
1 ¿Por qué es importante clasificar los ictus? ¿Cómo los podemos
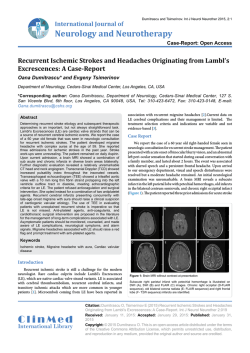
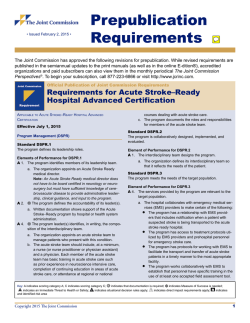
Ictus isquémico PROGRAMA DE FORMACIÓ CONTINUADA EN RADIODIAGNÒSTIC CURS BASIC Curs 2012‐2013 Clasificación radiológica de los infartos cerebrales. g Topografía y etiología. ¾87% de todos los ictus ¾Incrementa el riesgo: 9Recurrencias 9Enfermedad coronaria 9Enfermedad vascular periférica Àlex Rovira Cañellas Unitat RM. Servei de Radiologia Hospital Vall d’Hebron Barcelona. ¾Medidas de prevención secundaria necesarias alex.rovira@idi‐cat.org ¿Por qué es importante clasificar los ictus? ¾Seleccionar estrategia terapéutica en fase aguda ¾Establecer terapias de prevención secundaria ¾Riesgo de recurrencias, pronóstico ¾Indicación pruebas diagnósticas ¾Selección para ensayos clínicos ¾Comparación de cohortes Clasificación precisa y precoz ¿Cómo los podemos clasificar? ¾Perfiles de riesgo ¾Hallazgos clínicos ¾Marcadores biológicos, genéticos ¾P b di ó ti ¾Pruebas diagnósticas 9EKG 9Doppler 9Ecocardiografía 9TC: simple y avanzada 9RM: convencional y avanzada 9Angiografía por sustracción digital 1 Oxfordshire Community Oxfordshire Community Stroke Project (topografía y extensión) •Basado en signos y síntomas clínicos •Predice pronóstico •Buena correlación con los hallazgos radiológicos (TC) TOAST (Trial of rial of O ORG 10172 in RG 10172 in A Acute Stroke Treatment reatment)) Guias desarrolladas por clasificar prospectivamente los infartos en función de su mecanismo de origen 9Perfiles de riesgo: edad, diabetes, colesterol, HTA 9Hallazgos clínicos 9Pruebas paraclínicas: cerebrales, vasos, corazón 1. Total anterior circulation infarcts (TACI) 15‐17% f ( ) 1 Enf. de gran vaso (15‐20%) 1. Enf de gran vaso (15 20%) 2. Partial anterior circulation infarcts (PACI) 35% 2. Enf. de pequeño vaso (25%) 3. Lacunar infarcts (LACI) 25% 3. Cardioembolismo (15‐27%) 4. Posterior circulation infarcts (POCI) 25% 4. Otras etiologías (2%) (vasculitis, disección arterial,…) 5. Indeterminados o etiologías múltiples (~35%) •No predice mecanismo de infarto •Fácil de implementar en urgencias 9Precisión depende de la extensión y calidad de pruebas paraclínicas realizadas Bamford et al. Lancet 1991 Clasificación infartos basado en estudios NRx Clasificación infartos basado en estudios NRx Topografía Adams et al. Stroke 1993 Infartos territoriales anteriores Masivos Parciales 1. Infartos territoriales circulación anterior 2. Infartos territoriales circulación posterior ¾Infartos masivos 3. Infartos lacunares Afectan al menos 2 de los 3 territorios silvianos Elevada frecuencia de progresión clínica Elevada mortalidad 4. Infartos centro oval 5. Infartos frontera Mecanismo causal: TC/RM + estudio vascular Lee et al. Stroke 2000 2 Infartos territoriales anteriores ¾Infartos masivos: mecanismo causal ¾Infartos masivos: Infarto MALIGNO 9Cardioembolismo 9Oclusión ACI 9Disección ACI Infarto completo o casi completo de la ACM 10% de todos los infartos Deterioro clínico a los 2‐5 días 80% mortalidad C i t í d Craniotomía decompresiva reduce mortalidad i d t lid d Vahedi et al. Lancet Neurol 2007 Cardioembolismo Oclusión ACI – Enf. gran vaso Hemicraniectomía en infartos malignos ACM Seguimiento UCI Hemicraniectomia si: Desviación > 5 mm y/o PIC > 20 mmHg Desviación ≥ 5mm Hemicraniectomia Pooled analysis of DECIMAL, DESTINY, HAMLET clinical trials Tras cirugía descompresiva la probabilidad de supervivencia aumenta del 28% a casi el 80% y la probabilidad de alcanzar un mRS ≤3 se dobla. basal 24 h 48 h 48 h 6 d Vahedi et al. Lancet Neurol 2007 3 ¾Infartos masivos Infartos territoriales anteriores ¾Infartos parciales ¾Infartos parciales Afectan sólo 1 de los 3 territorios silvianos Baja frecuencia de progresión clínica Baja mortalidad Origen: g 9Cardioembolismo y ateroesclerosis de gran vaso Infartos arteria cerebral anterior Infartos arteria cerebral anterior ¾Baja incidencia: ~1% de ictus isquémicos 9% bilaterales 4% completos 9A 9Ateroesclerosis l i gran vaso: 73% Enfermedad ACA Enfermedad ACI Ambas 9Cardioembolismo: 10% 9Indeterminado: 15% Embolismo A-A Oclusión proximal Oclusión rama Kang et al. Neurology 2008 Kang et al. Neurology 2008 4 Infartos agudos múltiples multiterritoriales (AMBI) Infartos arteria cerebral anterior Circ. anterior / un hemisferio 44% Cardioembolismo oesclerótica gran vaso Enf. atero ¾Alta incidencia de disecciones (43%): causa más frecuente de infarto aislado de la ACAnt (jóvenes) (Sato et al. Cerebrovasc Dis 2009) Circ. anterior / ambos hemisfer. 21% Embolismo A‐A Circ. Posterior 23% 4. Cardioembolismo Enf. pequeño vaso Aumento fibrinógeno o hematocrito; microangiopatía trombótica Variantes anatómicas circ. anterior Cardioembolismo Cardíaco Arco aórtico Embolismo Circ. Anterior y posterior 12% 1. 2. 3. 1. 2. Ateroesclerosis gran vaso A Com Post persistente; ACP fetal Jae‐Kyu Roh et al. Stroke 2000 Infartos circulación posterior Infartos territoriales posteriores Distal Medio Proximal PICA AICA ACS ACP Caplan LR. et al. Ann Neurol 2004 5 Infartos circulación posterior Infartos circulación posterior: proximal Distal Embolismo 40 35 Proximal Hemodinámico 30 25 Medio 20 Oclusión rama 15 10 5 0 > 2/3 Ateroesclerosis de gran vaso (sistema vertebro basilar intra y extracraneal) Hemodinámico Embolismo arterio‐arterial cardíaco arterial Caplan LR. et al. Ann Neurol 2004 Caplan LR. et al. Ann Neurol 2004 Infartos territoriales de circulación posterior Mecanismos ictus (Caplan, 1996; Glass 2002) Mecanismos causales (Caplan, 1996; Glass 2002) ¾Enfermedad oclusiva de gran vaso – oclusion ramas: disección arteria vertebral ¾Enf. oclusiva de ramas arteriales Arterias circunferenciales 29% de infartos latero‐bulbares secundarios a disección de la AV Kameda et al. Stroke 2004 Arterias perforantes cortas largas 6 Infartos paramedianos pontinos Enf de gran vaso Lesión rama con origen en a. basilar Enf. de pequeño vaso Cardioembolismo El sistema arterial perforante El sistema arterial perforante Oclusión proximal de una arteria perforante A. Coroidea anterior (AChoA) A. lenticuloestriadas (ACM) A. lenticuloestriadas (ACA) A. de Heubner (ACA) A. talamoperforantes (ACP) Enf. pequeño vaso Erro et al. Eur J Neurol 2005 Erro et al. Eur J Neurol 2005 Cortesía Dr. Hendriksen. 7T Infartos lacunares Infartos lacunares El sistema arterial perforante El sistema arterial perforante A. Coroidea anterior (AChoA) A. lenticuloestriadas (ACM) •Infartos pequeños (<1.5cm) por oclusión/lesión de una arteria perforante única con origen en el polígono de Willis o de la arteria basilar •Corresponden al 11‐25% de ictus isquémicos •La mayoría son asintomáticos •Solitarios o múltiples •Mecanismo causal variable: enf. de pequeño vaso (75%) A. lenticuloestriadas (ACA) A. talamoperforantes (ACP) A. de Heubner (ACA) 9Ateroesclerosis 9C di 9Cardioembolismo b li 9Disección arterial 9Trombosis local (estados hipercoag.) Micheli et al. J Neurol 2008 7 Infartos lacunares Infartos lacunares grandes (únicos) Infartos lacunares Infartos lacunares pequeños (múltiples) Arteriopatía no ateroesclerótica •Microateromatosis •Oclusión proximal de una arteria perforante grande •Frecuentemente sintomáticos •No asociados siempre a hipertensión arterial •Sin lesiones isquémicas/hemorrágicas crónica asociadas (TC/RM) •Lesión destructiva de arterias penetrantes pequeñas (<200μm). Lipohialinosis •Frecuentemente asintomáticos •Asociados a hipertensión arterial crónica, DM, hematocritos altos •Con lesiones isquémicas/hemorrágicas crónica asociadas •Elevada El d tasa t d recurrencias de i (24.3% (24 3% vs 7.7%), 7 7%) peor pronóstico ó ti Arauz et al. Stroke 2003 Jackson et al. Stroke 2010 Infartos subcorticales pequeños (<20mm) y únicos Infartos subcorticales pequeños y únicos Arterias perforantes Arterias perforantes ACM Arterias perforantes Arterias perforantes ACM Nah et al. Stroke 2010 Distal Proximal sin lesión vascular Distal sin lesión vascular Proximal sin lesión vascular Proximal con lesión vascular Proximal con lesión vascular Nah et al. Stroke 2010 8 Infartos subcorticales pequeños y únicos Infartos lacunares Infartos lacunares Arterias perforantes Arterias perforantes ACM Arterias perforantes ACM/basilar Arterioesclerosis Distal sin lesión vascular Enf. de pequeño vaso Proximal sin lesión vascular No predileción Proximal con lesión vascular Arterioesclerosis Enf. de pequeño vaso Nah et al. Stroke 2010 Infartos lacunares Infartos lacunares Infartos frontera Afectan la unión distal de dos territorios arteriales no‐anostomóticos presión de perfusión baja ¾10% de primeros ictus isquémicos ¾75% de ictus tardíos en oclusiones ACI ¾5% de ictus iniciales en oclusiones ACI 5% de ictus iniciales en oclusiones ACI ¾Mecanismo causal no completamente conocido Aterosclerosis Lipohialinosis Perfusión miseria Embolismo (arterio‐arterial) Distal con lesión vascular Mangla et al. Radiographics 2011 9 Topografía de los infartos frontera Patogénesis de los infartos frontera Dos procesos interrelacionados: •hipoperfusión •embolización Infartos frontera internos Infartos frontera corticales anteriores Infartos frontera corticales posteriores Momjian‐Mayor I, et al. Stroke 2005; Yong SW. et al. Stroke 2006 Infartos frontera externos (corticales) ¾Localización variable 9 Circulación colateral leptomençingea 9 Diferencias individuales Infartos frontera internos (subcortical) ¾Mas frecuentes entre arterias lenticuloestriadas y ACM superficial ¾Paraventricular: patrón en rosario ¾Difícil de diferenciar de infartos territoriales Mecanismos: Mechanismos: Embolismo No asociado a compromiso hemodinámico Compromiso hemodinámico (estenosis‐oclusión arterial) Peor pronóstico Deterioro clínico Perfusión de miseria (PWI) Microembolias (corazón o gran vaso) Infarto frontera subcortical Infartos corticales Área de baja perfusión (limitada capacidad de lavado) Momjian‐Mayor I, et al. Stroke 2005; Yong SW. et al. Stroke 2006 Momjian‐Mayor I, et al. Stroke 2005;Yong SW. Et al. Stroke 2006 10 Compromiso hemodinámico territorio frontera: perfusión miseria Infarto frontera interno: perfusión miseria FLAIR TTP ASL DWI Hipoperfusión en oclusiones ACI Infartos frontera: compromiso hemodinámico Infartos frontera: ateroesclerosis intracraneal, disección arterial 11 Conclusiones •Los informes radiológicos deben utilizar una clasificación objetiva de los ictus isquémicos •La RM (utilizando secuencias convencionales, de difusión y angiográficas)) permite una aproximación temprana al mecanismo angiográficas causal de los ictus isquémicos •Esta información puede tener impacto en la toma de decisiones terapéuticas 12 1 CLASIFICACIÓN TOPOGRÁFICA Y CAUSAL DE LOS ICTUS ISQUÉMICOS Alex Rovira Cañellas, Unidad Resonancia Magnética. Servicio de Radiología Hospital Universitario Vall d’Hebron Passeig Vall d’Hebron 119-129 08035 Barcelona e-mail: [email protected] Introducción Clasificación neurorradiológica Infartos del sistema arterial pial o leptomeníngeo Infartos del sistema arterial perforante. Infartos lacunares Infartos del centro oval Infartos frontera Infartos agudos múltiples sincrónicos INTRODUCCIÓN El ictus isquémico se considera una emergencia médica ya que el pronóstico de los pacientes que lo presentan depende de la rapidez con que se adopten las medidas adecuadas para reducir el daño cerebral y disminuir el riesgo de recurrencias. El objetivo principal, por lo que hace referencia a la actuación médica, es conseguir que los pacientes con un ictus isquémico agudo (incluyendo los episodios transitorios) puedan ser evaluados, diagnosticados y tratados adecuadamente y de manera urgente en un centro hospitalario que disponga de una atención organizada del mismo. Para lograr este objetivo, tienen una especial relevancia las exploraciones neurorradiológicas, que no sólo permiten diferenciar un ictus isquémico de uno hemorrágico y descartar lesiones causales del cuadro clínico de origen no vascular, sino que ofrecen además información sobre la presencia, características y extensión del tejido isquémico, así como de la lesión vascular causante del mismo. La primera parte de este capítulo profundizará en la clasificación topográfica y causal de los infartos, y la 2 segunda, revisará el papel actual de las diferentes técnicas neuroradiológicas en la valoración del ictus isquémico en fase aguda, especialmente en el contexto de un potencial tratamiento recanalizador. CLASIFICACIÓN TOPOGRÁFICA Y CAUSAL DE LOS ICTUS ISQUÉMICOS Establecer un diagnóstico precoz y preciso tanto topográfico como etiológico de los diferentes tipos de ictus isquémico tiene influencia sobre su manejo clínico, pronóstico, riesgo de recurrencia y tratamiento específico. Los ictus isquémicos se pueden clasificar en relación con sus características topográficas y mecanismo causal en base a diferentes datos entre los que se incluyen el perfil de riesgo de los pacientes, los hallazgos clínicos, diferentes marcadores biológicos o genéticos y finalmente y, de forma especialmente relevante, las alteraciones detectables en diferentes pruebas diagnósticas que se pueden dividir en tres grandes grupos: cardiológicas (electrocardiograma, ecocardiografía), vasculares (Doppler transcraneal y cervical, angio-TC, angio-RM, angiografía intraarterial) y parenquimatosas cerebrales (TC, RM). Clasificación neurorradiológica La gran evolución que ha experimentado el diagnóstico neurorradiológico, especialmente con la utilización de la RM y de técnicas avanzadas de TC, que combinan el análisis del parénquima cerebral y de los vasos cráneo-cervicales, ha permitido realizar un diagnóstico más preciso y rápido de la topografía y mecanismo causal de los ictus isquémicos. Desde el punto de vista topográfico, los infartos se pueden clasificar en los siguientes grupos: • Infartos territoriales de la circulación anterior • Infartos territoriales de la circulación posterior • Infartos lacunares • Infartos del centro oval • Infartos frontera • Infartos agudos múltiples sincrónicos 3 Infartos del sistema arterial pial o leptomeníngeo 1. Infartos territoriales de la circulación anterior El territorio anterior corresponde a aquellas áreas del cerebro irrigadas por las arterias carótidas internas y sus ramas. Son el tipo más común de ictus isquémicos, representando aproximadamente el 70% del total de los mismos. La oclusión de la arteria cerebral media (ACM) o de sus ramas es la causa más frecuente de infartos de la circulación anterior (>90%), los cuales de dividen según su extensión en masivos o parciales. Los infartos masivos de la circulación anterior son aquellos que afectan al menos a dos de los tres principales territorios silvianos (superficial anterior, superficial posterior y profundo). Estos infartos muestran una elevada frecuencia de progresión clínica y mortalidad. El mecanismo causal de estos infartos suele ser cardioembólico, o por oclusión aterotrombótica o disección de la arteria carótida interna. Existe un subtipo de infarto masivo de la ACM, denominado infarto maligno, que se produce cuando se afecta de forma completa o casi completa al territorio silviano, con una rápida progresión en el efecto de masa por desarrollo de edema masivo. Representa un 10% de todos los infartos, y se asocia a una mortalidad de aproximadamente el 80% tras un deterioro clínico que se produce generalmente entre el 2º-5º día tras el episodio clínico inicial. En estos pacientes la craniectomía descompresiva realizada en las primeras 48 horas tras el inicio del ictus, es una medida que reduce la mortalidad y mejora el pronóstico. La identificación de un infarto masivo mediante TC o RM especialmente si va asociado a una oclusión de la arteria carótida interna en pacientes jóvenes, predice un elevado riesgo de desarrollar un infarto maligno de la ACM (perfil maligno). Los infartos parciales de la circulación anterior afectan sólo a uno de los tres territorios silvianos principales. Tanto la progresión clínica como la mortalidad son más bajas en relación con los infartos masivos. El origen suele ser cardioembólico o por aterosclerosis de gran vaso en porcentajes similares. La diferencia en el tamaño de los infartos silvianos ayuda a orientar su mecanismo causal. Así, cuanto más proximal sea la oclusión arterial que produce el infarto, 4 mayor será su tamaño, y a su vez, cuanto mayor sea el tamaño del trombo, más proximal se situará la oclusión arterial. De esta forma, los trombos de origen cardíaco, en ocasiones de gran de mayor tamaño, ocluirán con más frecuencia los segmentos proximales y producirán con mayor frecuencia infartos masivos, mientras que los de origen embólico arterio-arterial de causa aterotrombótica producen infartos de menor tamaño que en ocasiones adoptan un patrón fragmentado uniterritorial. Los infartos de la arteria cerebral anterior (ACA) representan aproximadamente un 1% del total de infartos. Hasta un 9% son bilaterales y solamente un 4% son completos. La causa más frecuente es la aterosclerosis de gran vaso, afectando bien la propia ACA, la arteria carótida interna o ambas. En pacientes con infartos aislados de la ACA la disección arterial es un mecanismo causal frecuente pero que con frecuencia se infradiagnostica. La etiología cardioembólica representa el 10%, mientras que un 15% son de origen indeterminado. 2. Infartos territoriales de la circulación posterior La RM es la técnica de imagen con mayor sensibilidad en la detección y caracterización topográfica de los infartos de la fosa posterior. Una clasificación de estos infartos, basada en la distribución territorial arterial, facilita el determinar su mecanismo causal más probable: 1. Territorio proximal (arterias vertebrales y cerebelosas postero-inferiores): más de dos tercios de estos infartos se producen como consecuencia de un compromiso hemodinámico o a embolismos arterio-arteriales secundarios a enfermedad aterotrombótica de gran vaso tanto de las arterias intra como extracraneales. Hasta un 29% de los infartos proximales que afectan la región lateral del bulbo son secundarios a disección de la arterial vertebral. La extensión de estos infartos proximales se ha asociado con su mecanismo de origen, siendo de mayor tamaño los secundarios a enfermedad aterotrombótica en comparación con los secundarios a disección de la arteria vertebral. 5 2. Territorio medio (tronco basilar y arterias cerebelosas antero-inferiores): se producen generalmente por ateroesclerosis del tronco basilar, o por microateromatosis del origen de las arterias perforantes o circunflejas cortas (infartos grandes) o por enfermedad lipohialinótica de las arterias perforantes (infartos pequeños). 3. Territorio distal (arterias cerebelosas superiores, top de la basilar y arterias cerebrales posteriores): el mecanismo causal más frecuente es el embolismo de origen cardíaco o arterio-arterial. Infartos del sistema arterial perforante. Infartos lacunares El sistema perforante lo componen las arterias que penetran en el parénquima encefálico desde su emergencia en el polígono de Willis, en la arteria coroidea anterior o en la arteria basilar (arterias perforantes). Estas arterias irrigan los ganglios de la base, el tálamo, subtálamo y epitálamo, la cápsula interna y la región paramediana del tronco. Estos infartos se producen por la oclusión (proximal o distal) de una arteria perforante. Por definición el diámetro de los infartos lacunares no debe superar los 15 mm en la fase crónica, si bien en las fases precoces pueden ser mayores debido a la presencia de edema. Los infartos lacunares se producen con mayor frecuencia por oclusión de las arterias lentículo-estriadas, las tálamo-perforantes y las perforantes con origen en la arteria coroidea anterior. Representan entre el 11 y 25% de los ictus, si bien la mayoría resultan asintomáticos. El mecanismo causal en el 75% de los casos es la enfermedad de pequeño vaso (microateromatosis o lipohialinosis) y menos de un 25% son secundarios a embolismos arteria-arteria, a cardioembolismo, a disección arterial o a trombosis local por hipercoagulabilidad. Estas causas menos frecuentes confieren un peor pronóstico. Los infartos lacunares que afectan los hemisferios cerebrales se pueden dividir en dos grandes grupos: 1. Infartos lacunares grandes: la causa más frecuente es la microateromatosis que afecta el origen de una arteria perforante (habitualmente con origen en 6 las arterias coroidea anterior y cerebral media), que produce su oclusión y consecuentemente infartos grandes, proximales y sintomáticos. Con frecuencia estos infartos se presentan de forma aislada, es decir sin asociarse a otras lesiones isquémicas cerebrales (desmielinización, microsangrados, infartos crónicos) y no se suelen asociar a hipertensión arterial. En este tipo de infartos la obtención de estudios de RM con secuencias ponderadas en T1 de alta resolución demuestran con frecuencia placas ateromatosas en el segmento horizontal de la ACM. 2. Infartos lacunares pequeños: se producen por una destrucción de las arterias perforantes pequeñas (<200 micras) en el contexto de una enfermedad lipohialinótica generalmente asociada a hipertensión arterial crónica. Estos infartos suelen acompañarse de otras lesiones isquémicas y a microsangrados. Son infartos de pequeño tamaño y de localización distal que con frecuencia son asintomáticos, y que se localizan habitualmente en la región estriato-capsular y talámica. Tienen una mayor tasa de recurrencias y un peor pronóstico que los infartos lacunares aislados secundarios a microateromatosis. Los infartos lacunares del tronco afectan predominantemente la región paramediana de la protuberancia, y se producen como consecuencia de una oclusión proximal o distal de las arterias perforantes con origen en el tronco basilar. Estos infartos paramedianos de tronco se pueden clasificar de forma similar a la descrita para los infartos lacunares que afectan los hemisferios cerebrales: 1. Infartos paramedianos grandes: son infartos de gran tamaño que de forma constante afectan el margen anterior de la protuberancia y que se producen como consecuencia de una oclusión proximal de una arteria perforante secundaria a una ateromatosis de la arteria basilar o a una microateromatosis que afecta su origen. En este tipo de infartos es frecuente la existencia de patología ateroesceróstica en la arteria fácilmente demostrable en secuencias ponderadas en T1 de alta resolución 7 2. Infartos paramedianos parciales, son infartos de menor tamaño y en situación distal, generalmente secundarios a enfermedad lipohialinótica de pequeño vaso secundaria a hipertensión arterial crónica. Estos infartos tiene una localización distal en la región paramediana de la protuberancia, respetando por tanto su margen anterior. Infartos del centro oval El centro oval es la región de la sustancia blanca de los hemisferios cerebrales irrigada por arterias medulares (origen en las arterias leptomeníngeas), que comprende la mayoría de la corona radiata superficial y los fascículos de asociación intrahemisféricos. Los infartos que afectan el centro oval incluyen los que se producen por oclusión de las arterias propias de dicha región (arterias medulares), así como los que afectan áreas limítrofes entre las arterias medulares y otros territorios arteriales (infartos frontera internos). Los infartos del centro oval pueden subdividirse en dos tipos en base a su tamaño: 1. Infartos mayores: son infartos grandes (>15 mm) que no se pueden explicar por una oclusión de una única arteria medular Se suelen producir como consecuencia de un compromiso hemodinámica secundario a una estenosis grave carotídea o de la arteria cerebral media homolateral. Corresponden a infartos frontera internos. 2. Infartos menores (<15 mm): afectan a una sola rama medular y suelen ser secundarios a enfermedad lipohialinótica de pequeño vaso o por embolismos arterio-arteriales o de origen cardíaco. En esta última situación es frecuente que los estudios de difusión por RM muestren infartos adicionales de distribución fragmentada que afectan la sustancia gris cortical, en cuyo caso es más adecuado clasificarlos como infartos territoriales fragmentados de la circulación anterior. Infartos frontera Los infartos frontera son aquellos que afectan a la unión distal de al menos dos territorios arteriales. El mecanismo causal de este tipo de infartos no está del todo bien 8 establecido, si bien parecen ser consecuencia de un compromiso hemodinámico (infartos de bajo flujo) secundario a una estenosis arterial grave proximal, de un embolismo arterio-arterial o de una combinación de ambos mecanismos. Representan el 10% de los primeros ictus isquémicos y el 75% de los ictus tardíos en oclusiones de la arteria carótida interna. Los infartos frontera supratentoriales se pueden dividir en tres tipos en base a su topografía: 1. Infartos frontera internos (corresponden a infartos de centro oval grandes): afectan el territorio limítrofe entre las arterias perforantes con origen en el polígono de Willis y las ramas leptomeníngeas de las arterias cerebrales anterior, media y posterior. 2. Infartos frontera corticales anteriores: afectan el territorio limítrofe entre las arterias cerebrales anterior y media. Se asocian con frecuencia a infartos frontera internos. 3. Infartos frontera corticales posteriores: afectan el territorio limítrofe entre las arterias cerebrales posterior y media. El embolismo arterio-arterial o cardíaco es el mecanismo causal más frecuente en los infartos frontera corticales, mientras que el hemodinámico probablemente asociado a embolismo arterio-arterial de origen ateroesclerótico es el más frecuente en los infartos frontera internos. Esta diferencia en el mecanismo causal de los infartos frontera, quizás pueda atribuirse a la dificultad de diferenciar radiológicamente los infartos frontera corticales aislados de los infartos territoriales parciales silvianos y a la variabilidad individual en la distribución de los diferentes territorios arteriales. Infartos agudos múltiples sincrónicos Hasta un 17% de los pacientes con un ictus isquémico agudo muestran infartos agudos múltiples en los estudios neuroradiológicos, especialmente cuando se obtienen secuencias de difusión por RM. Éstos pueden tener varios mecanismos causales, que pueden sugerirse en base a su patrón topográfico. Se han propuesto cinco tipos de infartos agudos múltiples sincrónicos (IAMS): 9 • Tipo I: IAMS de circulación anterior uni-hemisféricos: corresponden a infartos que afectan de forma fragmentada un único hemisferio cerebral. Son los más frecuentes (44%) y en la mayoría de casos son infartos uni-territoriales (afectan exclusivamente el territorio de la ACM). Se producen como consecuencia de una fragmentación de un trombo en una única arterial proximal. El origen más frecuente de estos émbolos proviene de una ateromatosis carotídea o silviana, o de una disección carotídea (émbolos de la falsa luz). Otra de las situaciones que se debe tener en cuenta es la posible fragmentación de un trombo tras tratamiento fibrinolítico o tras procedimientos diagnósticos o recanalizadores intraarteriales. • Tipo II: IAMS de circulación anterior bi-hemisféricos. Corresponden al 21% de los IAMS. Son por definición infartos multi-territoriales cuyo mecanismo causal más frecuente es la enfermedad aterotrombótica seguida de la cardioembólica. También deben considerarse causas menos frecuentes como estados de hipercoagulabilidad (coagulación intravascular diseminada, púrpura trombocitopénica trombótica), y la enfermedad de pequeño vaso (IAMS lacunares). Las variaciones anatómicas del polígono de Willis pueden causar este tipo de IAMS. Así, en la hipoplasia del segmento A1 de la arteria cerebral anterior (10-20% de sujetos), la migración de émbolos desde una lesión carotídea contralateral puede producir infartos que afectan los territorios irrigados por las arterias cerebrales media y anterior homolaterales a la lesión carotídea, y el de la arteria cerebral anterior contralateral. • Tipo III: IAMS que afectan exclusivamente la circulación posterior. Corresponden al 23% de los IAMS y pueden ser uni o multi-territoriales. El mecanismo causal más frecuente es la enfermedad ateroesclerótica vértebro-basilar. • Tipo IV: IAMS que afectan tanto la circulación anterior como la posterior. Representan el 12% de los IAMS y el mecanismo causal más frecuente es el embolismo de origen cardíaco o del arco aórtico. Un posible mecanismo aterotrombótico debe sin embargo considerarse en pacientes que presenten un origen fetal de la arteria cerebral posterior (15-25% de sujetos) o una 10 persistencia de la arteria comunicante posterior, en cuyo caso el material embólico con origen en la arteria carótida interna puede producir infartos sincrónicos que afectan unilateralmente territorios dependientes tanto de la circulación anterior (arterias cerebrales anterior y media) como posterior (arteria cerebral posterior). Referencias 1. Caplan LR, Wityk RJ, Glass TA, Tapia J, Pazdera L, Chang HM, Teal P, Dashe JF, Chaves CJ, Breen JC, Vemmos K, Amarenco P, Tettenborn B, Leary M, Estol C, Dewitt LD, Pessin MS. New England Medical Center Posterior Circulation registry. Ann Neurol. 2004; 56:389-98. 2. Erro ME, Gállego J, Herrera M, Bermejo B. Isolated pontine infarcts: etiopathogenic mechanisms. Eur J Neurol. 2005;12:984-8. 3. Jung JM, Kwon SU, Lee JH, Kang DW. Difference in infarct volume and patterns between cardioembolism and internal carotid artery disease: focus on the degree of cardioembolic risk and carotid stenosis. Cerebrovasc Dis. 2010;29:490-6 4. Kameda W, Kawanami T, Kurita K, Daimon M, Kayama T, Hosoya T, Kato T; Study Group of the Association of Cerebrovascular Disease in Tohoku. Lateral and medial medullary infarction: a comparative analysis of 214 patients. Stroke. 2004;35:694-9. 5. Kang SY, Kim JS. Anterior cerebral artery infarction: stroke mechanism and clinical-imaging study in 100 patients. Neurology. 2008;70:2386-93. 6. Klein IF, Lavallée PC, Touboul PJ, Schouman-Claeys E, Amarenco P. In vivo middle cerebral artery plaque imaging by high-resolution MRI. Neurology. 2006;67:327-9. 7. Lee LJ, Kidwell CS, Alger J, Starkman S, Saver JL. Impact on stroke subtype diagnosis of early diffusion-weighted magnetic resonance imaging and magnetic resonance angiography. Stroke 2000;31:1081-9 8. Mangla R, Kolar B, Almast J, Ekholm SE. Border zone infarcts: pathophysiologic and imaging characteristics. Radiographics. 2011;31:120114. 9. Micheli S, Agnelli G, Palmerini F, Caso V, Venti M, Alberti A, Biagini S, Paciaroni M. Need for extensive diagnostic work-up for patients with lacunar stroke.J Neurol. 2008; 255:637-42. 10. Nah HW, Kang DW, Kwon SU, Kim JS. Diversity of single small subcortical infarctions according to infarct location and parent artery disease: analysis of indicators for small vessel disease and atherosclerosis. Stroke 2010;41:2822-7. 11 11. Roh JK, Kang DW, Lee SH, Yoon BW, Chang KH. Significance of acute multiple brain infarction on diffusion-weighted imaging. Stroke 2000;31:68894. 12. Rovira A, Grivé E, Rovira A, Alvarez-Sabin J. Distribution territories and causative mechanisms of ischemic stroke. Eur Radiol 2005;15:416-26 13. Sato S, Toyoda K, Matsuoka H, Okatsu H, Kasuya J, Takada T, Shimode A, Uehara T, Naritomi H, Minematsu K. Isolated anterior cerebral artery territory infarction: dissection as an etiological mechanism. Cerebrovasc Dis. 2010;29:170-7. 14. Yonemura K, Kimura K, Minematsu K, Uchino M, Yamaguchi T. Small centrum ovale infarcts on diffusion-weighted magnetic resonance imaging. Stroke. 2002;33:1541-4. 15. Yong SW, Bang OY, Lee PH, Li WY. Internal and cortical border-zone infarction: clinical and diffusion-weighted imaging features. Stroke. 2006;37:841-6. 16. Wartenberg KE. Malignant middle cerebral artery infarction. Curr Opin Crit Care. 2012 Apr;18(2):152-63. Eur Radiol (2005) 15: 416–426 DOI 10.1007/s00330-004-2633-5 A. Rovira E. Grivé A. Rovira J. Alvarez-Sabin Received: 30 June 2004 Accepted: 13 December 2004 Published online: 19 January 2005 # Springer-Verlag 2005 A. Rovira (*) . E. Grivé . A. Rovira . J. Alvarez-Sabin Hospital Vall d’Hebron, Unidad de Resonancia Magnetica, Passeig Vall d’Hebron 119-129, 08035 Barcelona, Spain e-mail: [email protected] NEURO Distribution territories and causative mechanisms of ischemic stroke Abstract Ischemic stroke prognosis, risk of recurrence, clinical assessment, and treatment decisions are influenced by stroke subtype (anatomic distribution and causative mechanism of infarction). Stroke subtype diagnosis is better achieved in the early phase of acute ischemia with the use of multimodal MR imaging. The pattern of brain lesions as shown by brain MR imaging can be classified according to a modified Oxfordshire method, based on the anatomic distribution of the infarcts into six groups: (1) total anterior circulation infarcts, (2) partial anterior circulation infarcts, (3) posterior circulation infarcts, (4) watershed infarcts, (5) centrum ovale infarcts, and (6) lacunar infarcts. The subtype of stroke according to its causative mechanism is based on the TOAST Introduction Ischemic stroke prognosis, risk of recurrence, clinical assessment, and treatment decisions are influenced by stroke subtype. Nevertheless, treatment decisions are often made before an extensive, time-consuming evaluation to identify a likely diagnosis is completed. Therefore, early classification of ischemic stroke subtype is of substantial practical clinical value. The most widely used methods for stroke subtype classification are the Oxfordshire Community Stroke Project and the TOAST (Trial of ORG 10172 in Acute Stroke Treatment) method. In 1991 the Oxfordshire Community Stroke Project (OCSP) proposed four subgroups of cerebral infarction (Table 1) based solely on presenting signs and symptoms [1]. This method, which classifies stroke into five major etiologic groups: (1) largevessel atherosclerotic disease, (2) small-vessel atherosclerotic disease, (3) cardioembolic source, (4) other determined etiologies, and (5) undetermined or multiple possible etiologies. The different MR imaging patterns of acute ischemic brain lesions visualized using diffusionweighted imaging and the pattern of vessel involvement demonstrated with MR angiography are essential factors that can suggest the most likely causative mechanism of infarction. This information may have an impact on decisions regarding therapy and the performance of additional diagnostic tests. Keywords Diffusion . MRI . Stroke method has the ability to predict the prognosis and shows good correlation with the underlying pathophysiology and imaging findings on cranial computed tomography (CT) [2]. The TOAST method is a set of guidelines developed for prospectively classifying ischemic strokes into specific subtypes, based mainly on the mechanism of infarction [3, 4]. Stroke patients are classified into five major etiologic/pathophysiologic groups (Table 2). With the widespread use of diffusion-weighted MR imaging (DWI) and MR angiography (MRA) in the acute stage of ischemic stroke, accurate early diagnosis of ischemic stroke subtype can be better achieved [5]. This information can be helpful for establishing the most likely 417 Table 1 Topographic clinical pattern of brain infarction (Oxfordshire method) 1. Lacunar infarcts (LACI) Acute stroke that includes one of the major recognized lacunar syndromes: pure motor, sensory, or sensorimotor strokes, ataxic hemiparesis, and dysarthria (clumsy hand syndrome) 2. Total anterior circula- Clinical syndrome in which there is tion infarcts (TACI) ischemia in both the deep and superficial territories of the middle cerebral artery (higher cerebral dysfunction such as dysphasia, dyscalculia, visuospatial disorder; homonymous visual field defect; and ipsilateral motor and/or sensory deficit of at least two areas of the face, arm, and leg) 3. Partial anterior circula- Clinical syndrome that includes only tion infarcts (PACI) two of the three components of the TACI syndrome, with higher cerebral dysfunction alone, or with more restricted sensorimotor deficit than those classified as LACI 4. Posterior circulation in- Clinical syndrome that includes ipsifracts (POCI) lateral cranial nerve palsy with contralateral motor and/or sensory deficit; bilateral motor and/or sensory deficit; disorder of conjugate eye movement; cerebellar dysfunction without ipsilateral long-tract deficit (i.e., ataxic hemiparesis); or isolated homonymous visual field defect mechanisms of ischemia and the risk of clinical progression, and for initiating the most appropriate therapy. This review article is divided into three parts. The first addresses the topographic patterns of brain infarction, the second is devoted to the mechanisms implicated in the genesis of multiple synchronous acute brain infarcts, and the third part reviews the various stroke categories on the basis of their causative mechanisms. ditions that govern flow in leptomeningeal anastomoses connecting the different arterial territories [6]. Despite this variability, brain imaging can accurately locate an ischemic stroke lesion in a specific vascular distribution in the majority of cases [7–10]. Arterial cerebral circulation can be divided into two systems: (1) the leptomeningeal (also known as superficial or pial) artery system; and (2) the perforating (or deep perforating) artery system (Table 3). Leptomeningeal artery system The leptomeningeal arteries comprise the terminal branches of the cerebral and cerebellar arteries, which penetrate the cortex and subjacent white matter. Infarcts within the territories irrigated by these arteries are often described as territorial infarcts. Territorial anterior infarcts Territorial anterior infarcts, mostly related to the middle cerebral artery (MCA) territory, can be divided into large and limited types. Large infarcts, defined as those covering at least two of the three MCA territories (deep, superficial anterior, and superficial posterior), show a high frequency of clinical deterioration, a minimum chance of good outcome, and a high mortality rate. Large MCA infarctions are associated with cardioembolism, internal carotid artery (ICA) occlusion, and ICA dissection. In patients with large infarcts without ICA occlusion, the frequency of cardioembolic Table 3 Topographic radiologic pattern of brain infarction Leptomeningeal artery system Topographic pattern of brain infarcts The boundaries between vascular distributions are determined by anatomic variations and by hemodynamic conTable 2 Stroke categories (TOAST method) 1 2 3 4 5 Large-vessel disease Small-vessel disease Cardioembolism Other etiology Undetermined or multiple possible etiologies Deep perforator artery system Territorial anterior circulation infarcts Large Malignant Limited Territorial posterior circulation infarcts Large territorial Small or end zone infarcts Brainstem infarcts Centrum ovale infarcts Large Small Watershed infarcts Internal Cortical anterior Cortical posterior Lacunar infarcts 418 disease is clearly higher than in large infarcts with ICA occlusion or limited infarcts without ICA occlusion [11]. Malignant MCA infarction refers to life-threatening (80% associated mortality), complete or almost complete MCA infarction. This type of infarction occurs in up to 10% of all stroke patients. The main cause of death is severe post-ischemic brain edema leading to raised intracranial pressure. The clinical course is uniform, with clinical deterioration developing within the first 2 to 3 days after stroke. DWI in the early phase of large territorial anterior infarction is an accurate method for predicting malignant MCA infarction (lesion volume >145 cm3) [12] in patients with persistent arterial occlusion and signs of total anterior circulation infarction. Early detection may be important since treatment for these large infarcts, such as hypothermia and/or hemicraniectomy can significantly reduce mortality [13]. Limited infarcts, covering only one of the three MCA territories, show a very low frequency of clinical deterioration. The mechanism of infarction in these cases is either cardioembolism or large-artery atherosclerosis in equal numbers. The lower incidence of cardioembolism in limited MCA infarcts as compared to large infarcts can be explained by the fact that cardiac thrombi are generally larger than thrombi of the large vessels [2] (Fig. 1). Territorial posterior infarcts Fig. 1 Diffusion-weighted MR imaging in anterior choroidal artery (AChA) infarcts. Right acute lacunar infarct limited to the AChA territory with no significant stenosis in an ipsilateral large artery, probably related to small-vessel disease (A). Acute right AChA territory infarct associated with other ipsilateral internal carotid artery infarcts due to internal carotid artery dissection (arrow) (B). Centrum ovale infarcts With the use of MR imaging, posterior circulation infarcts can be diagnosed and their topography delineated with high sensitivity. Infarcts are recognized in the territory of the posterior inferior (PICA), anterior inferior (AICA), and superior (SCA) cerebellar arteries and their branches, and in the territory of the posterior cerebral arteries (PCA) [8]. Large-vessel atherosclerosis of the extracranial and intracranial vertebrobasilar arteries, has been demonstrated angiographically in more than two thirds of patients with cerebellar infarction, and in situ branch artery disease in almost one fifth of these patients. Proximal disease of the vertebral artery is the most common feature in large-artery disease, leading to PICA, SCA, and PCA infarcts. The vessels most frequently affected by intraarterial embolism are the intracranial vertebral artery (leading to PICA infarcts) and the distal basilar artery (leading to SCA and PCA infarcts). Thrombus originating from proximal vertebral artery disease never occludes the intracranial vertebral artery, but it can affect the PICA, AICA, and SCA. Therefore, vascular imaging in patients with atherothrombotic cerebellar infarcts must assess the proximal vertebral artery (V1) [14]. Clinical deterioration in posterior circulation infarcts is associated with severe brain atrophy (suggesting longstanding hypoperfusion), and significant stenosis in the vertebrobasilar arteries. This feature implies that large-vessel disease plays an important role in clinical worsening in posterior circulation infarcts [2]. Small cerebellar infarcts (<2 cm) are frequently recognized with MR imaging. These small infarcts were thought to affect the boundary zone between various territories (nonterritorial infarcts), but in fact, they seem to be very small territorial infarcts resulting from involvement of small distal arteries. Therefore, small cerebellar infarcts correspond to “end zone” infarcts, with embolic or local arterial disease as the mechanism of infarction in the majority of cases; a low-flow hemodynamic state is the likely cause of infarction in only a minority of patients. Territorial and nonterritorial (small) cerebellar infarcts are essentially the same, and it is likely that their extent and location simply depend on the size of the embolus causing the infarct [15, 16]. Brainstem infarcts may be related to large-vessel disease (stenosis or occlusion) affecting the vertebral and basilar arteries or their main branches. In this situation, brain MR usually shows additional infarcts involving the territories irrigated by the cerebellar and posterior cerebral arteries. The centrum ovale is the central white matter of the cerebral hemispheres, including the most superficial part of the corona radiata and the long associated fasciculi. The cen- 419 trum ovale is supplied by long (2 to 5 cm) noninterdigitating medullary arteries that perforate it and course toward the upper part of the lateral ventricles. At the deeper part of the corona radiata the medullary branches tend to form an area of junction with the deep perforating branches of the MCA and the AChA. Centrum ovale infarcts are those limited to the territory of the medullary branches without accompanying involvement of the cortex or deep perforator territory [17]. Centrum ovale infarcts can be large and small. Large centrum ovale infarcts (>1.5 cm) affect more than one medullary branch. A hemodynamic mechanism related to severe ipsilateral internal carotid or MCA disease may be the leading cause. In this situation, the infarct affects the area of the internal border zone, between the deep perforators and superficial medullary territories of the MCA (internal border zone infarcts). However artery-to-artery embolism and cardioembolism cannot be ruled out in some patients. Small centrum ovale infarcts (<1.5 cm) involve only one medullary branch. Small infarcts were thought to be related to small-vessel disease involving the medullary branches, in a manner similar to lacunar infarction. In fact, the neurologic picture of small infarct of the centrum ovale is consistent with a so-called lacunar syndrome, although the motor or sensory distribution pattern is less often complete (face, arm, and leg) than partial. However, recent studies have shown that in a significant percentage of patients, small centrum ovale infarcts are associated with largevessel and heart disease, and should be distinguished from the more common lacunar infarcts [18]. Identification of subsidiary small acute infarcts in addition to an acute small infarct in the centrum ovale on DWI suggests an embolic mechanism [17]. Watershed infarcts Watershed infarcts (WIs) are ischemic lesions that occur at the junction between two or three arterial territories and Fig. 2 Watershed infarcts. Diffusion-weighted MR images showing the classical pattern of anterior cortical (A), posterior cortical (B) and internal (C) watershed infarcts. account for approximately 10% of ischemic strokes. The pathogenesis of WIs is controversial. It may involve various mechanisms such as systemic hypotension, severe arterial stenosis or ICA occlusion, microemboli, or a combination of these. Watershed infarcts account for 72% of delayed strokes in patients with ICA occlusion, but are rarely the initial manifestation of ICA occlusion (5%) [19]. Recent data indicate that WIs are often explained by a combination of two inter-related processes: hypoperfusion and embolization. In fact, severe ICA occlusive disease and cardiac surgery cause both embolization and decreased brain perfusion. This decreased perfusion might alter blood flow currents, encouraging microemboli to reach recipient blood vessels with the least effective blood flow. Moreover, microemboli that reach a border zone area with decreased blood flow are difficult to wash out [20]. Two types of vascular border zone areas exist within the cerebral hemispheres: the cortical and the internal. Cortical border zone areas are located between the cortical supply of the ACA and MCA (anterior cortical border zone), and between the MCA and PCA (posterior cortical border zone). Internal border zone areas are located between the ACA (anterior cerebral artery), MCA, and PCA, and the area supplied by the Heubner, lenticulostriate, and ACh arteries (Fig. 2). Purely anterior cortical WIs are very rare, as in most cases they are associated with internal border zone infarcts. Posterior cortical WIs are frequently difficult to differentiate from limited territorial infarcts affecting the posterior division of the MCA. Embolism, not distal field perfusion failure, is the predominant stroke mechanism in this type of WI. Internal border zone infarcts, commonly associated with severe ICA stenosis, are larger than lacunar infarcts within the vascular territory of the deep perforators. In some cases it is difficult to distinguish internal border zone infarcts from centrum ovale infarcts within the territory irrigated by the medullary branches of the MCA. The presence of two or more lesions, appearing as a chain of round infarcts along the internal vascular border zone, suggests an internal bor- 420 der zone infarct. Lesions in the internal border zone are mainly attributed to the effect of hemodynamic impairment caused by severe stenosis or occlusion of the ICA or MCA. Nevertheless, some studies have suggested an embolic mechanism for both cortical watershed and internal border zone infarcts [21]. Watershed infarcts involving more than one of the border zone areas in a single hemisphere are mostly related to severe ICA stenosis or occlusion. Bilateral watershed infarcts are typically related to a profound global reduction in perfusion pressure (hypoxia, hypovolemia) or to diffuse cerebral vessel disease (sickle-cell disease). The perforating (or deep perforating) artery system The perforating arteries arise from the arterial circle of Willis, the AChA, and the basilar artery, perforating the brain parenchyma as direct penetrators and supplying the diencephalon (thalamus, hypothalamus, subthalamus, and epithalamus), basal ganglia, internal capsule, and brainstem [10]. Lacunar infarcts The strict pathologic definition of a lacunar infarction (LI) is a small (<1.5 cm in diameter), fluid-filled cavity representing the healed stage of a small deep infarct, which was likely due to occlusion of a single penetrator artery arising from the large arteries of the circle of Willis or from the basilar artery. The most frequently affected perforating arteries include the lenticulostriate, the thalamoperforate and the perforators arising from the AChA. Thus, LI can be located deep within the cerebral hemispheric white matter, the upper two thirds of the basal ganglia, the internal capsule, the thalamus or the paramedian and lateral regions of the brainstem. Brainstem LI are mainly found in the paramedian region of the pons, which is supplied by long arterioles (midline and anteromedial perforators) arising from the basilar artery. The medulla and midbrain are supplied by short arterioles, which are less vulnerable to aging and hypertension, and as a consequence LI are very uncommon in these locations. The maximum size of 15 mm is probably true for LI in the chronic stage. In fact, most of them have a diameter <10 mm, but this dimension does not apply in the acute phase, when cellular swelling and extracellular edema can produce LI larger than 15 mm in diameter. Most first-ever symptomatic LI are located in the area supplied by the AChA [9, 22], while multiple, asymptomatic LI are mainly located within the territory irrigated by perforating arteries arising from the MCA or ACA. Most LI are asymptomatic. Symptoms are related to size (most lesions less than 200 μm in diameter are silent) and location (LI in the posterior limb of the internal capsule or in the pontine base are usually symptomatic, whereas lesions in the basal ganglia tend to be silent). Although most lacunar strokes appear to be a consequence of small-vessel disease (atherosclerosis or lipohyalinosis) [23], many of the other potential causes of small-vessel occlusion rarely cause LI, such as infective or immune vasculitis, artery-to-artery or cardiogenic embolism, arterial dissection, and in situ thrombosis due to a variety of hypercoagulable states [24]. This non–smallvessel disease mechanism of LI is supported by the not infrequent association of acute LI and superficial infarcts. As a consequence, vascular imaging of the cervical and intracranial arteries and a focussed search for a cardiac source of the embolism is needed in first-ever lacunar strokes. The detection of subsidiary infarctions in patients presenting with a classic lacunar syndrome and often diagnosed with intrinsic small-vessel disease (with a high probability of excellent recovery, recommendation of antiplatelet agents for secondary prevention, and low priority placed on extensive cardiac or arterial testing for other causes of stroke), should prompt the physician to search for an underlying embolic source and tailor a secondary stroke prevention strategy to treat the underlying cause. Embolic infarcts can present as a clinically well-defined lacunar syndrome. However, the concept of embolic LI is dubious for two main reasons: the low likelihood of an embolus entering a vascular territory that receives such a small proportion of cerebral blood flow, and the sharp angle of the penetrating vessels arising from the parent vessel, which makes it more likely for an embolus to be directed toward the leptomeningeal arteries. However, as compared to a leptomeningeal territory, the lack of collateral flow pathways in the deep perforating artery territories may make them more susceptible to infarction on entry of a very small embolus. In fact, it has been suggested that a massive shower of emboli such as that occurring during cardiac and aortic operations, in cholesterol embolization from ulcerated atheroma, and in paradoxical fat or air embolism can produce LI. Acute multiple brain infarction Synchronous acute multiple brain infarcts (AMBIs) can have various mechanisms of origin, which are suggested by their topographic pattern. With the use of DWI, the different types of AMBI can be easily identified [25, 26]: (1) Internal watershed infarcts: multiple rosary-like infarcts within border zone areas. Unilateral watershed infarcts are usually related to ICA disease, whereas bilateral ones are typically related to a profound overall reduction in perfusion pressure or to diffuse cerebral vascular disease. (2) Multiple small cortical or subcortical infarcts within the same arterial territory. This type of AMBI is attri- 421 buted to fragmentation of an embolus near its origin or located within a major proximal intracranial artery. Most of these infarcts are found within one cerebral hemisphere in the anterior circulation. (3) Multiple small infarcts attributable to multiple arteryto-artery thromboembolic material (located in one or more major arterial territories, depending on the arterial anatomy). Sometimes these infarcts are located in two hemispheres and in both the anterior and posterior circulation. Acute multiple brain infarcts exclusively affecting the posterior circulation are, in most cases, related to large-artery atherosclerosis. The anatomic variations that may explain AMBI include (1) posterior communicating artery (PCoA) originating from the ICA (fetal-type PCA), which explains the simultaneous infarcts in the anterior and posterior cerebral artery territory (25% of cerebral hemispheres); (2) PCoA patency (67% of anatomic dissections), explaining multiple infarcts in both the anterior and posterior circulation; and (3) AMBI in the territories of both ACAs when a single artery supplies the two medial aspects of the hemispheres, occurring in 18% of the normal population. (4) Multiple infarcts located in one or more major arterial territories of the anterior and/or posterior circulation produced from embolic sources proximal to the cervical arteries (heart or aortic arch), not attributable to anatomic variations of the cervicocranial arterial vessels. The pattern of multiple, small and large bihemispheric AMBIs is especially frequent in nonbacterial thrombotic endocarditis (marantic endocarditis). (5) Multiple simultaneous deep perforators. Most of these cases are related to bilateral, simultaneous small-artery occlusion. Cardioembolism can be the mechanism of infarcts in groups 2, 3, and 4, although it is much more frequent in group 4. Nevertheless, bilateral carotid stenosis or occlusion can also be associated with acute infarcts in both cerebral hemispheres. The main causes of AMBI in one hemisphere in the anterior circulation are MCA and ICA disease (75%). Although the factors that determine contemporary infarcts in small-vessel occlusion or severe bilateral largevessel disease are unknown (groups 3 and 5), it is believed that erytrocytosis (elevated primary or secondary hematocrit) and increased serum fibrinogen, may be important contributory factors [25]. In fact, these factors are significantly associated with bilateral cerebral infarction in patients with large-artery atherosclerosis or small-artery occlusion. Other possible explanations for AMBI located in different vascular territories include bilateral or unilateral watershed infarctions, or diffuse thrombotic or inflammatory processes, such as thrombotic thrombocytopenic purpura, granulomatous angiitis, and anticardiolipin syndrome, which lead to multiple small-vessel occlusions within a short period of time. Stroke categories The subtype of stroke according to its causative mechanism (TOAST) is based on risk factor profiles, clinical features, and the results of diagnostic tests [3, 4]. The TOAST algorithm classifies patients with ischemic stroke into five major etiologic and pathophysiologic groups: large-vessel atherosclerotic disease, small-vessel atherosclerotic disease, cardioembolism, other etiologies, and undetermined or multiple possible etiologies. Examining responses to acute treatment in each one of these subgroups of stroke mechanisms is clinically important; therefore, highly accurate early stroke subtyping is needed. The sensitivity and positive predictive value of the initial TOAST diagnosis of large- and small-vessel disease improves considerably with the combined use of DWI and MRA techniques [5]. Large-vessel atherosclerotic disease Large-vessel atherosclerosis represents about 13% of all patients with a first-ever stroke. Cortical or cerebellar lesions and brainstem or subcortical hemispheric infarcts greater than 1.5 cm in diameter on brain imaging are considered to be potential large-artery disease strokes. Supportive evidence by vascular imaging of more than 50% stenosis in an appropriate intracranial or extracranial artery (presumably due to atherosclerosis) is needed. Embolic (artery-to-artery) and hemodynamic mechanisms are the cause of stroke in these patients. The coexistence of both mechanisms has been postulated. Five patterns of ischemic lesions can be differentiated in patients with acute stroke and large-vessel disease [27, 28] (Fig. 3). Cortical territorial infarction Cortical territorial infarcts are ischemic lesions involving the cerebral cortex and subcortical structures in one or more major cerebral artery territories. Almost half of the patients with ICA occlusion have territorial infarction. However about 20% of strokes in the territory of a highgrade symptomatic ICA are cardioembolic or lacunar. This pattern can be subclassified into three forms: (1) limited MCA infarction in occlusions of a distal MCA branch or the proximal MCA, associated with effective collateral circulation; (2) large MCA infarction, frequently related to large emboli that proximally occlude the MCA in the absence of an efficient collateral system, or to occlusions of the distal ICA with a partially effective collateral 422 Fig. 3 Different patterns of cortical territorial infarcts within the internal carotid artery (ICA) territory demonstrated with diffusion-weighted MR imaging and MR angiography. A Limited left middle cerebral artery (MCA) infarction due to occlusion of the proximal MCA. B Complete right ICA infarction due to occlusion of the ICA. C Large left MCA infarction due to occlusion of the MCA. D Subcortical right MCA infarction due to MCA occlusion with small fragmented subcortical and cortical subsidiary infarcts. E Fragmented right cortical MCA infarction due to severe MCA stenosis (arrow). F Small fragmented right infarctions in the left MCA territory due to severe stenosis at the origin of the right ICA. 423 system; and (3) complete infarcts involving two major ICA cerebral artery territories in distal occlusions of the ICA without an effective collateral system. Subcortical infarction Subcortical infarcts are ischemic lesions in the territory of the deep perforating branches arising from the distal ICA or MCA trunk in proximal occlusions of the MCA or ICA in the presence of patent collaterals. Additional fragmented small cortical or subcortical infarctions can be also identified. Cortical territorial infarction with fragmentation Large ischemic cortical lesions with additional smaller cortical or subcortical lesions due to partial fragmentation of an embolus fall into the category of cortical infarction with fragmentation. Fragmented infarction Fragmented infarcts are defined as several small, disseminated lesions sprinkled randomly in the cortical ICA regions due to multiple emboli or the break-up of an embolus. Fragmented infarctions are more common in moderate ICA stenosis or in fragmentation of a lodged embolus. In the latter case, there is often no evidence of stenosis or occlusion in the intracranial arteries (resolved embolism). Watershed infarction The pathogenesis of watershed infarctions is controversial. The leading mechanism is believed to be critical ICA stenosis or occlusion, which may or may not be associated with transient hypoperfusion. In fact, 75% of patients with WI have high-grade ICA stenosis or occlusion associated with hemodynamically significant heart disease, increased hematocrit, or acute hypotension. Conversely, 50% of patients with high-grade or subtotal ICA stenosis have watershed infarcts. Atherosclerotic disease of the MCA may also cause watershed infarcts. For this reason, in addition to the extracranial vessel, cerebrovascular investigation in these patients should include the large intracranial vessels. tension seems to be the main etiology of these pathologic events, but a variety of other conditions such as aging, hypoperfusion, generalized atherosclerosis, diabetes, and orthostatic hypotension can contribute to the brain microcirculation compromise. In fact, in a significant proportion of patients, small-vessel disease is identified in normotensive, nonelderly, nondiabetic individuals. Atherosclerosis Atherosclerosis of the small penetrator vessels or microatheromatosis is the leading cause of small-artery disease. Atheroma plaques are localized in the proximal perforating arteries (microatheroma), in the origin of the penetrator artery (junctional atheroma), or in the parent artery on the circle of Willis (mural atheroma). Mural atheroma is particularly frequent in the basilar artery, producing infarcts limited to its pontine perforating branches. The atheroma plaques result in occlusion of the proximal segment of the large penetrating arteries (300–900 μm) and usually lead to single, large, frequently symptomatic LI [29]. This type of small-vessel disease, which is not so strongly related to hypertension, seems to predominantly involve the penetrator vessels arising from the anterior choroidal artery. Radiologic studies in patients with a firstever lacunar stroke of this type commonly show no additional asymptomatic infarcts or leukoaraiosis (Fig. 4a). Lipohyalinosis Lipohyalinosis, a vascular disease associated with longlasting, severe hypertension, is the second small-vessel lesion of relevance in lacunar infarction. It is a destructive lesion of the small penetrating arteries (<200 μm) that leads to small LI, which are commonly asymptomatic and located predominantly in the striatocapsule and thalamus. Leukoaraiosis and old asymptomatic LI are commonly seen on brain imaging in these patients (Fig. 4b). The mechanism of infarction seems to be related to occlusive thrombosis (perhaps exacerbated by a hypercoagulable state) or to non-occlusive poststenotic hypoperfusion. Patients with this type of small-vessel disease have a better outcome and a smaller prevalence of large-vessel cerebral disease and coronary disease than patients with the atherosclerotic type. Cardioembolism Small-vessel disease (small-artery occlusion) Small-vessel disease is the cause of about 25% of all firstever strokes. The most frequent pathologic events related to small-vessel disease are atherosclerosis and lipohyalinosis limited to the small penetrator vessels [23]. Chronic hyper- Cardiogenic embolism is responsible for about 15–27% of all first-ever strokes. The incidence is higher in patients under 45 years old, primarily because of the lower incidence of atherosclerotic disease in this age group. About 16% of ischemic strokes are associated with atrial fibril- 424 Table 4 Sources of risk for cardioembolism Higher risk sources for cardioembolism Lower risk sources for cardioembolism Fig. 4 Acute LI (Fast-Flair and diffusion-weighted MR images). A Acute left internal capsule (territory of the anterior choroidal artery) infarct with no additional infarcts or leukoaraiosis, probably related to microatherosclerosis. B Acute left thalamic lacunar infarct associated with small chronic LI and dilated Virchow-Robin spaces, suggesting small-vessel atherosclerotic disease due to lipohyalinosis. lation, and 10% are probably due to embolism from an atrial appendage thrombus, with the remainder caused by other stroke mechanisms [30]. Cerebral infarction in atrial fibrillation tends to be large and severely disabling [31]. A possible or probable diagnosis of cardioembolic stroke requires the identification of at least one cardiac source for an embolus (high-risk or medium-risk sources) (Table 4). Evidence of a previous transient ischemic attack or stroke in more than one vascular territory or systemic embolism supports a clinical diagnosis of cardiogenic stroke. On brain imaging, large cortical territorial infarction should suggest a cardioembolic mechanism, particularly if it is not associated with ICA occlusion. The median volume of infarcts caused by cardiogenic embolism is more than twice the median volume of infarcts caused by artery-toartery embolism [31]. Although it has been suggested that simultaneous acute infarction indicates a cardioembolic mechanism, in the majority of cases they are not caused by a proximal embolism from the heart or aortic arch, but instead by arteryto-artery embolism or fragmentation of a proximal artery embolus. Atrial fibrillation Mural thrombus associated with acute myocardial infarction Prosthetic heart valve Dilated cardiomyopathy Bacterial endocarditis Rheumatic mitral stenosis Ascending aorta atheroma (≥4 mm in size) Intracardiac thrombus Spontaneous left atrial echo contrast Left ventricular aneurysm or large area of dyskinesia Nonbacterial (marantic) endocarditis Sick sinus syndrome Calcified aortic stenosis Patent foramen ovale or atrial septal defect Atrial septal aneurysm Mitral annulus calcification Ventricular septal defect Mitral valve prolapse Other etiologies Only 2% of all patients with a first-ever stroke fall into the other etiology category. The lesion can have any size or location. To classify a stroke under this category, cardiac sources of embolism and large-artery atherosclerosis should be excluded. These unusual mechanisms of stroke include nonatherosclerotic, nonhypertensive vascular diseases (Moya-Moya disease, craniocervical arterial dissection, and primary and systemic vasculitis), migraine, hypercoagulable states, hematologic disorders, stroke after catheter angiography, and sporadic or genetically determined small-vessel occlusion such as cerebral autosomal dominant arteriopathy (CADASIL) and Fabry’s disease. These rare forms of small-vessel occlusion cannot be differentiated radiologically from the classical atherosclerotic and hypertensive forms of small-vessel disease. Undetermined etiology or multiple possible etiologies Strokes classified as having undetermined or multiple possible etiologies must possess one of the following conditions: (1) No cause found despite extensive assessment. (2) Most likely cause could not be determined because more than one plausible cause was found (e.g., atrial fibrillation or lacunar infarct associated with >50% symptomatic large vessel stenosis). 425 This type of stroke represents about 35% of all patients with a first-ever stroke. However, this percentage can vary considerably, since in some cases an extensive diagnostic evaluation is performed (ECG, Duplex, MRI/MRA, transcraneal Doppler ultrasound, transesophageal echocardiography, laboratory tests for coagulation factors, proteins C and S, antithrombin III, and various autoantibodies), whereas in others the evaluation is cursory. Conclusion lesion and the presence of significant arterial stenosis or occlusion. Multimodal MR imaging facilitates the achievement of these diagnostic goals, improving the accuracy of early ischemic stroke subtype identification. The various MRI patterns of acute brain ischemia (topography, size, and multiplicity) visualized using DWI, the pattern of vessel involvement demonstrated with MR angiography, and the presence of previous ischemic lesions detected with conventional MRI, are essential factors that can suggest the most likely mechanisms of origin. This information may have an impact on decisions regarding therapy and the performance of additional diagnostic tests. The goal of imaging in the acute phase of ischemic stroke is to identify the location and extension of the relevant References 1. Bamford J, Sandercock P, Dennis M et al (1991) Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 337:1521–1526 2. Tei H, Uchiyama S, Ohara K, Kobayashi M, Uchiyama Y, Fukuzawa M (2000) Deteriorating ischemic stroke in 4 clinical categories classified by the Oxfordshire Community Stroke Project. Stroke 31:2049–2054 3. Adams HP, Bendixen BH, Kappelle LJ et al (1993) Classification of subtype of acute ischemic stroke: definitions for use in a Multicenter Clinical Trial. Stroke 24:35–41 4. Kolominsky-Rabas PL, Weber M, Gefeller O, Neundoerfer B, Heuschmann PU (2001) Epidemiology of ischemic stroke subtypes according to TOAST criteria: incidence, recurrence, and long-term survival in ischemic stroke subtypes: a populationbased study. Stroke 32:2735–2740 5. Lee LJ, Kidwell CS, Alger J et al (2000) Impact on stroke subtype diagnosis of early diffusion-weighted magnetic resonance imaging and magnetic resonance angiography. Stroke 31:1081–1089 6. van der Zwan A, Hillen B, Tulleken CA, Dujovny M, Dragovic L (1992) Variability of the territories of the major cerebral arteries. J Neurosurg 77:927– 940 7. Tatu L, Moulin T, Bogousslavsky J, Duvernoy H (1998) Arterial territories of the human brain: cerebral hemispheres. Neurology 50:1699–1708 8. Tatu L, Moulin T, Bogousslavsky J, Duvernoy H (1996) Arterial territories of human brain: brainstem and cerebellum. Neurology 47:1125–1135 9. Hupperts RM, Lodder J, Heuts-van Raak EP, Kessels F (1994) Infarcts in the anterior choroidal artery territory: anatomical distribution, clinical syndromes, presumed pathogenesis and early outcome. Brain 117:825–834 10. Takahashi S, Suzuki M, Matsumoto K, Ishii K, Higano S, Fukasawa H, Sakamoto K (1994) Extent and location of cerebral infarcts on multiplanar MR images: correlation with distribution of perforating arteries on cerebral angiograms and on cadaveric microangiograms. Am J Roentgenol 163:1215–1222 11. Heinsius T, Bogousslavsky J, Van Melle G (1998) Large infarcts in the middle cerebral artery territory: etiology and outcome patterns. Neurology 50:341–350 12. Oppenheim C, Samson Y, Manai R, Lalam T, Vandamme X, Crozier S, Srour A, Cornu P, Dormont D, Rancurel G, Marsault C (2000) Prediction of malignant middle cerebral artery infarction by diffusion-weighted imaging. Stroke 31:2175–2181 13. Georgiadis D, Schwarz S, Aschoff A, Schwab S (2002) Hemicraniectomy and moderate hypothermia in patients with severe ischemic stroke. Stroke 33:1584–1588 14. Min WK, Kim YS, Kim JY, Park SP, Suh CK (1999) Atherothrombotic cerebellar infarction: vascular lesion–MRI correlation of 31 cases. Stroke 30:2376–2381 15. Amarenco P, Kase CS, Rosengart A, Pessin MS, Bousser MG, Caplan LR (1993) Very small (border zone) cerebellar infarcts: distribution, causes, mechanisms and clinical features. Brain 116:161–186 16. Amarenco P, Levy C, Cohen A, Touboul PJ, Roullet E, Bousser MG (1994) Causes and mechanisms of territorial and nonterritorial cerebellar infarcts in 115 consecutive patients. Stroke 25:105–112 17. Bogousslavsky J, Regli F (1992) Centrum ovale infarcts: subcortical infarction in the superficial territory of the middle cerebral artery. Neurology 42:1992–1998 18. Yonemura K, Kimura K, Minematsu K, Uchino M, Yamaguchi T (2002) Small centrum ovale infarcts on diffusionweighted magnetic resonance imaging. Stroke 33:1541–1544 19. Bogousslavsky J, Regli F (1986) Borderzone infarctions distal to internal carotid artery occlusion: prognostic implications. Ann Neurol 20:346–350 20. Belden JR, Caplan LR, Pessin MS, Kwan E (1999) Mechanisms and clinical features of posterior border-zone infarcts. Neurology 53:1312–1318 21. Del Sette M, Eliasziw M, Streifler JY, Hachinski VC, Fox AJ, Barnett HJ (2000) Internal borderzone infarction: a marker for severe stenosis in patients with symptomatic internal carotid artery disease. For the North American Symptomatic Carotid Endarterectomy (NASCET) Group. Stroke 3:631–636 426 22. Boiten J, Lodder J, Kessels F (1993) Two clinically distinct lacunar infarct entities? A hypothesis. Stroke 24:652– 656 23. de Jong G, Kessels F, Lodder J (2002) Two types of lacunar infarcts: further arguments from a study on prognosis. Stroke 33:2072–2076 24. Lodder J, Bamford JM, Sandercock PA, Jones LN, Warlow CP (1990) Are hypertension or cardiac embolism likely causes of lacunar infarction? Stroke 21:375–381 25. Roh JK, Kang DW, Lee SH, Yoon BW, Chang KH (2000) Significance of acute multiple brain infarction on diffusionweighted imaging. Stroke 31:688–694 26. Baird AE, Lovblad KO, Schlaug G, Edelman RR, Warach S (2000) Multiple acute stroke syndrome: marker of embolic disease? Neurology 54:674– 678 27. Min WK, Park KK, Kim YS, Park HC, Kim JY, Park SP, Suh CK (2000) Atherothrombotic middle cerebral artery territory infarction: topographic diversity with common occurrence of concomitant small cortical and subcortical infarcts. Stroke 31:2055–2061 28. Szabo K, Kern R, Gass A, Hirsch J, Hennerici M (2001) Acute stroke patterns in patients with internal carotid artery disease: a diffusion-weighted magnetic resonance imaging study. Stroke 32:1323–1329 29. Arauz A, Murillo L, Cantu C, Barinagarrementeria F, Higuera J (2003) Prospective study of single and multiple lacunar infarcts using magnetic resonance imaging: risk factors, recurrence, and outcome in 175 consecutive cases. Stroke 34:2453–2458 30. Hart RG, Halperin JL (2001) Atrial fibrillation and stroke: concepts and controversies. Stroke 32:803–808 31. Timsit SG, Sacco RL, Mohr JP, Foulkes MA, Tatemichi TK, Wolf PA, Price TR, Hier DB (1993) Brain infarction severity differs according to cardiac or arterial embolic source. Neurology 43:728–733


© Copyright 2026