
Validation of Six-Minute-Walk Distance as a Surrogate
DOI: 10.1161/CIRCULATIONAHA.112.105890 Validation of Six-Minute-Walk Distance as a Surrogate Endpoint in Pulmonary Arterial Hypertension Trials Running title: Gabler et al.; Validation of 6MWD in PAH trials Nicole B. Gabler, PhD, MPH, MHA1; Benjamin French, PhD1,2 ; Brian L. Strom, MD, MPH1,2 ; Harold I. Palevsky, MD3,4 ; Darren B. Taichman, MD, PhD3,4 ; Steven M. Kawut, MD, MS1,3,4; Scott D. Halpern, MD, PhD1,2,3,4 1 Center for Clinical Epidemiology & Biostatistics and Dept of Biostatistics & Epidemiology; Leonard Le eon onar ardd Davis ar Davi Da v s In Institute nst s itute of Health Economics; 3Pu Pulmonary, Allergy, Aller ergy, and and Critical Care Division; 4 Pulmonary Pul Pu lm ry Vascular lmonar Vasc scul ular ar Disease Dis isea easee Program Pro P rogr gram am of of the the Penn Penn Cardiovascular Caard rdio iova v sccul ulaar ar Institute, Ins nsti tittutee, Perelman Pere Pe relm lman an School Sch S choo ooll of Medi Me dici di cine ci ne, Un ne Univ iv ver ersi sitty ooff P ennnsylvvan vania, nia,, P hila hi l de la dellph lphiaa, PA A Medicine, University Pennsylvania, Philadelphia, 2 C Correspondence: orrespond nden ence ce:: Ni Nicole l B. B Gabler, G bl PhD Perelman School of Medicine University of Pennsylvania 708 Blockley Hall 423 Guardian Drive Philadelphia, PA 19104-6021 Tel: 215-573-0779 Fax : 215-573-5315 E-mail: [email protected] Journal Subject Codes: [18] Pulmonary circulation and disease; [26] Exercise/exercise testing/rehabilitation; [100] Health policy and outcome research 1 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Abstract: Background - Nearly all available treatments for pulmonary arterial hypertension (PAH) have been approved based on change in six-minute-walk distance (¨6MWD) as a clinically important endpoint, but validity as a surrogate endpoint has never been shown. We aimed to validate the difference in ¨6MWD against the probability of a clinical event in PAH trials. Methods and Results - First, to determine if ¨6MWD between baseline and 12 weeks mediated the relationship between treatment assignment and development of clinical events, we conducted a pooled analysis of patient-level data from the ten randomized placebo-controlled trials previously submitted to the U.S. Food and Drug Administration (n=2404). Second, to identify a threshold effect for the ¨6MWD that indicated a statistically significant reduction in clinical g g 21 drug/dose g events,, we conducted a meta-regression among level combinations. ¨6MWD h m he etaet aaccounted for 22.1% (95% CI: 12.1%, 31.1%) of the treatment effect (p<0.001).. T The metaanalysis showed an average difference in ¨6MWD of 22.4 m (95% CI: 17.4 to 27.5), favoring y of a clinical event active treatment over placebo. Active treatment decreased the probability sum umma mary y OR: OR: 0.44; 0.4 .44; 4; 95% 5% CI: CI: 0.33, 0.333, 0.57). 0.557)). Thee meta-regression met etaa-regr gres e sion revealed rev e eaale ledd a significant sign gnif i icantt threshold thre th reshold (summary efffeect c of 41.8 m eters. s. effect meters. Conc Co ncclu usionss - O ur results ressullts suggest re suugg ges est that thatt ¨ 6M MWD WD does does not noot explain explai plainn a large larrge proportion prrop opor ortion on of of the th he Conclusions Our ¨6MWD reaatm tmentt effect, effect ef ct, has has only o ly on y modest mod odes e t validity v lidiity as va as a surrogate surrog su gat atee en endp dpoi o ntt ffor or cclinical linic icall eevents, vents,, aand ve ndd m a nnot ay o treatment endpoint may be a sufficien en nt su surr rrog rr oggat a e en ndp dpoi oint ntt. F urrth ther er rresearch esea es earc ea rchh is i nnecessary eces ec esssar aryy to o ddetermine eter et ermi er mine mi ne whether whe w heth he ther th er the sufficient surrogate endpoint. Further threshold value of 41.8 m is valid for long-term outcomes or if it differs among trials using background therapy or lacking placebo controls entirely. Key words: hypertension, pulmonary; meta-analysis; statistics; trials 2 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Introduction Pulmonary arterial hypertension (PAH) is a progressive disease leading to right heart failure and death.1-2 Seven drugs developed in the last 20 years have been shown to improve six-minutewalk distance (6MWD) in patients with PAH and have been approved for use in the U.S. on that basis. While 6MWD is viewed by regulatory agencies as a clinically important endpoint in its own right, several studies have shown that patients who achieve greater improvements in 6MWD (or reach certain absolute values of 6MWD) have better clinical outcomes.3-5 However, such observational data are insufficient to determine whether 6MWD is a valid surrogate endpoint for clinical events.6-9 Determining the validity of 6MWD as a surrogate endpoint in PAH trials ls iiss pa part particularly rttic icul ular ul a ly ar timely imely in light of conflicting results of recent meta-analyses.10-13 While some of these co ont ntra radi ra dict di ctio ct ions io ns may may be b due to inadequate samplee size size or follow-up, follow-upp, or tto o in iintrinsic trinsic limitations of contradictions study-level tud dyy level meta-analyses, meta me taa-aanaaly lyse sees, s these tthe hese he se differences difffe ferrenncess also also suggest suggeest st the tthhe possibility posssiibi bili liity that tha hatt 6WMD 6WMD is is a poor poor poo or 14-17 4-1 17 surrogate. urr rrog ogat og a e. In tthi at this his stud sstudy, tud dy, w we uused sed ttwo wo ccomplementary om mpl plem men ntaary aapproaches ppro pp roac ro acche hes to vva validate alid id dat atee 6M 6MWD 6MWD. WD.14 WD First, F Firs i st, patiien ntt leeve vell data da from fro om all all available a ai av aila labl la blee Phase bl Phas Ph asse III III randomized raand ndom omiz om ized iz e clinical cliini nica call trials ca ttri rial a s submitted al subm su bmitted for bm we used patient-level drug approval to assess whether changes in 6MWD ('6MWD) mediate the relationship between treatment assignment and clinical outcomes. Second, we quantified how treatment effects on '6MWD predicted treatment effects on patient-centered outcomes, with the goal of determining whether a threshold '6MWD exists beyond which investigators could reliably predict that superior clinical outcomes would follow in future trials. Methods Study Population Through a contract with the U.S. Food and Drug Administration (FDA) to one author (SDH), we 3 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 obtained de-identified individual patient data for all participants in Phase III placebo-controlled randomized trials submitted to the FDA through 2008 testing prostanoids, endothelin receptor antagonists, or phosphodiesterase inhibitors. Eleven clinical trials examined seven agents (ambrisentan, bosentan, sitaxsentan, iloprost, treprostinil, sildenafil, and tadalafil). We excluded one study (BREATHE-2) because it only included 33 participants and was not a Phase-III trial. Additional trial details are available elsewhere.18-25 We purposely included trials of treatments that were not approved by the FDA (e.g., sitaxsentan), a result of either unacceptable toxicity of effective dosages or dosages that were determined to be ineffective. Both the mediator and threshold analyses would be predictably biased if we only included FDA-approved treatments, and the resulting conclusions would not be useful for future trial design orr regulatory regullator at ry decisions. deci de cisi ci sion si o s. on s All included trials reported similar methodology, including outcome assessment and variable co olllec ecti tion ti on n at at 112-weeks 2-w -w weeks ee follow-up. collection C lin nic i al events event ntss Clinical Cl lin inic ical ic a eeve al vent ve n s in nt nclud cluded ed d aany ny ooff th thee foll ffollowing olllow wing ng bbefore efoore ef ore th he en endd of th he tr tria iaal: ddeath, eaath th,, lu lung ng Clinical events included the the trial: ransplantatio on, n atrial aatr tria tr iaal septostomy, sept se p os osto tomy to my,, ho my hosp pit i al aliz izzat atio io on du duee to o worsening woors w r en enin i g PA in PAH, H, w wit ithd hdra hd rawa ra wall for wa transplantation, hospitalization withdrawal worsening right-heart failure, or addition of other PAH medications. We did not consider a deterioration in 6MWD to represent a clinical event because it was the surrogate we were attempting to validate. Further details are provided in the Supplemental Material, Table 1. 6MWD Change in 6MWD was calculated as the difference, in meters, between the distance walked at baseline and 12 weeks. Baseline 6MWD was recorded at or within two weeks of randomization. In all analyses, patients who were missing a 12-week 6WMD because they died during the trial (n=45, 2%) were assigned a value of 0. We chose this value to reflect the fact that deaths are 4 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 extremely important clinical events and also to be consistent with the metric used in the majority of the trials included in our analysis. We used multiple imputation26 to designate values for patients who survived but were nonetheless missing 12-week 6MWD (n=182, 8%). The imputation model included variables associated with clinical events: baseline 6MWD, age, gender, weight, race, height, diagnosis category (idiopathic, connective tissue disease, HIV infection/anorexigen use, or congenital heart disease), 6MWD at 4 or 6-weeks follow-up, NYHA functional classification, warfarin use, baseline sodium, cardiac output, and mean pulmonary arterial pressure. Five datasets were imputed. All imputations were completed in SAS version 9.2.27 Mediator Analysis We utilized standard methodology to determine whether '6MWD mediates the relationship between treatment events beetw twee eenn trea ee tr rea e tmen tmen nt as aassignment signment and the development developm men e t of clinical ev ven e tss aatt 12 112-weeks -weeks follow-up.15-16 We defined d treatment tre reat attment nt assignment asssig ssignm nmen nm entt as either eithher active acttive treatment trreatm tm men entt or or placebo. pllaccebo bo.. W Wee cond cconducted ondducte ucte t d re regression egr greesssion analyses anal an alys al yses ys es to to ev eevaluate val aluuate uate tth the he ffour he our fo ou ffollowing llow ll owin ow ingg hy hypo hypotheses. poth po hes e es. Re Reje Rejecting ject je ctiing ct ing th the he nu null lll for or aall ll ffour ourr hypo ou hhypotheses ypo poth hes esees was necessary necessar arry to support sup uppo p rt po r '6MWD '6M 6MWD WD as as a mediator/surrogate medi me d at di a or or/s /sur /s urro ur r ga ro gate tee end end point. poi oint nt.. nt (1) Treatment assignment has a significant effect on '6WMD from baseline to 12 weeks; (2) '6MWD has a significant effect on the odds of developing a clinical event; (3) Treatment assignment has a significant effect on the odds of developing a clinical event; (4) The effect of treatment assignment on the odds of developing a clinical event is attenuated when '6MWD is added to the model. We used logistic or linear regression for binary or continuous outcomes, respectively. All regression models adjusted for study to account for study-level differences in treatment assignment, and for baseline walk distance to account for patient-level differences in risk of 5 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 clinical events. No other adjustments were made because patients were randomly assigned to treatment or placebo. After rejecting the null for the above four hypotheses, we determined the proportion of variability explained by the '6MWD in the relationship between treatment assignment and development of a clinical event.28-29 We used a generalized linear model with a logit link to quantify the relationship between treatment assignment and log odds of developing a clinical event with adjustment for study and baseline walk (‘reduced’ model). We then added the '6MWD to the model (‘full’ model). The subsequent change in the treatment assignment coefficient between the reduced and full models provided the proportion of variability explained by '6MWD. Bootstrap resampling was used to create a confidence interval for tthe he pper percent erce er cent ce nt change. Estimates of percent change were obtained for each resampled dataset, and the standard deviation devviat de viat atio ion of the tthhe estimates est stim i ates across 1000 resampled resampl p edd datasets datasets was used use seed as the tthhe he standard error.30 dit itio io on, wee uused sed ed a m oddif ifie ied dS obeel testt tto o ass sssesss whet w h theer th he amou aamount mountt off m eddiaatio a ti n w as In add addition, modified Sobel assess whether the mediation was statistically tat atis isti is tica ti call ca llyy si ll sign significant; gn nif ific ican ic ant; an t; the the h m modified odiifi od fieed ed ttes test estt ac es acco accounted coun co unte un tedd fo te forr th thee fa fact ct tthat hatt th ha thee su surr surrogate r og ogat atee (c at (con (continuous) onnti tinu nuou nu ous) ou s) 3 outccom omee (b (bin inar in a y) ar y w ere onn ddifferent er i feere if rent n ssca nt cale ca les. le s.16, 31 We eevaluated valu va l atted tthe lu he aassumption ssum ss umpt um ptio pt ionn of no effec io effect ct and the outcome (binary) were scales. modification between treatment and the mediator31 by fitting a logistic regression model for clinical events with an interaction term between treatment assignment and '6MWD. Threshold Effect Analysis We then conducted a trial-level meta-analysis and meta-regression to assess the relationship of the treatment effect on the mediator ('6MWD) with the treatment effect on the odds of developing a clinical event at 12-weeks follow-up. This threshold analysis proceeded in four steps. First, we estimated values for the exposure variable, placebo-adjusted study-level 6 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 '6MWD, by conducting linear regressions within each trial. In these trial-specific patient-level regressions, the exposure variable was treatment (drug and dose), entered as indicator variables (with placebo as the referent). The outcome variable was '6MWD, and adjustment again was made for baseline 6WMD. Second, we estimated values for the outcome, the placebo-adjusted study-level log odds of developing a clinical event between baseline and 12-weeks, using logistic regression analyses within each trial. In these trial-specific patient-level regressions, treatment (drug and dose, entered as indicator variables with placebo as the referent) was the exposure, clinical event (yes or no) was the outcome, and adjustment was made for baseline 6MWD. Exact logistic regression egression was used when the number of clinical events in a study was small. Third, we used the 21 drug/dose combinations vs. placebo across trials in a fixed-effects meta-regression relating '6MWD meeta ta--reg -re re ress s ionn re ss rela lating g estimated difference in ' 6MWD to the estimated estima es matted ted logg odds ratio for cllin cclinical nic ical events. The Th square sqquare of of the th inverse inveersse standard inve sttandarrd error erro or was wa used useed ed as a weight weig ig ght to to account acccou count unt for f r fo uncertainty estimated ratio. threshold effect calculating unce un ceert rtai aint ai ntyy in nt in tthe he eest stim st imat im ated at e llog og oodds ddss ra dd ati tio. o. We ddetermined eter et ermi er mine mi nedd th ne thee th hre resh shol sh oldd ef ol effe fect fe ct bby y ca alc lcul ulat ul atin at ingg in 95% prediction predicti tiion bands ban ands ds around aroun roun undd the th he meta-regression meta me ta-r -reg -r egre eg r ss re ssio ionn line. io l ne. The li The threshold thr hres esho hoold was was ccalculated alcu al cula cu late la tedd aass the valuee te of difference in '6MWD where the upper prediction band crossed the null value of 1.0 for relative odds of a clinical event. Prediction bands quantify the uncertainty in predicting the difference in clinical worsening in a single trial given a defined difference in '6MWD. Linearity of the final regression model was assessed via standard regression diagnostics. Finally, we sought to determine whether study-level patient characteristics confounded the association between '6MWD and relative odds of clinical events. Potential confounders were chosen a priori based on known differences in treatment response by race and sex,32 and by diagnosis and NYHA functional classification.33 Therefore, covariates in our regression model 7 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 were race (% black), sex (% female), PAH diagnostic category (% connective-tissue related), and NYHA functional classification (% III or IV). If a potential confounder altered the coefficient for the treatment variable by 10% or more, it was retained in the final model. We conducted two secondary analyses. First, we excluded the PHIRST study, in which patients were permitted to use background therapy with other approved PAH-specific agents. Second, we removed patients who were New York Heart Association (NYHA) class IV at randomization since it is unlikely that these patients will be included in future clinical trials. All regressions and meta-regressions were conducted in R version 2.13 (R Development Core Team, Vienna, Austria). This study was determined to be exempt by the Institutional Review Board Boar arrd of of the the University of Pennsylvania (approval #814001). All co-authors had access to the study data, take authority manuscript akee responsibility rres espo es po ons n ib ibilit itty for f r the analysis, and had auth fo hor o ity over manusc sccript pt ppreparation re reparation and the decision publication. deciisi deci s on to submit suubm mitt ffor or pub ubli ub lica li cattion ca tion.. Results Resu Re sult su ltss lt The ten trials included 2404 patients; 1563 (65%) were allocated to active treatment. Participants’ median age was 50 years (range: 10 to 90 years), 22% were male, and 5% were black (Table 1). Five hundred eighty one patients (25%) had a diagnosis of PAH due to connective tissue disease and 1349 (57%) were categorized as NYHA classification III or IV. Forty-five patients (2%) died between baseline and 12-weeks follow-up. An additional 153 patients (6%) experienced other clinical events; 83 of these did not have 12-week walk distance. Mean baseline walk distance was 341 m (standard deviation: 85.7 m). Demographic, anthropometric, laboratory, and hemodynamic values were similar between groups defined by treatment allocation. 8 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Characteristics of the ten trials are presented in Table 2. Study-level percentages of female patients and patients diagnosed with CTD-related PAH were consistent across studies. Percentages for NYHA classification III/IV and black race showed more variation across studies. Does 6MWD mediate the relationship between treatment assignment and clinical events? The four criteria necessary to establish '6MWD as a mediator of the relationship between treatment assignment and development of a clinical event are listed in Table 3. For each, we found a statistically significant result in the required direction. First, assignment to active treatment vs. placebo led to greater differences in the '6MWD (mean difference in '6MWD: 22.2 m; 95% CI: 15.6 to 28.9 m). Second, greater differences in '6MWD significantly reduced the he odds of clinical events at 12-weeks follow-up (OR: 0.89; 95% CI: 0.87 to 0.91) 0.991) 1 for for or a tenten en-meter increase in '6MWD. Third, assignment to active treatment vs. placebo significantly deecr creease eas d th he re ela lati tive v oodds dd ds off cclinical linica li c l ev ven e ts aatt 12 2-weeks ks ((OR: 0. 0.4 43; 95 95% % CI CI: 0. 0.31 too 0. 00.59). 59). 59 ) decreased the relative events 12-weeks 0.43; F naall Fi l y, the effec ct ooff ttreatment reaatmeent assi siign gnme ment oon me n the ddevelopment eveelo lopm pmennt ooff a clin pm niccal eev vent w as aattenuated ttenuuatted Finally, effect assignment clinical event was with wiith h the the addition aadd ddit dd itio io on of ' '6MWD 6MWD 6M W to WD to the the model mo ode dell (OR: (OR (O R: 0.52; R: 0.52; 52; 2 95% 95% CI: CI 0.37 0 37 to 0. to 0.73). 0.73 7 ). The 73 The proportion prop pr opor op orti or tion ti on ooff he effect off treatment trea tr eatm t en tm entt on tthe h oodd he ddds of ddeveloping evel ev elop opiing ing a cl lin inic icall eeve vent nt att 12 w wee eeks ks tthat hatt wa ha wass expl p ainedd the odds clinical event weeks explained by '6MWD was 22.1% (95% CI: 12.1% to 31.1%). Additionally, the modified Sobel test confirmed the statistical significance of the mediation (Z = 4.77, p<0.001). There was no significant interaction between treatment and '6MWD (estimate and 95% CI: 0.002 (-0.002, 0.006), p=0.25). Does a threshold effect exist for '6MWD? Compared with placebo, nearly all drug/dose combinations resulted in a greater '6MWD at 12weeks follow-up (Table 4). The summary results indicate an average difference in '6MWD of 22.4 m (95% CI: 17.4 to 27.5) for assignment to active treatment relative to placebo. The effect 9 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 on reduction of clinical events was consistent across drug/dose combinations. Relative to placebo, all 21 drug/dose combinations lowered the odds of developing a clinical event at 12 weeks follow-up (summary OR: 0.44; 95% CI: 0.33 to 0.57). Figure 1 illustrates the results of our meta-regression and threshold analysis. The upper prediction interval crossed the null value for relative odds of a clinical event at a difference in '6MWD of 41.8 meters. This value indicates the minimal summary difference in '6MWD that corresponds to a statistically significant reduction in clinical events. Models including race, sex, diagnosis category, and NYHA functional classification showed no evidence of confounding and these variables were not included in the final meta-regression model. In a sensitivity analysis, we removed the four drug/dose combinations from PHIRST f fro om th thee PH PHIR IRST IR ST study, tudy, as this study was the only one to allow concomitant background therapy. Excluding this study 25.7 difference tud udyy resulted resuult re lted ed d inn a smaller s aller threshold value of 25. sm 5.77 m for the differ erren e ce iinn '6MWD. In an additional analysis, NYHA class change ad dditi dit onal ana aly lyssiss, rremoving emov ovin ingg NYH N YHA cl cla ass IV patients pattieentss (n=127) (n= (n =127) =12 27) did did not noot appreciably apprrecia iabl blly ch chan ange an ge results. Further details provided esuult lts. s Fu s. Furt rthher rt her de eta tail ilss ar il aree pr rov o id ided ed iin n th thee Supplemental Supp Su ppllem pp lement ment n al Material. Mat M ater at erria iall. Discussion This study provides the first rigorous examination of the validity of '6WMD from baseline to 12 weeks as a surrogate endpoint in trials of PAH therapies. '6MWD met all criteria as a mediator of the relationship between treatment and development of a clinical event at 12 weeks. However, the proportion of this relationship explained by 6MWD was modest at 22%, suggesting that 6MWD may not be an adequate surrogate. A threshold effect of 41.8 meters was also identified, meaning that if a drug improved 6MWD over 12 weeks by 41.8 meters more than did placebo, investigators could predict, with 95% confidence, that the drug would reduce the in clinical event 10 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 rate over 12 weeks. We found that only 4 of the 21 drug-dose combinations produced effects on '6MWD that could be said, with conventional degrees of certainty, to be associated with clinical improvements (Figure 1). If the lower threshold value of 25.7 m is used, then 5 of the remaining 17 drug-dose combinations would be considered to produce statistically significant effects on clinical outcomes in the absence of background therapy. Of these 9 total drug-dose combinations that met the lower threshold value, one involved a drug that is not approved by the FDA (sitaxsentan) and two involve dosages that are not included in FDA labeling (sildenafil 40 mg TID and sildenafil 80 mg TID). Three drugs (iloprost, tadalafil, and treprostinil) did not meet either of the threshold values. It is essential to explore the validity of surrogate endpoints because valid surrogates provide efficient studies prrov ovid idee ef id effi fici fi cien ci nt mechanisms me for early phase stu udiees of new interventions. interrve v nttio ionns. ns Specifically, trials utilizing validated surrogate endpoints conducted more quickly, sample utiliizing iz valida date teed su urrog gat atee en ndp dpoi oinnts oi nts ccan an bbee con nducteed mor ndu m ore re qqui uick ckly y, with wi h ssmaller mall ma ller ll err ssam ampl am plee sizes, risks izees, fewer few few ewer er rris isks ks to to subjects, suubjjec ects, and and reduced redu re duce cedd research ce reseear re a ch ch ccosts osstss tha tthan hann trials ha t iaalss that tr ttha haat use use true true clinical cli linnica nicaal 3 endpoints.34-35 However, Howe Ho weve we ver, ve r, only onl nlyy if surrogate ssur urrro r ga gate te endpoints end ndpo poin po in ntss are aree va vali validated lida li date da ted wi te will l tthey ll heyy cl he clearly lea earl rlyy pr rl provide thesee virtues; in the absence of validation, there is considerable risk, as shown famously in the CAST trial,36 of falsely concluding the effectiveness of a new intervention. Our data also add to a growing literature on the use of 6MWD as an outcome measure in other settings. Using different methods, 6MWD has been evaluated in idiopathic pulmonary fibrosis,37 chronic obstructive pulmonary disease,38 and cardiac rehabilitation.39 In our study, we found that the proportion of the effect of treatment on preventing clinical events explained by the change in 6MWD was 22.1%, which falls well below the 50-75% threshold for a valid surrogate described by Freedman,28 although some consider this an overly stringent criterion.15 Clearly, 11 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 PAH treatments have unmeasured effects on the outcome that are not fully captured by the change in 6MWD.40 Thus, the finding of true but modest mediation by 6MWD suggests that it may not be sufficient to use on its own. Incorporation in a combination surrogate measure with hemodynamic or other assessments might improve its performance and warrants further study. The threshold value we identified of 41.8 meters for the difference in '6MWD may be considered for use as the level of improvement in '6MWD necessary to reliably conclude that the intervention will confer clinical benefits in future trials. Using different methods and patients from a single study (the SUPER study), Gilbert et al. estimated a minimally clinically important difference of 41 m that correlated with patient-reported improvement.41 Similarly, in untreated PAH patients, Paciocco et al. found that each increase in 50 m walked was associ associated ciiat ated ed w with ithh an it an 18% reduction in mortality.42 The consistency of findings across these studies using different methods me eth thoods od supports suupp pporrts the th robustness of this result. However, How owever, '6MWD D rem remains mai ain ins an inadeq inadequate quate surrogate urrrog o ate endpoi endpoint oiintt giv given iv ven n the hee m modest oddes estt ddegree egree ooff me mediation ediatio ionn of io of tthe h ttreatment he reeatm ment eeffect. ffeect. ff t Confidence Conf Co nfid nf iden ence en ce iinn ou ourr rresults esu suult ltss st stem stems emss fr from om tthe h llarge he argge sa ar samp sample mple mp le ssiz size izze em empl employed ploy pl oyed oy ed d aand nd tthe he ffact he actt that ac that the the h treatment reatment effects efffe fect ctss on changes ct ccha hang ha nges es in in 6MWD 6MWD and and on on clinical clin cl in niccal a eevents vent ve ntss w nt were eree ccon consistent onsi on sist si sten st entt ac acro across r ss all drug ro doses.43 Nonetheless, this study has limitations. First, as with any meta-analysis, the findings are subject to errors in the conduct, data entry, or analysis of the primary data. Second, these primary trials included mostly women and whites, and used relatively short follow-up periods. We are unable to evaluate clinical endpoints that occur after 12 weeks and our results should not be generalized beyond this time period. However, the demographics represented are consistent with the broader epidemiology of PAH, and the included trials all provided similar follow-up, clinical event definitions, and outcome measurement, making them well suited for our meta-analytic approach. 12 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 All of the trials that we examined were placebo-controlled, which is an additional strength. However, one allowed concomitant background therapy. Removal of the PHIRST trial reduced our threshold value, suggesting that future trials employing background therapies may be subject to larger threshold values than those reported here. In other words, in the presence of an effective PAH therapy, an RCT of a new therapy may need to produce larger differences in the '6MWD to provide confidence that the results correspond to differences in clinical outcomes. We were unable to further explore the role of background therapy due to small sample sizes. Future research, therefore, is needed, particularly in light of ethical questions surrounding the future conduct of placebo-controlled trials in PAH.44 Finally, we used statistical techniques to help address a clinical question. Wh W While ile ou ourr threshold hreshold estimate provides a clear idea of what '6MWD would be needed to indicate that the benefits be ene nefi fits fi ts off a ttreatment reaatmen tme t will be greater than zero,, the the inference of a “cli “clinically lini niically important” ddifference iffference in outcomes outtcoome ou omes might mig ighht ht warrant war arra rannt selection ra seelecttio on off a different dif ifffere fereent threshold. thrressholld. Individual Ind ndiivid ividua uall patients paatieents ents m may ay show how w clinical ccli lini li nica ni call improvement ca im mpr prov ovem ov emen em ent without en with wi t ouut reaching th reaachi re achi hing ng a cce certain ertaain erta i ' '6MWD 6MWD 6M WD threshold thr hres eshhold hold d vval value alue al ue and and ppatients atieent atie ntss who who improve their may clinical However, mprove thei eiir 6M 6MWD WD m ay y nnot ot nnecessarily e es ec e saari rily ly y eexhibit xhiibi xh bitt cl clin i iccal iimprovement. in mpro mp roveeme ment nt. H nt ow wev ever e , th er the population-level threshold values we have established are useful in designing future clinical trials. In conclusion, we used two complementary approaches to examine the validity of '6MWD as a surrogate endpoint in clinical trials of PAH therapies. We were able to identify significant threshold effects of '6MWD that can be used to guide future RCTs, and we found that '6MWD is a mediator in the relationship between treatment and clinical outcome. However, because '6MWD does not explain a large proportion of this treatment effect, it may not be sufficient to use it as a lone surrogate endpoint. Further studies are needed to identify 13 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 combination surrogate endpoints that may have superior characteristics, and to determine if this threshold value we identified applies to trials employing background therapy or not employing placebo controls at all. Acknowledgments: We are grateful to Maximilian Herlim and to Ziyue Liu, PhD, for their invaluable help preparing the data for analysis and to Dr. Norman Stockbridge and Dr. Salma Lemtouni at the U.S. Food and Drug Administration for providing us with the data to conduct this study. Funding Sources: This work was supported by an American Thoracic Society / Pfizer Research Grant in Pulmonary Hypertension (Dr. Halpern). Dr. Kawut was supported by K24 HL103844. Neither the FDA nor the funding source had a role in the design of this study nor in the decision to submit it for publication. The FDA did review the study prior to submission as a condition of the original contract,, but did not request anyy changes g q g to our text. Conflict of Interest Disclosures: Dr. Gabler has participated in unrelated projects project ctss funded fund fu ndded by by Pfizer, Inc. Dr. Strom has served as a consultant for Abbott, Amgen, Astra Zeneca, BMS, Boehringer Orexigen, Boehring ger Ingelheim, Glaxo, Novartis, NPS Pharma, Nuvo Research, O rexigen, Pfizer, Teva, and Pfizer, Shire, an nd Vivus Vivvus Vi vus an aandd has haas funded f nded research from AstraZeneca, fu AstraZe Zeene neca, BMS, Pfize zeer, S hirre, hi re and Takeda. He has received contributions Penn’s pharmacopeidemiology training ece ceiived iv con ntrib tr but utio i ns tto io o Pe Penn nn’s ’ss ppha harm rmac acop oppei eide dem mioologgy tr trai a ning ai ng pprogram rogr ro g am ffrom gr rom ro m Abbott, A bo Ab bott ttt, Amgen, Am mge g n, Hoffman, H offfman, ff LaR LaRoche, Rocchee, N Novartis, ova vart rtis rt iss, Pf Pfiz Pfizer, izzer er, San S Sanofi anofi fii P Pasteur, asteu eurr, aand eu nd dW Wyeth. yeth yeth h. Dr. Dr. Pa P Palevsky levs vssky hhas as rreceived ecei ec e ved ved consulting co onssul u ting ffees, ees, aadvisory ee dvisooryy bo boar board arrd fe fees fees, s, sp speaking peaking ng fee fees es aand/or ndd/o /orr rresearch essearrch h fun funding ndiing ffr from rom Ac rom Acte Actelion, tellioon, Bayer, Ba aye yer, r, G GeNO, eN NO, O G Gilead, ileead ead, d, Glaxo, Gla laxoo, Pfizer, Pfiz Pf izer iz er,, United er Unit Un ited it ed Therapeutics The h rap peu utiics aand ndd L Lun Lung unng Rx. Rx Th These hes e e ro roles ole less in n nno ow way ayy impacted mpa pact cted d onn this th his analysis ana naly lysis of o the the results re of previously ppre revi viou ouslyy published publ pu blis ishe hedd st studies. tud udie ies. s Dr Dr. Ka Kawu Kawut w t ha has re rece received ceiv i ed consulting fees, fee eees, advisory adv dvis i or is oryy board boar bo ardd fees, ar fees fe ess, speaking sppea eaki king ki ng fe ffees, es,, un es uunrestricted reest stri r ct ri c ed eedu duuca cattio iona nall gr na gran ants an ts,, an ts aand/or d/or educational grants, ese sear arch ch funding fun undi ding ng from fro rom m Pfizer, Pfiz Pf izer er Actelion, Acte Ac teli lion on Bayer, Baye Ba yerr Ikaria, Ika kari riaa N ovaart ov rtis is Me Merc rckk G ilea il eadd U nite ni tedd research Novartis, Merck, Gilead, United Therapeutics, and Lung Rx. Dr. Taichman has received institutional research funding from Actelion. References: 1. Taichman DB, Mandel J. Epidemiology of pulmonary arterial hypertension. Clin Chest Med. 2007;28:1-22. 2. Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Cottin V, Degano B, Jais X, Montani D, Souza R, Simonneau G. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156-163. 3. Provencher S, Sitbon O, Humbert M, Cabrol S, Jais X, Simonneau G. Long-term outcome with first-line bosentan therapy in idiopathic pulmonary arterial hypertension. Eur Heart J. 14 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 2006;27:589-595. 4. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Herve P, Rainisio M, Simonneau G. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: Prognostic factors and survival. J Am Coll Cardiol. 2002;40:780-788. 5. Miyamoto S, Nagaya N, Satoh T, Kyotani S, Sakamaki F, Fujita M, Nakanishi N, Miyatake K. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension - comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2000;161:487-492. 6. Baker SG, Kramer BS. A perfect correlate does not a surrogate make. BMC Med Res Methodol. 2003;3:16. 7. Prentice RL. Surrogate endpoints in clinical trials: Definition and operational criteria. Stat Med. 1989;8:431-440. Surrogate 8. Ventetuolo CE, Benza RL, Peacock AJ, Zamanian RT, Badesch DB, Kawut SM. M.. S Sur urro roga g te ga 2008;5:617and combined end points in pulmonary arterial hypertension. Proc Am Thorac Soc. Soc. 20 008 08;5 ;5:6 ;5 :617 :6 17622. hypertension: 9. Snow JL,, Kawut SM. Surrogate end points in pu ppulmonary lmonary arterial hyp ypertension: Assessing the response 2007;28:75-89. esppon onsse se to to therapy. therrap th apyy. y. Clin Chest Med. 2007;28:75 75 5-8 - 9. Macchia Marchioli Marfisi Scarano Levantesi G,, Ta Tavazzi Tognoni G.. A me meta110. 0. M acchia A, A M Mar arch chio ch oli R R,, Ma M arf rffissi R, R, Sca araano M, M Lev evan ev ante t si te s G Tava vaazzzi L, T og gno noni ni G m eta analysis trials pulmonary hypertension: clinical condition drugs an nallys y is of tr tria ials ooff pu ulm monnaryy hy hype erteens ensionn: A cl lin nic ical al ccon ondditioon llooking on ookking for for dr drug gs an andd rresearch eseearrch methodology. Heart me eth thod odol od olog ogy. og y. Am mH ea artt JJ.. 2007;153:1037-1047. 20 0077;1 ;153 53:1 53 :103 03377-11047 1047 47.. DL, Brown AW, Shorr AF. Analyzing short-term effect 11. Helman D L, B rown ro wn A W, JJackson acks ac k on ks o JJL, L, S Sho horr ho rrr A F An F. nal a yz yzin ingg th in thee sh shor ortor t-te term te rm eeff ffec ff ectt of ec o placebo therapy hypertension: Potential future her erap apyy in ppulmonary ulmo ul mona nary ry aarterial rter rt eria iall hy hype pert rten ensi sion on:: Po Pote tent ntia iall implications impl im plic icat atio ions ns for for the the design desi de sign gn ooff fu futu ture re clinical trials. Chest. 2007;132:764-777. 12. Galie N, Manes A, Negro L, Palazzini M, Bacchi-Reggiani ML, Branzi A. A meta-analysis of randomized controlled trials in pulmonary arterial hypertension. Eur Heart J. 2009;30:394403. 13. Macchia A, Marchioli R, Tognoni G, Scarano M, Marfisi R, Tavazzi L, Rich S. Systematic review of trials using vasodilators in pulmonary arterial hypertension: Why a new approach is needed. Am Heart J. 2010;159:245-257. 14. Johnson KR, Freemantle N, Anthony DM, Lassere MND. Ldl-cholesterol differences predicted survival benefit in statin trials by the surrogate threshold effect (ste). J Clin Epidemiol. 2009;62:328-336. 15. Buyse M, Molenberghs G. Criteria for the validation of surrogate endpoints in randomized experiments. Biometrics. 1998;54:1014-1029. 15 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 16. MacKinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Eval Rev. 1993;17:144-158. 17. Burzykowski T, Buyse M. Surrogate threshold effect: An alternative measure for metaanalytic surrogate endpoint validation. Pharm Stat. 2006;5:173-186. 18. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, Keogh A, Oudiz R, Frost A, Blackburn SD, Crow JW, Rubin LJ. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension - a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165:800-804. 19. Galie N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, Badesch DB, McGoon MD, McLaughlin VV, Roecker EB, Gerber MJ, Dufton C, Wiens BL, Rubin LJ. Ambrisentan for the treatment of pulmonary arterial hypertension - results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (aries) study 1 and 2. Circulation. 2008;117:3010-3019. Frost Roux S,, 20. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido T, Fros osst A, R Rou ouxx S arterial hypertension. Leconte I, Landzberg M, Simonneau G. Bosentan therapy for pulmonary arteria al hy ype pert rtten ensi sion si o .N on Engl J Med. 2002;346:896-903. Olschewski Simonneau 21. Ol O schewski H,, Si S monneau G, Galie N, Higenbottam T, Naeije R, Rubin LJ, Nikkho S, Speich Spei Sp eich ei ch R, R Hoeper Ho er MM, M Behr J, Winkler J, Sitbon on O, O Popov W, Ghofrani Gho h frran anii HA, Manes A, Kiely DG, Ewert Meyer A,, Co Corris PA, Delcroix Gomez-Sanchez Siedentop Seeger DG G, Ew E ertt R, M eyer ey er A Corr rris is P A, D Del elcr croi oixx M, Go Gome ezz-Sa Sanc Sa n heez M, M, S ieede d nt ntop op H H,, Se Seeg eger eg e W, er W, the t e th Aerosolized Iloprost Randomized Study iloprost severe pulmonary hypertension. A errosolized ro Il loppro ostt Ran R an ndo domi mize mi zedd Stud S tuddy G. IInhaled nhaleed ilop opro op rosst st ffor or sse ever e e pu ulm mon onar aryy hy hype peerttensi ensi s on. Med. 2002;347:322-329. N En Engl g J Med ed. 20 002;3 347 7:322 22 2-3 329 9. Frost EM, Oudiz R,, Sh Shapiro McLaughlin Hill 22. Ba Barst RJ RJ, Langleben Lang La gle lebe b n D, D F rost ro st A, A Horn rn E M, O udizz R Shap apir i o S, M c au cL augh ghli linn V, V H ill N, Robbins Zwicke Duncan Dixon RAF, Frumkin Sitaxsentan Tapson VF,, R obbi ob bins bi ns IIM, M Z M, wick wi ke D, D Dun unca un cann B, D ca ixon ix o R on AF,, Fr AF Frum u ki um k n LR LR.. Si S taaxs xsen enta en taan therapy pulmonary arterial Respir forr pu fo pulm lmon onar aryy ar arte teri rial al hhypertension. yper yp erte tens nsio ionn Am J R espi es pirr Crit Crit Care Car aree Med. Medd 2004;169:441-447. Me 2004 20 04;1 ;169 69:4 :441 41-447 447 23. Barst RJ, Langleben D, Badesch D, Frost A, Lawrence EC, Shapiro S, Naeije R, Galie N. Treatment of pulmonary arterial hypertension with the selective endothelin-a receptor antagonist sitaxsentan. J Am Coll Cardiol. 2006;47:2049-2056. 24. Galie N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, Fleming T, Parpia T, Burgess G, Branzi A, Grimminger F, Kurzyna M, Simonneau G, Sildenafil Use in Pulmonary Arterial Hypertension Study G. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005;353:2148-2157. 25. Galie N, Brundage BH, Ghofrani HA, Oudiz RJ, Simonneau G, Safdar Z, Shapiro S, White RJ, Chan M, Beardsworth A, Frumkin L, Barst RJ. Tadalafil therapy for pulmonary arterial hypertension. Circulation. 2009;119:2894-U2865. 26. Klebanoff MA, Cole SR. Use of multiple imputation in the epidemiologic literature. Am J Epidemiol. 2008;168:355-357. 16 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 27. SAS version 9.2, SAS Institute Inc., Cary, NC. 28. Freedman LS, Graubard BI, Schatzkin A. Statistical validation of intermediate end-points for chronic diseases. Stat Med. 1992;11:167-178. 29. Huang J, Huang B. Evaluating the proportion of treatment effect explained by a continuous surrogate marker in logistic or probit regression models. Stat Biopharm Res. 2010;2:229-238 30. Efron B, Tibshirani RJ. An introduction to the bootstrap. New York: Chapman and Hall; 1993. 31. Jasti S, Dudley WN, Goldwater E. Sas macros for testing statistical mediation in data with binary mediators or outcomes. Nurs Res. 2008;57:118-122. 32. Gabler NB, French B, Strom BL, Liu Z, Palevsky HI, Taichman DB, Kawut SM, Halpern SD. Race and sex differences in response to endothelin receptor antagonists for pulmonary arterial hypertension. Chest. 2012; 141:20-26. Outcome 33. Kuhn KP, Byrne DW, Arbogast PG, Doyle TP, Loyd JE, Robbins IM. Outco ome inn 91 epoprostenol. Respir consecutive patients with pulmonary arterial hypertension receiving epoprostenol ol. Am J R Res espi pir ir Crit Care Med. 2003;167:580-586. 34. Lassere MN.. The evaluation 34 4. La Las sserre MN sser M Th biomarker-surrogacy evalua uatiion schema: A rreview ua evie ieew of o the biomarkersurrogate literature proposal criterion-based, quantitative, multidimensional urrrogate li lite teera r tu ture re aand ndd a ppro r poosa ro sall fo forr a cr crit iter erio ionn-ba based, ba d,, qqua uant ua n ittat ativve, m u tidi ul dime mens me n io ns iona nall levels schema status hhierarchical hier i rar a chical lev evel e s off eevidence viide denc ncee sc nc sche hema he ma ffor or eevaluating vaaluaatinng tthe hee sst tattus of bbiomarkers iom marke keerss aass su ssurrogate r og rr ogat atee at endpoints. en ndppoints. St Stat a Methods Methoods Med Meed Res. M Ress. 20 22008;17:303-340. 08;1 ; 7:30 303-3440. 30 0. Holland six-minute walk test: 35. Rasekaba Rasekkaba Ra b T, T, Lee Leee AL, A , Naughton AL Naug Na ught hton o MT, T, Williams Wil Williiam ams TJ, TJJ, Ho Holl llan andd AE AE.. Th The si sixx mi minu nute t w alkk te test st: A cardiopulmonary Med 2009;39:495-501. useful metricc fo forr th thee ca card r io opu pulm mon o ar aryy pa ppatient. tien ti entt. en t. In IIntern tern te rnn M ed JJ.. 20 2009 0 ;3 09 39: 9:49 49549 5 50 55 1. 1 36. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson DW, and the CAST Investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The cardiac arrhythmia suppression trial. N Engl J Med. 1991;324:781-788. 37. du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, Lancaster L, Noble PW, Sahn SA, Szwarcberg J, Thomeer M, Valeyre D, King TE, Jr. Six-minute-walk test in idiopathic pulmonary fibrosis: Test validation and minimal clinically important difference. Am J Respir Crit Care Med. 2011;183:1231-1237. 38. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: The six minute walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155:1278-1282. 39. Hamilton DM, Haennel RG. Validity and reliability of the 6-minute walk test in a cardiac rehabilitation population. J Cardiopulm Rehabil. 2000;20:156-164. 17 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 40. Fleming TR, DeMets DL. Surrogate end points in clinical trials: Are we being misled? Ann Intern Med. 1996;125:605-613. 41. Gilbert C, Brown MC, Cappelleri JC, Carlsson M, McKenna SP. Estimating a minimally important difference in pulmonary arterial hypertension following treatment with sildenafil. Chest. 2009;135:137-142. 42. Paciocco G, Martinez FJ, Bossone E, Pielsticker E, Gillespie B, Rubenfire M. Oxygen desaturation on the six-minute walk test and mortality in untreated primary pulmonary hypertension. Eur Respir J. 2001;17:647-652. 43. Buyse M, Molenberghs G, Burzykowski T, Renard D, Geys H. The validation of surrogate endpoints in meta-analyses of randomized experiments. Biostatistics. 2000;1:49-67. 44. Halpern SD, Doyle R, Kawut SM. The ethics of randomized clinical trials in pulmonary arterial hypertension. Proc Am Thorac Soc. 2008;5:631-635. 18 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Table 1. Characteristics of study participants; summaries provided as median (Q1-Q3) unless otherwise indicated by n (%). Characteristic Age, years Male, n (%) Race, n (%) White Black Other Height, cm Weight, kg BMI, kg/m2 PAH diagnosis, n (%) Idiopathic Connective tissue disease HIV infection / anorexigen use Congenital heart disease NYHA functional classification, n (%) I/II III/IV Baseline hemodynamics M eann ri ea rright ghtt at gh tri rial a ppressure, al ressure, mmHg Mean atrial Mea M ean pu ulm monnar ary y arterial pressure, mmHg Mean pulmonary Cardiac ooutput, utpu ut putt, L pu /m min Cardiac L/min Cardiac index, L/min/m C ardiac ind dex x, L /m min//m2 Pulmonary capillary wedge mmHg Pulmonaary y ca apillary yw ed dge ge ppressure, resssur re urre, m mH Hg Pulmonary resistance, Wood Units Pul P ulmo ul mona narry na ry vvascular asccula cularr re esi sist s an ncee, W ood Un ood Unit itss it Baseline Ba ase seli line in laboratory lab laborrat atory y values valluess va Hemoglobin, g/dL Hemoglo H lobi bin, n,, g g/d /dL L Sodium, mEq/L Sod S odiu ium, m, mEq m Eq//L /L Warfarin use, n (%) Baseline 6MWD, m Study, n (%) ARIES-1 ARIES-2 BREATHE-1 AIR SUPER STRIDE-1 STRIDE-2 STRIDE-4 PHIRST Treprostinil Active treatment (n=1563) 50 (38-61) 335 (21) Placebo (n=841) 49 (37-60) 192 (23) 1244 (80) 86 (6) 221 (14) 163 (157-169) 69.4 (59.0-82.1) 25.5 (22.5-30.0) 678 (81) 39 (5) 118 (14) 163 (157-170) 70.1 (60.6-83.9) 26.1 (22.9-30.4) 946 (62) 388 (25) 41 (3) 155 (10) 508 (62) 193 (24) 18 (2) (12) 97 ((12 12)) 628 (41) 917 (59) 389 38 9 (4 (47) 7) 432 (53) 8.0 (5.0-12.0) 0)) 52.0 (43.0 .0-62 .0 2.0 0) (43.0-62.0) 4.0 (3 4.0 3.2 .2-5 -5.1 5.1 . ) (3.2-5.1) 22.4 .4 4 (1 ((1.9-3.1) .9--3.1)) (6.0-12.0) 99.0 .0 0 (6. .0-12.0)) (7.1-16.8) 10.99 ((7 10 7.1--16 16.8 8) 88.0 .0 (5.0-12.0) 54.0 ((45.0-64.5) 45.0-64.5) 3.9 3. 9 (3 (3.2 .2-4 .2 -4.9 .9) 9) (3.2-4.9) 2. 2.3 .3 ((1.9-3.1) 1.9 9-3 -3..1) 99.0 .00 ((6.0-12.0) 6.0 0-12..0)) 111.2 1.2 (7.5 1.2 ((7.5-16.0) 7 5-1 -166.0) 0) 14.7 ((13.4-16.0) 14.7 13.4 13 .4-1 -1 16. 6.0) 0)) 140 14 40 (138-142) (138 (1 38-1 -142 42)) 42 860 (59) 356 (287-408) (13.3-16.0) 114.6 14. 4.6 6 (1 (13 3.3 3-16 16.0) 0) 140 14 40 (138-142) (138 (1 38-1 142 42)) 470 (64) 352 (276-410) 134 (9) 127 (8) 145 (9) 101 (6) 204 (13) 118 (8) 123 (8) 64 (4) 314 (20) 233 (15) 67 (8) 65 (8) 69 (8) 101 (12) 65 (8) 60 (7) 62 (7) 34 (4) 81 (10) 237 (28) BMI, body mass index; HIV, human immunodeficiency virus; NYHA, New York Heart Association ; ARIES, Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies; AIR, Aerosolized Iloprost Randomized;BREATHE, Bosentan: Randomized Trial of Endothelin receptor Antagonist Therapy; STRIDE, Sitaxsentan To Relieve Impaired Exercise; SUPER, Sildenafil Use in Pulmonary Hypertension; PHIRST, Pulmonary Arterial Hypertension and Response to Tadalafil 19 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Table 2. Characteristics of participating studies and drug/dose combinations Study Drug and dose N Ambrisentan 5 mg Ambrisentan 10 mg Placebo 67 67 67 ARIES-1 ARIES-2 Clinical events 10 Study Level Statistics % NYHA % female % black III/IV 84 7.3 65 % CTD 31 20 74 0 54 32 9 79 7.1 100 22 41 67 1.5 100 23 7 79 8.1 67 2244 8 77 13.1 13 63 29 2 84 84 6.7 67 6. 39 1155 17 76 2.6 61 30 39 78 9.7 67 24 45 81 5.3 7 19 Ambrisentan 2.5 mg 64 Ambrisentan 5 mg 63 Placebo 65 BREATHE-1 Bosentan 125 mg Bosentan 250 mg Placebo 75 70 69 Iloprost Placebo 101 101 Sitaxsentan 100 mg Sitaxsentan 300 mg Placebo Pla laace cebo b 55 63 60 AIR STRIDE-1 STRIDE-2 ST TRI RID DE 2 DE-2 Sitaxsentan Sita Si taxs ta x en xs enta tan ta n 50 mg mg Sitaxsentan Sittax Si xsen enta tan n 100 100 mg mg Placebo Pla acebo 61 662 2 662 2 Sitaxsentan Sitaxs Si xsen entan n 50 5 mg mg Sitaxsentan Sita Si taxs xsen enta tan n 10 100 0 mg g Placebo P lacebo lace b bo 32 32 3 2 334 4 Sildenafil 20 mg Sildenafil 40 mg Sildenafil 80 mg Placebo 68 65 71 65 STRIDE-4 ST TRI R DE DE-4 -4 SUPER PHIRST Tadalafil 2.5 mg Tadalafil 10 mg Tadalafil 20 mg Tadalafil 40 mg Placebo 79 79 81 75 81 Treprostinil Treprostinil Placebo 233 237 20 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Table 3. Criteria to establish change in 6MWD as a mediator Criteria to establish '6MWD as a mediator in the relationship Results* between treatment assignment and development of a clinical event at 12-weeks follow-up Mean difference: 22.4 Treatment assignment has a significant effect on '6MWD from (95% CI: 15.9, 28.9) baseline to 12-weeks follow up Odds ratio: 0.89 per ten meters '6MWD has a significant effect on the odds of developing a (95% CI: 0.87, 0.91) clinical event Treatment assignment has a significant effect on the odds of Odds ratio: 0.43 developing a clinical event at 12-weeks follow-up (95% CI: 0.31, 0.59) The effect of treatment assignment on the odds of developing a Odds ratio: 0.52 clinical event (compare with above) is attenuated with the addition (95% CI: 0.37, 0.73) of '6MWD to the model * All models include adjustment for study and baseline walk; assignment to placebo is the reference for all models that included treatment. Table 4. Drug/dose-specific placebo-adjusted results Study Drug and dose ARIES-1 AR RIE IES S-1 S-1 Am Ambrisentan 5 mg Ambrisentan A Am bris br isen is enta en tann 100 mg ta mg Ambrisentan A Ambr mbr bris iseenta enta tann 2.5 2.5 mg A Ambrisentan mbrriseentaan 5 mgg B Bosentan ose senntaan an 125 255 m mg g Bosentan mg Bose Bo seent ntan an 250 250 0m g Ilop Il Iloprost opro op rost ro st Sitaxsentan mg S itax it axse ax sent n an nt n 1100 0 m 00 g Sit Si Sitaxsentan t 30 3000 mg Sitaxsentan 50 mg Sitaxsentan 100 mg Sitaxsentan 50 mg Sitaxsentan 100 mg Sildenafil 20 mg Sildenafil 40 mg Sildenafil 80 mg Tadalafil 2.5 mg Tadalafil 10 mg Tadalafil 20 mg Tadalafil 40 mg Treprostinil ARIES-2 A RIIES-2 IE BR BREATHE-1 REA ATH THEE1 AIR AI R STRIDE-1 STRIDE-2 STRIDE-4 SUPER PHIRST Difference in '6MWD, m (95% CI) OR for clinical events (95% CI) Meta regression weight 24.9 (0.32, (0.3 (0 .322, 49.4) 41.4 41.4 (15.6, ((155.66, 67.2) 67.2 .2) 2) 37.3 (8.2, 337 7.3 (8 8.2 2, 66.3) 66 6.3 3) 53.6 53..6 (24.4, (2 24. 4.44, 82.8) 82. 2.8) 8) 33.4 33 4 ((8.6, 8.66, 6, 558.3) 8.33) 8. 3) 46.3 (21.1, 71.6) 46 .3 3 ((21 21.1, 1, 71 1.6 .6) 6) 24 24.5 .5 5 ((-2.4, -22.4, 4 51 51.3) .3) 3) 33.3 33 .3 3 ((9.1, 9 1, 9. 1 57.4) 57..4) 224.6 4 6 ((-0.45, 0 45 49 49.7) 7) -7.1 (-27.6, 13.5) 15.2 (-4.7, 35.1) -19.1 (-49.9, 11.8) 6.9 (-23.5, 37.5) 39.3 (15.0, 63.6) 45.2 (20.6, 69.8) 42.1 (18.0, 66.3) -0.3 (-20.7, 20.0) 17.1 (-4.3, 38.5) 24.6 (5.1, 44.1) 18.2 (-2.2, 38.6) 9.9 (-6.7, 26.4) 22.4 (17.4, 27.5) 00.58 . 8 (0 .5 (0.13, 0.1 .13 13, 2.53) 0.38 0.38 ((0. (0.07, 0.07 0 , 2. 07 2.04 2.04) 04 4) 1.12) 0.35 0. 35 ((0.11, 0 111, 1. 0. .122) 0.22 0.22 (0 (0.06, 0.0 06, 00.88) .8 88) 00.58 .58 (0 (0.12 (0.12, 2, 22.80) .80) .8 0 0) 00.42 0. .42 42 ((0.07, 0 07 0. 07,, 22.47) .47 47)) 47 0.47 0.47 47 ((0 (0.23, 0.23 23, 00.96) 23 .96 96)) 96 (0.02, 00.20 .220 (0 (0.0 .0 02, 2 11.99) .99) .9 9) 00.36 36 ((0.06, 0 06 22.15) 15)) 15 0.54 (0.09, 3.20) 0.77 (0.13, 4.72) 0.71 (0, 4.42) * 0.73 (0, 2.07) * 0.36 (0.09, 1.47) 0.25 (0.05, 1.28) 0.59 (0.17, 1.98) 0.49 (0.18, 1.34) 0.30 (0.10, 0.90) 0.59 (0.23, 1.51) 0.27 (0.08, 0.90) 0.52 (0.27, 0.99) 0.44 (0.33, 0.57) 1.8 1. 1.4 .4 22.8 2. .88 2.1 11.5 .5 11.2 1. 2 77.3 .33 00.7 .7 11.2 2 1.2 1.2 < 0.1 < 0.1 1.9 1.5 2.6 3.8 3.1 4.4 2.7 9.2 Treprostinil Summary † CI, confidence interval Reference group is the placebo group in each study All analyses are adjusted for baseline walk distance * Obtained from exact logistic regression † Obtained from fixed-effects meta-analysis (p-value for heterogeneity = 0.99) 21 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 DOI: 10.1161/CIRCULATIONAHA.112.105890 Figure Legend: Figure. Results of the meta-regression analysis showing the relationship between changes in 6MWD between baseline and 12-weeks follow-up at the drug/dose level by study on the odds of a clinical event at 12-weeks. The circles each represent a drug/dose combination, with sizes proportionate to study weights (detailed in Table 4, and based on inverse variance weighting). The shaded grey area corresponds to the bounds of the 95% prediction intervals. The threshold value is indicated on the horizontal axis at 41.8 m. 22 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 Validation of Six-Minute-Walk Distance as a Surrogate Endpoint in Pulmonary Arterial Hypertension Trials Nicole B. Gabler, Benjamin French, Brian L. Strom, Harold I. Palevsky, Darren B. Taichman, Steven M. Kawut and Scott D. Halpern Circulation. published online June 13, 2012; Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/early/2012/06/11/CIRCULATIONAHA.112.105890 Data Supplement (unedited) at: http://circ.ahajournals.org/content/suppl/2012/06/11/CIRCULATIONAHA.112.105890.DC1.html http://circ.ahajournals.org/content/suppl/2013/10/02/CIRCULATIONAHA.112.105890.DC2.html Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/ Downloaded from http://circ.ahajournals.org/ by guest on July 11, 2016 SUPPLEMENTAL MATERIAL: (1) Supplemental Table 1: Clinical event definitions by study Study name: Clinical event definition: - Death - Lung or heart transplantation - Hospitalization for PAH - Refractory systolic arterial hypotension AIR - Worsening right heart failure - Rapidly progressive cardiogenic, hepatic or renal failure - Addition of new PAH medication - A decline in measure of hemodynamic function ARIES-I ARIES-II BREATHE-1 PHIRST STRIDE-I STRIDE-II - Death - Lung transplantation - Hospitalization for PAH - Atrial septostomy - Addition of other PAH therapeutic agents - An increase of 1 or more WHO functional class - Worsening right ventricular failure - Rapidly progressing cardiogenic, hepatic, or renal failure - Refractory systolic hypotension - Death - Lung transplantation - Hospitalization for PAH - Atrial septostomy - Addition of other PAH therapeutic agents - An increase of 1 or more WHO functional class - Worsening right ventricular failure - Rapidly progressing cardiogenic, hepatic, or renal failure - Refractory systolic hypotension - Death - Lung transplantation - Hospitalization for worsening PAH - Atrial septostomy - Lack of clinical improvement leading to discontinuation - Need for epoprostenol therapy - Death - Lung transplantation - Atrial septostomy - Hospitalization due to worsening PAH - Initiation of new PAH therapy - Worsening WHO functional class - Death - Epoprostenol use - Atrial septostomy - Need for lung transplantation - Death - Hospitalization for worsening PAH STRIDE-IV SUPER Treprostinil - Atrial septostomy - Need for heart/lung or lung transplantation - Addition of any new type of chronic PAH treatment due to worsening PAH - Death - Hospitalization for worsening PAH - Need for heart/lung or lung transplantation - Atrial septostomy - Addition of any new type of chronic PAH treatment due to worsening PAH - Death - Hospitalization due to worsening PAH - Lung transplantation - Addition of additional medication due to worsening PAH - Death - Lung transplantation - Clinical deterioration (2) Results of sensitivity analysis removing NYHA class IV patients. Our data included 127 (5%) patients who were NYHA class IV. These patients accounted for 25 (13%) of the clinical events. Removing the NYHA class IV patients does not appreciably change any of the results (Supplemental Table 1). The proportion of the effect of treatment on the odds of developing a clinical event at 12 weeks that was explained by ∆6MWD was 20.4% (95% CI: 9.8% to 30.3%) after removing these patients, rather than 22.1% among the full cohort. Additionally, we found a threshold effect value of 49.3 m, slightly larger than the threshold effect of 41.8 m found among the full cohort. Supplemental Table 2: Criteria to establish ∆6MWD as a mediator, data excludes NYHA class IV patients Criteria to establish ∆6MWD as a mediator in the relationship between treatment assignment and development of a clinical event at 12-weeks follow-up Results Treatment assignment has a significant effect on ∆6MWD from baseline to 12-weeks follow-up Mean difference: 22.5 ∆6MWD has a significant effect on the odds of developing a clinical event Odds ratio: 0.89 per 10 m Treatment assignment has a significant effect on the odds of developing a clinical event as 12-weeks follow-up Odds ratio: 0.39 The effect of treatment assignment on the odds of developing a clinical event (compare with above) is attenuated with the addition of ∆6MWD to the model (95% CI: 15.9, 29.1) (95% CI: 0.87, 0.91) (95% CI: 0.28, 0.55) Odds ratio: 0.48 (95% CI: 0.33, 0.68) (3) Results of sensitivity analysis removing patients participating in the PHIRST trial. Removing the PHIRST patients from the mediation analysis did not change the results reported in the manuscript (Supplemental Table 2). The proportion of the effect of treatment on the odds of developing a clinical event at 12 weeks that was explained by ∆6MWD was 24.6% (95% CI: 12.1% to 37.1%), compared with 22.1%. Supplemental Table 3: Criteria to establish ∆6MWD as a mediator, data excludes PHIRST trial Criteria to establish ∆6MWD as a mediator in the relationship between treatment assignment and development of a clinical event at 12-weeks follow-up Results Treatment assignment has a significant effect on ∆6MWD from baseline to 12-weeks follow-up Mean difference: 23.3 (95% CI: 16.0, 30.7) ∆6MWD has a significant effect on the odds of developing a clinical event Odds ratio: 0.88 per 10 m (95% CI: 0.86, 0.90) Treatment assignment has a significant effect on the odds of developing a clinical event at 12-weeks follow-up Odds ratio: 0.43 (95% CI: 0.31, 0.62) The effect of treatment assignment on the odds of developing a clinical event (compare with above) is attenuated with the addition of ∆6MWD to the model Odds ratio: 0.53 (95% CI: 0.36, 0.78) As reported in the manuscript, excluding this study resulted in a smaller threshold value of 25.7 meters. Artículo original Validación de la distancia recorrida en 6 minutos como variable de valoración sustitutiva en los ensayos realizados en la hipertensión arterial pulmonar Nicole B. Gabler, PhD, MPH, MHA; Benjamin French, PhD; Brian L. Strom, MD, MPH; Harold I. Palevsky, MD; Darren B. Taichman, MD, PhD; Steven M. Kawut, MD, MS; Scott D. Halpern, MD, PhD Antecedentes—Casi todos los tratamientos existentes para la hipertensión arterial pulmonar han sido aprobados basándose en el cambio producido en la distancia recorrida en 6 minutos (Δ6MWD) como variable de valoración clínicamente importante, pero no se ha demostrado nunca la validez de esta variable de valoración sustitutiva. El objetivo de este análisis fue validar la diferencia del Δ6MWD respecto a la probabilidad de aparición de un evento clínico en los ensayos realizados en la hipertensión arterial pulmonar. Métodos y resultados—En primer lugar, con objeto de determinar si el Δ6MWD entre la situación basal y el examen realizado al cabo de 12 semanas intervenía en la relación entre la asignación del tratamiento y la aparición de eventos clínicos, llevamos a cabo un análisis combinado de los datos a nivel de paciente, de 10 ensayos controlados con placebo y aleatorizados presentados anteriormente a la Food and Drug Administration de EEUU (n = 2.404 pacientes). En segundo lugar, para identificar un efecto umbral en el Δ6MWD que indicara una reducción estadísticamente significativa de los eventos clínicos, llevamos a cabo una metarregresión en 21 combinaciones de fármacos/niveles de dosis. El Δ6MWD explicó el 22,1% (intervalo de confianza del 95%, 12,1%– 31,1%) del efecto del tratamiento (p < 0,001). El metanálisis mostró una diferencia media de Δ6MWD de 22,4 m (intervalo de confianza del 95%, 17,4 –27,5 m), favorable al tratamiento activo en comparación con placebo. El tratamiento activo redujo la probabilidad de un evento clínico (odds ratio de resumen, 0,44; intervalo de confianza del 95%, 0,33– 0,57). La metarregresión puso de relieve la existencia de un efecto umbral significativo para un valor de 41,8 m. Conclusiones—Nuestros resultados sugieren que el Δ6MWD no explica una gran parte del efecto del tratamiento, tiene una validez tan solo modesta como variable de valoración sustitutiva de los eventos clínicos, y puede no ser un parámetro de valoración sustitutivo suficiente. Serán necesarias nuevas investigaciones para determinar si el valor umbral de 41,8 m es válido para los resultados a largo plazo o si difiere en los distintos ensayos que utilizan el tratamiento de base o carecen por completo de controles con placebo. (Traducido del inglés: Validation of 6-Minute Walk Distance as a Surrogate End Point in Pulmonary Arterial Hypertension Trials. Circulation. 2012;126:349-356.) Palabras clave: hypertension, pulmonary ■ meta-analysis ■ statistics ■ trials L a hipertensión arterial pulmonar (HAP) es una enfermedad progresiva que lleva a la insuficiencia cardiaca derecha y a la muerte1,2. Siete fármacos desarrollados en los últimos 20 años han resultado eficaces para mejorar la distancia recorrida en 6 minutos (6MWD) en los pacientes con HAP y basándose en ello, han sido autorizados para su uso en EEUU. Aunque la 6MWD es considerada por los organismos reguladores una variable de valoración clínicamente importante de por sí, varios estudios han indicado que los pacientes que alcanzan una mayor mejora de la 6MWD (o que llegan a determinados valores absolutos de la 6MWD) presentan mejores resultados clínicos3–5; sin embargo, estos datos observacionales son insuficientes para determinar si la 6MWD constituye o no una variable de valoración válida sustitutiva de los eventos clínicos6–9. Recibido el 9 de diciembre de 2011; aceptado el 16 de mayo de 2012. Center for Clinical Epidemiology and Biostatistics and Department of Biostatistics and Epidemiology (N.B.G., B.F., B.L.S., S.M.K., S.D.H.); Leonard Davis Institute of Health Economics (B.F., B.L.S., S.D.H.); Pulmonary, Allergy, and Critical Care Division (H.I.P., D.B.T., S.M.K., S.D.H.); y Pulmonary Vascular Disease Program of the Penn Cardiovascular Institute (H.I.P., D.B.T., S.M.K., S.D.H.), Perelman School of Medicine, University of Pennsylvania, Filadelfia, PA. El suplemento de datos de este artículo, disponible solamente online, puede consultarse en http://circ.ahajournals.org/lookup/suppl/doi:10.1161/ CIRCULATIONAHA.112.105890/-/DC1. Remitir la correspondencia a Nicole B. Gabler, PhD, Perelman School of Medicine, University of Pennsylvania, 708 Blockley Hall, 423 Guardian Dr, Philadelphia, PA 19104-6021, EEUU. Correo electrónico [email protected] © 2012 American Heart Association, Inc. Puede accederse a la versión original de Circulation en http://circ.ahajournals.org 4 DOI:10.1161/CIRCULATIONAHA.112.105890 Gabler y cols. Validación de la distancia recorrida en 6 minutos 5 Véase la Editorial en la página 1 Véase la Perspectiva Clínica en la página 12 La determinación de la validez de la 6MWD como variable de valoración sustitutiva en los ensayos realizados en la HAP es especialmente oportuna teniendo en cuenta los resultados contradictorios obtenidos en metanálisis recientes10–13. Aunque algunas de estas contradicciones pueden deberse a un tamaño muestral o un seguimiento insuficiente o a limitaciones intrínsecas de los metanálisis realizados a nivel de estudios, estas diferencias sugieren también la posibilidad de que la 6WMD sea una mala variable sustitutiva indirecta. En el presente estudio, hemos utilizado 2 enfoques complementarios para validar la 6MWD14–17. En primer lugar, empleamos los datos procedentes de pacientes de todos los ensayos clínicos aleatorizados de fase 3, existentes, y presentados para la aprobación de fármacos, con objeto de determinar si los cambios de la 6MWD (Δ6MWD) intervienen en la relación entre la asignación del tratamiento y los resultados clínicos. En segundo lugar, cuantificamos el grado en el que los efectos del tratamiento sobre el Δ6MWD predecía los efectos del tratamiento sobre los resultados centrados en el paciente, con el objetivo de determinar si existe un umbral del Δ6MWD que en caso de ser superado permita a los investigadores predecir que se producirán unos resultados clínicos superiores en futuros ensayos. Métodos Población en estudio A través de un contrato de la Food and Drug Administration (FDA) de EEUU con uno de los autores (S.D.H.), obtuvimos los datos de los pacientes individuales desidentificados de todos los participantes en ensayos aleatorizados y controlados con placebo de fase 3 presentados a la FDA hasta 2008 en los que se evaluaron prostanoides, antagonistas de los receptores de la endotelina o inhibidores de la fosfodiesterasa. En once ensayos clínicos se examinaron 7 fármacos (ambrisentán, bosentán, sitaxentán, iloprost, treprostinilo, sildenafilo y tadalafilo). Excluimos 1 estudio (ensayo BREATHE-2, el Bosentan Randomized Trial of Endothelin Antagonist Therapy for HAP) por que incluía tan solo 33 participantes y no era un ensayo de fase 3. Se ha presentado información adicional de los ensayos en otras publicaciones18–25. Incluimos intencionadamente ensayos de tratamientos que no fueron aprobados por la FDA (por ejemplo, sitaxentán) a causa de una toxicidad inaceptable con las dosis efectivas o del uso de dosis que se determinó que no eran efectivas. Tanto en los análisis de mediador como los de umbral cabría prever un sesgo si incluyéramos tan solo los tratamientos aprobados por la FDA, y las conclusiones obtenidas no serían útiles para el diseño de futuros ensayos ni para las decisiones de las autoridades reguladoras. Todos los ensayos incluidos describían una metodología similar, incluida la evaluación de los resultados y la obtención de datos en un seguimiento de 12 semanas. Eventos clínicos Los eventos clínicos fueron cualquiera de los siguientes antes del final del ensayo: muerte, trasplante de pulmón, septostomía auricular, hospitalización a causa de agravamiento de la HAP, abandono por agravamiento de insuficiencia cardiaca derecha o adición de otras medicaciones para la HAP. No consideramos que un deterioro de la 6MWD constituyera un evento clínico, ya que esta era la variable de valoración sustitutiva que pretendíamos validar. Se presenta una información adicional en la Tabla I del Suplemento de Datos Online. Distancia recorrida en seis minutos El cambio de la 6MWD se calculó mediante la diferencia en metros entre la distancia recorrida en la situación basal y la observada a las 12 semanas. La 6MWD basal se registró a las 2 semanas de la asignación aleatoria o dentro de este periodo de tiempo. En todos los análisis, a los pacientes para los que no se dispuso de la 6WMD a las 12 semanas porque habían fallecido durante el ensayo (n = 45, 2%) se les asignó un valor de 0. Optamos por ese valor para reflejar el hecho de que las muertes son eventos clínicos de extraordinaria importancia y para mantener la uniformidad con la medida empleada en la mayoría de los ensayos incluidos en nuestro análisis. Utilizamos imputaciones múltiples26 para los valores de los pacientes que sobrevivieron pero para los que no se dispuso de la 6MWD a las 12 semanas (n = 182, 8%). El modelo de imputación incluía variables asociadas a los eventos clínicos, es decir: 6MWD basal, edad, sexo, peso, raza, altura, categoría diagnóstica (idiopática, enfermedad del tejido conjuntivo, infección por VIH/uso de anorexígenos o cardiopatía congénita), 6MWD en el seguimiento a las 4 o 6 semanas, clasificación funcional de la New York Heart Association (NYHA), uso de warfarina, sodio basal, gasto cardiaco y presión arterial pulmonar media. Se imputaron cinco conjuntos de datos. Todas las imputaciones se llevaron a cabo en el programa SAS versión 9.2. Análisis de mediador Utilizamos una metodología estándar para determinar si el Δ6MWD interviene en la relación entre la asignación del tratamiento y la aparición de eventos clínicos en el seguimiento de 12 semanas15,16. Definimos la asignación del tratamiento como tratamiento activo o placebo. Realizamos un análisis de regresión para evaluar las siguientes 4 hipótesis: (1) La asignación del tratamiento tiene un efecto significativo sobre el Δ6WMD a las 12 semanas respecto al valor basal. (2) El Δ6MWD tiene un efecto significativo sobre la probabilidad de sufrir un evento clínico. (3) La asignación del tratamiento tiene un efecto significativo sobre la probabilidad de sufrir un evento clínico. (4) El efecto de la asignación del tratamiento sobre la probabilidad de sufrir un evento clínico se atenúa cuando se añade al modelo el Δ6MWD. Era necesario rechazar la hipótesis nula en los 4 casos para respaldar el papel del Δ6MWD como mediador/variable de valoración sustitutiva. Utilizamos una regresión logística o lineal para los parámetros binarios y continuos, respectivamente. En todos los modelos de regresión se introdujo un ajuste respecto al estudio con objeto de tener en cuenta las diferencias existentes a nivel de estudio en la asignación del tratamiento y respecto a la distancia recorrida basal para tener en cuenta las diferencias existentes a nivel de paciente en el riesgo de eventos clínicos. No se aplicó ningún otro ajuste, ya que los pacientes fueron asignados aleatoriamente a los grupos de tratamiento o placebo. Tras rechazar la hipótesis nula para las 4 hipótesis indicadas, determinamos la parte de la variabilidad que se explicaba por el Δ6MWD en la relación entre la asignación del tratamiento y la aparición de un evento clínico27,28. Utilizamos un modelo lineal generalizado con una función de enlace logit (Logit link) para cuantificar la relación entre la asignación del tratamiento y la log-odds (logit de la probabilidad de presentar un evento clínico), con un ajuste respecto al estudio y a la distancia recorrida en la situación basal (modelo “reducido”). A continuación añadimos al modelo el Δ6MWD (modelo “completo”). El posterior cambio del coeficiente de asignación de tratamiento entre los modelos reducido y completo indicó la parte de la variabilidad explicada por el Δ6MWD. Se utilizó un método de remuestreo bootstrap para establecer un intervalo de confianza (IC) del cambio porcentual. Se obtuvieron estimaciones del cambio porcentual para cada conjunto de datos de remuestreo, y se utilizó la desviación estándar de las estimaciones realizadas en 1.000 conjuntos de datos de remuestreo como error estándar29. 6 Circulation Enero, 2013 Además, utilizamos una prueba de Sobel modificada para determinar si la cantidad de mediación era estadísticamente significativa; la prueba modificada tenía en cuenta el hecho de que la variable de valoración sustitutiva (continua) y el resultado clínico (binario) se expresaban en escalas diferentes16,30. Evaluamos el supuesto de que no hubiera ninguna modificación del efecto entre el tratamiento y el mediador30 mediante un ajuste de un modelo de regresión logística para los eventos clínicos, con un término de interacción entre la asignación del tratamiento y el Δ6MWD. Análisis de efecto umbral A continuación realizamos un metanálisis y metarregresión a nivel de ensayo para determinar la relación del efecto del tratamiento sobre el mediador (Δ6MWD) con el efecto del tratamiento sobre la probabilidad de sufrir un evento clínico en un seguimiento de 12 semanas. Este análisis de umbral se llevó a cabo en 4 pasos. En primer lugar, estimamos los valores de la variable de exposición, el Δ6MWD a nivel de estudio, con un ajuste respecto al placebo, mediante la realización de regresiones lineales dentro de cada ensayo. En estas regresiones a nivel de paciente, específicas para cada ensayo, la variable de exposición fue el tratamiento (fármaco y dosis), que se introdujo en forma de variables indicadoras (con el placebo como referencia). La variable de resultado fue el Δ6MWD, y nuevamente se utilizó un ajuste respecto a la 6WMD basal. En segundo lugar, estimamos los valores del resultado, la logodds a nivel de estudio, con un ajuste para el placebo, de sufrir un evento clínico entre la situación basal y el seguimiento de 12 semanas, utilizando análisis de regresión logística dentro de cada ensayo. En estas regresiones a nivel de paciente y específicas para cada ensayo, el tratamiento (fármaco y dosis, entraron en forma de variables indicadoras, con el placebo como referencia) fue la exposición, el evento clínico (sí o no) fue el resultado, y se introdujo un ajuste respecto a la 6MWD basal. Se utilizó una regresión logística exacta cuando el número de eventos clínicos de un estudio era bajo. En tercer lugar, utilizamos las 21 combinaciones de fármaco/ dosis en comparación con placebo de todos los ensayos en una metarregresión de efectos fijos que relacionaba la diferencia estimada de Δ6MWD con el valor estimado de log odds ratio (OR) para los eventos clínicos. Se utilizó el cuadrado del inverso del error estándar como factor de ponderación para tener en cuenta la incertidumbre en la estimación del log OR. Determinamos el efecto umbral mediante el cálculo de las franjas de predicción del 95% alrededor de la línea de metarregresión. El umbral se calculó determinando el valor de la diferencia de Δ6MWD en el lugar en el que la franja de predicción superior cortaba el valor nulo de 1,0 para la probabilidad relativa de un evento clínico. Las franjas de predicción cuantifican la incertidumbre existente en la predicción de la diferencia de agravamiento clínico en un solo ensayo dada una diferencia definida del Δ6MWD. La linealidad del modelo de regresión final se evaluó con un método de diagnóstico de regresión estándar. Por último, intentamos determinar si las características de los pacientes a nivel de estudio introducían una confusión en la asociación entre el Δ6MWD y las probabilidades relativas de eventos clínicos. Los posibles factores de confusión se decidieron a priori en función de las diferencias conocidas de la respuesta al tratamiento según la raza y el sexo31 y según el diagnóstico y la clasificación funcional de la NYHA32. En consecuencia, las covariables de nuestro modelo de regresión fueron las siguientes: raza (porcentaje de raza negra), sexo (porcentaje de mujeres), categoría diagnóstica de la HAP (porcentaje de casos asociados al tejido conjuntivo) y clasificación funcional de la NYHA (porcentaje de clase III o IV). Si un posible factor de confusión modificaba el coeficiente de la variable de tratamiento en ≥ 10%, se mantenía en el modelo final. Tabla 1. Características de los participantes en el estudio Característica Tratamiento activo (n 1.563) Edad, años 50 (38 – 61) Varones, n (%) 335 (21) Raza, n (%) Blancos 1.244 (80) Negros 86 (6) Otros 221 (14) Altura, cm 163 (157–169) Peso, kg 69,4 (59,0–82,1) IMC, kg/m2 25,5 (22,5–30,0) Diagnóstico de HAP, n (%) Idiopática 946 (62) Enfermedad del tejido conjuntivo 388 (25) Infección por VIH/uso de anorexígenos 41 (3) Cardiopatía congénita 155 (10) Clasificación funcional de la NYHA, n (%) I/II 628 (41) III/IV 917 (59) Hemodinámica basal Presión auricular derecha 8,0 (5,0–12,0) media, mmHg Placebo (n 841) 49 (37– 60) 192 (23) 678 (81) 39 (5) 118 (14) 163 (157–170) 70,1 (60,6–83,9) 26,1 (22,9–30,4) 508 (62) 193 (24) 18 (2) 97 (12) 389 (47) 432 (53) 8,0 (5,0–12,0) Presión arterial pulmonar media, mmHg 52,0 (43,0–62,0) 54,0 (45,0–64,5) Gasto cardiaco, L/min Índice cardiaco, L/min/m2 4,0 (3,2–5,1) 3,9 (3,2–4,9) 2,4 (1,9–3,1) 9,0 (6,0–12,0) 2,3 (1,9–3,1) 9,0 (6,0–12,0) 10,9 (7,1–16,8) 11,2 (7,5–16,0) 14,7 (13,4–16,0) 140 (138–142) 860 (59) 356 (287–408) 14,6 (13,3–16,0) 140 (138–142) 470 (64) 352 (276–410) 134 (9) 127 (8) 145 (9) 101 (6) 204 (13) 118 (8) 123 (8) 64 (4) 314 (20) 233 (15) 67 (8) 65 (8) 69 (8) 101 (12) 65 (8) 60 (7) 62 (7) 34 (4) 81 (10) 237 (28) Presión capilar pulmonar enclavada, mmHg Resistencia vascular pulmonar, unidades Wood Valores analíticos basales Hemoglobina, g/dL Sodio, mEq/L Uso de warfarina, n (%) 6MWD basal, m Estudio, n (%) ARIES-1 ARIES-2 BREATHE-1 AIR SUPER STRIDE-1 STRIDE-2 STRIDE-4 PHIRST Treprostinilo IMC indica índice de masa corporal; HAP, hipertensión arterial pulmonar; VIH, virus de la inmunodeficiencia humana; NYHA, New York Heart Association; 6MWD, distancia recorrida en 6 minutos; ARIES, Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies; AIR, Aerosolized Iloprost Randomized; BREATHE, Bosentan: Randomized Trial of Endothelin receptor Antagonist Therapy; STRIDE, Sitaxsentan To Relieve Impaired Exercise; SUPER, Sildenafil Use in Pulmonary Hypertension; y PHIRST, Pulmonary Arterial Hypertension and Response to Tadalafil. Los resúmenes estadísticos se presentan en forma de mediana (cuartil 1-cuartil 3) a menos que se indique lo contrario con n (%). Gabler y cols. Validación de la distancia recorrida en 6 minutos 7 Tabla 2. Características de los estudios y las combinaciones de fármacos Estadísticas a nivel de estudio Estudio y fármaco/dosis n ARIES-1 Ambrisentán 5 mg 67 Ambrisentán 10 mg 67 Placebo 67 ARIES-2 Ambrisentán 2,5 mg 64 Ambrisentán 5 mg 63 Placebo 65 BREATHE-1 Bosentán 125 mg 75 Bosentán 250 mg 70 Placebo 69 AIR Iloprost 101 Placebo 101 STRIDE-1 Sitaxentán 100 mg 55 Sitaxentán 300 mg 63 Placebo 60 STRIDE-2 Sitaxentán 50 mg 61 Sitaxentán 100 mg 62 Placebo 62 STRIDE-4 Sitaxentán 50 mg 32 Sitaxentán 100 mg 32 Placebo 34 SUPER Sildenafilo 20 mg 68 Sildenafilo 40 mg 65 Sildenafilo 80 mg 71 Placebo 65 PHIRST Tadalafilo 2,5 mg 79 Tadalafilo 10 mg 79 Tadalafilo 20 mg 81 Tadalafilo 40 mg 75 Placebo 81 Treprostinilo Treprostinilo 233 Placebo 237 Eventos clínicos, n % Mujeres % Negros % NYHA III/IV % ETC 10 84 7,3 65 31 20 74 0 54 32 9 79 7,1 100 22 41 67 1,5 100 23 7 79 8,1 67 24 8 77 13,1 63 29 2 84 6,7 39 15 17 76 2,6 61 30 39 78 9,7 67 24 45 81 5,3 7 19 NYHA indica New York Heart Association ETC, enfermedad del tejido conjuntivo; ARIES, Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies; BREATHE, Bosentan: Randomized Trial of Endothelin receptor Antagonist Therapy; AIR, Aerosolized Iloprost Randomized; STRIDE, Sitaxsentan To Relieve Impaired Exercise; SUPER, Sildenafil Use in Pulmonary Hypertension; y PHIRST, Pulmonary Arterial Hypertension and Response to Tadalafil. Llevamos a cabo 2 análisis secundarios. En primer lugar, excluimos el estudio PHIRST (Pulmonary Arterial Hypertension and Response to Tadalafil), en el que se permitió que los pacientes utilizaran un tratamiento de base con otros fármacos específicos para la HAP aprobados. En segundo lugar, excluimos a los pacientes que estaban en la clase IV de la NYHA en el momento de la aleatorización, ya que es improbable que estos pacientes sean incluidos en futuros ensayos clínicos. Todas las regresiones y metarregresiones se realizaron 8 Circulation Enero, 2013 Tabla 3. Criterios para establecer que el cambio de la 6MWD interviene en la relación entre la asignación del tratamiento y la aparición de un evento clínico en un seguimiento de 12 semanas Criterios Resultados* La asignación del tratamiento tiene un efecto significativo en el Δ6MWD respecto al valor basal a las 12 semanas de seguimiento El Δ6MWD tiene un efecto significativo en la probabilidad de presentar un evento clínico Diferencia media, 22,4 (IC del 95%, 15,9 –28,9) La asignación del tratamiento tiene un efecto significativo sobre la probabilidad de presentar un evento clínico a las 12 semanas de seguimiento El efecto de la asignación del tratamiento sobre la probabilidad de presentar un evento clínico (en comparación con lo indicado antes) es atenuado con la adición del Δ6MWD al modelo OR, 0,43 (IC del 95% 0,31-0,59) OR, 0,89 por 10 m (IC del 95%, 0,87–0,91) OR, 0,52 (IC del 95% 0,37-0,73) 6MWD indica distancia recorrida en 6 minutos; IC, intervalo de confianza; y OR, odds ratio. *Todos los modelos incluyen un ajuste respecto al estudio y a la distancia recorrida en la situación basal; la asignación al grupo placebo constituye el grupo de referencia para todos los modelos que incluían el tratamiento. con el programa R versión 2.13 (R Development Core Team, Viena, Austria). El comité ético de la University of Pennsylvania determinó que este estudio estaba eximido de la exigencia de autorización (aprobación número 814001). Todos los coautores tuvieron acceso a los datos del estudio, asumen la responsabilidad del análisis, y tuvieron autoridad en la elaboración del manuscrito y la decisión de presentarlo para publicación. Resultados Los 10 ensayos incluían un total de 2.404 pacientes; a 1.563 (65%) se les asignó el tratamiento activo. La mediana de edad de los participantes era de 50 años (rango, 10–90 años), un 22% eran varones, y un 5% eran de raza negra (Tabla 1). En 581 pacientes (24%) el diagnóstico era de HAP causada por una enfermedad del tejido conjuntivo, y 1.349 (56%) fueron clasificados en clase III o IV de la NYHA. Fallecieron 45 pacientes (2%) entre la situación basal y el seguimiento realizado a las 12 semanas. Otros 153 pacientes (6%) presentaron otros eventos clínicos; en 83 de ellos no se dispuso de datos de distancia recorrida a las 12 semanas. La media de la distancia recorrida en la situación basal fue de 341 m (DE, 85,7 m). Los valores demográficos, antropométricos, analíticos y hemodinámicos fueron similares en los distintos grupos definidos según la asignación del tratamiento. Las características de los 10 ensayos se indican en la Tabla 2. Los porcentajes a nivel de estudio de mujeres y de pacientes con diagnóstico de HAP relacionada con enfermedad del tejido conjuntivo fueron uniformes en los diversos estudios. Los porcentajes de clase III/IV de la NYHA y de pacientes de raza negra mostraron una mayor variación en los diversos estudios. ¿Interviene la 6MWD en la relación entre la asignación del tratamiento y los eventos clínicos? Los 4 criterios necesarios para establecer que el Δ6MWD es un mediador en la relación entre la asignación del tratamiento y la aparición de un evento clínico se indican en la Tabla 3. Para cada uno de ellos, observamos un resultado estadísticamente significativo en el sentido requerido. En primer lugar la asignación al tratamiento activo en comparación con la asignación a placebo dio lugar a diferencias mayores en el Δ6MWD (diferencia media del Δ6MWD, 22,4 m; IC del 95%, 15,9–28,9 m). En segundo lugar, las diferencias mayores del Δ6MWD reducían significativamente las probabilidades de eventos clínicos en el seguimiento realizado a las 12 semanas (OR para un aumento de 10 m en el Δ6MWD, 0,89; IC del 95%, 0,87–0,91). En tercer lugar, la asignación al tratamiento activo en comparación con la asignación a placebo redujo significativamente la probabilidad relativa de eventos clínicos a las 12 semanas (OR, 0,43; IC del 95%, 0,31–0,59). Por último, el efecto de la asignación del tratamiento sobre la aparición de un evento clínico se atenuaba con la adición del Δ6MWD al modelo (OR, 0,52; IC del 95%, 0,37–0,73). La parte del efecto del tratamiento sobre las probabilidades de sufrir un evento clínico a las 12 semanas que se explicaba por el Δ6MWD fue del 22,1% (IC del 95%, 12,1–31,1%). Además, la prueba de Sobel modificada confirmó la significación estadística de la mediación (Z = 4,77, p < 0,001). No hubo interacciones significativas entre el tratamiento y el Δ6MWD (estimación [IC del 95%], 0,002 [-0,002 a 0,006], p = 0,25). ¿Existe un efecto umbral para el Δ6MWD? En comparación con placebo, casi todas las combinaciones de fármaco/dosis produjeron un valor superior del Δ6MWD en el seguimiento realizado a las 12 semanas (Tabla 4). El resumen de los resultados indica una diferencia media del Δ6MWD de 22,4 m (IC del 95%, 17,4 –27,5 m) con la asignación al tratamiento activo en comparación con placebo. El efecto sobre la reducción de los eventos clínicos fue uniforme con las diversas combinaciones de fármaco/dosis. En comparación con placebo, las 21 combinaciones de fármaco/dosis redujeron las probabilidades de aparición de un evento clínico en el seguimiento de 12 semanas (OR de resumen, 0,44; IC del 95%, 0,33–0,57). En la Figura se muestran los resultados de nuestra metarregresión y análisis de umbral. El intervalo superior de la predicción cortaba el valor nulo para la probabilidad relativa de un evento clínico con una diferencia de Δ6MWD de 41,8 m. Este valor indica la diferencia mínima del Δ6MWD que corresponde a una reducción estadísticamente significativa de los eventos clínicos. Los modelos que incluían los factores de raza, sexo, categoría diagnóstica y clase funcional de la NYHA no mostraron indicio alguno de un efecto de confusión y estas variables no se incluyeron en el modelo de metarregresión final. En un análisis de sensibilidad, excluimos las 4 combinaciones de fármaco/dosis del estudio PHIRST, ya que este estudio fue el único en el que se permitió el uso de un tratamiento de base concomitante. La exclusión de este estudio hizo que el Gabler y cols. Validación de la distancia recorrida en 6 minutos 9 Tabla 4. Resultados específicos para fármaco/dosis ajustados según el efecto placebo Estudio y fármaco/dosis Diferencia de Δ6MWD, m (IC del 95%) OR para los eventos clínicos (IC del 95%) Ponderación en la metarregresión ARIES-1 Ambrisentán 5 mg 24,9 (0,32–49,4) 0,58 (0,13–2,53) 1,8 Ambrisentán 10 mg 41,4 (15,6–67,2) 0,38 (0,07–2,04) 1,4 Ambrisentán 2,5 mg 37,3 (8,2–66,3) 0,35 (0,11–1,12) 2,8 Ambrisentán 5 mg 53,6 (24,4–82,8) 0,22 (0,06–0,88) 2,1 Bosentán 125 mg 33,4 (8,6–58,3) 0,58 (0,12–2,80) 1,5 Bosentán 250 mg 46,3 (21,1–71,6) 0,42 (0,07–2,47) 1,2 24,5 ( 2,4–51,3) 0,47 (0,23–0,96) 7,3 Sitaxentán 100 mg 33,3 (9,1–57,4) 0,20 (0,02–1,99) 0,7 Sitaxentán 300 mg 24,6 ( 0,45–49,7) 0,36 (0,06–2,15) 1,2 7,1 ( 27,6–13,5) 0,54 (0,09–3,20) 1,2 0,77 (0,13–4,72) 1,2 ARIES-2 BREATHE-1 AIR Iloprost STRIDE-1 STRIDE-2 Sitaxentán 50 mg Sitaxentán 100 mg 15,2 ( 4,7–35,1) STRIDE-4 Sitaxentán 50 mg 19,1 ( 49,9–11,8) 0,71 (0–4,42)* 0,1 Sitaxentán 100 mg 6,9 ( 23,5–37,5) 0,73 (0–2,07)* 0,1 SUPER Sildenafilo 20 mg 39,3 (15,0–63,6) 0,36 (0,09–1,47) 1,9 Sildenafilo 40 mg 45,2 (20,6–69,8) 0,25 (0,05–1,28) 1,5 Sildenafilo 80 mg 42,1 (18,0–66,3) 0,59 (0,17–1,98) 2,6 PHIRST Tadalafilo 2,5 mg 0,49 (0,18–1,34) 3,8 Tadalafilo 10 mg 17,1 ( 4,3–38,5) 0,3 ( 20,7–20,0) 0,30 (0,10–0,90) 3,1 Tadalafilo 20 mg 24,6 (5,1–44,1) 0,59 (0,23–1,51) 4,4 Tadalafilo 40 mg 18,2 ( 2,2–38,6) 0,27 (0,08–0,90) 2,7 9,9 ( 6,7–26,4) 0,52 (0,27–0,99) 9,2 Treprostinilo Treprostinilo Resumen† 22,4 (17,4–27,5) 0,44 (0,33–0,57) 6MWD indica distancia recorrida en 6 minutos; IC, intervalo de confianza; OR, odds ratio; ARIES, Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies; BREATHE, Bosentan: Randomized Trial of Endothelin receptor Antagonist Therapy; AIR, Aerosolized Iloprost Randomized; STRIDE, Sitaxsentan To Relieve Impaired Exercise; SUPER, Sildenafil Use in Pulmonary Hypertension; y PHIRST, Pulmonary Arterial Hypertension and Response to Tadalafil. El grupo de referencia es el grupo placebo en cada estudio. Todos los análisis incluyen un ajuste respecto a la distancia recorrida en la situación basal. *Obtenido mediante regresión logística exacta. †Obtenido mediante metanálisis de efectos fijos (p para la heterogeneidad = 0,99). valor umbral fuera más bajo, de 25,7 m, para la diferencia del Δ6MWD. En otro análisis adicional, la exclusión de los pacientes que estaban en la clase IV de la NYHA (n = 127) no modificó los resultados de manera apreciable. Se presenta una información adicional al respecto en el Suplemento de Datos Online. Discusión Este estudio presenta el primer examen riguroso de la validez del Δ6WMD a las 12 semanas respecto al valor basal como variable de valoración sustitutiva en los ensayos terapéuticos de la HAP. El Δ6MWD cumplió todos los criterios de mediador de la relación entre el tratamiento y la aparición de un evento clínico en el seguimiento de 12 semanas; sin embargo, la parte de esta relación explicada por la 6MWD era modesta, de un 22%, lo cual sugiere que la 6MWD puede no ser una variable sustitutiva suficiente. Se identificó también un efecto umbral de 41,8 m, lo cual significa que si un fármaco mejora la 6MWD a lo largo de 12 semanas en 41,8 m más de lo que lo hace el placebo, los investigadores podrían predecir, con un nivel de confianza del 95%, que el fármaco reduciría la tasa de eventos clínicos a lo largo de 12 semanas. 10 Circulation Enero, 2013 Figura. Resultados del análisis de metarregresión que muestra la relación entre los cambios de la distancia recorrida en 6 minutos (6MWD) a las 12 semanas de seguimiento respecto a la situación basal a nivel de fármaco/dosis según el estudio con la probabilidad de un evento clínico a las 12 semanas. Cada círculo corresponde a una combinación de fármaco/dosis, y los tamaños son proporcionales a la ponderación del estudio (tal como se detalla en la Tabla 4 y en función de una ponderación inversa de la varianza). El área gris sombreada corresponde a los límites de los intervalos de predicción del 95%. El valor umbral se indica en el eje horizontal en 41,8 m. Observamos que tan solo 4 de las 21 combinaciones de fármaco-dosis producían efectos sobre el Δ6MWD que pudiera afirmarse, con un grado de certeza convencional, que se asociaban a una mejoría clínica (Figura). Si se utiliza el valor de umbral inferior de 25,7 m, 5 de las 17 combinaciones de fármaco-dosis restantes producirían efectos estadísticamente significativos sobre los resultados clínicos en ausencia de un tratamiento de base. De estas 9 combinaciones de fármaco-dosis que cumplían el criterio del valor umbral inferior, 1 correspondía a un fármaco que no ha sido autorizado por la FDA (sitaxentán) y 2 a dosis que no se incluyen en el prospecto de la FDA (sildenafilo 40 mg 3 veces al día y sildenafilo 80 mg 3 veces al día). Tres fármacos (iloprost, tadalafilo y treprostinilo) no cumplían ninguno de los dos criterios de valor umbral. Es esencial explorar la validez de las variables de valoración sustitutivas, ya que las que son válidas proporcionan un mecanismo eficiente para la realización de los estudios de nuevas intervenciones en las fases iniciales. Concretamente, los ensayos que utilizan variables de valoración sustitutivas validadas pueden llevarse a cabo con mayor rapidez, con tamaños muestrales menores, con menos riesgos para los participantes y con un menor coste de investigación, en comparación con los ensayos que utilizan las variables de valoración clínicas reales33,34. Sin embargo, estas ventajas solamente se dan de forma clara si las variables de valoración sustitutivas han sido validadas; en ausencia de validación, existe un considerable riesgo, tal como hizo famoso el Cardiac Arrhythmia Suppression Trial (CAST)35, de que se llegue erróneamente a una conclusión de efectividad de una nueva intervención. Estos datos añaden también nueva información a la cada vez más amplia literatura existente sobre el uso de la 6MWD como variable de valoración en otros contextos. Con el empleo de diferentes métodos, se ha evaluado la 6MWD en la fibrosis pulmonar idiopática36, la enfermedad pulmonar obstructiva crónica37 y la rehabilitación cardiaca38. En el presente estudio, observamos que la parte del efecto de tratamiento en la prevención de los eventos clínicos que se explicaba por el cambio de la 6MWD era de un 22,1%, lo cual está por debajo del umbral del 50% a 75% descrito para una variable sustitutiva válida por Freedman y cols.27 aunque algunos autores consideran que este criterio es demasiado estricto15. Parece claro que los tratamientos de la HAP ejercen unos efectos sobre el resultado no medidos que no son explicados plenamente por el cambio de la 6MWD39. Así pues, la observación de una mediación real aunque modesta por parte de la 6MWD sugiere que puede no ser suficiente utilizarla sola. La incorporación en una medida sustitutiva combinada, junto con evaluaciones hemodinámicas o de otro tipo podría mejorar su rendimiento y justificar la realización de nuevos estudios. El valor umbral de 41,8 m que identificamos para la diferencia del Δ6MWD puede tenerse en cuenta para un uso como nivel de mejora del Δ6MWD que es necesario para poder concluir de manera fiable que la intervención aportará un beneficio clínico en futuros ensayos. Con el empleo de diferentes métodos y pacientes de un único estudio (el estudio SUPER [Sildenafil Use in Pulmonary Arterial Hypertension), Gilbert y cols.40 estimaron una diferencia mínima clínicamente importante de 41 m, que estaba correlacionada con la mejoría descrita por el paciente. De igual modo, en pacientes con HAP no tratados, Paciocco y cols.41 observaron que cada 50 m de aumento en la distancia recorrida se asociaban a una reducción de la mortalidad del 18%. La coincidencia de los resultados en los diversos estudios realizados con el empleo de métodos diferentes respalda la solidez de este resultado. Sin embargo, el Δ6MWD continúa siendo una variable de valoración sustitutiva insuficiente, dado el grado modesto de mediación en el efecto del tratamiento. La fiabilidad de los resultados del presente estudio deriva del gran tamaño muestral utilizado y del hecho de que los efectos del tratamiento sobre los cambios de la 6MWD y sobre los eventos clínicos fueron uniformes con todas las dosis de medicación42. No obstante, el presente estudio tiene ciertas limitaciones. En primer lugar, como ocurre en cualquier metanálisis, los resultados están sujetos a posibles errores en la realización, entrada de datos o análisis de los datos principales. En segundo lugar, estos ensayos principales incluyeron principalmente a mujeres y a individuos blancos, y utilizaron unos periodos de seguimiento relativamente breves. No pudimos evaluar los resultados clínicos posteriores a las 12 semanas, y nuestros resultados no deben generalizarse a un periodo superior a este. Sin embargo, las características demográficas representadas concuerdan con la epidemiología más amplia de la HAP, y todos los ensayos incluidos tenían unas características similares en cuanto a seguimiento, definiciones de los eventos clínicos y evaluación de los resultados, lo cual hace que sean apropiados para un planteamiento metanalítico. Todos los ensayos que hemos examinado utilizaron un diseño controlado con placebo, lo cual constituye un punto Gabler y cols. Validación de la distancia recorrida en 6 minutos 11 fuerte adicional; sin embargo, 1 estudio permitió el uso de un tratamiento de base concomitante. La exclusión del ensayo PHIRST redujo nuestro valor umbral, lo cual sugiere que en futuros ensayos en los que se empleen tratamientos de base puede ser preciso utilizar valores umbrales superiores a los indicados aquí. En otras palabras, en presencia de un tratamiento efectivo para la HAP, un ensayo controlado y aleatorizado de un nuevo tratamiento puede requerir la obtención de mayores diferencias del Δ6MWD para indicar de manera fiable que los resultados corresponden a diferencias en la evolución clínica. No pudimos explorar con mayor profundidad el papel del tratamiento de base debido al pequeño tamaño muestral. Así pues, serán necesarias nuevas investigaciones teniendo en cuenta las cuestiones éticas que se plantean en relación con la futura realización de ensayos controlados con placebo en la HAP43. Por último, utilizamos técnicas estadísticas para poder abordar mejor una cuestión clínica. Aunque nuestra estimación del umbral proporciona una idea clara del grado de Δ6MWD que sería necesario para indicar que los efectos beneficiosos de un tratamiento serán superiores a cero, la inferencia de una diferencia “clínicamente importante” en los resultados podría justificar el empleo de un umbral diferente. Los pacientes individuales pueden mostrar una mejoría clínica sin alcanzar un determinado valor umbral del Δ6MWD, y hay pacientes que mejoran su 6MWD sin presentar necesariamente una mejoría clínica. Sin embargo, los valores umbral a nivel de población que hemos establecido serán útiles para el diseño de futuros ensayos clínicos. En conclusión, hemos utilizado 2 enfoques complementarios para examinar la validez del Δ6MWD como variable de valoración sustitutiva en ensayos clínicos de tratamientos para la HAP. Pudimos identificar un efecto umbral significativo del Δ6MWD que puede usarse como guía para futuros ensayos controlados y aleatorizados, y observamos que el Δ6MWD es un mediador en la relación entre el tratamiento y los resultados clínicos. Sin embargo, dado que el Δ6MWD no explica una gran parte de este efecto del tratamiento, puede no ser suficiente para poder usarlo como variable de valoración sustitutiva por sí sola. Serán necesarios nuevos estudios para identificar variables de valoración sustitutivas combinadas que puedan tener unas características mejores y para determinar si este valor umbral que identificamos es aplicable a los ensayos que utilizan un tratamiento de base o que no emplean ningún control de placebo. Agradecimientos Agradecemos a Maximilian Herlim y a Ziyue Liu, PhD, su inestimable ayuda en la preparación de los datos para el análisis y a los Drs. Norman Stockbridge y Salma Lemtouni de la FDA que nos proporcionaran los datos para la realización de este estudio. Fuentes de financiación Este trabajo fue financiado por una subvención de la American Thoracic Society/Pfizer para investigación en hipertensión pulmonar (Dr. Halpern). El Dr. Kawut recibió la subvención K24 HL103844. Ni la FDA ni las fuentes de financiación intervinieron en modo alguno en el diseño de este estudio ni en la decisión de presentarlo para pu- blicación. La FDA revisó el estudio antes de la presentación, según la condición establecida en el contrato original, pero no solicitó la introducción de cambio alguno en nuestro texto. Declaraciones de intereses El Dr. Gabler ha participado en proyectos no relacionados financiados por Pfizer, Inc. El Dr. Strom ha sido consultor de Abbott, Amgen, Astra Zeneca, BMS, Boehringer Ingelheim, GlaxoSmithKline, Novartis, NPS Pharma, Nuvo Research, Orexigen, Pfizer, Teva y Vivus, y ha recibido financiación para investigación de AstraZeneca, BMS, Pfizer, Shire y Takeda. Ha recibido pagos por la contribución al programa de formación en farmacoepidemiología de Penn, por parte de Abbott, Amgen, Hoffman LaRoche, Novartis, Pfizer, Sanofi Pasteur y Wyeth. El Dr. Palevsky ha recibido pagos por consultoría, por pertenencia a consejos asesores, por conferencias y/o financiación para investigación de Actelion, Bayer, GeNO, Gilead, GlaxoSmithKline, Pfizer, United Therapeutics y Lung Rx. Estas labores no han influido en modo alguno en este análisis de los resultados de estudios publicados con anterioridad. El Dr. Kawut ha recibido pagos por consultoría, pertenencia a consejos asesores y conferencias, subvenciones de formación no condicionadas y/o financiación para investigación de Pfizer, Actelion, Bayer, Ikaria, Novartis, Merck, Gilead, United Therapeutics y Lung Rx. El Dr. Taichman ha recibido financiación para investigación del centro por parte de Actelion. Los demás autores no declaran ningún conflicto de intereses. Bibliografía 1. Taichman DB, Mandel J. Epidemiology of pulmonary arterial hypertension. Clin Chest Med. 2007;28:1–22. 2. Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, ReynaudGaubert M, Haloun A, Laurent M, Hachulla E, Cottin V, Degano B, Jais X, Montani D, Souza R, Simonneau G. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156 –163. 3. Provencher S, Sitbon O, Humbert M, Cabrol S, Jais X, Simonneau G. Long-term outcome with first-line bosentan therapy in idiopathic pulmonary arterial hypertension. Eur Heart J. 2006;27:589 –595. 4. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Herve P, Rainisio M, Simonneau G. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002;40:780 –788. 5. Miyamoto S, Nagaya N, Satoh T, Kyotani S, Sakamaki F, Fujita M, Nakanishi N, Miyatake K. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension: comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2000;161:487– 492. 6. Baker SG, Kramer BS. A perfect correlate does not a surrogate make. BMC Med Res Methodol. 2003;3:16. 7. Prentice RL. Surrogate endpoints in clinical trials: definition and operational criteria. Stat Med. 1989;8:431– 440. 8. Ventetuolo CE, Benza RL, Peacock AJ, Zamanian RT, Badesch DB, Kawut SM. Surrogate and combined end points in pulmonary arterial hypertension. Proc Am Thorac Soc. 2008;5:617– 622. 9. Snow JL, Kawut SM. Surrogate end points in pulmonary arterial hypertension: assessing the response to therapy. Clin Chest Med. 2007;28:75–89. 10. Macchia A, Marchioli R, Marfisi R, Scarano M, Levantesi G, Tavazzi L, Tognoni G. A meta-analysis of trials of pulmonary hypertension: a clinical condition looking for drugs and research methodology. Am Heart J. 2007;153:1037–1047. 11. Helman DL, Brown AW, Jackson JL, Shorr AF. Analyzing the short-term effect of placebo therapy in pulmonary arterial hypertension: potential implications for the design of future clinical trials. Chest. 2007;132:764–777. 12. Galie N, Manes A, Negro L, Palazzini M, Bacchi-Reggiani ML, Branzi A. A meta-analysis of randomized controlled trials in pulmonary arterial hypertension. Eur Heart J. 2009;30:394 – 403. 12 Circulation Enero, 2013 13. Macchia A, Marchioli R, Tognoni G, Scarano M, Marfisi R, Tavazzi L, Rich S. Systematic review of trials using vasodilators in pulmonary arterial hypertension: why a new approach is needed. Am Heart J. 2010; 159:245–257. 14. Johnson KR, Freemantle N, Anthony DM, Lassere MND. LDL-cholesterol differences predicted survival benefit in statin trials by the surrogate threshold effect (STE). J Clin Epidemiol. 2009;62:328 –336. 15. Buyse M, Molenberghs G. Criteria for the validation of surrogate endpoints in randomized experiments. Biometrics. 1998;54:1014 –1029. 16. MacKinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Eval Rev. 1993;17:144 –158. 17. Burzykowski T, Buyse M. Surrogate threshold effect: an alternative measure for meta-analytic surrogate endpoint validation. Pharm Stat. 2006;5:173–186. 18. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, Keogh A, Oudiz R, Frost A, Blackburn SD, Crow JW, Rubin LJ. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165:800 – 804. 19. Galie N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, Badesch DB, McGoon MD, McLaughlin VV, Roecker EB, Gerber MJ, Dufton C, Wiens BL, Rubin LJ. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy (ARIES) Study 1 and 2. Circulation. 2008;117: 3010 –3019. 20. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido T, Frost A, Roux S, Leconte I, Landzberg M, Simonneau G. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346:896–903. 21. Olschewski H, Simonneau G, Galie N, Higenbottam T, Naeije R, Rubin LJ, Nikkho S, Speich R, Hoeper MM, Behr J, Winkler J, Sitbon O, Popov W, Ghofrani HA, Manes A, Kiely DG, Ewert R, Meyer A, Corris PA, Delcroix M, Gomez-Sanchez M, Siedentop H, Seeger W; the Aerosolized Iloprost Randomized Study Group. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med. 2002;347:322–329. 22. Barst RJ, Langleben D, Frost A, Horn EM, Oudiz R, Shapiro S, McLaughlin V, Hill N, Tapson VF, Robbins IM, Zwicke D, Duncan B, Dixon RAF, Frumkin LR. Sitaxsentan therapy for pulmonary arterial hypertension. Am J Respir Crit Care Med. 2004;169:441– 447. 23. Barst RJ, Langleben D, Badesch D, Frost A, Lawrence EC, Shapiro S, Naeije R, Galie N. Treatment of pulmonary arterial hypertension with the selective endothelin-A receptor antagonist sitaxsentan. J Am Coll Cardiol. 2006;47:2049 –2056. 24. Galie N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, Fleming T, Parpia T, Burgess G, Branzi A, Grimminger F, Kurzyna M, Simonneau G; Sildenafil Use in Pulmonary Arterial Hypertension Study Group. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005;353:2148 –2157. 25. Galie N, Brundage BH, Ghofrani HA, Oudiz RJ, Simonneau G, Safdar Z, Shapiro S, White RJ, Chan M, Beardsworth A, Frumkin L, Barst RJ. Tadalafil therapy for pulmonary arterial hypertension. Circulation. 2009; 119:2894 –2903. 26. Klebanoff MA, Cole SR. Use of multiple imputation in the epidemiologic literature. Am J Epidemiol. 2008;168:355–357. 27. Freedman LS, Graubard BI, Schatzkin A. Statistical validation of intermediate end-points for chronic diseases. Stat Med. 1992;11:167–178. 28. Huang J, Huang B. Evaluating the proportion of treatment effect explained by a continuous surrogate marker in logistic or probit regression models. Stat Biopharm Res. 2010;2:229 –238. 29. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. New York, NY: Chapman and Hall; 1993. 30. Jasti S, Dudley WN, Goldwater E. SAS macros for testing statistical mediation in data with binary mediators or outcomes. Nurs Res. 2008; 57:118 –122. 31. Gabler NB, French B, Strom BL, Liu Z, Palevsky HI, Taichman DB, Kawut SM, Halpern SD. Race and sex differences in response to endothelin receptor antagonists for pulmonary arterial hypertension. Chest. 2012;141:20 –26. 32. Kuhn KP, Byrne DW, Arbogast PG, Doyle TP, Loyd JE, Robbins IM. Outcome in 91 consecutive patients with pulmonary arterial hypertension receiving epoprostenol. Am J Respir Crit Care Med. 2003;167:580 –586. 33. Lassere MN. The biomarker-surrogacy evaluation schema: a review of the biomarker-surrogate literature and a proposal for a criterion-based, quantitative, multidimensional hierarchical levels of evidence schema for evaluating the status of biomarkers as surrogate endpoints. Stat Methods Med Res. 2008;17:303–340. 34. Rasekaba T, Lee AL, Naughton MT, Williams TJ, Holland AE. The six-minute walk test: a useful metric for the cardiopulmonary patient. Intern Med J. 2009;39:495–501. 35. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson DW; CAST Investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo: the Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324:781–788. 36. du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, Lancaster L, Noble PW, Sahn SA, Szwarcberg J, Thomeer M, Valeyre D, King TE Jr. Six-minute-walk test in idiopathic pulmonary fibrosis: test validation and minimal clinically important difference. Am J Respir Crit Care Med. 2011;183:1231–1237. 37. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the six minute walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155:1278 –1282. 38. Hamilton DM, Haennel RG. Validity and reliability of the 6-minute walk test in a cardiac rehabilitation population. J Cardiopulm Rehabil. 2000; 20:156 –164. 39. Fleming TR, DeMets DL. Surrogate end points in clinical trials: are we being misled? Ann Intern Med. 1996;125:605– 613. 40. Gilbert C, Brown MC, Cappelleri JC, Carlsson M, McKenna SP. Estimating a minimally important difference in pulmonary arterial hypertension following treatment with sildenafil. Chest. 2009;135:137–142. 41. Paciocco G, Martinez FJ, Bossone E, Pielsticker E, Gillespie B, Rubenfire M. Oxygen desaturation on the six-minute walk test and mortality in untreated primary pulmonary hypertension. Eur Respir J. 2001;17: 647– 652. 42. Buyse M, Molenberghs G, Burzykowski T, Renard D, Geys H. The validation of surrogate endpoints in meta-analyses of randomized experiments. Biostatistics. 2000;1:49 – 67. 43. Halpern SD, Doyle R, Kawut SM. The ethics of randomized clinical trials in pulmonary arterial hypertension. Proc Am Thorac Soc. 2008;5: 631– 635. PERSPECTIVA CLÍNICA Este estudio pone de manifiesto que el cambio de la distancia recorrida en 6 minutos (6MWD) satisface los criterios estadísticos de un factor mediador entre el tratamiento farmacológico y los resultados clínicos en los ensayos clínicos aleatorizados. Se identificaron umbrales del cambio de la 6MWD para los que se considera que si futuros fármacos produjeran tales cambios, podría inferirse que dichos fármacos producirían también efectos clínicos. Es posible que sean necesarios umbrales más altos de 6MWD al evaluar nuevos fármacos en presencia de un tratamiento de base para la hipertensión arterial pulmonar; sin embargo, nuestros resultados indican que probablemente la 6MWD no sea adecuada para el uso como variable de valoración sustitutiva en los ensayos clínicos en la hipertensión arterial pulmonar, ya que tan solo una parte modesta del efecto de los fármacos sobre los resultados clínicos reales se explica por los cambios de la 6MWD. Serán necesarias nuevas investigaciones para identificar variables de valoración sustitutivas o combinaciones de ellas que sean más sólidas.


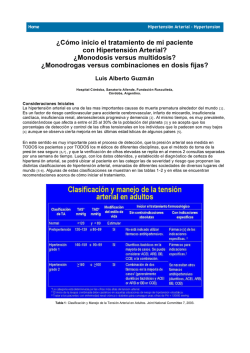
© Copyright 2026