
Continuous Glucose Monitoring in the ICU: Meeting a Critical Unmet
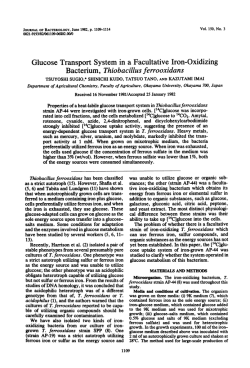
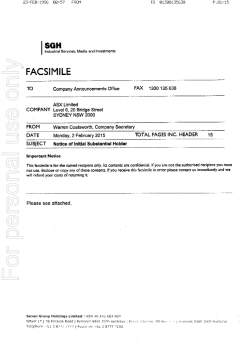
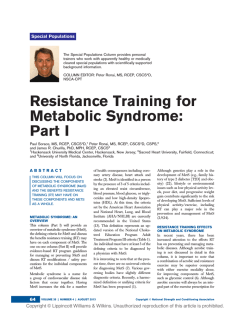
FIRST IN A SERIES SPONSORED BY Continuous Glucose Monitoring in the ICU: Meeting a Critical Unmet Need Aiming to Achieve Better Glucose Management Practices Inpatient glucose control has become an important standard of care for limiting hospital morbidity and mortality, however, good glucose control is difficult to achieve. Today, the importance of inpatient glycemic management – especially among the critically ill – is well appreciated, whether in patients undergoing cardiac surgery, neurosurgery, post myocardial infarction or other critical illness. Studies have shown reduced morbidity and mortality in those whose glucose has been controlled to less than 10 mmol/L, (180 mg/dL).1-8 However, ongoing surveillance and clinical studies have shown that good glycemic control is difficult to achieve, and remains elusive for most hospital settings.9, 10 Multi-disciplinary teams supporting development and implementation of evidence-supported protocols have become the new standard as institutions work to improve glucose control within the critical care setting. These protocols and procedures can vary among hospitals, between nursing units within hospitals, and even between managing clinicians.9 And, importantly, the one consensus among societies across specialties regarding glycemic management appears to be that there is no consensus on what the standard glucose target should be. Glucose Control Improves Outcomes Much of the research demonstrating the benefit of glucose control has come from notable European institutions.11-13 While the range of sophistication of these programs, protocols and procedures varies from paper-based instructions to highly complex computer algorithms, the evidence suggests that improved outcomes can be achieved: Reduced morbidity • At 12 months, with a total of 1548 patients enrolled, the insulin therapy protocol used in Leuven I, helped reduce bloodstream infections by 46%, acute renal failure requiring dialysis or hemofiltration by 41%, the median number of red-cell transfusions by 50%, and critical-illness polyneuropathy by 44%.12 Reduced mortality • The intensive insulin therapy in the Leuven I trial reduced mortality during intensive care from 8.0% with conventional treatment to 4.6%, with the greatest reduction in mortality involving deaths due to multiple organ failure with a proven septic focus. Overall in-hospital mortality was reduced by 34%.12 Prior to the Leuven trials, hyperglycemia was considered common during critical illness.14 This stress hyperglycemia was deemed a beneficial, adaptive response to provide energy substrate to those organs such as brain, cardiac and renal cells that rely on glucose during the hypermetabolic stress state.14 While it seems clear that the findings from the Leuven trials created a paradigm shift with respect to glucose management in the ICU, there is still a great deal of ground to cover to reach the optimal methods for safe glucose control in critically ill patients. Additionally, the initial enthusiasm for tight glucose Morbidity and Mortality Reduction 60 50 40 41% 44% 46% 50% 34% 30 20 10 0 Mortality Acute Renal Failure Polyneuropathy Bloodstream Red cell Infections Transfustions Van den Berghe et al., N Engl J Med. 2001; 345:1359-67 control that followed the first Leuven trial has been tempered by the less favorable findings of the NICE-SUGAR study.15 As the pendulum swings back towards less intensive glucose management practices, the conversation continues to intensify in an effort to drive to a consensus. A recent publication from several of the NICE-SUGAR investigators concludes that the available clinical trial data does not support widespread adoption of intensive glucose control in critically ill patients, but neither does it support ignoring glucose control.16 In spite of measurable progress, much of the initial promise of tight glycemic control has not been realized,15-18 leaving a significant unmet need in the critically ill population. Questions about ideal glucose target ranges and current practice limitations go unresolved, inhibiting the evolution of glucose management in the ICU. What is the ideal blood glucose target range? Is there an absolute target or is controlling variability more important? • Prior to the paradigm shift in glucose management in 2001, most intensivists allowed blood glucose levels to remain high, unless the levels exceeded 11 to 12 mmol/L, (200 to 215 mg/dL). However, the Leuven trials showed the merits of keeping patients in a normoglycemic range of 4.4 to 6.2 mmol/L (80 to 110 mg/dL).12 • In 2007, international recommendations for glucose control in adult, non-diabetic critically ill patients were developed by the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD)19 and more recently by French Society of Anesthesia and Intensive Care which validated experts from other societies within the European Union13 stating “A glucose target of less than 10 mmol/L is strongly suggested, using intravenous insulin following a standard protocol [...]. Definition of the severe hypoglycemia threshold of 2.2 mmol/L is recommended, regardless of the clinical signs.” • In 2009, the US societies ADA and AACE established glycemic target ranges in response to the NICE SUGAR trial of 7.8 to 10.2 mmol/L, (140mg/dL to 180 mg/dL).20 Recent publications are in broad agreement with the ADA recommendations for targeting glucose concentration, generally between 140 and 180 mg/dL (8-10 mmol/L) once insulin is started.16,21 Although these ranges minimize risk of severe hypoglycemia [as defined by blood glucose less than or equal to 2.2 mmol/L (40 mg/dL)], advocates of tighter glycemic control are concerned that the benefits of glycemic control as established by the Leuven I and Leuven II studies will no longer be realized.11 Additionally, with all of the discussion around ideal target ranges, there is growing research and interest into the effects of glycemic variability (GV) on patient outcomes. One study concluded that GV was strongly related to increasing mortality in a heterogeneous population of critically ill patients and that patients in the lowest quartile of GV had shorter lengths of stay.22 How much does typical frequency of testing (q1-q4 hrs) limit the ability to detect and/or avoid hypoglycemia and Blood Glucose Measurements (2 hour protocol) dangerous excursions? • Hypoglycemia is strongly independently associated with increased mortality and increased intensive care unit length of stay16, 23-25 and close monitoring Target Range for Blood Glucose Level of glucose blood levels is strongly recommended for the early detection of severe hypoglycemia.13 0 2 4 6 8 10 Time (hours) • Some guidelines even recommend BG testing ranging from every 30 minutes to 2 hours for patients receiving IV insulin infusions.20 • Researchers employing continuous glucose monitoring (CGM) technology have demonstrated the ability to identify hypoglycemic events that were otherwise missed with standard glucose monitoring, and detected hypoglycemic excursions hours before the patient exhibits symptoms alerting healthcare providers to the event.26 • Additionally, studies using real time CGM devices have shown reduced rates of hypoglycemic episodes because the ability to monitor trends enables clinicians to detect lower glucose levels and reverse them before dangerous levels are reached.27, 28 A consensus for these questions and others will be addressed with ongoing scientific investigation. However, a fundamental underlying limitation remains in the method by which glucose is most commonly measured and the resulting impact on protocol administration, safety and efficacy. Protocols requiring hourly (or less frequent) blood glucose measurements are leaving gaps of time and data between measures and may be insufficient to realize the full benefits of glycemic management.12 This is specifically a concern in the prevention of hypoglycemia, since recent studies have shown that even mild hypoglycemia, BG less than 3.9 mmol/L (BG < 70 mg/dL) is independently associated with increased risk of mortality.23 Unmet Needs = New Opportunities Continuous glucose monitoring technology represents a significant step toward realizing the promised, but as yet unrealized benefits of glycemic control among the critically ill. The evolution of glycemic management has reached a stage where new technology, such as inpatient CGM tools, are necessary to optimize glucose management and ultimately clinical and economic outcomes.9, 29, 30 Continuous Glucose Measurements Continuous glucose monitoring can reveal the trend of a glucose Unnoticed excursions excursion from a normal and stable glucose level to an impending, unstable and abnormal level. With this information, clinicians can be Predictive alarms could help to reduce number and severity of hypoglycemic events proactive rather than reactive 0 2 4 6 8 10 in adjusting insulin dosing and Time (hours) limit iatrogenic glucose variability resulting from insulin dosing adjustments. CGM devices also provide the opportunity to assess glycemic variability and may lead to a greater understanding of variability data within individual patients and across heterogeneous populations.22, 31, 32 What is needed is new, commercially supported technology that enables greater visibility into glucose levels without a proportionate increase in nursing burden, patient inconvenience or costs. Evolution toward Continuous Glucose Monitoring in the ICU The current body of knowledge on this topic leads to one conclusion; that glucose management in the ICU is far from optimal. As we move towards creating better solutions, real time CGM offers the possibility of performing clinical trials without increased rates of hypoglycemia because CGM not only detects excursions but helps investigators prevent them.24 A commercial CGM solution designed to monitor critically ill patients in the ICU has the potential to provide the necessary visibility into glycemic variability while supporting more predictive (versus reactive) glycemic management. This new tool should enable clinicians to monitor glucose in a timely way, and manage glucose levels to a target without increasing the risk of dangerous hypoglycemic events. Ultimately, use of CGM technology could be instrumental in driving the evolution of safe and effective glucose management protocols that will support more consistent glycemic management standards within ICU’s and across institutions. Works Cited: 1. The NICE-SUGAR Study Investigators, Intensive versus Conventional Glucose Control in Critically Ill Patients. N Engl J Med. 2009 Mar 26;360(13):1283-1297. Epub 2009 Mar 24. NICE-SUGAR online abstract at http://ajrccm.atsjournals.org/cgi/data/172/11/1358/ DC1/1 2. Furnary AP, Cheek DB, Holmes SC et al. Achieving tight glycemic control in the operating room: lessons learned from 12 years in the trenches of a paradigm shift in anesthetic care. Semin Thorac Cardiovasc Surg. 2006; 18: 339–345. 3. Moyer MT. Performance improvement measures in achieving glycemic control in the acute brain injury population. J Neurosci Nurs. 2009; 41:72-82. 4. Kosiborod M, Rathore SS, Inzucchi SE et al. Admission glucose and mortality in elderly patients hospitalized with acute myocardial infarction: implications for patients with and without recognized diabetes. Circulation. 2005; 111: 3078–3086. 5. Kosiborod M, Inzucchi SE, Krumholz HM et al. Glucose normalization and outcomes in patients with acute myocardial infarction. Arch Intern Med. 2009; 169: 438–446. 6. Deedwania P, Kosiborod M, Barrett E et al. Hyperglycemia and acute coronary syndrome: a scientific statement from the American heart association diabetes committee of the council on nutrition, physical activity, and metabolism. Circulation. 2008; 117: 1610–1619. 7. Sinnaeve PR, Steg PG, Fox KA et al. Association of elevated fasting glucose with increased short-term and 6-month mortality in st-segment elevation and non-st-segment elevation acute coronary syndromes: the global registry of acute coronary events. Arch Intern Med. 2009; 169: 402–409. 8. Bagshaw SM, Egi M, George C, et al. Early blood glucose control and mortality in critically ill patients in Australia. Crit Care Med. 2009; 37:463-470. 9. Cook CB, Elias B, Kongable G, et al. Diabetes and hyperglycemia quality improvement efforts in hospitals in the United States: current status, practice variation and barriers to implementation. Endocr Pract. 2010; 16:219-230. 10. Swanson CM, Potter DJ, Kongable G, Cook CB, et al. An update on inpatient glycemic control in US hospitals. Endocr Pract. 2012; DOI:10.4158/EP11042.OR. 11. Mesotten, G. Van den Berghe, G. Clinical benefits of tight glycaemic control: focus on the intensive care unit. Best Pract Res Clin Anaesthesiol. 2009; 23: 421–429. 12. Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Eng J Med. 2001; 345:1359-1367. 13. Ichai C, Preiser JC, et al. International recommendations for glucose control in adult non-diabetic critically ill patients. Critical Care. 2010; 14:R166. 14. Mizock BA. Alterations in carbohydrate metabolism during stress: a review of the literature. Am J Med. 1995; 98:75–84. 15. The NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Eng J Med. 2009; 360:1283-1297. 16. Egi M, Finfer S, Bellomo R. Glycemic control in the ICU. Chest. 2011; 140: 212-220. 17. Weiner RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: A meta-analyses. JAMA. 2008; 300:933-944. 18. Griesdale DE, de Souza RJ, van Dam RM, et al. Intensive insulin therapy and mortality among critically ill patients: a metaanalysis including NICE-SUGAR Study data. Canadian Medical Anesthesia Journal. 2009; 180:821-827. 19. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD), Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. Eur Heart J. 2007; 28:88-136. 20. Moghissi E, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists/American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009; 15:353-369. 21. Kavanagh B, McCowen K, Glycemic control in the ICU. N Eng J Med. 2010; 363:2540-2546. 22. Krinsley J, Glycemic Variability: A strong independent predictor of mortality in critically ill patients. Crit Care Med. 2008. 36:3008-3013. 23. Krinsley JS, Schultz MJ, Spronk PE et al., Mild hypoglycemia is strongly associated with increased intensive care unit length of stay. Ann Intensive Care. 2011; 1:49 24. Egi M , Bellomo R , Stachowski E , et al. Hypoglycemia and outcome in critically ill patients. Mayo Clin Proc . 2010; 85:217-224. 25. Hermanides J, Bosman RJ, Vriesendorp TM. Hypoglycemia is associated with intensive care unit mortality. Crit Care Med. 2010; 38:1430-1434. 26. Ryan MT, Savarese VW, Hipszer B, Dizdarevic I, Joseph M, Shively N, Joseph JI. Continuous glucose monitor shows potential for early hypoglycemia detection in hospitalized patients. Diabetes Technol Ther. 2009; 11:745-747. 27. Holzinger I, Warszawska J, Kitzberger R, et al., Real time continuous glucose monitoring in critically ill patients: A prospective, randomized trial. Diabetes Care. 2010; 33:467-472. 28. Brunner R, Kitzberger, R, Miehsler W, et al., Accuracy and reliability of a subcutaneous continuous glucose-monitoring system in critically ill patients. Crit Care Med. 2011; 39:1-6. 29. Miller M, Skladany MJ, Ludwig CR, and Guthermann JS. Convergence of continuous glucose monitoring and in-hospital tight glycemic control: closing the gap between caregivers and industry. J Diabetes Sci Technol. 2007: 903-906. 30. Joseph J, Hipszer B, Mraovic B, et al. Clinical need for continuous glucose monitoring in the hospital. J Diabetes Sci Technol. 2009; 3: 1309-1318. 31. Egi M, Bellomo R, Reade MC. Is reducing variability of blood glucose the real but hidden target of intensive insulin therapy? Critical Care. 2009; 13:302. 32. Monnier L, Colette C, Owens DR. Glycemic variability: the third component of the dysglycemia in diabetes. Is it important? How to measure it? J Diabetes Sci Technol. 2008; 2:1094-1100. 9404610-011 20120316 © Medtronic MiniMed, Inc. 2012. All rights reserved.






© Copyright 2026