
Anti–Nogo-A Antibody Infusion 24 Hours After
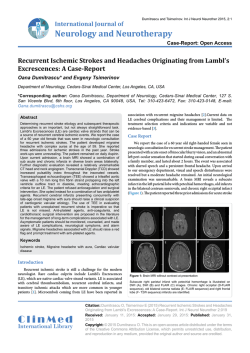
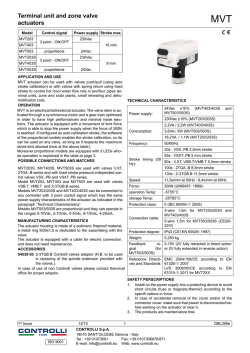
Journal of Cerebral Blood Flow & Metabolism 23:154–165 © 2003 The International Society for Cerebral Blood Flow and Metabolism Published by Lippincott Williams & Wilkins, Inc., Philadelphia Anti–Nogo-A Antibody Infusion 24 Hours After Experimental Stroke Improved Behavioral Outcome and Corticospinal Plasticity in Normotensive and Spontaneously Hypertensive Rats *Christoph Wiessner, †Florence M. Bareyre, ‡Peter R. Allegrini, *Anis K. Mir, *Stefan Frentzel, ‡Mauro Zurini, †Lisa Schnell, †Thomas Oertle, and †Martin E. Schwab *Nervous System Research, ‡Core Technology Area, Novartis Pharma AG, Basel; †Brain Research Institute, University of Zurich, and Department of Biology, Swiss Federal Institute of Technology Zurich, Zurich, Switzerland Summary: Nogo-A is a myelin-associated neurite outgrowth inhibitory protein limiting recovery and plasticity after central nervous system injury. In this study, a purified monoclonal anti–Nogo-A antibody (7B12) was evaluated in two rat stroke models with a time-to-treatment of 24 hours after injury. After photothrombotic cortical injury (PCI) and intraventricular infusion of a control mouse immunoglobulin G for 2 weeks, long-term contralateral forepaw function was reduced to about 55% of prelesion performance until the latest time point investigated (9 weeks). Forepaw function was significantly better in the 7B12-treated group 6 to 9 weeks after PCI, and reached about 70% of prelesion levels. Cortical infarcts were also produced in spontaneously hypertensive rats (SHR) by permanent middle cerebral artery occlusion (MCAO). In the control group, forepaw function remained between 40% and 50% of prelesion levels 4 to 12 weeks after MCAO. In contrast, 7B12-treated groups showed significant improvement between 4 and 7 weeks after MCAO from around 40% of prelesion levels at week 4 to about 60% to 70% at 7 to 12 weeks after MCAO. Treatment in both models was efficacious without influencing infarct volume or brain atrophy. Neuroanatomically in the spinal cord, a significant increase of midline crossing corticospinal fibers originating in the unlesioned sensorimotor cortex was found in 7B12-treated groups, reaching 2.3 ± 1.5% after PCI (control group: 1.1 ± 0.5%) and 4.5 ± 2.2% after MCAO in SHR rats (control group: 1.8 ± 0.8%). Behavioral outcome and the presence of midline crossing fibers in the cervical spinal cord correlated significantly, suggesting a possible contribution of the crossing fibers for forepaw function after PCI and MCAO. The results suggest that specific anti–Nogo-A antibodies bear potential as a new rehabilitative treatment approach for ischemic stroke with a prolonged time-to-treatment window. Key Words: Nogo—Neurite outgrowth inhibitor—Focal cerebral ischemia—Sensorimotor function—Plasticity. Injuries to the adult human cerebral motor cortex often result in persisting limb movement deficits (Nudo et al., 2001). The leading cause of cortical injury and serious long-term disability is ischemic stroke (Stapf and Mohr, 2002). Epidemiologic data suggest that after a long period of decline, stroke incidence is now rising again (Gillum and Sempos, 1997). Because treatment options are limited to thrombolysis with a time-to-treatment window of only 3 hours (The NINDS study group, 1997; del Zoppo, 2000), and a large number of neuroprotective drugs failed in clinical trials (Martinez-Vila and Sieira, 2001), an urgent medical need for new treatment strategies for stroke exists. In comparison to the adult brain, recovery of motor function after injury is much better in the neonatal brain (Milner, 1974; Whishaw and Kolb, 1988), and neuroanatomic plasticity is thought to be the underlying mechanism. Studies in newborn rats have shown that, after sensorimotor cortical lesion, the uninjured contralateral cortex is able to form bilateral connections with the striatum (Kolb et al., 1992), thalamus (Yu et al., 1995), red nucleus (Naus et al., 1985), tectum (Leong and Lund, 1973), basilar pontine gray (Kartje-Tillotson et al., 1986), and spinal cord (Rouiller et al., 1991). The capacity to form such new connections declines with progressing myelination (Huber and Schwab, 2000), which led to the hypothesis that plasticity in the adult brain is restricted by neurite outgrowth inhibitors residing in myelin (Kapfhammer and Schwab, 1994). One of the most Received July 4, 2002; final version received September 18, 2002; accepted September 19, 2002. Supported by the NCCR on Neural Plasticity and Repair. Address correspondence and reprint requests to Dr. Christoph Wiessner, Novartis Pharma AG, Nervous System Research, Neurodegeneration Unit WKl125.5.15, CH-4002 Basel, Switzerland; e-mail: [email protected] 154 DOI: 10.1097/01.WCB.0000040400.30600.AF ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE potent neurite growth inhibitory activities associated with oligodendrocyte membranes and CNS myelin is the membrane protein Nogo-A, which has recently been cloned (Chen et al., 2000; Grand Pre´ et al., 2000; Prinhja et al., 2000). A neutralizing antibody (mAb IN-1), raised against NI-250 (Caroni and Schwab, 1988), improved regeneration of lesioned axons in the adult rat spinal cord, optic nerve, or brain (Schnell and Schwab, 1990; Huber and Schwab, 2000), and increased compensatory fiber growth of unlesioned tract systems (Thallmair et al., 1998; Z’Graggen et al., 2000; Wenk et al., 1999). In behavioral assays in rats, functional recovery was observed after injury and IN-1 hybridoma treatment (Thallmair et al., 1998; Z’Graggen et al., 1998). In all of these studies, IN-1 was delivered by implanted antibodysecreting hybridoma cells with concomitant immunosuppression. As an important step towards transfer of Nogo-A neutralization to the level of clinical trials, we generated a new monoclonal anti–Nogo-A antibody of the immunoglobulin G (IgG)1-subtype (7B12), which was purified and delivered in a highly controlled manner by minipumps. In the present study, we showed that 7B12 infusion initiated 24 hours after stroke improved long-term behavioral recovery without affecting lesion volumes. Behavioral outcome correlated with sprouting of corticospinal fibers of the unlesioned sensorimotor cortex, which was stimulated in 7B12-treated animals. The results support the concept that Nogo-A neutralization augments the inherent and functionally meaningful plastic capacity of the adult CNS, which is restricted by outgrowth inhibitors. MATERIAL AND METHODS Characterization of monoclonal antibody 7B12 Binding of purified antirat monoclonal antibody (mAb) 7B12 (IgG1) to rat NiG (the protein domain specific to Nogo-A) and rat NiG delta-6 fragment (Oertle et al., 2000) was determined by enzyme-linked immunosorbent assay. NiG and NiG delta-6 were coated on enzyme-linked immunosorbent assay plates at a concentration of 2 g/mL and incubated with different concentrations of 7B12 mAb. The binding of 7B12 to the two proteins was quantified by using a goat antimouse horseradish peroxidase–coupled antibody and peroxidase substrate (Roche Diagnostics, Rotkreuz, Switzerland) and reading the optical density of the color reaction in an enzyme-linked immunosorbent assay plate reader at 450 nm (Spectracount; Packard, Mississauga, Ontario, Canada). Results are means ± SD of samples in at least duplicate wells. Animals. Animal maintenance conditions and all surgical procedures were approved by the veterinary authorities of the Kanton Basel-Stadt, Switzerland. Photothrombotic cortical injury. A modification of a method described by Watson et al. (1985) was used. Male Fischer F344 rats (Iffa Credo, L’Arbresele, France) weighing 300 g were anesthetized with 2% isoflurane in a 70:30 (by volume) nitrous oxide–oxygen mixture and 80 mg/kg RoseBengal in saline was infused into the femoral vein (0.5 mL/kg at 95 L/min). Immediately afterwards, a fiberglass probe with 155 10-mm diameter was positioned directly over the exposed right skull. The skull was illuminated (Volpi Intralux 6000, 150 W; Volpi AG, Schlieven, Switzerland) for 7 minutes at maximum output. Body temperature was maintained at 37°C by means of a heating pad (CMA 150; Carnegie Medicine, Stockholm, Sweden) connected to a rectal probe during surgery and until animals regained consciousness. Thereafter, animals were returned to their home cages and allowed free access to food and water. Permanent middle cerebral artery occlusion in spontaneously hypertensive rats. Irreversible right middle cerebral artery occlusion (MCAO) was performed in male spontaneously hypertensive rats (SHR) rats, 220 to 300 g (Iffa Credo), as described previously (Barone et al., 1993), with minor modifications. Briefly, animals were anesthetized (see preceding paragraph) and the right middle cerebral artery was exposed by a subtemporal craniectomy and occluded by bipolar electrocoagulation. Afterwards, retracted soft tissue was replaced, wounds were sutured, and anesthesia was discontinued. Body temperature was maintained at 37°C during surgery and until animals regained consciousness (see preceding paragraph). Thereafter, animals were returned to their home cages and were allowed free access to food and water. Magnetic resonance imaging. Infarct volume was determined 24 hours after PCI or MCAO by means of quantitative in vivo magnetic resonance imaging (MRI). Measurements were performed on a 4.7-T 30-cm-bore Spectrospin DBX (Bruker, Karlsruhe, Germany) equipped with a 20-cm gradient coil as described in detail elsewhere (Allegrini and Sauer, 1992; Wiessner et al., 2000). Briefly, rats were anesthetized with isoflurane (see preceding paragraphs) and the head was positioned in a 35-mm resonator. Thirteen contiguous T2-weighted coronal slices with a thickness of 1.2 mm were taken using a RARE sequence (repetition time, 3,000 milliseconds; effective echo time, 87 milliseconds; spatial resolution in plane, 156 m2; measure time, 5 minutes). For morphometric evaluation, damaged tissue was segmented by setting an intensity threshold using a semiautomatic image analysis software (Analyze, Biomedical Imaging Resource; Mayo Foundation, Rochester, MN, U.S.A.) on a Silicon Graphics (Mountain View, CA, U.S.A.) O2 computer. Infarct volume was calculated based on the damaged area in each slice and the distance between slices. Nine weeks after PCI, volumes of the infarcted and contralateral hemispheres were measured again by MRI and the atrophy of the infarcted hemisphere was calculated as their difference. Statistical comparison between control and treatment groups was made using t-test or analysis of variance (ANOVA) followed by Bonferroni t-test. A P value < 0.05 was regarded as being statistically significant. Treatment with 7B12. A brain infusion cannula (Alzet brain infusion kit; Alza Corp., Palo Alto, CA, U.S.A.) was stereotaxically implanted under anesthesia (2% isoflurane in 70:30 nitrous oxide–oxygen mixture) in the left lateral ventricle (coordinates: lateral 1.3; anterior–posterior −0.8; dorsoventral −3.8, relative to bregma). Control antibody (mouse IgG; Chemicon, Temecula, CA, U.S.A.) or 7B12 were applied intraventricularly in phosphate-buffered saline (PBS) by continuous infusion for 2 weeks using Alzet osmotic minipumps (5 L/h; model 2ML2; Alza Corp.). After PCI, total antibody doses were 5 mg control mouse IgG (n ⳱ 13) or 5 mg 7B12 (n ⳱ 14) infused at 15 g/h. After MCAO in SHR rats, total antibody doses were 1.68 mg 7B12 (5 g/h; n ⳱ 9), or 5 mg 7B12 (15 g/h; n ⳱ 9). In this experiment, the control antibody was given at a dose of 1.68 mg 7B12 (5 g/h; n ⳱ 9), to match the lower dose 7B12 group. The pumps were removed after 2 weeks and quantitative delivery was controlled. The surgeons J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 156 C. WIESSNER ET AL. implanting osmotic minipumps were masked with respect to treatment. In addition, brains from animals receiving 7B12, control antibody, or PBS were sampled 2 weeks or 4 weeks after pump implantation (n ⳱ 3 to 5) and frozen at −70°C in Tissue-Tek O.C.T. compound (Sakura, Zoeterwoude, Netherlands). Coronal sections (10 m) of these brains were cut on a cryostat, and 7B12 distribution was visualized using a biotinylated antimouse antibody and the ABC kit (Vector Laboratories, Burlingame, CA, U.S.A.) as recommended by the supplier. Evaluation of sensorimotor performance. Montoya’s staircase test was carried out as described in detail previously (Montoya et al., 1991) and by investigators masked with regard to treatment. Rats were placed in a Plexiglas box with a baited double staircase. Food pellets were placed on the staircase and presented bilaterally at seven graded stages of reaching difficulty to provide objective measures of maximum forelimb extension and grasping skill. Rats were food deprived for at least 24 hours before and throughout the whole weekly test session, being fed once a day with approximately 10 g standard rat chow. A complete test series was done on 4 consecutive days. On the first 2 days, the platform was baited with 4 chow pellets (Dustless Precision Pellets [45 mg]; Bio-Serv, Frenchtown, NJ, U.S.A.) at the far end of the central platform, and in addition stairs 1 and 2 were baited bilaterally with 2 pellets each. The rats were tested twice daily (morning/afternoon) for 10 minutes each. On days 3 to 4, stairs 2 to 6 were bilaterally baited with three pellets each to avoid rats successfully retrieving pellets with their tongue or with the “unaffected” paw. The rats were tested again twice daily for 10 minutes each. After each test series, the total number of pellets grasped and eaten on days 3 to 4 with each forepaw was counted. In addition, the number of displaced pellets was determined. Performance in the staircase test was expressed in percent of the last test session before lesioning (eaten pellets) or in success rate (eaten pellets × 100/[eaten pellets + displaced pellets]). For statistical analysis between groups, two-way repeated-measures ANOVA was used followed by a pairwise multiple comparison procedure (i.e., Bonferroni t-test). For analysis of recovery within the groups, the first test session after lesioning was used as a reference value, and statistical analysis was done using one-way repeated-measures ANOVA. Anterograde tracing with biotinylated dextran amine. Tracing and analysis was performed by an investigator masked with regard to treatment. Location of the forelimb sensorimotor cortex was determined by measuring positions on the skull relative to Bregma (Neafsey et al., 1986). Nine weeks after PCI or 13 weeks after MCAO, pressure injections of a 10% solution of biotinylated dextran amine (10,000 d [Molecular Probes, Eugene, OR, U.S.A.], in 0.01 mol/L phosphate buffer, pH 7.4) were made into the left forelimb sensorimotor cortex (0.5 mm posterior, 2.5 mm lateral; 1.5-mm depth, relative to bregma) through a glass capillary that remained in its position for 2 minutes after the end of the injection. Two weeks after biotinylated dextran amine injection, animals were deeply anesthetized with pentobarbital (450 mg/kg intraperitoneally; Abbott Laboratories, Cham, Switzerland) and perfused transcardially with 100 mL of Ringer solution containing 100,000 IU/L heparin (Liquemin; Roche, Basel, Switzerland) and 0.25% NaNO2 followed by 300 mL of 4% paraformaldehyde in 0.1 mol/L phosphate buffer with 5% sucrose. Brains and spinal cords were dissected and postfixed overnight at 4°C in the same fixative. Meninges were removed and the pons and cervical enlargement (C4–C6) was embedded in a gelatine–chicken albumin solution polymerized with 2.5% glutaraldehyde. Fiftymicrometer coronal sections were cut using a vibratome (Leica J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 vt 1000S). All sections were collected in 50 mmol/L Trisbuffered 0.9% saline, pH 8, and 0.5% Triton X-100 (TBS-Tx). They were serially mounted on slides (Superfrost/Plus; Menzel-Gla¨ ser, Braunschweig, Germany) according to the semifree floating technique (Herzog and Brosamle, 1997). Sections were washed three times for 30 minutes in TBS-Tx before overnight incubation in avidin-peroxidase in TBS-Tx (ABC Elite; Vector Laboratories). The following day, the slides were washed three times for 30 minutes in TBS-Tx. After an additional wash in 50 mmol/L Tris-HCl, pH 8, a preincubation for 10 minutes in 0.4% ammonium nickel sulfate (Sigma, St. Louis, MO, U.S.A.) was performed, followed by a second preincubation in 0.4% ammonium nickel sulfate and 0.015% 3,3⬘diaminobenzidine (DAB; Sigma, Buchs, Switzerland) for 10 minutes. The tissue was then reacted in 0.4% ammonium nickel sulfate, 0.015% DAB, and 0.004% H2O2 in 50 mmol/L Tris buffer, pH 8, for another 10 minutes. The process was stopped by washing with Tris-HCl buffer. The sections were air dried, slightly counterstained with cresyl violet, and coverslipped with Eukitt (Kindler, Freiburg, Germany). Corticospinal projections were quantified by counting the number of axons sprouting across the midline in the pons and in the cervical enlargement. The bilateral innervation of the pons was determined using an image analysis software routine (MCID/M4; Imaging Research, St. Catherines, Ontario, Canada). The pixels per area were automatically quantified in the ipsilateral and contralateral sides after defining a threshold for the background that was kept identical all through the analysis. A ratio between the contralateral and ipsilateral sides was then computed. For the cervical enlargement, the fibers sprouting across the midline were counted manually. Quantification of the total number of fibers labeled in the main corticospinal tract (CST) was also performed to generate a ratio of crossing fibers to account for differences in biotinylated dextran amine labeling. After PCI, successful tracing was achieved in 12 of 13 control-Ab–treated animals and in all 7B12-treated animals (n ⳱ 14). After MCAO, success rates for tracing were 8 of 9 in controlAb–treated animals, and 7 of 9 animals in both groups treated with 7B12. All data were analyzed using a nonparametric Kruskal-Wallis test in case of multiple comparisons followed by nonparametric Mann-Whitney test in case of paired comparisons. Significance was taken to be P < 0.05. RESULTS Generation and characterization of the monoclonal anti–Nogo-A antibody 7B12 The antirat Nogo-A antibody mAb 7B12 has subnanomolar binding for the Nogo-A specific domain NiG (amino acids 174 to 979 of Nogo-A; Chen et al., 2000) (Fig. 1) and within NiG for a part called NiGdelta-6 comprising amino acids 763 to 975 of Nogo-A (Fig. 1; Chen et al., 2000). Details of antibody generation and further characterization have been described elsewhere (Oertle et al., 2000). Briefly, female mice, 5 to 6 weeks old, (C3H- and C57BI6/J-strains) were immunized subcutaneously with recombinant prokaryotically produced rat NiR-G, corresponding to amino acids 1 to 979 of Nogo-A, that is, Nogo-A lacking the C-terminal reticulon domain (Chen et al., 2000). Positive clones were subcloned twice, and the supernatants were collected to ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE FIG. 1. Binding of purified antirat monoclonal antibody (mAb) 7B12 (immunoglobulin G1) to rat NiG (the protein domain specific to Nogo-A) and rat NiG delta-6 fragment (Oertle et al., 2002) using enzyme-linked immunosorbent assay (ELISA). Both proteins were coated in the ELISA plates at a concentration of 2 µg/mL and incubated with different concentrations of 7B12 mAb. The binding of 7B12 to the two proteins was quantified by using a goat antimouse horseradish peroxidase–coupled antibody and peroxidase substrate and reading the optical density (OD) of the color reaction in an ELISA plate reader at 450 nm. Results are means ± SD of samples in at least duplicate wells. Note the binding of the mAb 7B12 to the Nogo-A fragment used for immunization (rat NiG delta-6) and the full-length Nogo-A– specific fragment (rat NiG) at low nanomolar concentrations. be tested on a standard fibroblast spreading test in vitro as described (Spillmann et al., 1998). Like the extensively characterized antibodies IN-1 and AS-472 (Chen et al., 2000), mAb 7B12 recognizes a single 190-kd band in Western blots of rat and mouse oligodendrocyte lysates corresponding to Nogo-A (T. Oertle, unpublished observations, 2002). In addition, in living cultures of oligodendrocytes incubated with 7B12, immunostaining of cell bodies and radial processes was observed, showing that the Nogo-A domain recognized by 7B12 is at the cell surface (T. Oertle, unpublished observations, 2002). Infarct morphology and volumes after photothrombotic cortical injury and 7B12 treatment Lesions were measured noninvasively by T2-weighted MRI 24 hours after PCI, and before the implantation of minipumps (Fig. 2). At this time, hyperintensive regions denoting cytotoxic edema were sharply demarcated in the MRI scan in the right hemisphere (Fig. 3A). The lesions extended from approximately bregma 5.0 mm to bregma −6.0 mm. Affected cortical areas included the frontal cortex (area 1, 2, and 3), parietal cortex, the forelimb and hind-limb area of the cortex, and partly the occipital cortex (according to Paxinos and Watson, 1986) in all animals. Previous experiments had shown that lesions of this type resulted in persisting deficits of grasping performance with the contralateral forepaw, whereas smaller lesions were followed by complete recovery (C. Wiessner, unpublished observations, 2001). The total infarct volume was 308.1 ± 26.7 L (mean ± SD) and 157 313.0 ± 24.3 L in the control-Ab group and the 7B12 group, respectively (Table 1). Thus, both groups had very similar lesion volumes 24 hours after PCI and before Nogo-A antibody treatment was initiated. Magnetic resonance imaging measurements were repeated 9 weeks after PCI, that is, 7 weeks after termination of antibody infusion (Fig. 3A). Loss of brain tissue (brain atrophy) was determined by subtracting the volumes of the lesioned and unlesioned hemisphere. Brain atrophy was very similar in the control-Ab–treated and the 7B12treated groups (Table 1), indicating that 7B12 infusion did not influence the development of brain atrophy. In addition, body weight—a sensitive general indicator for the severity of the brain lesion and of the animal’s health status—was not significantly different among the groups before or at any time point after surgery (Table 1). These results excluded the possibility that any observed differences in sensorimotor performance or fiber sprouting between both groups could be attributed to variations of lesion size, or differences in the general health status of the animals. Behavioral improvement after photothrombotic cortical injury and delayed treatment with 7B12 A skilled forepaw-reaching test was used to evaluate sensorimotor function after PCI by counting food pellets successfully grasped with the left or the right forepaw and subsequently eaten (Montoya’s staircase test, Fig. 3B). Before PCI, rats were trained daily for 2 weeks to establish the baseline performance, which was very similar in the control-Ab and the 7B12 groups (Table 1). In the first week after PCI, grasping performance with the (left) forepaw contralateral to the lesioned (right) hemisphere was reduced to about 10% of prelesion values FIG. 2. Experimental protocol. The time flow of experiments is shown on the left. On the right, the ischemia-induced cortical lesion in the right hemisphere is shown as a shaded area. The site of the brain infusion cannula for pump-controlled antibody infusion was in the left lateral ventricle. The biotinylated dextran amine tracer injection site was in the forelimb region of the left sensorimotor cortex (i.e., contralateral to the lesion). MRI, magnetic resonance imaging; icv, intracerebroventricular. J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 158 C. WIESSNER ET AL. FIG. 3. After photothrombotic cortical injury (PCI), treatment with the anti–Nogo-A antibody 7B12 improved regaining of contralateral forepaw function. (A) Representative example for lesion morphology (bright areas) in the right hemisphere of the same rat 24 hours and 9 weeks after PCI as determined by noninvasive T2-weighted magnetic resonance imaging. (B) As a behavioral readout, Montoya’s staircase test (Montoya et al., 1991), which is an integrative sensorimotor task for the forelimbs, was used. Rats enter the compartment containing the baited staircase voluntarily from an anteroom partially visible on the right. (C) Grasped and eaten pellets with the left forepaw were counted and expressed in percent of baseline (prelesion) performance determined in the last test session before lesioning (Table 1). Performance was significantly better in the 7B12-treated group from 6 weeks after lesion onward. The control group received unspecific mouse immunoglobulin Gs. Two-way repeated-measures analysis of variance: treatment, P = 0.031; time, P = 0.001; time × treatment; P = 0.43; *0.05 versus control group, t-test. (D) Successful attempts (eaten pellets × 100/[eaten pellets + displaced pellets]) with the left forepaw. This measure excluded the possibility that differences resulted from less motivation to use the impaired forepaw in the control group. *0.05 versus control group, t-test. Error bars indicate standard deviation. without significant differences between groups (Fig. 3C). In the control group, grasping ability with the left paw recovered between week 1 and week 6 after lesion, reaching about 55% of prelesion performance without further improvement at 7 and 9 weeks (Fig. 3C). Thus, PCI resulted in a persistent sensorimotor deficit. This result was similar to a previous pilot study, where rats received an intracerebroventricular infusion of PBS after PCI (n ⳱ 8; lesion volume: 310.6 ± 15.5 L). In these animals, grasping ability with the left forepaw was reduced to 12.5% and 56% in week 1 and week 8 after lesion, respectively. In the 7B12-treated group, behavioral improvement also occurred between week 1 and week 6, however, was better than in the control group and reached a plateau at about 70% of prelesion performance, which was significantly different from the control group 6 to 9 weeks after PCI (P < 0.05). Similar results were obtained when the percentage of eaten pellets in relation to the total number of grasping attempts (⳱ successful attempts) was determined (Fig. 3D). This finding excluded differences in motivation to perform the sensorimotor task between the groups. J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 A moderate initial impairment of grasping ability was observed for the (right) forepaw ipsilateral to the lesion, amounting to 65% ± 22% and 67% ± 20% of prelesion performance in the control group and the 7B12 group, respectively. Five weeks after PCI performance had recovered to 92% ± 11% and 91% ± 29% in the control group and 7B12 group, respectively, and remained in the range of 90% to 100% of prelesion performance up to TABLE 1. Body weight and lesion volumes after photothrombotic cortical injury PCI Control-Ab (n ⳱ 13) 7B12 (n ⳱ 14) Baseline performance (%) Body weight, prelesion (g) Body weight, 9 wk (g) Infarct volume, 24 h (L) Brain atrophy, 9 wk (L) 70.2 ± 7.3 235.4 ± 4.6 310.6 ± 14.3 308.1 ± 26.7 91.8 ± 35.6 71.7 ± 6.0 237.0 ± 8.8 310.0 ± 11.6 313.0 ± 24.3 90.5 ± 31.5 Baseline performance is expressed as the rate (%) of successful grasping attempts in the week before photothrombotic cortical injury (PCI); no significant differences were found for any of the parameters shown. Control-Ab, group treated with mouse immunoglobulin G; 7B12, groups treated with monoclonal antibody anti–Nogo-A. ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE 9 weeks after PCI, the latest time point investigated. Differences between the groups were not significant at any time after PCI. Brain distribution of intraventricularly infused antibodies after photothrombotic cortical injury The brain distribution of 7B12 and control antibody was investigated by antimouse IgG immunohistochemistry in brains 2 weeks and 4 weeks after PCI. Two weeks after PCI (i.e., at the end of the infusion period into the left lateral ventricle), a staining gradient from the ventricles and surface staining was found (Fig. 4A). Staining intensity was highest in the left hemisphere, where the antibody was infused, but was also prominent in the lesioned hemisphere. The antibody distribution was widespread and extended far into the caudal direction, including the hippocampus and gray matter of the cervical spinal cord (Fig. 4A). Higher magnification showed predominantly diffuse parenchymal staining for both 7B12 (Fig. 4B) and the control antibody (not shown). Both antibodies were still detectable 4 weeks after PCI (i.e., 2 weeks after removal of the pumps), again showing a very similar distribution pattern (Figs. 4C and E). Instead of the diffuse parenchymal distribu- 159 tion, a more localized pattern was observed, including the lesion border, corpus callosum, dorsolateral striatum (Figs. 4C and E), cerebral peduncle, and the fascicles of the capsula interna (Fig. 4C). In addition, moderate staining of the gray matter in the cervical spinal cord was still observable (Fig. 4C). Higher magnification showed staining of punctate and also elongated structures in the mentioned areas, exemplified for the corpus callosum in Fig. 4D. The precise nature of these structures remains to be determined using techniques such as electron microscopy and double-staining immunohistochemistry. The specificity of detection of mouse IgGs in brain tissue was demonstrated by using brain sections from rats subjected to PCI followed by minipump infusion of the carrier solution (PBS). In this case no staining was observed (Fig. 4F). In antibody-infused but unlesioned animals, 2 weeks after termination of infusion only marginal staining around the infusion site (visible only at highpower magnification) was found (Fig. 4G), indicating an involvement of the brain lesion in the prolonged presence of the infused mouse antibodies in the brain. In summary, these results demonstrated that the mouse IgG1 antibodies were widely distributed in the brain and spinal cord after intraventricular infusion and were still FIG. 4. After photothrombotic cortical injury (PCI) and 2 weeks of intraventricular infusion into the left lateral ventricle, antibodies displayed widespread brain distribution and were still detectable 2 weeks after termination of intracerebroventricular infusion. Mouse immunoglobulin G (IgG), 7B12 or control-Ab groups, was shown by immunostaining with an antimouse IgG antibody. (A) Typical antibody distribution exemplified for 7B12 after 2-week infusion in two brain sections (bregma −0.8 mm to 3.2 mm) and one section from the cervical spinal cord (C5). (Space bar = 1.5 mm.) (B) At higher magnification, mostly diffuse parenchymal distribution of the infused antibodies was observed after 2 weeks of infusion. (Scale bar = 20 µm.) (C) Brain distribution of 7B12 4 weeks after PCI (i.e., 2 weeks after termination of intraventricular pump infusion). Note the clearly detectable but more restricted distribution pattern as compared with A. (D) Higher magnification 4 weeks after PCI showed staining of elongated and punctate structures. As an example, staining in the corpus callosum of a 7B12-infused animal is shown. (Scale bar = 20 µm.) (E) Distribution patterns 4 weeks after PCI were similar for 7B12 and the mouse control–antibody, as exemplified in this image. (F) Only weak background staining was observed in brains of animals receiving infusions of phosphate-buffered saline into the lateral ventricle after PCI, showing the specificity of mouse IgG detection. (G) After intraventricular infusion of antibodies into unlesioned brains, no widespread distribution was found 2 weeks after the end of infusion. (Scale bars in A, C, E, F, G = 1.5 mm.) J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 160 C. WIESSNER ET AL. present in the brain at a time when control-Ab–treated and 7B12-treated animals were beginning to diverge in grasping performance. Anterograde tracing of the pyramidal tract after photothrombotic cortical injury We hypothesized that recovery could be related to neuroanatomic changes of fiber tracts originating in the unlesioned cortex contralateral to the lesion. The anterograde tracer biotinylated dextran amine was, therefore, injected into the forelimb region of the left sensorimotor cortex 9 weeks after PCI. Two weeks later, the cortical projection to the ipsilateral pons showed the typical topographical forelimb-specific innervation pattern as described earlier (Z’Graggen et al., 1998). Labeled fibers running in the cerebral peduncle over the basilar pons left the peduncle ventrally and formed typical termination fields (Figs. 5A and B). We have previously observed that in normal Lewis rats or after pyramidotomy, only very few fibers cross the midline and terminate within the contralateral pontine gray (Wenk et al., 1999; Z’Graggen et al., 1998). In the present study, photothrombotic-lesioned Fischer rats from the control-Ab group showed a prominent bilateral innervation of the pons (Fig. 5A) that, however, was not significantly different in the 7B12-treated group (Figs. 5B and C). The crossed projection formed a termination pattern specific for fibers originating in the forelimb area, mirroring the projections of the ipsilateral side. No correlation between crossed fibers in the pons and grasping performance in the staircase test was found. When fiber outgrowth from the dorsal pyramidal tract in the cervical spinal cord was examined, animals receiving the control antibody showed only few midline crossing fibers (Fig. 5D). Treatment with 7B12 prominently increased the number of midline crossing fibers at this level (Fig. 5E). Quantification confirmed that in the 7B12-treated group, midline crossing increased significantly in the cervical spinal cord from 1.1% ± 0.5% to 2.3% ± 1.5% (P < 0.05) (Fig. 5F). The degree of fiber crossing in the cervical spinal cord correlated significantly with grasping performance 9 weeks after PCI (Fig. 5G). Delayed anti–Nogo-A antibody treatment after middle cerebral artery occlusion in spontaneously hypertensive rats Because hypertension is the single most important risk factor for stroke, we sought to investigate effects of 7B12 in a stroke model in SHR rats—an animal model of genetically determined chronic hypertension resulting in vascular changes and increased susceptibility to brain ischemia (Barone et al., 1992). Permanent focal cerebral ischemia was induced by distal MCAO, resulting in infarcts extending from approximately bregma +3 mm to bregma −5 mm and including the sensorimotor cortex J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 FIG. 5. Midline crossing of corticospinal fibers originating in the unlesioned left sensorimotor cortex after photothrombotic cortical injury (PCI) increased in 7B12-treated animals and correlated with left forepaw function. The anterograde tracer biotinylated dextran amine (BDA) was injected into the left sensorimotor cortex. (A) Cross section at the midpontine level of a control-Ab– treated animal. Note that numerous BDA-labeled fibers end in the contralateral pons (arrows). (B) Cross section at the midpontine level of a 7B12-treated animal showing a similar BDA staining pattern compared with control animals. (C) Quantification of bilateral innervation of the pons at the midpontine level did not disclose significant differences between the groups. (D) Pyramidal tract labeling at the level of the cervical spinal cord in a control animal receiving mouse immunoglobulin G. Substantial midline crossing of fibers is not obvious. (E) In an animal treated with 7B12, numerous pyramidal tract fibers cross the midline and terminate in the gray matter of the left cervical spinal cord (arrows). The inlet shows the fibers marked by the left arrow at higher magnification. (F) For quantification, fibers sprouting across the midline in the cervical spinal cord and the total number of fibers labeled in the right pyramidal tract (originating in the left sensorimotor cortex) were counted and used to generate the ratio of crossing fibers in percent. Error bars indicate standard error. Data were analyzed using nonparametric Mann-Whitney test. Significance was taken at P < 0.05. (G) Percentage of midline crossing fibers in the cervical spinal cord was plotted against performance (success rate [see Fig. 2D] in the last staircase session before tracing for all animals, that is, including 7B12treated and control-Ab–treated animals]. Linear regression analysis showed a significant correlation of fiber crossing the cervical spinal cord and grasping ability. (Scale bar in A, B, D, E = 0.25 mm.) (Fig. 6A). The infarct volume at 24 hours after MCAO amounted to 238.8 ± 51.8 L, 216.5 ± 36.9 L, and 223.8 ± 49.2 L in the control group, the low-dose 7B12 group (1.68 mg), and the high-dose 7B12 group (5 mg), respectively (Table 2). Differences in infarct volume between the groups before treatment were not significant. ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE 161 FIG. 6. Treatment with the anti–Nogo-A antibody 7B12 improved recovery of grasping ability and midline crossing of corticospinal fibers after middle cerebral artery occlusion (MCAO) in spontaneously hypertensive rats. (A) Representative example for the lesion morphology (bright areas) in the right hemisphere 24 hours after MCAO as determined by T2-weighted magnetic resonance imaging. (B) Grasped and eaten pellets with the left forepaw in the staircase test were counted and expressed in percent of baseline performance determined in the last test session before lesioning. Two-way repeated-measures analysis of variance showed a significant time effect (P < 0.001). The significance of time effect within treatment groups was isolated by the StudentNewman-Keuls method (#P < 0.05 versus 4-week test). (C) After anterograde tracing of fibers from the left unlesioned sensorimotor cortex, more pyramidal tract fibers crossing the midline and terminating in the gray matter of the left cervical spinal cord (left part of figure) are obvious in a 7B12-treated animal (right) as compared with a controlAb–infused animal (middle). (D) Quantification of midline crossing fibers in the cervical spinal cord was done exactly as described for the photothrombotic cortical injury experiment (see Fig. 4). Error bars indicate standard deviation. Data were analyzed using nonparametric Kruskal-Wallis test. (E) Midline crossing of fibers in the cervical spinal cord was plotted against performance in the last staircase session (week 12 after MCAO) before tracing for all animals, that is, including both 7B12-treated groups and control-Ab–treated animals. Linear regression analysis showed a significant correlation between fiber crossing in the cervical spinal cord and grasping ability. The same was true for the baseline performance in the staircase test before MCAO (Table 2). Of note, the baseline performance (in absolute terms) of the SHR rats in the staircase test after the 2-week training period was inferior compared with normotensive Fischer rats, and the interindividual variability was higher (Table 2). Because of the invasive nature of MCAO, the first assessment of sensorimotor function could be done 4 weeks after MCAO. At this time, all three groups showed grasping deficits with the paw contralateral to the lesion in the range of about 40% of prelesion performance (Fig. 6B). In the control group, no significant subsequent improvement was observed up to 12 weeks after MCAO, and the deficit remained in the range of 50% of baseline performance, which is in good agreement with previously published data (Grabowski et al., 1993). In contrast, for both 7B12-treated groups, prominent improvement in the staircase test was observed 7 to 12 weeks after MCAO, approaching 70% of prelesion performance. Because of high interindividual variability of TABLE 2. Body weight and lesion volumes after permanent middle cerebral artery occlusion pMCAO (SHR) Control-Ab (n ⳱ 9) 7B12, 1.68 mg (n ⳱ 9) 7B12, 5 mg (n ⳱ 9) Baseline performance (%) Body weight, prelesion (g) Body weight, 12 wk (g) Infarct volume, 24 h (L) 50.4 ± 10.7 212.8 ± 9.4 310.9 ± 9.4 238.8 ± 51.8 48.2 ± 8.8 213.9 ± 6.0 323.7 ± 14.6 216.5 ± 36.9 45.5 ± 8.2 215.0 ± 8.3 313.1 ± 14.1 223.8 ± 49.2 Baseline performance is expressed as the rate (%) of successful grasping attempts in the week before permanent middle cerebral artery occlusion (pMCAO); no significant differences were found for any of the parameters shown. Control-Ab, group treated with mouse immunoglobulin G; 7B12, groups treated with monoclonal antibody anti–Nogo-A; SHR, spontaneously hypertensive rats. J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 162 C. WIESSNER ET AL. SHR rats in the staircase test, two-way repeatedmeasures ANOVA showed that the differences in performance between the groups did not reach significance (P > 0.05); statistical analysis, however, indicated a highly significant time effect. The significance of time effect for the individual groups was isolated by the Student-Newman-Keuls method and showed that, compared with the 4-week measurement, only both 7B12-treated groups significantly (P < 0.05) improved 7 to 12 weeks after MCAO (Fig. 6B). In the group treated with a lower dose of 7B12 (1.68 mg), performance continued to improve until the latest time point measured (12 weeks). From these results, it appeared that the higher dose of 7B12 accelerated the speed of recovery, whereas the maximal level of recovery was similar with both 7B12 doses. Anterograde tracing of the pyramidal tract after middle cerebral artery occlusion Tracing was done as described for PCI, and a similar staining pattern was obtained. At the level of the pons, the mean values for midline crossing fibers were in a similar range as observed for the PCI-lesion experiment, amounting to 7.5% ± 6.5%, 10.1% ± 4.5%, and 15.6% ± 12.5% in the control group, 7B12 (1.68 mg) group, and 7B12 (5 mg) group, respectively. Although there appeared to be a dose-dependent increase of crossing fibers in the pons in this experiment, the differences between the groups were not statistically significant. In line with the findings after PCI, no correlation between midline crossing in the pons and grasping performance with the left paw was found (not shown). In the cervical spinal cord, 1.8% ± 0.8% midline crossing of CST fibers was found in the control-Ab group. Treatment with 7B12 triggered a dose-dependent increased of midline crossing fibers (Fig. 6C), amounting to 2.9% ± 1.6%, and 4.5% ± 2.2% when given at 1.68 mg and 5 mg, respectively (Fig. 6D). Therefore, similar to the PCI experiment, 5 mg of 7B12 more than doubled the number of midline crossing fibers, and this increase was statistically significant (P < 0.05). As for the PCI experiment, a significant correlation between midline crossing fibers in the cervical enlargement and grasping performance determined 12 weeks after MCAO was observed (Fig. 6E). DISCUSSION This study showed that pump-controlled delivery of a Nogo-A–specific antibody (7B12) initiated 24 hours after experimental stroke promoted improvement of long-term neurologic outcome in normotensive and SHR rats. Treated animals showed an increase of midline crossing in the cervical spinal cord of corticospinal fibers originating from the unlesioned sensorimotor cortex (Fig. 7). Midline crossing correlated with grasping abilJ Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 FIG. 7. Diagram of projections from the left forelimb motor cortex to the right cervical spinal cord. A significant increase of midline sprouting to the left side of the cervical spinal cord was observed after treatment with the anti–Nogo-A antibody 7B12 both after photothrombotic cortical injury in normotensive Fischer rats and after middle cerebral artery occlusion in spontaneously hypertensive rats. BDA, biotinylated dextran amine. ity, suggesting a possible contribution of the crossing fibers for behavioral improvement. Pump infusion of 7B12 after experimental stroke improved neurologic outcome The experimental protocol in this study (Fig. 2) was designed to evaluate postacute treatment effects on endpoint behavioral outcome without confounding influences of infarct size. To achieve this goal, lesion volumes were determined 24 hours after stroke by T2weighted MRI before treatment was initiated. It has previously been shown that lesion volumes derived from noninvasive T2-weighted MRI highly correlate with volumes as determined by conventional histologic methods (Rudin et al., 1999). After focal cerebral ischemia in rodents, few sensorimotor tasks uncover permanent deficits (Virley et al., 2000; Hunter et al., 2000). One of these is Montoya’s staircase test (Montoya et al., 1991; Grabowski et al., 1993), which is an integrative sensorimotor task for the forelimbs implicated with cortical as well as subcortical circuitries (Whishaw et al., 1986). Combining Montoya’s staircase test and MRI-controlled cortical ischemia, we showed that grasping ability of the forepaw contralateral to the lesion was permanently depressed in control rats, reaching a plateau at about 50% of baseline performance up to the latest time points investigated (9 to 12 weeks). When rats with infarct volumes MRI-matched to the control group were treated with 7B12 in the postacute phase after stroke (24 hours), grasping ability improved significantly and reached about 70% of baseline levels. These ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE findings agree with a recent study showing improvement of skilled forelimb movements after MCAO by IN-1 hybridoma treatment initiated at the time of MCAO and under immunosuppression (Papadopoulos et al., 2002). Beneficial effects with 7B12 in the present study were observed both in healthy normotensive rats and in SHR, which develop vascular abnormalities, have reduced collateral cerebral blood flow, and show premature mortality (Barone et al., 1993). Thus, these results indicate that anti–Nogo-A antibodies could be a promising rehabilitative treatment approach for human stroke with a prolonged time-to-treatment window. Intraventricular administration of antibodies, however, seems not to be suitable for patients who have had stroke. Considering disturbances of the blood–brain barrier after stroke (Huber et al., 2001), it will be important to explore whether peripheral administration can be achieved. For spinal cord injury and head trauma, the demonstration of efficacy after pump infusion of 7B12 has immediate clinical relevance. In previous studies showing behavioral recovery after CNS injury, the antibody IN-1 was secreted by implanted hybridoma cells under concomitant immunosuppressive treatment with cyclosporin (Z’Graggen et al., 1998; Papadopoulos et al., 2002; Merkler et al., 2001; Raineteau et al., 2001), which would not be applicable to patients. Pump-controlled intrathecal drug administration, however, is an established clinical method that is routinely used after spinal cord injury (Schwab, 2002) and head trauma (Stempien and Tsai, 2000). Intraventricularly infused antibodies of the IgG isotype are cleared rapidly from the cerebrospinal fluid via an Fc-receptor-mediated mechanism and with a half-life of less than an hour (Zhang and Pardridge, 2001). After continuous pump infusion for 2 weeks, however, the IgG1 antibodies in the present study were found at high levels throughout the brain including the cervical spinal cord, indicating a steady-state concentration gradient sufficient to drive penetration. The antibodies were still detectable 2 weeks after termination of infusion in brain structures for which plastic changes have been previously reported after cortical injury, such as the perilesion cortex (Carmichael et al., 2001), the dorsolateral striatum (Kartje et al., 1999; Papadopoulos et al., 2002), and the cerebral peduncle (Wenk et al., 1999). Therefore, it seems that intraventricular infusion of anti–Nogo-A antibodies could be utilized for clinical indications where this route of administration is feasible. Corticospinal plasticity was enhanced after 7B12 treatment and correlated with behavioral outcome Neuroanatomically, 7B12 treatment more than doubled the number of midline crossing CST fibers in the cervical spinal cord originating in the unlesioned sensorimotor cortex in normotensive and SHR rats (Fig. 6). A similar extent of compensatory fiber growth from the 163 CST was found after unilateral CST transection caudal from the lesion after IN-1 hybridoma treatment (Thallmair et al., 1998). Corticospinal projections across the midline have been also described after sensorimotor cortex lesion in neonatal rats (Rouiller et al., 1991), where the degree of spontaneous behavioral recovery after comparable cortical lesions is much better compared with adult animals. In previous studies, plasticity after cortical injury and IN-1 hybridoma treatment has not been investigated in the spinal cord, but interhemispheric fiber outgrowth in corticostriatal (Kartje et al., 1999), corticorubral (Wenk et al., 1999), and corticopontine (Wenk et al., 1999) pathways is well documented. Corticostriatal plasticity was found also after MCAO in black-hooded rats (Papadopoulos et al., 2002). In the present study, the number of corticopontine fibers crossing the midline was relatively high even in control-Ab– treated animals, and there was no increase in the 7B12treated rats. It is important to note that even untreated rats displayed corticospinal fiber crossing in the spinal cord (1% to 2%), although to a significantly lesser degree than 7B12-treated animals. Similar observations were made for interhemispheric corticostriatal fiber outgrowth after cortical ablation (Kartje et al., 1999) or thermocoagulation (Napieralski et al., 1996). The correlation analysis of fiber crossing with endpoint forepaw function for all animals irrespective of treatment showed a significant correlation for both normotensive and SHR rats. It therefore seems that lesion-induced fiber outgrowth in the cervical spinal cord possibly contributed to the behavioral improvement after PCI and MCAO in SHR rats. Importantly, treatment with 7B12 did not induce a qualitatively new fiber outgrowth pattern, but augmented an endogenous lesion-induced plastic capacity of the adult CNS. Without lesion, it has been shown that anti– Nogo-A antibodies induced only short-lasting transient sprouting of Purkinje axons in the adult cerebellum (Buffo et al., 2000). The finding that the correlation coefficients for corticospinal collateral sprouting and behavioral improvement were—although significant—in a moderate range suggests that other brain areas and systems also are involved in the sensorimotor task and that such areas and systems may also be affected by the 7B12 antibody. From previous studies with the antibody IN-1 (see above), it appears that corticostriatal and corticorubral tracts could be involved (Kartje et al., 1999; Papadopoulos et al., 2002). Spontaneous although limited improvement of deficits after experimental and clinical stroke is well recognized, and functional takeover in the unlesioned hemisphere has been implicated as a mechanism for recovery after stroke by functional MRI studies. These studies showed that electrical forelimb (Dijkhuizen et al., 2001) or hind-limb stimulation (Abo et al., 2001) resulted in activation of normally silent brain J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 164 C. WIESSNER ET AL. regions ipsilateral to stimulation. Noninvasive imaging techniques such as positron emission tomography, functional MRI, transcranial magnetic simulation, and magnetoencephalography have been used to investigate functional organization of the cortex after stroke in humans (Nudo et al., 2001; Pineiro et al., 2001). These studies provided evidence that recovery of hand function was associated with increased bilateral activation of brain areas. Experimental and clinical studies also showed that reorganization in the ipsilateral injured cortex is a very important mechanism for recovery after stroke (Abo et al., 2001; Carmichael et al., 2001; Dijkhuizen et al., 2002; Nudo et al., 1996; Pineiro et al., 2001). Plastic changes in the lesioned hemisphere are also likely to play an important role in behavioral improvement in our experimental paradigms. Whether and how anti–NogoA antibody treatment influences plasticity and sprouting in the injured hemisphere will be addressed in future studies. Underlying mechanisms for compensatory sprouting in the spinal cord The Nogo-A–specific domain inhibits neurite outgrowth and causes growth cone collapse in neurons via an elusive receptor (Oertle et al., 2002) that is distinct from the Nogo-66 receptor NgR (Fournier et al., 2001), and involves Rho-mediated downstream signaling to the cytoskeleton (De Marco et al., 2002). Creation of a permissive environment facilitating fiber outgrowth therefore requires the local presence of the neutralizing antibody. In our study the presence of 7B12 in the spinal cord after intraventricular infusion can explain the effect on fiber outgrowth from the unlesioned pyramidal tract. In addition, tonic Nogo-A–dependent inhibition of growth-related genes in the cell bodies of cortical neurons may be released by Nogo-A neutralization with 7B12 in cortical parenchyma. At present, it cannot be excluded that 7B12 (or other anti–Nogo-A antibodies) do not only neutralize Nogo-A by binding to extracellular epitopes, but that binding results in an internalization and thus downregulation of Nogo-A. In vitro and in vivo studies have shown that anti–Nogo-A antibody IN-1 induced the expression of growth-related genes, such as c-jun, junD, synaptophysin, and GAP-43 (Zagrebelsky et al., 1998; Huber and Schwab, 2000). In summary, the results of this study suggest that anti– Nogo-A antibodies bear potential as a new rehabilitative treatment for ischemic stroke with a time-to-treatment window of at least 24 hours. Although the precise mechanisms of the beneficial effects of anti–Nogo-A antibodies in the presented experimental stroke models need to be further explored, the results indicate that compensatory growth of corticofugal fibers could be involved. J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003 Acknowledgments: The authors thank Pascale Brebbia, Francesco D’Amato, Thomas Hafner, and Willi Theilka¨ s for their excellent technical help. REFERENCES Abo M, Chen Z, Lai LL, Reese T, Bjelke B (2001) Functional recovery after brain lesion-contralateral neuromodulation: an fMRI study. Neuroreport 12:1543–1547 Allegrini PR, Sauer D (1992) Application of magnetic resonance imaging to the measurement of neurodegeneration in the rat brain: MRI data correlate strongly with histology and enzymatic analysis. Magn Reson Imag 10:773–778 Barone FC, Price WJ, White RF, Willette RN, Feuerstein GZ (1992) Genetic hypertension and increased susceptibility to cerebral ischemia. Neurosci Behav Rev 16:219–233 Barone FC, Clark RK, Price WJ, White RF, Feuerstein GZ, Storer BL, Ohlstein EH (1993) Neuron-specific enolase increases in cerebral and systemic circulation following focal ischemia. Brain Res 623:77–82 Buffo A, Zagrebelsky M, Huber AB, Skerra A, Schwab ME (2000) Application of neutralising antibodies against NI-35/250 myelinassociated neurite outgrowth inhibitory proteins to the adult rat cerebellum induces sprouting of uninjured Purkinje cell axons. J Neurosci 20:2275–2286 Carmichael ST, Wei L, Rovainen CM, Woolsey TA (2001) New patterns of intracortical projections after focal cortical stroke. Neurobiol Dis 8:910–922 Caroni P, Schwab ME (1988) Antibody against myelin-associated inhibitor of neurite growth neutralizes nonpermissive substrate properties of CNS white matter. Neuron 1:85–96 Chen MS, Huber AB, van der Haar ME, Frank M, Schnell L, Spillmann AA, Christ F, Schwab ME (2000) Nogo-A is a myelin-associated neurite outgrowth inhibitor and an antigen for monoclonal antibody IN-1. Nature 403:434–439 Del Zoppo GJ (2000) Antithrombotic treatments in acute ischemic stroke. Curr Opin Hematol 7:309–315 De Marco SJ, Noth P, Oertle T, Schwab ME, Bandtlow CE (2002) The neurite outgrowth inhibitor Nogo-A activates the Rho-A pathway. Program no. 333.11. 2002 Abstract Viewer/Itinerary Planner. Washington, DC: Society for Neuroscience. Available at: http://sfn.scholarone.com/ Dijkhuizen RM, Ren J, Mandeville JB, Wu O, Ozdag FM, Moskowitz MA, Rosen RB, Finklestein SB (2001) Functional magnetic resonance imaging of reorganization in rat brain after stroke. Proc Natl Acad Sci U S A 98:12766–12771 Fournier AE, Grand Pre´ T, Strittmatter SM (2001) Identification of a receptor mediating Nogo-66 inhibition of axonal regeneration. Nature 409:341–346 Gillum RF, Sempos CT (1997) The end of the long-term decline in stroke mortality in the Unites States? Stroke 28:1507–1517 Grabowski M, Brundin P, Johansson BB (1993) Paw-reaching, sensorimotor, and rotational behavior after brain infarction in rats. Stroke 24:889–895 Grand Pre´ T, Nakamura F, Vartanian T, Strittmatter SM (2000) Identification of the Nogo inhibitor of axon regeneration as a reticulon protein. Nature 403:439–444 Herzog A, Brosamle C (1997) Semifree-floating treatment—a simple and fast method to process consecutive sections for immunohistochemistry and neuronal tracing. J Neurosci Methods 72:57–63 Huber AB, Schwab ME (2000) Nogo-A, a potent inhibitor of neurite outgrowth and regeneration. Biol Chem 381:407–419 Huber JD, Egleton RD, Davis TB (2001) Molecular physiology and pathophysiology of tight junctions in blood-brain barrier. Trends Neurosci 24:719–725 Hunter AJ, Hatcher J, Virley D, Nelson P, Irving E, Hadingham SJ, Parsons AA (2000) Functional assessments in mice and rats after focal stroke. Neuropharmacology 39:806–816 Kapfhammer JP, Schwab ME (1994) Inverse patterns of myelination and GAP-43 expression in the adult CNS: neurite outgrowth inhibitors as regulators of neuronal plasticity. J Comp Neurol 340:194–206 ANTI–NOGO-A ANTIBODY TREATMENT AFTER STROKE Kartje-Tillotson GL, Neafsey EJ, Castro AJ (1986) Topography of corticopontine remodeling after cortical lesion in newborn rats. J Comp Neurol 250:206–214 Kartje GL, Schulz MK, Lopez-Yunez A, Schnell L, Schwab ME (1999) Corticostriatal plasticity is restricted by myelin-associated neurite growth inhibitors in the adult rat. Ann Neurol 45:778–786 Kolb B, Gibb R, Van der Kooy D (1992) Cortical and striatal structure and connectivity are altered by neonatal hemidecortication in rats. J Comp Neurol 322:311–324 Leong SK, Lund RD (1973) Anomalous bilateral corticofugal pathways in albino rats after neonatal lesions. Brain Res 62:218–221 Martinez-Vila E, Sieira P (2001) Current status and perspectives of neuroprotection in ischemic stroke treatment. Cerebrovasc Dis 11 (suppl 1):60–70 Merkler D, Metz GAS, Raineteau O, Dietz V, Schwab ME, Fouad K (2001) Locomotor recovery in spinal cord-injured rats treated with an antibody neutralizing the myelin-associated neurite growth inhibitor Nogo-A. J Neurosci 21:3665–3673 Milner B (1974) Functional recovery after lesions of the brain. Part III: developmental processes in neural plasticity: sparing of language functions after early unilateral brain damage. Neurosci Res Program Bull 12:213–217 Montoya CP, Campbell-Hope LJ, Pemberton KD, Dunnet SB (1991) The “staircase test”: a measure of independent forelimb reaching and grasping abilities in rats. J Neurosci Methods 36:219–228 Napieralski JA, Butler AK, Chesselet MF (1996) Anatomical and functional evidence for lesion-specific sprouting of corticostriatal input in the adult rat. J Comp Neurol 373:484–497 National Institute of Neurological Disorder and Stroke rt-PA Study Group (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581–1587 Naus CC, Flumerfelt BA, Hrycyshyn AW (1985) An anterograde HRPWGA study of aberrant corticorubral projection following neonatal lesions of the rat sensorimotor cortex. Exp Brain Res 59:365–371 Neafsey EJ, Bold EL, Haas G, Hurley-Gius KM, Quirk G, Sievert CF, Terreberry RR (1986) The organization of the rat motor cortex: a microstimulation mapping study. Brain Res 396:77–96 Nudo RJ, Wise BM, SiFuentes F, Miliken GW (1996) Neural substrates for the effects of rehabilitative treatment in motor recovery after ischemic stroke. Science 272:1791–1794 Nudo RJ, Plautz EJ, Frost SB (2001) Role of adaptive plasticity in recovery after damage to motor cortex. Muscle Nerve 24:1000– 1019 Oertle T, Bandtlow C, Schwab ME (2000) Characterization of the gene structure and the inhibitory regions of Nogo/RTN4 [Abstract]. Soc Neurosci Abstr 26:573 Oertle T, Buss A, Dodd D, van der Haar ME, Robeva A, Burfeind P, Vallon R, Schwab ME (2002) Membrane topologies and receptors of the oligodendrocyte protein Nogo-A. Program no. 333.1 2002 Abstract Viewer/Itinerary Planner. Washington, DC: Society for Neuroscience. Available at: http://sfn.scholarone.com/ Papadopoulos CM, Tsai S-Y, Alsbiei T, O’Brien TE, Schwab ME, Kartje GL (2002) Functional recovery and neuroanatomical plasticity following middle cerebral artery occlusion and IN-1 antibody treatment in adult rat. Ann Neurol 51:433–441 Paxinos G, Watson C (1986) The rat brain in stereotaxic coordinates, 2nd ed. London: Academic Press Pineiro R, Pendlebury S, Johansen-Berg H, Matthews PM (2001) Functional MRI detects posterior shifts in primary sensorimotor cortex activation after stroke: evidence of local adaptive organization? Stroke 32:1134–1139 Prinjha R, Moore SE, Christie G, Michalovich D, Simmons DL, Walsh FS (2000) Inhibitor of neurite outgrowth in humans. Nature 403:383–393 Raineteau O, Fouad K, Noth P, Thallmair M, Schwab ME (2001) Functional switch between motor tracts in the presence of the mAb IN-1 in the adult rat. Proc Natl Acad Sci U S A 98:6929–6934 165 Rouiller EM, Liang FY, Moret V, Wiesendanger M (1991) Trajectory of redirected corticospinal axons after unilateral lesion of the sensorimotor cortex in neonatal rat; a phaseolus vulgarisleucoagglutinin (PHA-L) tracing study. Exp Neurol 114:53–65 Rudin M, Beckmann N, Porszasz R, Reese T, Bochelen D, Sauter A (1999) In vivo magnetic resonance methods in pharmaceutical research: current status and perspectives. Magn Reson Imag 15:69–97 Schnell L, Schwab ME (1990) Axonal regeneration in the spinal cord produced by an antibody against myelin-associated neurite growth inhibitors. Nature 343:269–272 Schwab ME (2002) Repairing the injured spinal cord. Science 295:1029–1031 Spillmann AA, Bandtlow CE, Lottspeich F, Keller F, Schwab ME (1998) Identification and characterization of a bovine neurite growth inhibitor (bNI-220). J Biol Chem 273:19283–19293 Stapf C, Mohr JP (2002) Ischemic stroke therapy. Annu Rev Med 53:453–475 Stempien L, Tsai T (2000) Intrathecal baclofen pump use for spasticity: a clinical survey. Am J Phys Med Rehabil 79:536–541 Thallmair M, Metz GAS, Z’Graggen WJ, Raineteau O, Kartje GL, Schwab ME (1998) Neurite outgrowth inhibitors restrict plasticity and functional recovery following corticospinal tract lesion. Nature Neurosci 1:124–131 Virley D, Beech JS, Smart SC, Williams SCR, Hodges H, Hunter AJ (2000) A temporal MRI assessment of neuropathology after transient middle cerebral artery occlusion in the rat: correlation with behavior. J Cereb Blood Flow Metab 20:563–582 Watson BD, Dietrich WD, Busto R, Wachtel MS, Ginsberg MD (1985) Induction of reproducible brain infarction by photochemically initiated thrombosis. Ann Neurol 17:497–504 Wenk CA, Thallmair M, Kartje GL, Schwab ME (1999) Increased corticofugal plasticity after unilateral cortical lesions combined with neutralization of the IN-1 antigen in adult rats. J Comp Neurol 410:143–157 Whishaw IQ, O’Connor WT, Dunnett SB (1986) The contributions of motor cortex, nigrostriatal dopamine and caudate-putamen to skilled forelimb use in the rat. Brain 109:805–843 Whishaw IQ, Kolb B (1988) Sparing of skilled forelimb reaching and corticospinal projections after neonatal motor cortex removal of hemidecortication in the rat: support for the Kennard doctrine. Brain Res 451:97–114 Wiessner C, Sauer D, Alaimo D, Allegrini PR (2000) Protective effect of a caspase inhibitor in models for cerebral ischemia in vitro and in vivo. Cell Mol Biol 46:53–62 Yu X, Moret V, Rouiller EM (1995) Re-examination of the plasticity of the corticothalamic projection after unilateral neonatal lesion of the sensorimotor cortex in the rat: a phaseolus vulgaris leucoagglutinin tracing study. J Brain Res 91:123–133 Zagrebelsky M, Buffo A, Skerra A, Schwab ME, Strata P, Rossi F (1998) Retrograde regulation of growth-associated gene expression in adult rat Purkinje cells by myelin-associated neurite outgrowth inhibitory proteins. J Neurosci 18:7912–7929 Z’Graggen WJ, Metz GAS, Kartje GL, Thallmair M, Schwab ME (1998) Functional recovery and enhanced corticofugal plasticity after unilateral pyramidal tract lesion and blockade of myelinassociated neurite growth inhibitors in adult rats. J Neurosci 18:4744–4757 Z’Graggen WJ, Fouad K, Raineteau O, Metz AS, Schwab ME, Kartje GL (2000) Compensatory sprouting and impulse rerouting after unilateral pyramidal tract lesion in neonatal rats. J Neurosci 20:6561–6569 Zhang Y, Pardridge WM (2001) Mediated efflux of IgG molecules from brain to blood across the blood-brain barrier. J Neuroimmunol 114:168–172 J Cereb Blood Flow Metab, Vol. 23, No. 2, 2003





© Copyright 2026