
o - Blood
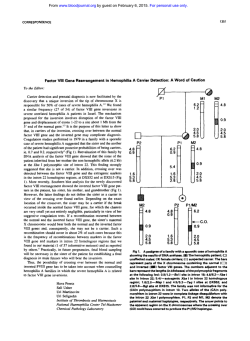
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Factor VI11 Gene Inversions in Severe Hemophilia A: Results of an International Consortium Study By S.E. Antonarakis, J.P. Rossiter, M. Young, J. Horst, P. de Moerloose, S.S. Sommer, R.P. Ketterling, H.H. Kazazian Jr, C. Negrier, C. Vinciguerra, J. Gitschier, M. Goossens, E. Girodon, N. Ghanem, F. Plassa, J.M. Lavergne, M. Vidaud, J.M. Costa, Y . Laurian, S.-W. Lin, S.-R. Lin, M.-C. Shen, D. Lillicrap, S.A.M. Taylor, S. Windsor, S.V. Valleix, K. Nafa, Y. Sultan, M . Delpech, C.L. Vnencak-Jones, J.A. Phillips 111, R.C.R. Ljung, E. Koumbarelis, A. Gialeraki, T. Mandalaki, P.V. Jenkins, P.W. Collins, K.J. Pasi, A. Goodeve, I. Peake, F.E. Preston, M . Schwartz, E. Scheibel, J. Ingerslev, D.N. Cooper, D.S.Millar, V.V. Kakkar, F. Giannelli, J.A. Naylor, E.F. Tizzano, M. Baiget, M. Domenech, C. Altisent, J. Tusell, M. Beneyto, J.I. Lorenzo, C. Gaucher, C. Mazurier, K. Peerlinck, G. Matthijs, J.J. Cassiman, J. Vermylen, P.G. Mori, M. Acquila, D. Caprino, and H. lnaba Twenty-two molecular diagnostic laboratories from 14 countries participatedin a consortium studyto estimate the impact of Factor Vlll gene inversions in severe hemophilia A. A total of2,093 patients with severehemophilia A were studied; of those, 740 (35%) had a type 1 (distal) factor Vi11 inversion, and 140 (7%) showed a type 2 (proximal) inversion. In 25 cases, the molecular analysis showed additional abnormal or polymorphic patterns. Ninety-eight percent of 532 mothers ofpatients with inversions were carriers ofthe abnormal factorVlll gene; when onlymothers of nonfamilial cases were studied, 9 de novo inversions in maternal germ cells were observed among 225 cases(m 1 de novomaternal origin of the inversion in 25mothersofsporadiccases). When the maternal grandparental origin was examined, the inversions occurred de novo in male germ cells in 69 cases and female germcells in l case.The presence of factor Vlll inversions is not a major predisposing factor for the development offactor VI11 inhibitors; however, slightly more patients with severe hemophilia A and factor Vlll inversions develop inhibitors (130of 642 [20%1) than patientswith severe hemophilia A without inversions (131 of 821 [16%1). 0 1995 by The American Society of Hematology. HEMOPHILIA and many mutations have been ~haracterized.~-~ Most of the mutations are private, ie, they have been found in one or only a fewunrelatedfamilies.Recently,acommoninversion of factor VlII gene was identified in many unrelated patients with severe hemophilia A.’,’ The inversion is mediatedby the presenceofthree copies of a particular DNA sequence (termed sequence A)’”’; one copy is located within intron 22 of the factor VIII gene’ and the other two are 4 0 0 kbtelomeric to the first.’”’3 Unequal crossing-over between two ofthese sequences results in inversion of a portion of the factor WI gene (exons 1 to 22) so that no intact factor VTII protein is produced. Cross-over between the most distal sequence A and its IVS22 homolog results in a type l inversion, apparently the mostcommoninversional e~ent.7.’~ Cross-overbetweenthe proximal extragenic sequenceA and its NS22 homolog results in a type 2 inversion. Both of these inversions can easily be diagnosed bySouthernblotanalysisusing a probe from the IVS22.7 It appears that there is also a polymorphism of the A sequencesthatlieoutside ofthe factor VIII gene, as some individuals have more than two copies ofthe extragenic sequence A.14The Southern blot diagnostic patterns of inversions in thesepatients are different from thoseof types 1 and2, termed here types 3A and 3B (Fig 1). In a recent study using DNA polymorphismanalysistodeterminethe origin of de novo inversions, the origin was almost always ~aternal.’~ The same study concluded that almost all mothers of patients with severe hemophilia A that was caused by factor Wr inversion were carriers of the in~ersion.’~ To determine the frequency of factor VI11 inversions in populations of severe hemophilia A patients, we collected data from a considerable number of hemophilia or molecular genetic diagnostic laboratories; this paper describes the results of these consortium DNA diagnostic studies for factor VI11 inversion mutations in hemophilia A. A, ONE OF THE most common coagulation disorders with an incidence of about 1 in 5,000 to 10,OOO males, is caused by mutations in the gene for coagulation factor VIII.’ This gene was cloned almost a decade agoz From the Geneva UniversityMedical School and CantonalHospital, Geneva, Switzerland; Johns Hopkins University School of Medicine, Baltimore, MD: University OfMiinster, Germany: Mayo Clinic, Rochester, MN; University of Pennsylvania, Philadelphia: Regional Hemophilia Center, Lyon, France; University of Lund, Malmo, Sweden; INSERM U91, Hdpital Henri Mondor, Crkteil, France: INSERM U143, Hdpital de Bic2treand Hdpital Ame‘ricain, Paris, France; National Taiwan University, Taipei, Taiwan; Queen ’S University, Kingston, Ontario, Canada; Hdpital Cochin, Paris, France; Vanderbilt University, Nashville, TN; Laikon Hospital, Athens, Greece; Tokyo Medical College, Japan; Royal Free Hospital and School of Medicine, London, UK; Royal HallamshireHospital, Shef jield, UK; Rigshospitalet, Copenhagen, Denmark: Skejby Hospital, Arhus, Denmark; Thrombosis Research Institute, London, UK; Guy’s Hospital, London, UK; HospitaldeSanPau, Barcelona, Spain: Hospital Val1d’Hebron, Barcelona, Spain; University Hospital La Fe, Valencia, Spain; Centre de Transfusion, Lille, France; University of Leuven, Belgium: University of California, San Francisco; Gianninn Gaslini Institute, Genova, Italy. Submitted February 24, 1995; accepted May 15, 1995. Supported by grants from the National Institutes of Health, the Swiss National Science Foundation, the Nationaaf Fonds voor Wetenschappelijk Onderzoek (Belgium), theSheffield University Research Stimulation grant (Sheffield, UK), the Swedish Medical Research Council, andthe Fondo de Investigaciones Sanilarias (Spain). Address reprint requests to Stylianos E. Antonarakis, Division de Ge‘nitique Medicale, Centre Medical Universitaire, l rueMichel Servet, 1211 Gedve, Switzerland. The publication costs of this article were defrayedin part by page charge payment. This article must therefore beherebymarked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8606-0025$3.00/0 2206 MATERIALS AND METHODS Each investigator contributed data to the first author’s laboratory via a data submission questionnaire. Included were the number of Blood, Vol 86, No 6 (September 15). 1995 pp 2206-2212 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2207 HEMOPHILIA A FACTOR Vlll INVERSIONS - a $ 8.m * 55 s3 ~ a ~ ~ a q m *9 q ~q *r . y~ q wq m - *" . *" q - t *" q wq - m! ~ m ~ ; ; ~ w s~ 5so N gm " Z * ; e l = 0:: ; ~ Q > $; ~ o ~ 8 0 +e 2 ~ ~ o 0 0 0 0 0 0 t - W 0 0 m u I O ~ ~ " c . " SE$ = ~ s s ~ s x ; e m c c r ~ ~ r - o o g:; ~ ~ a s N - c r a2 3 . L . U o ~ s gE? 5s g Q . . * y f N ~ ~ r~nwt - qmr mn m t q ~ r " ~ n rt nr mn m t f - vt )f mt *S mt +t U) 3 x W W N W ~ ~ % ~ : g: 9 .. & z e a w eP 2: 8 Q: ~ 3 ~ ~ - 0 k 5 s S- , O a " 0 0 ~ 0 0 0 0 0 0 m N 0 0 . - m 0 m 0 0 w 0 w 0 o r - ~ ~ g ~ 0 0 9 0 0 ~ 9 9 9 9 9 9 9 9 9 9 9 9 9 9 ' 9 E P ,o 0' k: : L .z._ 2 > g o o o o o c r 0 o - m o ~ o o m 0 ~ 0 0 ~ ~ ~ ~ ~ ~ 'EI !p t e -g ii 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 9 8.a F 2 2 81;:b o o o o o o ~ N O O r m o c u o o N O N O o N ~ = ~ ~ m 3 .S e g g c .. z g .h .. r m EI l- f ? ?k Sm S 'g - > 00 U. a .-m e LP E I m + > 4' ~ s s s s s a s 8 s s s 8 s s s s s s ~ i8s iEs:,o~ b m 3 8. w i d = L + m .c Q i? e 3 0 W- U)- .B m a l ?L+ m o o o o ~ ~ ~ o o o ~ ~ o zm 2Q o .E .z C$ o o - ~ o % ~ ~ o o ~ ~ P 2 2 Y 0 5 ab m ?? O O ~ ~ E z m 9c m z Cl N W O O O O ~ - ~ W O O ~ ~ O ~ O O * W N + > 9 r 9r 9r 9 9 9 9c 9r9 9 9r9 9c 9- 9 9 9 9 9 9 ~ .-S 9 r c c S S:$'-, g+ N +L z m t m N w c w * t - - m m t q * N r n t r n t ~ r n ~ q A - '2 U) 0P % + ~ ~ c- ~ 2 ~ 3 ~5 % % :S ~ ~ ~ ~ m ~ m W m m N N m N v ) m N v ) r W W ~ ..I h? 0 > 8.5 ~ ~ r 7o r ro r Nw 9 rwr V oN 9~ N ~ 7 ' 7 o Nw w * m v ) m m w 24 w0 0 ~ " ' 0 ' ~ ~ ~ ~ 0 p r , %er sf EW a ii ~ N t - N W . ~t N 9w ' : ~ .-m0 0 c' & b.i .-z s g " W ~ * N ~ " ~ ~ - N W w t n o ~ * m d t w * w t - m = E a 5 C D W O g m= & s 'c ~ o m w N ~ m ~ o T . &C > % z @ H & i s k2a N ~ .'E >' ~ w c 0 ~ ~ w 0 0 m - m c v ) ~ o o t - ~ ~ O ~ 0 2 Wc .= m ~ w 9 m w ~ m w ~ 9 w ~ ~ ? 20s2 f &2 y ;0 izg ~ x s ~ ~ ~ ~ s $ ? Em E= w r - ~ ~ w w o r N r o m c r m w o w ~ w m * v ) ".trn'Y.Nrnrnbrn*!tmV~Nrntrnmh!rntrn_, $ 1 ~ % r 0 ~ t m ~ 8 ~ ~ v ) ~ o w t - w wN w 8 ~ r ~ 4 t r ~ -~ ro r m - 8 o ~ R m r m o r o s w t - I P r- m m * " w r - w m ~ $ :3g a g~a i ~ bj k ~ ~ ~ ~ % $ c , 2 5 a C O ~ ,sS ~ + ~f . !Y$ - - !Q4 m E P ? ki t - * ~22gmc ~ " w m w ~ w, w ~ am . m o s ~ 2m-l c 9 c" cm ._ mO '5 E .- n 0, 0 0 .= ~ g @S m , > ~ 6 c C.: ~ c u p N - E-Pirj 8- -n P ;S ~ s s s s = ~ 6 s x ~ 6 8 8 s s 8 6 6P O s a= s~ ~ 8 8. v) = C P Dl- ~ ~ ~ ~ z ~ ~ From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2208 ANTONARAKIS ET AL WQe 2 Fig 1. Schematic representation of the mechanisms of the different factor Vlll gene inversions caused by intrachromosomalcrossing-over between homologous sequences A. The mechanisms of types 1 and 2 are as proposed.' The mechanisms of inversions 3A and 38 are t w o of several alternatives to explain the Southern blot patterns. The bottom of the figure schematically show the results of Southern blot analysis in the different types of factor Vlll inversions. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. HEMOPHILIA A FACTOR VI11 INVERSIONS 2209 Types of inversions of factor Vlll gene in severe hemophiliaA Fig 1. (Cont'd) unrelated patients with severe hemophilia A (factor VI11 activity less than I % of normal) studied by Southern blotting, the number of patients with each type of inversion, whether any inversion patient presented a mildhoderate phenotype, the number of mothers of inversion factor VI11 patients who were carriers either by pedigree or Southern blot analysis, the number of cases in which the origin of a de novo mutation was found, and the number of patients with severe hemophilia A with or without inversions that have developed factor VI11 inhibitors (antifactor VI11 antibodies). The diagnosis of the inversions in all laboratories was performed using Southern blot analysis as described.' Genomic DNA from patients with hemophilia A and members of their families was digested with Bcl I, the DNA fragments were electrophoresed on 0.7% agarose gels for 24 hours at SO V and transferred to nitrocellulose or nylon membranes. The membranes were probed with the 0.9-kb EcoRUSsr I fragment from plasmid p482.6' (American Type Culture Collection [ATCC] catalogue no. 57203). Earlier versions of the results from several laboratories have been published or presented in RESULTS AND DISCUSSION Twenty-two datasets from investigators in 14 countries are included in the study (Table 1). A total of 2,093 patients with severe hemophilia A have been studied by Southem blot for the presence of a factor VIII inversion. Because some laboratories havealso studied patients withmildmoderate hemophilia A,thetotalnumber ofpatient..studiedwas2,560. Table 1 shows the numberof patients with inversions ofthe factorVm gene. The DNA analysis showed 740 unrelated patients with a type 1 factor VIII inversion(35%ofpatientswithsevere hemophilia A studied, or 82% of the patients with inversions). This percentage varied from 25% of severe hemophiliacs in group 4 to 47% in thepatientsof group 2. There were 140 patients with a type 2 inversion of factor VITI, ie, 7% of those with severe hemophilia A or 15% of patients with inversions. This percentage varied from0% of severe hemophilia Ain the collection of patients of group 22 to 19% in those from group 20. Thus, the total number of unrelated patients with severe hemophilia A andeithertype 1 or type 2factor Vm gene inversion was 880 of 2,093, or 42%. This varied from 28%in the sample of group 4 to 53% in the sample of group 2. The overall frequency of 42% does not differ significantly from that reported in the original studies of Lakich et al? Naylor et al? &d Rossiter et al.?' Thus, the search for inversions of factor VIII should be considered as the first DNA diagnostic option in a patient or a family with severe hemophilia A. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. ANTONARAKIS ET 2210 Table 2. Hemophilia A, F8 Inversions Consortium-Origin of F8 Inversions Group Mother Carrier 54 1 53 2 17 18 4 18 519 (l 19 28 6 28 7 9 8 (0.98) 87 49 10 2 1 1 (1.00) 65 49 43 19 12 (0.98) 13 7 14 (0.82) 18 17 15 28 16 15 17 (0.94) 17 18 17 16 19 (1.00) 20 7 49 21 22 7 (0.98) 532 Total 523 Mother Tested Mother Mother Carrier Tested Mother Novo (% Carrier) De No-FH No-FH Familial 0.98) 1 ( 1 .OO) .OO) 9 89 2 65 44 7 22 17 28 16 17 17 7 49 15 7 MGF De Novo Novo 22 7 6 MGM De 1 19 (1.00) 9 9 ( 1 .OO) 2 2 (1.00) 14 5 8 2 10 2 3 3 2 1 3 6 4 7 2 ( 1 .OO) ( 1 .OO) 1 1 17 17 ( 1 .OO) 17 17 1 7 1 7 3 3 1 (1.00) ( 1 .OO) 15 (1.00) 34 4 A total of 25 patients had Southern blot patterns that differed both from normal and from type 1 or type 2 inversions, representing 1% of patients with severe hemophilia A analyzed. Ten of the 25 rare patterns belong to the type 3A or 3B categories (5 and 5, respectively); in the remaining 15 cases, the molecular basis of the Southern blot results has not yet been elucidated. These 15 cases may represent polymorphic (normal) variants or deletionshearrangements that involve intron 22 of the factor VI11 gene. Results were also provided on the number of carrier mothers of patients with factor VI11 inversion severe hemophilia A (Table 2). Based on family history and/or Southern blot analysis, 523 of 532 (98%) mothers were carriers of the inversion. This result confirms the earlier observation14 that almost all mothers of patients with severe hemophilia A that was caused by factor VIII inversions are carriers of the abnormal factor VI11 gene. A total of 255 of the 520 mothers were members of pedigrees with positive family history of hemophilia A, and therefore, the mothers were obligate carriers. There were 225 cases of inversion hemophilia A without family history in which the mothers were tested for carrier status by Southern blot analysis. In the 225 mothers, 216 (96%) were carriers of the factor VI11 inversions (Table 2). Therefore, it seems that in sporadic cases of hemophilia A, there is 1 new mutation in the mother’s germ cells (a mother who is not a carrier) in every 25 cases. The data on the origin of de novo factor VI11 inversions from the laboratory of group 14 in Malmo, Sweden, differ from these of all the other datasets. The inversion originated in 4 of 14 mothers of patients with sporadic, severe hemophilia A with factor VI11 inversion. These data have been carefully checked on a second sample from the respective families. 1 9 9 69 1 The origin of certain de novo inversions of factor VI11 in the grandparental generation has been studied by Southern blotting and by analysis of DNA polymorphisms within or near the factor VI11 gene. The data collected on the origin of inversion mutations do not represent a thorough study of all cases; it is rather an opportunistic study based on the availability of DNA samples from the necessary family members. The de novo factor VI11 inversion originated in the male germ cells (maternal grandfather) of 69 cases and in the female germ cells of one case (maternal grandmother). These results include the data of Rossiter et all4of 20 cases of grandparental origin. The grandmaternal origin from group 4 was obtained using an extragenic polymorphic marker (DXS52) for which the error rate in this determination is 1% to 5%. These data also concur with the earlier conclusion that the overwhelming majority of de novo mutations occur in male germ ~ e l 1 s .Because l~ the mean paternal age was not advanced in the study of Rossiter et al,I4 the hypothesis is that most de novo inversions occur in male meiosis. The presence of inhibitors in patients with severe hemophilia A with or without inversions is also reported by the majority of the groups. The inhibitor titres variedwidely among the groups. The frequency of inhibitors in the two categories of patients also varied widely among the different groups (Table 3). A total of 130 patients of 642 studied (20%) with factor VIII inversions had developed inhibitors. Similarly, 131 patients of 821 studied (16%) with severe hemophilia A without factor VI11 inversions had developed inhibitors. The difference is marginally statistically significant (x2 = 4.53; df = 1; P = .033). The odds ratio for developing inhibitors in severe hemophilia A according to the presence or absence of factor VI11 inversions is 1.34 (95% confidence interval, 1.02 to 1.75). Therefore, we con- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2211 HEMOPHILIA A FACTOR Vlll INVERSIONS Table 3. Hemophilia A, FS Inversions ConmtiumDevelopment of F8 lnhbitors Group Inv 1 2 3 4 6 7 9 10 11 12 13 14 15 17 18 19 20 21 22 Total Inh With Inv Total With 5 3 2 2 14 6 2 3 24 1 9 6 10 6 0 3 9 16 9 130 17 15 69 10 38 22 10 34 90 31 37 22 38 31 51 48 21 43 15 642 Inh Without (% Inh) Inv Inv (0.29) (0.20) (0.03) (0.20) (0.37) (0.27) (0.20) (0.09) (0.27) (0.03) (0.24) 10.27) (0.26) (0.19) (0.00) (0.06) (0.43) 10.37) (0.60) (0.20) Total Without l% Inh) 5 3 3 14 15 95 (0.36) (0.20) (0.03) 12 16 42 22 (0.29) 10.73) 4 20 5 8 5 19 1 3 7 6 9 5 131 68 107 35 64 27 81 36 53 62 26 59 15 82 1 (0.06) (0.19) (0.14) (0.13) (0.19) (0.23) (0.03) (0.06) (0.11) (0.23) (0.15) (0.33) (0.16) Abbreviations: Inh, inhibitors; Inv, inversion. clude that the presence of factor VI11 gene inversion is not a major predisposing factor for the development of inhibitors. The results presented here suffer from the limitations of studies based on questionnaires. The Southern blot analyses were performed in different laboratories with slightly different methodologies; no exchange of samples was done to perform interlaboratory quality assessment. In addition, in the data reported on inhibitors, no attempt was made to distinguish high versus low titer, or transient versus longterm inhibitors. In summary, the results from the analysis of 2,093 severe hemophilia A patients in the consortium study of factor WI inversions indicate that (1) the type 1 inversion accounts for 35% and the type 2 inversion accounts for 7% of cases with severe hemophilia A , (2) in about 1% of cases of severe hemophilia A, rare Southern blot patterns are found (types 3A and 3B and other variants); (3) because of inversion, =98% of mothers of severe hemophilia A patients are carriers of the mutant factor VIII gene and, among mothers of sporadic cases, the frequency of carriers is 96%; (4) the majority of the de novo inversion mutation occurs in male germ cells; and (5) the presence of factor VIII inversions is not a major predisposing factor for the development of factor VIII inhibitors. ACKNOWLEDGMENT We thank H. Hanabusa, T. Nagao, M.A. Moms, P. Hutter for their contributions to the data collection. REFERENCES 1. Hoyer LW: Hemophilia A. N Engl J Med 33038, 1994 2. Gitschier J, Goralka TM, Wion KL, Chen EY, Eaton DE, Vehar GA, Capon DJ, Lawn RM: Characterization of the human factor VIII gene. Nature 312326, 1984 3. Antonarakis SE, Kazazian HH Jr, Tuddenham EGD: Molecular etiology of factor VIII deficiency in hemophilia A. Hum Mutat 5:1, 1995 4. Higuchi M,Antonarakis SE, Kasch L, Oldenburg J, EconomowPetersen E, Olek K, Inaba H, Kazazian HH: Towards a complete characterization of mild to moderate hemophilia A: Detection of the molecular defect in 25 of 29 patients by denaturing gradient gel electrophoresis. Proc Natl Acad Sci USA 88:8307, 1991 5 . Higuchi M, Kazazian HH, Kasch L, Warren TC, McGinniss M, Phillips JA, Kasper C, Janco R, Antonarakis S E Molecular characterization of severe hemophilia A suggests that about half the mutations are not within the coding region and splice junctions of the factor VI11 gene. Proc Natl Acad Sci USA 88:7405, 1991 6. Naylor JA, Green PM, Rizza CR, Gianelli F Analysis of factor WLI mRNA reveals defects in every one of 28 hemophilia A patients. Hum Mol Genet 2:11, 1993 7. Lakich D, Kazazian HH, Antonarakis SE, Gitschier J: Inversions disrupting the factor VIII gene as a common cause of severe hemophilia A. Nature Genet 5:236, 1993 8. Naylor JA, Brinke A, Hassock S , Green PM, Giannelli F: Characteristic mRNA abnormality found in half the patients with severe hemophilia A is due to large DNA inversions. Hum Mol Genet 2:1773, 1993 9. Levinson B, Kenwrick S , Lakich D, Hammonds G, Gitschier J: A transcribed gene in an intron of the human factor VIII gene. Genomics 7:1, 1990 10. Levinson B, Bermingham J R , Metzenberg A, Kenwrick S, Chapman V, Gitschier J: Sequence of the human factor VIII-associated gene is conserved in mouse. Genomics 13:862, 1992 11. Levinson B, Kenwrick S , Game1 P, Fisher K, Gitschier J: Evidence for a third transcript from the human factor V m gene. Genomics 14585, 1992 12. Freije D, Schlessinger D: A 1.6-Mb contig of yeast artificial chromosomes around the human factor VIII gene reveals three regions homologous to probes for the DXSl15 locus and two for the DXYS64 locus. Am J Hum Genet. 5 1 5 6 , 1992 13. Palmieri G, Romano G, Ciccodicola A, Casamassimi A, Campanile C , Esposito T, Cappa V, Lania A, Johnson S , Reinbold R, Poustka A, Schlessinger D, Durso M: YAC Contig organization and CpG island analysis in Xq28. Genomics 24: 149, 1994 14. Rossiter JP, Young M, Kimberland ML, Hutter P, Ketterling RP, Gitschier J, Horst J, Moms MA, Schaid DJ, deMoerloose P, Sommer S S , Kazazian HH, Antonarakis SE: Factor WI gene inversions causing severe hemophilia A originate almost exclusively in male germ cells. Hum Mol Genet 3:1035, 1994 15. Ljung RCR: Intron 22 inversions and haemophilia. Lancet 343:791, 1994 16. Tizzano EF, Domenech M, Altisent C, Tusell J, Baiget M: Inversions in the factor VIII gene in Spanish hemophilia A patients. Blood 83:3826, 1994 17. Tizzano EF, Altisent C, Tusell J, Domenech M, Baiget M: Intron 22 inversions and haemophilia. Lancet 343:792, 1994 18. Millar DS,Kakkar VV, Cooper DN: Screening for inversions in the factor VIII (F8) gene causing severe haemophilia A. Blood Coag Fibrinol. 5239, 1994 19. Windsor S , Taylor SAM, Lillicrap D: Direct detection of a common inversion mutation in the genetic diagnosis of severe hemophilia A. Blood 84:2202, 1994 20. Jenkins PV, Collins PW, Goldman E, Mccraw A, Riddell A, Lee CA, Pasi KJ: Analysis of intron 22 inversions of the factor VIII gene in severe hemophilia A-Implications for genetic counseling. Blood 84:2197, 1994 21. Goodeve AC, Preston FE, Peake R:Factor VI11 gene re- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 2212 arrangements in patients with severe haemophilia A. Lancet 343:329, 1994 22. Inaha H, Shibata H, Yoshida S , Hagiwara T, Hanahusa H, Nagao T, Fukutake K: Inversion in Japanese patients with hemophilia A. Thromb Haemost 1995 (in press) 23. Van de Water NS, Williams R, Nelson J, Browett PJ: Inversions of the factor VI11 gene in severe hemophilia A. Blood 84:62a, 1994 (abstr, suppl 1) 24. Acquila M, Caprin0 D, Binocchi P, Mori MP: New tool in the carrier detection and prenatal diagnosis of hemophilia A. Blood 84:62a, 1994 (abstr, suppl 1) ANTONARAKIS ET AL 25. Vnencak-Jones CL, Phillips JA 111, Janco RL, Cohen MP, Kazazian HH Jr, Rossiter J P Analysis of factor VI11 gene intrachromosomal inversions in 166 unrelated hemophilia A families. Blood 84:239a, 1994 (abstr, suppl 1) 26. Gaucher C, Mazurier C: Characterization of factor VI11 gene inversions using a non-radioactive detection method: A survey of 102 unrelated hemophilia A patients from Northern France. Nouv Rev Fr Hematol 37:131, 1995 27. Figueiredo MS, Tavella MH, Simoes BP: Large DNA inversions, deletions, and TaqI site mutations in severe hemophilia A. Hum Genet 94:473, 1994 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1995 86: 2206-2212 Factor VIII gene inversions in severe hemophilia A: results of an international consortium study SE Antonarakis, JP Rossiter, M Young, J Horst, P de Moerloose, SS Sommer, RP Ketterling, HH Jr Kazazian, C Negrier and C Vinciguerra Updated information and services can be found at: http://www.bloodjournal.org/content/86/6/2206.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.
© Copyright 2026