CODE QTY > PACKAGE SIZE MISSING/INVALID DIAG BILL MEDCARE NEB MED KIDMED TIMELY FILLIN DAYS SUPPLY OVER MAX QTY OF 1 = 1 VIAL NDC OBSOLETE/MFTR MFT SAYS FOOD SUPPLM SITE N/ALLW BILL/DOS 2A,2B-RX NOT FILLED DRUG/DRUG INTERACT THERAPEUTIC OVERLAY M/I SERVICE PROVIDER DUP DRUG THERAPY PREGNANCY PRECAUTION MON.EARLY/LATE REFIL GIVE DATE FOR TRANSP BILL MEDICARE FIRST PRESCRIBER NOT ON FI PRESC DENTAL AGE ERR SCH2 NARC NO REFILL SCH2 NARC OVER 5 DAY NEW PRESC OVER 6 MOS REFILL OVER 6 MONTHS NOT USED - AVAILABLE QTY OVER PROGRAM MAX MAC/FUL COST IS ZERO DENY FOR FILE REVIEW NDC MAY BE OBSOLETE REFILLS NOT PAYABLE NDC TERMINATED/CMS MAC OVERRIDE NOT NEE DRUG IS KIT/VERF.QTY INVALID NDC HRD COPY REQ-FERTILI COV MDCARE IF INSULI JUSTIFY EYEGLASSES EYEWEAR DENIED ANES AND MED DOC REQ BILLING PROVIDER IS NOT THE DESIGNTED PROV. OF RECORD NOT USED - AVAILABLE BILL CM HOUR CODE BEFORE 15 MIN CODE PSYCHIATRIC SERVICES NOT COVERED UNDER HOME HEALTH ADMINISTRATIVE PEND NOT PAYABLE FOR MED NEEDY PROGRAM MODIFIER NOT NEEDED-REMOVE AND RESUBMIT MISSING/INVALID PROFESSIONAL SERVICE CODE QUANTITY EXCEEDS PACKAGE SIZE MISSING/INVALID DIAGNOSIS CODE BILL MEDICARE NEBULIZER MED KM CLAIMS SHOULD BE SUBMITTED WITHIN 60 DAYS OF SERVICE DAYS SUPPLY >100 EXCEEDS PROGRAM MAXIMUM DRUG IS A VIAL. QUANTITY OF 1 = 1 VIAL MANUFACTURER NOTIFIED US THAT NDC IS OBSOLETE MANUFACTURER HAS IDENTIFIED PRODUCT AS FOOD SUPPLEMENT PROV SITE NOT ALLWD TO BILL SCR TYPE ON DATE OF SERVICE OUTCOME 2A OR 2B -RX NOT FILLED -TRANSACTION REPORTING DRUG/DRUG INTERACTION THERAPEUTIC OVERLAY MISSING/INVALID SERVICE PROVIDER DUPLICATE DRUG THERAPY PREGNANCY PRECAUTION COMPLIANCE MONITORING/EARLY OR LATE REFILL TRANSPLANT DISCHARGE DATE OR OTHER DX NEEDED BILL MEDICARE FIRST BASED ON DISCHARG DATE PRESCRIBING PROVIDER NOT ON FILE DENTAL PRESCRIBER, RECIPIENT 21 OR OVER SCHEDULE 2 NARCOTIC CANNOT BE REFILLED SCHEDULE 2 NARCOTIC NOT FILLED WITHIN 5 DAYS NEW PRESCRIPTION NOT FILLED WITHIN 6 MOS. OF DATE PRESC REFILL NOT FILLED WITHIN 6 MONTHS NOT USED - AVAILABLE QUANTITY AND/OR DAYS SUPPLY EXCEEDS PROGRAM MAXIMUM MAC/FUL COST IS ZERO/CALL HELP DESK DENY FOR REVIEW / CALL POS HELP DESK NDC POSSIBLY OBSOLETE REFILLS NOT PAYABLE CMS NOTIFIED US THAT NDC IS TERMINATED DRUG DOES NOT NEED MAC OVERRIDE DRUG UNIT OF MEASUREMENT IS A KIT.PLEASE VERIFY QUANTIT INVALID NDC - NOT AVAILABLE HARD COPY REQUIRED-FERTILITY PREPARATION ITEM COVERED BY MEDICARE IF REC IS INSULIN TREATED SEND DOCUMENTATION FOR MORE THAN 3 EYEGLASSES PER YEAR LIMITATION MET - SUBMIT JUSTIFICATION FOR ADD'L EYEWEAR ATTACH ANESTHESIA RECORD AND DOCUMENT MEDICAL NECESSITY CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 4 2 3 3 2 2 2 2 3 3 3 2 3 3 3 3 3 3 2 2 3 3 2 3 3 3 3 3 3 2 3 2 2 3 2 3 2 1 3 1 3 1 185 24 16 96 133 96 4 16 16 16 22 29 154 16 96 96 171 115 153 153 206 18 153 154 16 22 184 133 96 96 176 176 15 154 133 16 16 96 16 133 153 16 252 22 251 119 252 093 M20 N174 N30 N517 N56 N378 M76 N378 N448 N59 N428 N522 N341 N410 N410 452 084 040 088 453 562 476 021 116 187 221 221 218 107 021 216 216 216 021 216 216 216 021 116 132 109 216 263 263 263 255 025 562 190 N517 N65 M119 N410 M119 M119 N29 N464 N435 N439 483 110 046 218 483 218 021 001 218 001 373 121 294 294 NCCI = CODE USED FOR NCCI ONLY. 216 724 279 483 287 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 11 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------471 472 473 474 475 476 477 478 479 480 481 482 483 484 485 486 487 488 489 490 491 492 493 494 495 496 497 498 499 500 501 502 503 504 CLMCHK-505 506 507 508 509 510 511 512 513 514 515 516 517 19:11:13 DRUG-DRUG INTERACTIO MFCTR NOT IN REBATE EDITED FOR MEDICARE EDITED FOR INSURANCE QW MODIFIER NEEDED BILL VISITS--SEE CPT JUSTIFY OVER 1/A/YR SONOGRAM-AND REPORTS DUR DATA UNNECESSARY DEDUCT EXCEEDS MAX JUSTIFY LAB TEST THERAPEUTIC DUP DENY PREGNANCY DENIAL NEW RX REQUIRES PA PA REQUIRED PA EXPIRED PA-EMERGENCY-OVERRID ONLY-1ST DIAG,VS PD INVALID PRESCRIBERNO UTILIZE HMO PRESCRIBER IS GROUP HMO REVIEW NON HOSPICE PROVIDER INVALID MSA CODE NOT HOSPICE ELIGIBLE LEERS DATA CONFLICT INV PRESCRIB ID QUAL NO OF RX GR THAN LIM JUSTIFY PATH CONSULT USE 62/66 MOD,RESUB CANNOT ADJUST PREPAY EXACT DUPE 16 TO 02 EXACT DUPE 16 TO 16 EXACT DUPE 17 TO 01 CLM RECD NO CC EDITS SUB PROV NON PAR BYU SUBMIT TO PREPAID PL NON WAIVER PAY IP M/I SERV PRV ID QUAL ALLOW 1 PER 7 YEARS PROV/HOSPICE NO MTCH VNS REPROGRAMMING HCPCS REQ NO PRESCRIPTIVE AUTH O/R REQ-SEND TO PA CANNOT REVERSE CLAIM KIDMED FORMAT REQUIR DRUG TO DRUG INTERACTION-DENY MANUFACTURER HAS NOT ENTERED INTO HCFA REBATE AGREEMENT EDITED FOR MEDICARE -SERV. PAYABLE EDITED FOR INSURANCE SERV. PAYABLE QW MODIFIER NEEDED FOR TYPE OF CLIA CERTIFICATE SEE CPT-MEDICAL TREATMENT OF ABORTION USE E AND M CODES SEND DOC TO JUSTIFY OVER ONE PROCEDURE PER YEAR SEND WRITTEN SONOGRAM RESULTS WITH OP,PATH AND HISTORY DUR DATA UNNECESSARY FOR CONFLICT,INTERVENTION,OUTCOME DEDUCTIBLE EXCEEDS MAXIMUM SEND DOCUMENTS TO JUSTIFY SPECIFIC LAB TEST THERAPEUTIC DUPLICATION DENIAL-LIMITED TO SPECIFIC CLAS PREGNANCY PRECAUTION-DENIAL-FDA CATEGORY X NEW RX WILL REQUIRE PA MD MUST CALL ULM-PA OPERATIONS STAFF MD MUST CALL ULM-PA OPERATIONS STAFF EMERGENCY OVERRIDE OF DRUG THAT REQUIRES PA KELOID TREATMENT-ONLY FIRST DIAGNOSTIC VISIT IS PAID PROVIDER TYPE NOT AUTHORIZED TO PRESCRIBE MUST UTILIZE HMO SERVICES PRESCRIBER NUMBER NOT FOR INDIVIDUAL PRESCRIBER HMO EOB REQUIRES REVIEW SUBMIT JUSTIFICATION FOR SERVICES MSA CODE IS INVALID NOT HOSPICE ELIGIBLE CONFLICT W LEERS DATA. VERIFY INFORMATION ON BIRTH REC INVALID PRESCRIBER ID QUALIFIER MUST BE 01 OR 05 NUMBER OF PRESCRIPTIONS GREATER THAN LIMIT SEND DOCUMENT TO JUSTIFY PATH CONSULT USE OF 62/66 MOD INDICATED BY REPORT;RESUB &/OR ADJUST CANNOT ADJUST ZERO-PAID CLAIM FROM PRE-PAY RVW PROCESS EXACT DUP ERROR: ADULT DAY CARE AND LTC EXACT DUPE: IDENTICAL ADULT DAY CARE CLAIMS EXACT DUPE: HABILITATION AND HOSPITAL CLAIM DID NOT RECEIVE CLAIMCHECK EDITS SUBMIT TO RECIPIENTS SHARED PLAN SUBMIT TO RECIPIENTS PREPAID PLAN WAIVER SVC NOT PAYABLE WHILE IP MISSING/INVALID SERVICE PROVIDER ID QUALIFIER ONLY 1 OF THESE PROCS IN 7 YEARS PER RECIP/PROVIDER PROV ID NO ON CLAIM MUST MATCH PROV ID NO ON RECI FILE SUBMIT MEDICAL DOCUMENTATION TO JUSTIFY REPROGRAMMING HCPCS REQUIRED PRESCRIBING PROVIDER DOES NOT HAVE PRESCRIPTIVE AUTHORI OVERRIDE REQUIRED-SEND TO DENTAL PA UNIT PHARMACY CLAIM CANNOT BE REVERSED CLAIM MUST BE SUBMITTED IN KIDMED FORMAT CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 2 3 3 2 3 3 1 3 1 3 3 3 2 2 2 3 3 4 3 3 2 3 1 2 3 1 2 3 2 2 2 3 3 4 3 2 3 2 1 2 3 2 2 2 96 16 22 22 4 11 119 252 95 1 252 B5 B5 B5 15 15 15 B5 184 24 184 133 B9 16 96 252 16 119 252 4 B13 18 18 18 119 166 24 96 16 119 16 252 16 184 16 18 16 M80 M119 N517 N435 M29 N29 N517 N517 N517 M49 N30 N29 N31 N362 M29 N517 N522 N522 N522 N45 M2 N253 M86 N521 N29 M20 M76 N522 N34 216 001 001 001 453 454 294 300 566 483 294 054 626 048 048 046 048 103 25 139 025 046 021 021 084 287 577 483 311 453 021 054 054 054 020 132 114 249 745 483 021 287 021 025 123 743 483 216 287 216 219 216 441 490 087 101 050 080 050 507 743 021 732 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 12 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------518 519 520 521 522 523 524 525 526 527 528 529 530 531 532 533 534 535 536 537 538 539 540 541 542 543 544 545 CLMCHK-546 CLMCHK-547 CLMCHK-548 CLMCHK-549 550 551 552 553 CLMCHK-554 555 556 557 CLMCHK-558 559 560 561 562 563 CLMCHK-564 19:11:13 KIDMED INFO MISSING NEWBORN ZERO PD BILLED AMT MUST BE 0 USE INDIV PRESC NO MOTH/NEWBRN BILL SEP CANNOT BE ADJUSTED ELIG FOR PACE ONLY LOC NOT ON RECI FILE KATRINA EVACUE/CAT11 KATRINA EVACU/PARISH LACHIP AFFORDABLE EXCEEDS MAX DOSE SERVICE ALREADY PAID DG USE NOT WARRENTED OOS SRVC REQ APPRVL EXCEEDS MAX ER REVS PA APRVD PROC DELETD BILL MEDICARE PART D BILL MEDICARE PART B OBRA 90 EXCLUDED DRU REV MED NECESSITY CLAIM REQ DETAIL FP VISIT OVER MAX IP SERV NOT COV FP UNITS > DAILY MAX UNITS 33-47 CT NOT COV FP REV CODE INVALID NDC LINE ADDED-REB PROC REB REL TO CURR PROC REB REL TO HIST HST PROC VOIDED-REB NO MULTI - PROVIDERS PRE-PAY REVIEW 0-PAY SUSPCT DUPE 16 TO 02 SUSPCT DUPE 16 TO 16 DUPLICATE SERVICES SUBMIT CLAIM TO SMO ATND PRV NOT LNK BYU PRE-PAY REV OVERRIDE ASSIST SURG INVALID HOME LEAVE DAYS ADJ ALL BUT MAJ. NEED 51 ADJ SEC,51 AND 62/66 EDC ON 96 AND NOTES ADJ-ADD-ON-WITH-51 MAX SERVICE LIFETIME IMMUNIZATION AND SUSPECTED CONDITION INFO REQUIRED NEWBORN CLAIM ZERO PAID VACCINES FROM VFC AT NO COST-BILLED AMT MUST BE 0 PRESCRIBING PRVI BILLED IS GROUP USE INDIVIDUAL PRES NO MOTHER/NEWBORN MUST BE BILLED SEPARATE ADJUSTMENT IS INVALID, VOID AND REBILL CAPITATED-SERVICE MUST BE AUTHORIZE/PAID BY PACE PROVDR LEVEL OF CARE NOT ON RECIPIENT FILE HURRICAN KATRINA EVACUEE/AID CAT 11 HURRICANE KATRINA EVACUEE/PARISH LACHIP AFFORDABLE SUBMIT CLAIM TO BCBS EXCEEDS MAXIMUM DAILY DOSE RECIPIENT WAS REIMBURSED FOR THIS SERVICE DRUG USE NOT WARRENTED OUT OF STATE SERVICES REQUIRE DHH APPROVAL LETTER EXCEEDS MAXIMUM ER REVENUE CODES PER VISIT PRIOR AUTHORIZATION APPROVED PRIOR TO DELETION OF CODE BILL MEDICARE PART D BILL MEDICARE PART B OBRA 90 EXCUDED DRUG PAID BY MEDICAID REV DIAGNOSIS AND/OR ATTACHMENT FOR MEDICAL NECESSITY CLAIM REQUIRES DETAILED BILLING FP VISIT EXCEEDS ANNUAL MAXIMUM ALL OWED INPATIENT SERVICES ARE NOT COVERED BY THE FP PROGRAM UNITS EXCEED MAXIMUM DAILY ALLOWED LIMIT UNITS PAID BETWEEN 33 AND 47 CLAIM TYPE/FORMAT NOT COVERED BY THE FP PROGRAM REVENUE CODE INVALID FOR REPORTING NDC INFO CLAIM LINE ADDED AS A RESULT OF CLAIMCHECK REBUNDLING PROCEDURE REBUNDLED DUE TO CURRENT CLAIM/CLAIMCHECK PROCEDURE REBUNDLED DUE TO HISTORY CLAIM/CLAIMCHECK HISTORY PROC VOIDED DUE TO REBUNDLING/CLAIMCHECK MULTIPLE PROVIDERS WILL NOT BE PAID FOR THIS PROCEDURE ZERO PAID DUE TO PRE-PAYMENT REVIEW SUSPCT DUPE: ADULT DAY CARE AND LTC SUSPCT DUPE: IDENTICAL ADULT DAY CARE CLAIMS DUPLICATE UNILATERAL/BILATERAL SERVICE-CLAIMCHECK SUBMIT CLAIM TO LBHP SMO ATTENDING/SERVICING PROVIDER NOT LINKED TO BYU PLAN ALLOW ADJUST/VOID FOR PREPAY ZERO-PAID CLAIM ASSISTANT SURGEON INVALID FOR THIS PROCEDURE/CLAIMCHECK HOME LEAVE DAYS AT 75% CANNOT PAY MAJOR UNTIL SECONDARY IS PAID AT 50% ADJUST SECONDARY PROC WITH 51 MOD AND WITH 62 OR 66 LESS THAN 30 DAYS NEED EDC ON 96 AND RECORDS TO SUPPORT ADJ ADD-ON CODE WITH 51 MOD THEN REBILL PRIMARY PROC MAXIMUM SERVICES EXCEEDED-LIFETIME/CLAIMCHECK CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 1 3 2 2 3 2 4 2 3 3 3 3 3 3 3 3 3 3 3 3 2 3 3 3 3 3 2 3 4 4 3 2 3 2 2 2 4 3 3 3 3 2 1 2 3 252 128 16 16 96 16 24 16 119 119 22 153 119 50 197 119 96 22 22 23 133 107 119 96 119 119 96 199 59 97 97 59 18 96 18 18 18 24 185 216 54 119 59 4 252 4 35 N29 M79 N31 N15 N152 N54 N45 N45 N111 N180 N362 N448 M86 N30 N362 N45 N30 N522 N10 N522 N522 N522 MA67 N45 N517 N29 N517 021 102 178 132 238 001 094 021 001 001 114 483 065 001 001 483 021 171 171 216 287 021 483 227 612 104 227 021 012 012 012 012 676 20 054 054 054 317 455 724 446 048 507 279 626 084 626 084 455 054 20 154 001 001 001 001 530 521 483 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 13 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------CLMCHK-565 566 CLMCHK-567 568 569 570 571 572 CLMCHK-573 CLMCHK-574 575 576 577 578 CLMCHK-579 580 581 CLMCHK-582 CLMCHK-583 CLMCHK-584 CLMCHK-585 CLMCHK-586 CLMCHK-587 CLMCHK-588 CLMCHK-589 590 CLMCHK-591 CLMCHK-592 CLMCHK-593 CLMCHK-594 CLMCHK-595 CLMCHK-596 597 598 599 600 601 602 603 604 605 606 607 608 609 610 611 19:11:13 MAX SERVICE SAME DAY ADJ MAJOR WITH 62/66 INCIDENTAL PROC/CURR NOT LTC ELIGIBLE HOSP LEAVE DAY ADJ. ADJ. REL BUDGET CUTS NH OFFSET ER TRANSPORT OFFSET INCIDENTAL PROC/HIST HIST PROC VOIDED-INC MISS/INV DIAG CODE MISS/INVLD PA/MC COD OVERRIDE OF RX LIMIT INV POS/MOD COMBO MUTUALLY EXCLU-CURR ADJ INTO PAID LINE HURRICANE-REL WO ATT MUTUALLY EXCLU-HIST HIST PROC VOIDED-ME PROC/SEX CONFLICT PRE-OP PROC/CURR PRE-OP PROC/HIST HIST PROC VOIDED-PRE POST-OP PROC/CURR POST-OP PROC/HIST RECI IS MEDCARETCHOI HIST PROC VOIDED-PST E&M NOT PAYABLE/CURR E&M NOT PAYABLE/HIST HIST PROC VOIDED/VIS PROC SPL REL TO CURR LINE ADDED-SPL PA/CLM MOD NOT SAME PA TOOTH/CAV NQ CLM SONOS NOT JUSTIFIED TEMP PEND/NEW PROG ADULT DENTAL-UNDER21 SURFACE CODE CONF TOOTH/CAVITY CDE REQ EPSDT DENT AGE GR 21 OVER LMT PER PREG ADULT DENTAL REQ PA PA DATE GR SERV DATE SEAL.NOT PAY.TOOTH RESTOR NOT ALLOW-AGE NOT USED - AVAILABLE PULPOTOMY NO PAY-PER MAXIMUM SERVICES EXCEEDED SAME DAY/CLAIMCHECK ADJ MAJOR WITH 62 OR 66 THEN SECONDARY (S) WILL BE PAID PROCEDURE INCIDENTAL TO PROC ON CURR CLAIM-CLAIMCHECK NOT LTC ELIGIBLE HOSP LEAVE DAY ADJ. REL TO MEDICAID SPENDING RED PLAN ADJUSTMENT RELATED TO MEDICAID SPENDING REDUCTION PLAN NH OFFSET ADJ. REL TO M'CAID SPEND REDUCT PLAN $1.11 ER TRANSPORT OFFSET REL TO M'CAID SPEND RED PLAN PROCEDURE INCIDENTAL TO PROC IN HISTORY-CLAIMCHECK HISTORY PROC VOIDED-INCIDENTAL TO CURRENT/CLAIMCHECK MISSING OR INVALID DIAGNOSIS CODE MISSING OR INVALID PA/MC CODE OR NUMBER FOR RX OVERRIDE OVERRIDE OF MONTHLY PRESCRIPTION LIMIT INVALID PLACE OF SERVICE/PROCEDURE MODIFIER COMBINATION PROC MUTUALLY EXCLUSIVE TO ANOTHER CURR PROC/CLAIMCHECK COMBINE CHARGES AND ADJUST THIS LINE INTO THE PAID LINE HURRICANE RELATED CLAIMS ALLOWED TO PROCESS W/O ATTACHM PROCEDURE MUTUALLY EXCLUSIVE TO PAID PROC/CLAIMCHECK HIST PROC VOIDED-MUTUALLY EXCLUSIVE TO CURR/CLAIMCHECK PROCEDURE CODE/SEX CONFLICT-CLAIMCHECK PROCEDURE DENIED IN PRE-OP PERIOD-CURR/CLAIMCHECK PROCEDURE DENIED IN PRE-OP PERIOD-HIST/CLAIMCHECK HISTORY PROC VOIDED-PRE-OP PERIOD OF CURR/CLAIMCHECK PROCEDURE DENIED IN POST-OP PERIOD-CURR/CLAIMCHECK PROCEDURE DENIED IN POST-OP PERIOD-HIST/CLAIMCHECK RECIPIENT IS MEDICARETCHOICE HISTORY PROC VOIDED-POST-OP PERIOD OF CURR/CLAIMCHECK E&M CODE NOT PAYABLE SAME DAY-CURR/CLAIMCHECK E&M CODE NOT PAYABLE SAME DAY-HIST/CLAIMCHECK HISTORY PROC VOIDED-E&M NOT PAYABLE/CLAIMCHECK PROCEDURE SPLIT TO ALLOW PARTIAL PAYMENT/CLAIMCHECK CLAIM LINE ADDED AS A RESULT OF CLAIMCHECK SPLIT PA MODIFIER DOES NOT MATCH CLAIM MODIFIER PA TOOTH/ORAL CAVITY CODE NOT SAME AS CLAIM DOCUMENTATION DOES NOT JUSTIFY ADDITIONAL SONOGRAMS TEMPORARY PEND FOR NEW PROGRAM ADULT DENTAL CLAIM FILED FOR RECIP UNDER 21 CLAIM DOES NOT INDICATE CORRECT NUMBER OF SURFACES TOOTH CODE/ORAL CAVITY DESIGNATOR REQUIRED EPSDT DENTAL CLAIM - RECIPIENT AGE GREATER THAN 21 EXCEEDS LIMIT PER PREGNANCY ADULT DENTAL CLAIM MUST BE PRIOR AUTHORIZED PA DATE GREATER THAN SERVICE DATE SEALANT NOT PAYABLE FOR THIS TOOTH RESTORATION NOT ALLOWABLE DUE TO PATIENT AGE NOT USED - AVAILABLE PULPOTOMY NOT PAYABLE FOR PERMANENT TOOTH CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 2 3 3 3 3 3 3 3 3 2 2 3 3 3 4 1 3 3 3 4 4 4 4 4 3 4 4 4 4 4 4 2 2 3 3 2 2 3 3 2 3 2 3 3 3 119 4 59 96 96 96 96 96 59 59 16 16 119 5 231 97 252 231 231 7 97 97 97 97 97 22 97 97 97 97 97 97 4 15 50 133 6 16 16 6 119 15 198 16 6 96 96 N362 N517 N30 MA67 MA67 MA67 MA67 MA63 M62 N45 M77 M15 N29 N517 M144 M144 M144 M144 M144 M144 N20 N20 N20 N123 N123 N519 N517 N225 N129 N75 N37 N129 M86 N517 N351 N39 N129 N174 N174 483 530 465 187 001 001 001 001 465 465 255 322 483 249 465 042 020 465 465 474 454 454 454 454 454 085 454 187 187 187 258 258 453 084 284 040 089 240 244 089 483 252 642 244 475 107 NCCI = CODE USED FOR NCCI ONLY. 521 453 590 158 158 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 14 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------612 613 614 615 616 617 618 619 620 621 622 623 624 625 626 627 628 629 630 631 632 633 634 635 636 637 638 639 640 641 642 643 644 645 646 647 648 649 650 651 652 653 654 655 656 657 658 19:11:13 PIN NOT PAY THIS TOO INV TOOTH/CAVITY CDE HEMA.COMP/IND/BILLED REBIL W/APP PRIM CDE ONE PANEL/PREGNANCY PYMNT INCDL DELV FEE URINALYSIS NOT BILLE PAN & IND CODE/ PANE PAN & IND CODE/ PANE NEED OP/PATH/HISTORY EXACT DUPE 01 TO 03 EXCEEDS ONE PER YEAR THIS SERV NOT PAYABL MED NEC INSUFFICIENT SEND EPSDT REFERRAL SEND MED NECESSITY NEED EPSDT & MED NEC ALLOW 1 PER 8 YEARS DOC/FAILED RESTORATI EPSDT AGE ERROR NOT USED - AVAILABLE VOID COMPON,REBILL VOID REBILL HIGH COD HIGH CODE TRIAD PAID REBILL VISIT CODE SEE MED SERV MANUAL ONLY LO-LEVEL OFFICE MC-XOVER-NON-FINANCE EXCEEDS MAX,PHYS,YRS EXCEEDS MAX/HOSPITAL 1 CONSLT/PHYS/HOSP EXCEEDS DAY MAX VISI VISIT CODE PD/DOS NEW/EST PT CONFLICT EXCEEDS DAY MAX VISI RXNO USE GR THAN LIM DOC REQ CONCUR CARE PAY ADMIN ONLY PAY RED TO STATE MAX HOSP CUTBACK APPLIED SCH2 NARC NO REFILL NOT USED - AVAILABLE NEW PRESC OVER 10 DA REFILL OVER 6 MONTHS OVER MAX DURATION QTY OVER PROGRAM MAX PRIOR PAYMNT REDUCED PIN NOT PAYABLE FOR THIS TOOTH INVALID TOOTH CODE/ORAL CAVITY DESIGNATOR HEMATOLOGY COMPONENT/INDICE/PROFILE BILLED INCORRECTLY MUST BE BILLED WITH APPROPRITATE PRIMARY CODE ONLY ONE PRENATAL LAB PANEL PER PREGNANCY PAYMENT INCLUDED IN DELIVERY FEE URINEALYSIS BILLED INCORRECTLY BILLED PANEL AND INDIVIDUAL CODE WITHIN PANEL ONE URINALYSIS,PER PREGNANCY PAYABLE RESUBMIT WITH OPERATIVE AND PATH REPORTS AND HISTORY OUTPATIENT AND INPATIENT HOSPITAL SERVICES ON SAME DAY SEND DOCUMENTAION TO JUSTIFY MORE THAN ONE PER YEAR THIS CHIROPRACTIC SERVICE NO LONGER PAYABLE DOCUMENTATION OF MEDICAL NECESSITY INSUFFICIENT SEND EPSDT REFERRAL AND PROOF OF MEDICAL NECESSITY SEND PROOF OF MEDICAL NECESSITY AND EPSDT REFERRAL NEED EPSDT REFERRAL AND PROOF OF MEDICAL NECESSITY ONLY 1 OF THESE PROCES IN 8 YEARS PER RECIP/PROVIDER RESUBMIT WITH DOCUMENTATION OF PREV FAILED RESTORATION EPSDT AGE OVER 21 NOT USED - AVAILABLE VOID COMPONENTS, REBILL PANEL CODE VOID PAID CODE; REBILL HIGHER CODE IN TRIAD HIGHER CODE IN TRIAD ALREADY PAID CRITICAL CARE/CONSULT NOT DOCUMENTED-BILL CORRECT VISIT MATERNITY ANES. SEE PG. 10-5 OF MEDICAL SERVICES MANUAL ONLY LOW LEVEL OFF VISIT ALLOWED MEDICARE CROSSOVER ADJUSTMENT MON-FINANCIAL EXCEEDS MAXIMUM ALLOWED BY SAME PHYSICIAN W/I 3 YEARS EXCEEDS MAXIMUM ALLOWED PER HOSPITALIZATION ONLY 1 INITIAL CONSULT-SAME PHYS.PER HOSPITALIZATION EXCEEDS DAILY MAXIMUM ALLOWED VISITS VISIT CODE ALREADY PAID FOR THIS DATE OF SERVICE NEW/ESTABLISHED PATIENT CONFLICT EXCEEDS DAILY MAXIMUM VISITS PER PROVIDER/SPECIALTY USAGE OF SAME RX NUMBER GREATER THAN SYSTEM LIMIT RESUBMIT W/DOCUMENTATION SUBSTANTIATING CONCURRENT CARE ADMINISTRATION ONLY IS REIMBURSABLE PAYMENT MADE AT STATE MAXIMUM HOSPITAL CUTBACK APPLIED SCHEDULE 2 NARCOTIC CANNOT BE REFILLED NOT USED - AVAILABLE NEW PRESCRIPTION MUST BE FILLED WITHIN 10 DAYS REFILL MUST BE FILLED WITHIN 6 MONTHS EXCEEDS MAXIMUM DURATION OF THERAPY QUANTITY EXCEEDS PROGRAM MAXIMUM PRIOR PAYMENT REDUCED CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 2 3 2 3 3 3 3 3 1 3 1 3 3 3 3 3 3 1 3 2 4 4 4 2 3 2 3 3 3 3 3 3 3 3 3 1 3 3 3 3 0 3 3 3 3 2 96 16 B13 107 119 96 96 49 119 252 60 252 96 50 50 50 50 119 251 6 16 97 97 97 16 95 16 23 119 119 B14 119 B14 B16 119 B5 252 B20 96 96 154 29 29 29 119 154 4 N174 N37 M86 N20 M86 M86 M86 M29 N29 N30 N225 N225 N225 N225 M86 N464 N129 MA30 M15 M15 N20 N56 M51 M86 M86 M86 M86 M86 N362 N29 N381 N381 107 244 419 021 507 483 419 419 419 419 304 054 483 107 287 287 287 403 483 123 475 419 419 419 294 193 262 483 065 483 483 483 483 054 107 483 219 294 287 490 483 483 001 216 N30 N362 N517 216 701 216 701 352 483 453 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 15 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------659 660 661 662 663 664 665 666 667 668 669 670 671 672 673 674 675 676 677 678 679 680 681 682 683 684 685 686 687 688 689 690 691 692 693 694 695 696 697 698 699 700 701 702 703 704 705 19:11:13 REBIL W/ONE PRIM CDE RED TO MULTI-SRC MAX MEDICARE-COVERAGE PAY REDUCED BY COPAY NO ABORTION DONE 1 PAYABLE/180 DAYS RESUB HRDCPY ADJ/VOI CLAIM FROM BYU UHC CLAIM FROM BYU CHS NO HIST.INSULIN REQ. USE CODE W3340 VOID REBILL VISIT PAID. DO NOT REBILL SERVICE IN PD 77427 EVAL & MGT PD DOS DOCUMENT NAME CHANGE VACCINE/ADM CONFLICT PRIMARY CODE DENIED RESTORATIVE/SURG REQ GLOBAL CODE PD COMPONENT CODE PD ABORT PD MOTHER LIFE BLK 82/83 SRGN NAME 96A INCOMPLETE/INCOR 96A DATED AFTER HYST NEED EDC ON FORM 96 NEED SPECIFIC REPORT ADMIT HIST,PHY,DISCH USE 52 REDUCE SERVIC ICFMR RESPONSIBILITY MHR SERV PD THIS DOS PAYMENT IN SURG FEE REBILL SURGERY SEND TEST AND RESULT ADJUST PAID LINE DID NOT SUB REQ DOC HOSP DISCHARGE PAID PROBLEM CODE PD 2YRS EXCEEDS MAX DURATION CUTBACK-SERV 1 YEAR REPR DENIED 1 YEAR INCLD TOTAL OB CARE FOLLOW UP VS CHG NEW PT/EST PT CD CON SEPARATE CHGS EPIS. ER VISIT/INP HOS SER AID/RN/PT NO SAME DY REBILL.ONLY ONE PRIMARY VACCINE ADMIN CODE ALLOWED/DAY PAYMENT REDUCED TO MULTI-SOURCE MAXIMUM CLM VOID/ADJ BY STATE**RECIPIENT HAS MEDICARE COVERAGE PAYMENT REDUCED BY COPAY ABORTION NOT DONE-FETUS NOT ALIVE AT TIME OF PROCEDURE ONLY ONE (1) PAYABLE PER 180 DAYS MEDICARE ADJ/VOID;RESUBMIT HARDCOPY ADJ OR VOID CLAIM CLAIM SUBMITTED TO MOLINA BY BYU UHC (UNITED) CLAIM SUBMITTED TO MOLINA BY BYU CHS (COMMUNITY) NO PATIENT HISTORY OF INSULIN REQUIREMENTS REBILL USING CODE W3340 WITH APPROPRIATE MODIFER VOID PAID URINALYSIS REBILL VISIT INCLUDED IN PAID PRE/POSTNATAL CAREVISIT. DO NOT REBILL SERVICE INCLUDED IN PAID 77427 EVAL AND MGT CODE PAID FOR THIS DOS 96/96A--DOC.NAME CHANGE-PG28 PROF SERV 2000 TRAIN PACK VACC & ADM MUST PAY/AGREE;IF ONLY ONE PAYS TOTAL DENIES PAYABLE ONLY IF PRIMARY CODE IS PAID RESTORATIVE AND/OR SURGICAL SERVICE REQ ON SAME DOS GLOBAL CODE PD THIS DOS THIS RECIP COMPONENT CODE PD THIS DOS RECIP ABORTION PAID MOTHERS LIFE ENDANGERED NEED SURGEONS NAME IN BLOCK 82 OR 83 ON UB92 96A INCOMPLETE OR INCORRECT 96A DATED AFTER HYST-RESUB WITH EMERGENCY DOCUMENTATION NEED EDC ON 96-SIGNATURE LESS THAN 30 DAYS FROM TUBAL RESUBMIT WITH SPECIFIC RELATED REPORT RESUBMIT WITH ADMIT HISTORY,PHYSICAL,DISCHARGE SUMMARY RESUBMIT WITH 52 MODIFIER FOR REDUCED SERVICES ICFMR FACILITY IS REQUIRED TO PROVIDE THIS SERVICE MHR SERVICES ALREADY PAID FOR THIS DATE OF SERVICE PAYMENT INCLUDED IN SURGERY FEE VISIT PAID IN GSP.VOID VISIT;REBILL SURGERY VISUAL FIELD TEST AND RESULTS NEEDED FOR REVIEW ONLY A PAID LINE/THE CORRECT PAID LINE CAN BE ADJUSTED REQUESTED DOCUMENTS WERE NOT SUBMITTED ONE HOSPITAL DISCHARGE SERVICE PAID PER ADMISSION PROBLEM ORIENTED CODE PAID WITHIN 2 YEARS EXCEEDS MAX DURATION MD FAX OVERRIDE FORM 866-797-2329 CUTBACK-REPAIR MUST YIELD DENTURE SERVICEABLE FOR 1 YR REPAIR DENIED FOR 1 YR POST INSERTION INCLUDED IN FEE FOR TOTAL OB CARE. CONSULT FOLLOW-UP VISITS NOT ALLOWED. NEW PATIENT/ESTABLISHED PATIENT CODE CONFLICT EPISIOTOMY INCLUDED IN DELIVERY CHARGE ER VISIT ON DATE OF INP HOS SERVICES AIDE/RN/PT VISIT SAME DAY NOT ALLOWED/H.HEALTH CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 3 3 3 3 1 4 4 3 2 4 4 4 4 1 2 2 2 3 3 3 2 1 1 1 1 1 2 4 2 4 4 1 2 1 2 3 3 3 3 4 4 3 4 3 3 96 96 22 3 11 119 252 24 24 153 4 97 97 97 97 251 107 107 107 B15 B15 119 16 251 251 251 252 252 4 97 18 97 97 252 16 252 18 B5 35 B5 96 97 97 B16 97 96 96 N362 N381 M86 N29 N517 N20 M80 M80 M80 N28 N20 N20 N45 N261 N28 N28 N28 N29 N221 N517 M97 N522 M144 M80 M29 N152 N29 N522 M86 M144 M86 N19 N20 N20 216 631 101 001 106 001 291 483 001 279 373 001 001 012 012 012 001 216 104 454 419 419 001 125 294 471 294 304 308 453 107 054 107 107 398 001 095 107 107 352 483 107 039 107 107 107 107 107 NCCI = CODE USED FOR NCCI ONLY. 054 291 466 258 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 16 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------706 CLMCHK-707 708 709 CLMCHK-710 711 712 713 714 715 716 717 718 719 720 721 722 723 724 725 726 727 728 729 730 NCCI -731 732 733 734 735 736 737 738 739 740 741 742 743 744 745 746 747 748 749 750 751 752 19:11:13 SEPARATE NB CARE CHG RESUB W/MOD-50 1UNIT SEP.CHG.FETAL MONIT STERIL CONSENT VOID PD CLM-SUB W/50 SAME SPEC/SUBSP PAID INITIAL HOSP INPT PD MULTI-CHANN TEST SEP EXCEEDS DAILY MAX 2ND. VISIT SAME DAY PROC INCLUDED IN OV FOUND TWO PANEL CODE CODE INC FRAMES/LENS EMERG COMB XRAY ONLY TO BE BILLED BY PROV SUR ASST NOT NEEDED BILL EMERG OV/XRAY PROV RESPONSIBLE/SVC EXCEEDS MAX DOLLAR D&C/BIOP-CERVIX CRG MULTIPLE SURGERY EXCEEDS DAILY MAX BLOOD COMP + PANEL URINE COMP + PANEL 1 INP HSP VST PER DA CCI:INCIDENTAL-CURR ATTACH DETAIL.DESCR. 95165-90 DAYS EXCEEDS-MAX-UNITS-AL PREV PD ANES-SAME RE ATTACH DET.DESCR DX FEE IN SCREEN. FEE NOT CCM ELIGIBLE EXCEEDS-MAX-UNITS-AL 1-INTRAOCULAR-LEN-AL ONLY 1 PER YEAR/RECI ALLOW 1 PER 5 YEARS PREG EXCEEDED 13/PREG-158A NEEDED 1/PREG-158A NEEDED SAME ATTD PD IP CONS PROVIDE SPEC RADIONU 1 DEL.ALLOW. 6MTH.SP DEL HYST/STER CONFLI STERILIZATION INDIC HYST REQ ACK TL NEEDS OFS 96 FOLLOWUP NB CARE BILLED SEPARATELY BILATERAL-RESUBMIT WITH MODIFIER-50-ONE UNIT FETAL MONITORING INCLUDED IN DELIVERY FEE STERILIZATION CONSENT F0RM INCORRECT/ILLEGIBLE BILATERAL-VOID PAID CLAIM-RESUBMIT WITH MOD-50 ONE UNIT SAME SPECIALTY/SUBSPECIALTY PAID ON SAME DATE OF SERV ONE INITIAL HOSPITAL INPATIENT SERVICE PAID PER ADMISS PANEL AUTOMATED MULTICHANNEL TEST EXCEEDS DAILY SERVICE MAXIUM FOUND DUPLICATE VISIT SAME DAY PROCEDURE INCLUDED IN THE PHYSICIAN VISIT MAX ALLOW ONE PANEL A DAY/BILLING PROVIDER CD 00089 INCL FRAME&LENS-HIST INDIC COMP PMT EMERGENCY CAN BE COMBINED WITH X-RAY ONLY MUST BE BILLED BY PROVIDER OF SERVICE PROCEDURE DOES NOT WARRANT SURGICAL ASSIST EMERGENCY CANNOT BE COMBINED WITH CODES OTHER THAN XRAY PROVIDER RESPONSIBLE FOR THIS SERVICE EXCEEDS MAXIMUM DOLLAR AMOUNT PER TOOTH SEE CPT-CODE 57520 INCLUDES D&C/DO NOT BILL CODE 58120 MULTIPLE SURGERY-PENDED FOR REVIEW EXCEEDS DAILY SERVICE MAXIMUM BLOOD COMPONENT BILLED ALONG WITH PANEL CODE URINE COMPONENT BILLED ALONG WITH PANEL CODE ONE INP HOSP INITIAL/SUBSEQ CARE VISIT ALLOWED PER DAY CCI:PROCEDURE INCIDENTAL TO ANOTHER CURRENT PROCEDURE ATTACH DETAILED DESCRIPTION OF PROCEDURE 95165-90 DAYS RECIPIENT HAS EXCEEDED MAXIMUM ALLOWED SERVICES PER 6MO PREVIOUSLY PAID ANES.OR SUPERVISING ANES,SAME RECI/DOS ATTACH DETAILED DESCRIPTION OF DIAGNOSIS FEE INCLUDED IN SCREENING FEE RECIPIENT NOT ELIG FOR THIS SERVICE-ON DATE OF SERVICE RECIPIENT HAS EXCEEDED MAXIMUM ALLOWED SERVICES PER YR ONLY ONE PROCEDURE V2630,V2631,V2632 ALLOWED PER RECIP ONLY 1 D0120/D0272/D1110/D1120/D1203/D1204 PER YR/RECI ONLY 1 OF THESE PROCS ALLOWED IN 5 YEARS PER RECIP/PROV MAX PER PREGNANCY EXCEEDED 13 ALLOWED PER PREGNANCY; 158-A NEEDED FOR EXTENSION ONE ALLOWED/PREG.;158-A NEEDED FOR UNUSUAL SITUATIONS SAME ATTENDING PROV PAID INPT CONSULTATION SAME STAY RESUB W/SPECIFIC NUCLIDE/AMT USED PER PT/AMT PD/INVOICE ONLY 1 DELIVERY ALLOWED IN 6 MONTH SPAN DELIVERY BILLED AFTER HYSTERECTOMY/STERLIZ WAS DONE FOUND PROC. 2 X INDICATES STERILIZATION HYST REQ ACKNOWLEDGEMENT OR PROOF PREVIOUSLY STERILE STERILIZATION REQUIRES OFS FORM 96. CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 4 2 4 1 2 2 2 4 3 2 4 3 4 3 3 3 3 3 3 4 3 4 4 3 3 1 3 3 2 1 4 3 3 3 3 3 3 1 1 2 1 3 2 1 1 97 4 97 251 4 18 18 97 96 18 97 119 97 96 96 54 96 119 96 97 133 96 97 97 96 59 252 119 119 18 252 97 31 119 96 119 119 119 252 252 18 252 119 16 216 251 251 M86 N517 M144 N28 N517 N522 N522 N20 N20 N522 N122 M86 N20 M80 N32 M80 N362 N59 N122 N20 N122 N122 N20 N29 M86 M86 N522 N29 N20 M90 M86 M90 M86 M86 M42 N170 N522 N225 M86 MA66 N28 N28 238 107 046 107 107 419 483 054 107 054 107 107 487 414 107 106 483 107 046 483 419 419 483 001 306 483 483 107 123 012 109 483 483 483 483 483 483 483 107 001 483 451 001 107 421 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 17 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------753 754 755 756 757 758 NCCI -759 760 761 762 763 764 765 766 767 768 769 770 771 772 773 774 775 776 777 778 779 780 781 782 783 784 785 786 787 788 789 790 791 CLMCHK-792 793 794 CLMCHK-795 796 797 798 799 19:11:13 REBILL-DELIVERY RVW READMIT/DSCHG DX BILL AS ADJ/CNT STAY DOC/READMIT SAME DAY ADJ PD LINE 51 MOD FND DUP SERV SM DAY CCI:INCIDENTAL-HIST AIR TRNSPT REQS P/A SEND DATED OP REPORT SEND DATED NOTES CORRECT OFS 96 SEC 1 CORRECT OFS 96 SEC 2 CORRECT OFS 96 SEC 3 CORRECT OFS 96 SEC 4 OFS96 NONCORRECTABLE RESUB/CORRECT MOD REFERRED TO P.A. PERTINENT HIST/REQ SEND L & D RECORDS JUSTIFY/#UNITS IN TRANSPLANT FEE INC IN RELATED SERV PAY CUT SAME TOOTH ONGOING CM PRIOR TO ABORTION RAPE-PAID CIRCLE UNLISTED DESC PROC:EXTRCT NOT PAY REBILL CORRECT UNITS MODIFIER NOT CORRECT SEND DATED NOTES EXCEEDS SONOS/270DAY EXCEEDS MO LIMIT SERV REV/CHIRO CNSLT UNKNOWN ABBREVATION SEND ALL DOCUMENTS DAILY NOTES NEEDED ABORTION INCEST-PAID 3 HOSP VISIT SERV PD CODE CONFLICT CLM BYPASS CC EDITS PCA SERV LIMIT EXCEE INPT SER PD SAME ATT CLM BYPASS PAM EDITS ORIG/ADJ PROV DIFF DUP ADJ. RECORD HIST ALREADY ADJSTED NO ADJ HISTORY REBILL DELIVERY (DELIVERY-SURGERY) CODE & OFFICE VISIT PEND FOR REVIEW OF READMIT/DISCHARGE DIAGNOSIS THIS SHOULD BE BILLED AS ADJUST.FOR CNT STAY RESUBMIT WITH DOCUMENTATION OF DISC/READMIT SAME DATE ADJUST PAID LINE WITH 51 MODIFIER THEN RESUBMIT MAJOR FOUND DUPLICATE SERVICE SAME DAY CCI:PROCEDURE INCIDENTAL TO PROCEDURE IN HISTORY AIR TRANSPT CLAIMS REQUIRES STATE APPROVAL SEND DATED OPERATIVE REPORT FOR DATE BILLED SEND SPECIFIC DATED NOTES FOR EACH DATE BILLED OFS 96 CORRECTABLE ERROR IN SECTION 1 OFS 96 CORRECTABLE ERROR IN SECTION 2 OFS 96 CORRECTABLE ERROR IN SECTION 3 OFS 96 CORRECTABLE ERROR IN SECTION 4 OFS 96 ERROR IN 7 8 10 11 14 15-DO NOT RESUBMIT NO DOCUMENTATION FOR 62/66;CORRECT/RESUBMIT TO BE REVIEWED BY PRIOR AUTHORIZATION;DO NOT RESUBMIT RESUBMIT WITH PERTINENT HISTORY RESUBMIT WITH LABOR AND DELIVERY RECORDS SEND NOTES JUSTIFYING # OF UNITS BILLED INCLUDED IN GLOBAL FEE FOR TRANSPLANT INCLUDED IN RELATED SERVICE PAYMENT CUTBACK SAME TOOTH ONGOING CM PRIOR TO INITIAL CM ~ ABORTION DUE TO RAPE PAID CIRCLE UNLISTED CODE DESCRIPTION IN-OPERATIVE REPORT PROCEDURE ON EXTRACTED TOOTH NOT PAYABLE UNITS AVAILABLE FOR CODE--REBILL USING UNITS INAPPROPRIATE PROCEDURE CODE MODIFIER-REBILL EXCEEDS SONOGRAMS/PREGNANCY IN 270 DAYS JUSTIFY ADDITIONAL SONOGRAMS W PERTINENT DATED NOTES EXCEEDS MONTHLY LIMIT SERVICE LIMIT REVIEW BY CHIROPRACTIC CONSULTANT RESUBMIT WITH ABBREVATION LEGEND INADEQUATE DOCUMENTATION-SEE FEB 94 & AUG 93 UPDATES DAILY NOTES(TREATMENT,PROGRESS)NEEDED ABORTION DUE TO INCEST PAID 3 HOSPITAL INPATIENT SERV PAID FOR SAME DATE OF SERVICE BILLED CODE CONFLICTS WITH CODE ALREADY PAID CLAIM BYPASSED THE CLAIMCHECK EDITS PCA SERVICE LIMIT EXCEEDED INPT HOSP SERV PAID FOR SAME DOS TO SAME ATTENDING PROV CLAIM BYPASSED THE PAM EDITS/CLAIMCHECK ORIG/ADJ BILLING PROVIDER NUMBER DIFFERENT DUPLICATE ADJUSTMENT RECORDS ENTERED HISTORY RECORD ALREADY ADJUSTED NO HISTORY RECORD ON FILE FOR THIS ADJUSTMENT CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 2 1 2 2 3 2 1 1 1 1 1 1 1 1 3 1 1 1 4 4 3 3 3 1 2 2 2 3 1 3 1 1 1 3 3 3 4 3 2 4 2 2 2 2 96 133 16 251 4 18 59 15 252 252 251 251 251 251 251 252 96 252 252 252 97 97 96 B16 119 251 16 16 4 119 252 119 133 252 252 252 119 96 119 97 119 18 97 16 18 18 16 N61 N50 N222 N517 N522 N517 M29 N29 N28 N28 N28 N28 N28 N29 N10 N29 N29 N29 M144 M80 N59 N45 N233 N39 M53 N519 M86 N29 M86 N29 N29 N29 N45 N20 M86 N130 M86 N522 N130 N257 N522 N522 N152 238 046 001 294 001 054 483 048 298 297 021 021 021 021 021 294 046 406 294 297 012 012 054 451 291 306 451 476 453 483 294 483 046 001 021 297 001 107 483 065 483 107 065 521 054 521 035 NCCI = CODE USED FOR NCCI ONLY. 317 065 065 065 065 065 453 317 287 317 054 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 18 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------800 801 802 803 804 805 806 807 808 CLMCHK-809 810 811 812 813 814 815 816 817 818 819 CLMCHK-820 CLMCHK-821 822 823 CLMCHK-824 CLMCHK-825 826 827 828 CLMCHK-829 830 CLMCHK-831 832 833 CLMCHK-834 835 CLMCHK-836 837 838 839 840 CLMCHK-841 842 843 844 845 846 19:11:13 ON-LINE DUPE DENY EXACT DUPE 01 TO 01 EXACT DUPE 01 TO 14 EXACT DUPE 02 TO 02 EXACT DUPE 02 TO 14 EXACT DUPE 03 TO 03 EXACT DUPE 03 TO 05 EXACT DUPE 03 TO 06 EXACT DUPE 03 TO 07 CLAIMCHECK RESERVED EXACT DUPE 03 TO 09 EXACT DUPE 03 TO 13 EXACT DUPE 03 TO 15 EXACT DUPE 04 TO 04 EXACT DUPE 04 TO 15 EXACT DUPE 05 TO 05 EXACT DUPE 05 TO 06 EXACT DUPE 05 TO 07 EXACT DUPE 05 TO 08 EXACT DUPE 05 TO 09 CLAIMCHECK RESERVED CLAIMCHECK RESERVED EXACT DUPE 06 TO 06 EXACT DUPE 06 TO 07 CLAIMCHECK RESERVED CLAIMCHECK RESERVED EXACT DUPE 06 TO 13 EXACT DUPE 06-14 EXACT DUPE 07 TO 07 CLAIMCHECK RESERVED EXACT DUPE 07 TO 09 CLAIMCHECK RESERVED EXACT DUPE 07 TO 15 EXACT DUPE 08 TO 08 CLAIMCHECK RESERVED EXACT DUPE 08 TO 13 CLAIMCHECK RESERVED EXACT DUPE 09 TO 09 EXACT DUPE 09 TO 13 EXACT DUPE 09 TO 15 EXACT DUPE 10 TO 10 CLAIMCHECK RESERVED EXACT DUPE 11 TO 11 EXACT DUPE 12 TO 12 EXACT DUPE 13 TO 13 EXACT DUPE 04 TO 13 EXACT DUPE 14 TO 14 DUPLICATE OF PREVIOUSLY PAID CLAIM EXACT DUPLICATE ERROR: IDENTICAL HOSPITAL CLAIMS EXACT DUPLICATE ERROR: HOSPITAL AND TITLE18-INSTITUTION EXACT DUPLICATE ERROR: IDENTICAL LTC CLAIMS EXACT DUPLICATE ERROR: LTC AND TITLE18-INSTITUTIONAL EXACT DUPLICATE ERROR: IDENTICAL OUTPATIENT CLAIMS EXACT DUPLICATE ERROR: OUTPATIENT AND REHAB SERVICES EXACT DUPLICATE ERROR: OUTPATIENT AND HOME HEALTH EXACT DUPLICATE ERROR: OUTPATIENT AND AMBULANCE CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: OUTPATIENT AND DURABLE-EQUIPMENT EXACT DUPLICATE ERROR: OUTPATIENT AND EPSDT EXACT DUPLICATE ERROR: OUTPATIENT AND TITLE18 EXACT DUPLICATE ERROR: IDENTICAL PHYSICIAN CLAIMS EXACT DUPLICATE ERROR: PHYSICIAN AND TITLE18 EXACT DUPLICATE ERROR: IDENTICAL REHAB-SERVICES CLAIMS EXACT DUPLICATE ERROR: REHAB-SERVICES AND HOME HEALTH EXACT DUPLICATE ERROR: REHAB-SERVICES AND AMBULANCE EXACT DUPLICATE ERROR: REHAB-SERVICES AND NON-AMBULANCE EXACT DUPLICATE ERROR: REHAB-SERVICES AND DURABLE EQUIP CLAIMCHECK RESERVED CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: IDENTICAL HOME HEALTH CLAIMS EXACT DUPLICATE ERROR: HOME HEALTH AND AMBULANCE CLAIMCHECK RESERVED CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: HOME HEALTH AND EPSDT EXACT DUPE ERROR-HOME HEALTH & TITLE 18 EXACT DUPLICATE ERROR: IDENTICAL AMBULANCE CLAIMS CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: AMBULANCE AND DURABLE-EQUIP CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: AMBULANCE AND TITLE18 EXACT DUPLICATE ERROR: IDENTICAL NON-AMBULANCE CLAIMS CLAIMCHECK RESERVED EXACT DUPLICATE ERRORS: NON-AMBULANCE AND EPSDT CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: IDENTICAL DURABLE-EQUIP CLAIMS EXACT DUPLICATE ERROR: DURABLE-EQUIPMENT AND EPSDT EXACT DUPLICATE ERROR: DURABLE-EQUIPMENT AND TITLE18 EXACT DUPLICATE ERROR: IDENTICAL DENTAL-EPSDT CLAIMS CLAIMCHECK RESERVED EXACT DUPLICATE ERROR: IDENTICAL DENTAL-ADULT CLAIMS EXACT DUPLICATE ERROR: IDENTICAL PHARMACY CLAIMS EXACT DUPLICATE ERROR: IDENTICAL EPSDT CLAIMS EXACT DUPLICATE ERROR: PHYSICIAN AND EPSDT EXACT DUPLICATE ERROR: IDENTICAL TITLE18 INST CLAIMS CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 2 2 2 2 2 2 18 18 18 18 18 18 18 18 18 N522 N522 N522 N522 N522 N522 N522 N522 N522 054 054 054 054 054 054 054 054 054 2 2 2 2 2 2 2 2 2 2 18 18 18 18 18 18 18 18 18 18 N522 N522 N522 N522 N522 N522 N522 N522 N522 N522 054 054 054 054 054 054 054 054 054 054 2 2 18 18 N522 N522 054 054 2 2 2 18 18 18 N522 N522 N522 054 054 054 2 18 N522 054 2 2 18 18 N522 N522 054 054 2 18 N522 054 2 2 2 2 18 18 18 18 N522 N522 N522 N522 054 054 054 054 2 2 2 2 2 18 18 18 18 18 N522 N522 N522 N522 N522 054 054 054 054 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 19 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------847 848 849 850 851 852 853 854 855 856 857 858 859 860 861 862 863 864 865 866 867 868 869 870 871 872 873 874 875 876 877 878 879 880 881 882 883 884 885 886 887 888 889 890 891 892 893 19:11:13 EXACT DUPE 15 TO 15 EXACT DUPE 12 TO 15 PD SAME ATTEN/DIF BL UNSPECIF SUSPCT DUPE SUSPCT DUPE 01 TO 01 SUSPCT DUPE 01 TO 14 SUSPCT DUPE 02 TO 02 SUSPCT DUPE 02 TO 14 SUSPCT DUPE 03 TO 03 ONLY EXM&XRAY ON DOS SUSPCT DUPE 01 TO 06 NOT USED - AVAILABLE SUSPCT DUPE 03 TO 08 INVALID COB ID NOT USED - AVAILABLE SUSPCT DUPE 03 TO 15 SUSPCT DUPE 04 TO 04 SUSPCT DUPE 04 TO 15 SUSPCT DUPE 05 TO 05 SUSPCT DUPE 05 TO 06 SUSPCT DUPE 05 TO 07 SUSPCT DUPE 05 TO 08 SUSPCT DUPE 05 TO 09 NOT USED - AVAILABLE SUSPECT DUPE 05-14 SUSPCT DUPE 06 TO 06 SUSPCT DUPE 06 TO 07 SUSPCT DUPE 06 TO 08 NOT USED - AVAILABLE SUSPCT DUPE 06 TO 13 SUSPECT DUPE 06-14 SUSPCT DUPE 07 TO 07 SUSPCT DUPE 07 TO 08 NOT USED - AVAILABLE NOT USED - AVAILABLE SUSPCT DUPE 07 TO 15 SUSPCT DUPE 08 TO 08 SUSPCT DUPE 08 TO 09 SUSPCT DUPE 08 TO 13 NOT USED - AVAILABLE SUSPCT DUPE 09 TO 09 SUSPCT DUPE 09 TO 13 SUSPCT DUPE 09 TO 15 SUSPCT DUPE 10 TO 10 NOT USED - AVAILABLE SUSPCT DUPE 11 TO 11 SUSPCT DUPE 12 TO 12 EXACT DUPLICATE ERROR: IDENTICAL TITLE18 PROF CLAIMS EXACT DUPLICATE ERROR:IDENTICAL DRUG & PARTB MC CLAIMS ALREADY PAID SAME ATTENDING DIFFERENT BILLING PROVIDER SUSPECT DUPLICATE OF PREVIOUSLY PROCESSED CLAIM SUSPCT DUPLICATE ERROR: IDENTICAL HOSPITAL CLAIMS SUSPT DUPLICATE ERROR: HOSPITAL AND TITLE18 SUSPCT DUPLICATE ERROR: IDENTICAL LTC CLAIMS SUSPCT DUPLICATE ERROR LTC AND TITLE18-INSTITUTIONAL SUSPCT DUPLICATE ERROR: IDENTICAL OUTPATIENT CLAIMS ONLY EXAM&XRAY MAY BE ON SAME DOS AS FULL MOUTH DEBRIDE SUSPCT DUPLICATE ERROR: OUTPATIENT AND HOME-HEALTH NOT USED - AVAILABLE SUSPCT DUPLICATE ERROR: OUTPATIENT AND NON-AMBULANCE INVALID COB-1 ID COB-1 PAYER ID MUST BE PLAN ID NOT USED - AVAILABLE SUSPCT DUPLICATE ERROR: OUTPATIENT AND TITLE18-PROF SUSPCT DUPLICATE ERROR:IDENTICAL PHYSICIAN CLAIMS SUSPCT DUPLICATE ERROR: PHYSICIAN AND TITLE18-PROF SUSPEC DUPLICATE ERROR: IDENTICAL REHAB-SERVICES CLAIMS SUSPCT DUPLICATE ERROR: REHAB-SERVICES AND HOME HEALTH SUSPCT DUPLICATE ERROR: REHAB-SERVICES AND AMBULANCE SUSPCT DUPLICATE ERROR: REHAB-SERVICES AND NON-AMBULANC SUSPCT DUPLICATE ERROR: REHAB-SERVICES AND DME NOT USED - AVAILABLE SUSPECT DUPE ERROR-REHAB SERVICES & TITLE 18 SUSPCT DUPLICATE ERROR: IDENTICAL HOME HEALTH CLAIMS SUSPCT DUPLICATE ERROR: HOME HEALTH AND AMBULANCE SUSPCT DUPLICATE ERROR: HOME HEALTH AND NON-AMBULANCE NOT USED - AVAILABLE SUSPCT DUPLICATE ERROR: HOME HEALTH AND EPSDT SUSPECT DUPE ERROR-HOME HEALTH & TILE 18 SUSPCT DUPLICATE ERROR: IDENTICAL AMBULANCE CLAIMS SUSPCT DUPLICATE ERROR: AMBULANCE AND NON-AMBULANCE NOT USED - AVAILABLE NOT USED - AVAILABLE SUSPECT DUPLICATE ERROR: AMBULANCE AND TITLE18 SUSPECT DUPLICATE ERROR: IDENTICAL NON-AMBULANCE CLAIMS SUSPECT DUPLICATE ERROR: NON-AMBULANCE AND DME CLAIMS SUSPECT DUPLICATE ERROR: NON-AMBULANCE AND EPSDT CLAIMS NOT USED - AVAILABLE SUSPECT DUPLICATE ERROR: IDENTICAL DURABLE-EQUIP CLAIMS SUSPECT DUPLICATE ERROR: DURABLE-EQUIPMENT AND EPSDT SUSPECT DUPLICATE ERROR: DME AND TITLE18 CLAIMS SUSPECT DUPLICATE ERROR: IDENTICAL DENTAL-EPSDT CLAIMS NOT USED - AVAILABLE SUSPECT DUPLICATE ERROR: IDENTICAL DENTAL-ADULT CLAIMS SUSPECT DUPLICATE ERROR: IDENTICAL PHARMACY CLAIMS CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 2 2 2 2 2 2 3 3 18 18 18 18 18 18 18 18 18 96 96 N522 N522 N522 N522 N522 N522 N522 N522 N522 M80 N20 054 054 054 054 054 054 054 054 054 107 054 3 1 96 251 N20 N464 054 2 2 2 2 3 3 3 3 18 18 18 18 96 96 96 96 N522 N522 N522 N522 N20 N20 N20 N20 054 054 054 054 054 054 054 054 2 2 3 3 18 18 96 96 N522 N522 N20 N20 054 054 054 054 3 2 2 3 96 18 18 96 N20 N522 N522 N20 054 054 054 054 2 2 3 3 18 18 96 96 N522 N522 N20 N20 054 054 054 054 2 3 2 2 18 96 18 18 N522 N20 N522 N522 054 054 054 054 2 2 18 18 N522 N522 054 054 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 20 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------894 895 896 897 898 899 900 901 902 903 904 905 906 907 908 909 910 911 912 913 CLMCHK-914 915 916 917 918 919 920 CLMCHK-921 922 923 924 925 926 927 928 929 930 931 932 CLMCHK-933 CLMCHK-934 935 936 937 CLMCHK-938 939 940 19:11:13 SUSPCT DUPE 13 TO 13 SUSPCT DUPE 13 TO 15 SUSPCT DUPE 14 TO 14 SUSPCT DUPE 15 TO 15 EXACT DUPE SAME ICN SUSPCT DUPE 12 TO 15 LIFETIME LIMITS-ONE UNITS WERE CUTBACK LTC HOME LV OVER MAX NEEDS MANUAL CUTBACK SVC BEYOND TIME LIM LTC MED-LOA OVER 15 EXCEEDS MAX ALLOWED PHY/CLINIC OVER MAX HH VISITS OVER 50 LTC HOME LVD OVER 9 ICF-MR LIMIT OVER 45 HOSP DAYS OVER MAX PENICL INJ OVER 12 PHY/HOSP VIS OVER MX UNITS NOT=SVC DAY EMERG OP OVER 3 NON-EMER OP OVER 12 OVER LIFETIME LIMIT REDUCED BY TPL REDUCED BY SPENDDOWN OVER 5 REFILLS UNITS NOT=SITE MOD EOMB MUST ATTACH CHIROP E&M VISIT MAX EFF 11/5/10 NDC REQU SEND RECORDS FOR DOS NOT USED - AVAILABLE OFS FORMS MISSING PD PATIENT RESP AMT MCAID PD ALLOWABLE BILL ONE PROC.PER L DENIED PER TPL EOB BILL 3RD PARTY CARRI INVALID PROC/MOD MOD 51 REQ'D-ADDED BATCHED INCORRECTLY PROCESSING ERROR MC-CROSSOVER-ADJVOID MOD 51 INVAL-REMOVED CUTBACK PER SURS DENY TO BE REBILLED SUSPECT DUPLICATE ERROR: IDENTICAL EPSDT CLAIMS SUSPECT DUPLICATE ERROR: EPSDT AND TITLE18 CLAIMS SUSPECT DUPLICATE ERROR: IDENTICAL TITLE18-INST CLAIMS SUSPECT DUPLICATE ERROR: IDENTICAL TITLE18-PROF CLAIMS EXACT DUPE SAME ICN - DROPPED SUSPECT DUPLICATE ERROR:DRUG & PARTB MC CLAIMS ONLY 1 NEWBORN HOSPITAL CARE PER RECIPIENT ALLOWED SERVICE LIMITS EXCEEDED - PARTIAL/FULL CUTBACK APPLIED LTC LEAVE DAYS EXCEED LIMIT DAILY LIMITS EXCEEDED - MANUALLY APPLY PARTIAL PAYMENT SERVICE PERFORMED BEYOND REQUIRED TIME SPECIFICATIONS LTC LEAVE DAYS EXCEED LIMIT - 15 PER HOSPITAL STAY EXCEEDS MAMIMUM ALLOWED PHYSICIAN/CLINIC VISITS EXCEEDS ANNUAL MAXIMUM HOME HEALTH VISITS EXCEEDS ANNUAL MAXIMUM ALLOWED (50) LTC HOME LEAVE EXCEEDS ANNUAL MAXIMUM ALLOWED (9) ICF-MR HOME LEAVE EXCEEDS ANNUAL MAXIMUM ALLOWED (45) HOSPITAL DAYS EXCEED ANNUAL MAXIMUM ALLOWED PENICILLIN/BICILLIN INJCTNS EXCEED ANNUAL ALLOWED (12) PHYSICIAN HOSPITAL VISITS EXCEED ANNUAL MAXIMUM UNITS DO NOT MATCH DATES OF SERVICE/CLAIMCHECK EMERGENCY OUTPATIENT VISITS EXCEED ANNUAL MAXIMUM (3) NON-EMERGENCY OUTPATIENT VISITS EXCEED MAXIMUM (12) LIFETIME LIMITS FOR THIS SERVICE HAVE BEEN EXCEEDED MEDICAID ALLOWABLE AMOUNT REDUCED BY OTHER INSURANCE MEDICAID ALLOWABLE AMOUNT REDUCED BY RECIPIENT SPENDOWN MORE THAN 5 REFILLS PER PRESCRIPTION NOT REIMBURSABLE UNITS DO NOT MATCH SITE-SPECIFIC MODIFIER/CLAIMCHECK MEDICARE EOMB INVALID/OR MISSING. CHIROPRACTIC E & M VISIT MAX REACHED EFF 11/5/10 PAS FOR THIS HCPC REQUIRES CORRECT NDC CODE SEND OFFICE RECORDS FOR DATE OF SERVICE NOT USED - AVAILABLE OFS FORMS 158B & ACKNOWLEDGEMENT REQUIRED PAID PATIENT RESPONSIBILITY AMT PER THE EOB PRIMARY INS NON-COVERED SERVICE - MCAID ALLOWABLE PAID BILL ONE PROCEDURE PER LINE FOR EACH DATE OF SERVICE DENIED PER THE TPL EOB INFORMATION PLEASE BILL THIRD PARTY CARRIER FIRST INVALID PROCEDURE-MODIFIER COMBINATION/CLAIMCHECK MODIFIER 51 REQUIRED. ADDED TO CLAIM-CLAIMCHECK BATCHED INCORRECTLY/ RE-ENTER PROCESSING ERROR MEDICARE CROSSOVER ADJUSTMENT OR VOID MODIFIER 51 INVALID. REMOVED FROM CLAIM-CLAIMCHECK CUTBACK PER SURS GUIDELINES MEDICARE DENIED,IF COVERED BILL WITH PROVIDER EOB CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 2 2 2 2 2 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 2 3 3 3 3 3 3 2 1 3 2 1 2 1 3 3 2 3 2 2 2 3 3 3 2 3 2 18 18 18 18 18 96 119 119 96 119 119 96 119 119 119 96 96 119 119 119 16 119 119 35 23 178 119 4 251 119 16 252 18 251 23 23 16 23 16 4 4 B5 B5 23 4 96 16 N522 N522 N522 N522 N522 N20 M80 N45 N43 N362 N362 N43 M86 M86 M86 N43 N43 M86 M86 M86 N345 M86 M86 M86 N519 N4 M86 M119 N29 N522 N28 N63 MA92 N519 N517 N519 N35 MA04 054 054 054 054 054 054 483 483 483 483 483 483 483 483 483 483 483 483 483 483 476 483 483 483 550 450 517 483 476 286 483 218 294 287 001 107 65 001 107 171 453 453 021 684 021 481 065 453 001 001 NCCI = CODE USED FOR NCCI ONLY. LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 21 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------941 942 943 944 CLMCHK-945 946 CLMCHK-947 948 949 950 951 952 953 954 955 956 957 958 959 960 CLMCHK-961 CLMCHK-962 963 CLMCHK-964 965 966 CLMCHK-967 968 CLMCHK-969 970 971 972 973 974 975 976 CLMCHK-977 978 979 980 CLMCHK-981 NCCI -982 983 NCCI -984 985 986 987 19:11:13 DENIED PER SURS DENY, NOT TO REBILL SPEND DOWN FORM NOT PAID BY MEDICARE INVALID W/O PRIMARY SPLIT BILL FOR PART. MAX # CLM LINES EXC INC IN MAJ SUR PROC ANESTH TIME MISSING OPER & HIST REPT REQ DISCH DATE NOT COV INC IN OV/RELAT PROC JUSTIFY 22 MOD PROC INAPPROPRIATE PAID ACC TO MED REV PROC/DX AGE RESTRICT PROC/DIAG NO MED NEC DENY BY MED REVIEW RESUB SURGEONS CODE NEED-AUTH-AND-REPORT MOD -50 INVALID MAX SERVICE SAME DAY PROC./DIAG. DESP.REQ MOD 51 DOESN'T APPLY NOT COVERED BE HH CLAIM HARD COPY NEED INVALID W/O PRIMARY PROC/SERV REND CONF PP CARE INCL IN DEL INAPPROPRIATE CODE, MEDICARE CLAIM > 6MO MEDICARE PAID 100% NO SURGERY MODIFIER DIA CODE/DESC CONF FY COST SETTLED STAMPED SIGNATURE. PP PREVIOUSLY PAID CAL.PRICE IS ZERO CLAIM IN PROCESS INVALID ADJ REASON CLAIMCHECK RESERVED CCI:HIST VOIDED-INC SYS CALC NET TOTAL CCI:MUT EXCLUS-CURR REBILL-MOTHERS INFO REBILL-BABYS INFO DENIED TO REBILL/ADJ DENIED PER SURS GUIDELINES DENIED BY MEDICARE, NOT COVERED BY MEDICAID SPEND DOWN FORM 110MNP INVALID/MISSING NOT PAID BY MEDICARE ADD-ON PROCEDURE INVALID WITHOUT PRIMARY/CLAIMCHECK SPLIT BILL FOR PARTIAL ELIGIBILITY. MAX EXCEEDED FOR ADDED CLAIM LINES-RESUBMIT/CLAIMCHECK INCLUDED IN MAJOR SURGICAL PROCEDURE ANESTHESIA MINUTES INVALID OR MISSING ATTACH BOTH OPERATIVE AND HISTORY REPORT DATE OF DISCHARGE NOT COVERED INCLUDED IN OFFICE VISIT/RELATED PROCEDURE RESUBMIT WITH JUSTIFICATION FOR USE OF 22 MODIFIER INAPPROPRIATE PROCEDURE - SEE CPT FOR VALID CODE PAID ACCORDING TO MEDICAL REVIEW PROC/DX NOT COVERED FOR RECIPIENT THIS AGE PROCEDURE/DIAGNOSIS NOT MEDICALLY NECESSARY DENIED ACCORDING TO MED REVIEW GUIDELINES RESUBMIT CLAIM USING CODE SURGEON BILLED ATTACH BHSF AUTHORIZATION LETTER AND OPERATIVE REPORT MODIFIER -50 INVALID/CLAIMCHECK MAXIMUM SERVICES EXCEEDED SAME DAY/CLAIMCHECK PROCEDURE/DIAGNOSIS DESCRIPTION REQUIRED. MODIFIER 51 DOES NOT APPLY TO THIS PROC CODE-CLAIMCHECK SERVICE NOT COVERED BY HOME HEALTH PROGRAM SUBMIT HARD COPY OF CLAIM PROCEDURE INVALID W/O PRIMARY PD/CLAIMCHECK PROCEDURE CODE DOES NOT REFLECT SERVICES RENDERED PP CARE INCLUDED IN REIMBURSEMENT FOR DELIVERY/CLAIMCHK INAPPROPRIATE CODE, BILL LAB OR SPECIFIC HANDLING. CLAIM EXCEEDS FILLING LIMIT COIN/DEDUCT. ALLOWABLE AMOUNT PAID IN FULL BY MEDICARE CLAIM DESCRIPT INDICATES PROC CODE SHOULD HAVE MODIFIER DIAGNOSIS CODE/DESCRIPTION CONFLICT FISCAL YEAR COST SETTLED STAMPED SIGNATURE NOT ALLOWED. POSTPARTUM CARE PREVIOUSLY PAID-EXCEEDS MAX/CLAIMCHECK CALCULATED PRICING IS ZERO/CALL HELP DESK CLAIM IN PROCESS INVALID ADJUSTMENT REASON CLAIMCHECK RESERVED CCI:HISTORY PROCEDURE INCIDENTAL TO CURRENT-HIST VOIDED SYSTEM CALCULATED TOTAL - NET BILLED NOT IN BALANCE CCI:PROCEDURE MUTUALLY EXCLUSIVE TO ANOTHER CURRENT PRO REBILL UNDER MOTHERS NAME & MID NUMBER REBILL-BABYS MID & MOTHERS D/C DATE AS BABYS ADMIT DATE DENIED TO BE REBILLED ON ADJUSTMENT FORM. CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 3 2 3 3 3 3 4 2 1 3 4 1 2 3 3 3 3 2 2 2 3 1 2 3 1 3 2 3 2 3 3 2 2 3 2 3 2 3 3 2 3 3 3 2 96 96 16 23 59 200 B5 97 16 252 96 97 252 16 119 6 50 150 16 15 4 119 252 4 96 252 59 16 59 16 29 23 4 16 B13 16 59 133 133 16 59 59 16 231 128 96 16 N35 N425 N58 N19 N203 M29 N174 M80 N29 N56 N45 N129 N163 N56 N517 N519 N362 N29 N519 N174 N29 N56 N56 N517 MA63 MA70 MA69 M54 N15 N34 046 585 450 654 465 178 121 012 251 298 190 012 453 454 046 475 287 046 666 048 453 483 021 453 107 277 510 021 465 454 483 591 453 254 1 466 465 222 476 021 465 001 400 102 102 001 001 NCCI = CODE USED FOR NCCI ONLY. 088 298 255 065 632 507 521 065 LAM5M111 RUN: 01/28/15 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM REPORT NO: RF-0-77 DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING PAGE: 22 LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERROR CORE ADJ REMARK CODE SHORT DESCRIPTION LONG DESCRIPTION GRP RSN CODE CODE CLAIM STATUS ---------------------------------------------------------------------------------------------------------------------------------988 -989 990 991 NCCI -992 993 994 CLMCHK-995 996 997 998 999 NCCI 19:11:13 COVERED BY MEDICARE CCI:MUT EXCLUS-HIST 2 PROC SAME TOTH/DAY PROCEDURE IN PANEL CCI:HX VOIDED-MUT EX MID CORRECTED. DOCUMENT NOT LEGIBLE CLAIMCHECK RESERVED MC-PAYMENT-REDUCED COMP A-MODE ECHOENCH NOT USED - AVAILABLE ADMIN CORRECTION ITEM COVERED BY MEDICARE CCI:PROCEDURE MUTUALLY EXCLUSIVE TO PROCEDURE IN HISTOR EMERGENCY/DEFINITIVE NOT PAYABLE ON SAME TOOTH/SAME DAY PROCEDURE INCLUDED IN PANEL CCI:HISTORY PROC MUTUALLY EXCLUSIVE TO CURR-HIST VOIDED MID HAS BEEN CORRECTED/PLEASE UPDATE YOUR FILES. DOCUMENTS NOT LEGIBLE, PLEASE RESUBMIT RESERVED FOR CLAIMCHECK DEDUCTIBLE & OR CO-INSURANCE REDUCED TO MAX ALLOWABLE COMPLETE A-MODE ECHOENCHEPHALOGRAPHY-BILL HCPC Z9100 NOT USED - AVAILABLE ADMINISTRATIVE CORRECTION CLMCHK = CODE USED FOR CLAIMCHECK ONLY. 3 3 3 4 3 2 1 3 2 3 22 231 96 97 231 140 251 106 119 16 55 129 N20 N122 N205 N45 M20 171 510 054 419 510 153 021 107 483 305 MA67 NCCI = CODE USED FOR NCCI ONLY. 632 242 632 277 LAM5M111 RUN: 01/28/15 19:11:13 LOUISIANA MEDICAID MANAGEMENT INFORMATION SYSTEM DEPARTMENT OF HEALTH AND HOSPITALS - BUREAU OF HEALTH SERVICES - FINANCING SUMMARY REPORT OF ERRTXT CODES LA MEDICAID ERROR CODE/HIPAA ERROR CODE CROSSWALK ERR CODES = ZERO 001 CODES OBSOLETE 000 ERRTXT CODES READ 1,000 REPORT NO: RF-0-77 PAGE: 23
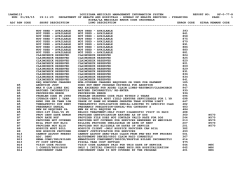




© Copyright 2026