
Resistance Training for Metabolic Syndrome: Part I
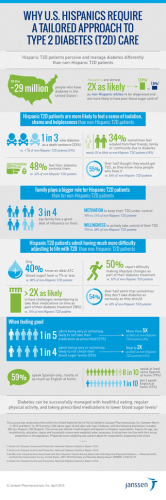
Special Populations The Special Populations Column provides personal trainers who work with apparently healthy or medically cleared special populations with scientifically supported background information. COLUMN EDITOR: Peter Ronai, MS, RCEP, CSCS*D, NSCA-CPT Resistance Training for Metabolic Syndrome: Part I Paul Sorace, MS, RCEP, CSCS*D,1 Peter Ronai, MS, RCEP, CSCS*D, CSPS,2 and James R. Churilla, PhD, MPH, RCEP, CSCS3 1 Hackensack University Medical Center, Hackensack, New Jersey; 2Sacred Heart University, Fairfield, Connecticut; and 3University of North Florida, Jacksonville, Florida ABSTRACT THIS COLUMN WILL FOCUS ON DISCUSSING THE COMPONENTS OF METABOLIC SYNDROME (MetS) AND THE BENEFITS RESISTANCE TRAINING (RT) MAY HAVE ON THESE COMPONENTS AND METS AS A WHOLE. METABOLIC SYNDROME: AN OVERVIEW This column (Part I) will provide an overview of metabolic syndrome (MetS), the defining criteria for MetS and discuss the benefits resistance training (RT) may have on each component of MetS. The one on one column (Part II) will provide evidence-based RT program guidelines for managing or preventing MetS and discuss RT modifications / safety precautions for the individual components of MetS. Metabolic syndrome is a name for a group of cardiovascular disease risk factors that occur together. Having MetS increases the risk for a number 64 of health consequences including coronary artery disease, heart attack and stroke (2). MetS is identified in a person by the presence of 3 of 5 criteria including an elevated waist circumference, blood pressure, blood glucose, or triglycerides and low high-density lipoproteins (HDL). At this time, the criteria set by the American Heart Association and National Heart, Lung, and Blood Institute (AHA/NHLBI) are currently recommended in the United States (13). This definition represents an updated version of the National Cholesterol Education Program Adult Treatment Program III criteria (Table 1). An individual must have at least 3 of the defining criteria to be diagnosed by a physician with MetS. It is interesting to note that at the present time, there are no universal criteria for diagnosing MetS (7). Various governing bodies have slightly different diagnostic criteria. Recently, a harmonized definition or unifying criteria for MetS has been proposed (1). VOLUME 35 | NUMBER 4 | AUGUST 2013 Although genetics play a role in the development of MetS (e.g., family history of type 2 diabetes [T2D] and obesity) (22), lifestyle or environmental issues such as low physical activity levels, poor diet, and progressive weight gain contribute significantly to the risk of developing MetS. Sufficient levels of physical activity/exercise, including RT can play a major role in the prevention and management of MetS (2,9,24). RESISTANCE TRAINING EFFECTS ON METABOLIC SYNDROME In recent years, there has been increased attention to the effects RT has on preventing and managing metabolic diseases. Although aerobic training is not discussed in detail in this column, it is important to note that a combination of aerobic and resistance exercise may be superior compared with either exercise modality alone, for improving components of MetS, such as glycemic control (6). Although aerobic exercise will always be an integral part of the exercise prescription for Copyright Ó National Strength and Conditioning Association RT does contribute to overall caloric expenditure, it is generally recommended as an adjunct to aerobic or endurance training in persons with dyslipidemia (2). Table 1 Defining criteria for metabolic syndromea Elevated waist circumference Men—equal to or greater than 40 in. (102 cm) PREHYPERTENSION/ HYPERTENSION Women—equal to or greater than 35 in. (88 cm) Elevated triglycerides Equal to or greater than 150 mg/dL or on pharmacotherapyb Reduced high-density lipoproteins (HDL cholesterol) Men—less than 40 mg/dL or on pharmacotherapyb Women—less than 50 mg/dL or on pharmacotherapyb Elevated blood pressure Equal to or greater than 130/85 mm Hg or on pharmacotherapyb Elevated fasting glucose Equal to or greater than 100 mg/dL or on pharmacotherapyb Information obtained from Ref. 13. a A person must meet at least 3 of these criteria to be diagnosed by a physician with MetS. b Defined as taking physician-prescribed medication(s) to treat the health condition. individuals with cardiovascular disease risk factors, it is important to understand the effects and benefits of RT on the various components of MetS. Recent evidence shows that RT performed at least 2 days/wk can reduce the risk and prevalence of MetS and its individual components in U.S. adults (8, 9). Resistance training has a clinically significant effect on MetS risk factors and should be part of the lifestyle management of MetS (24). IMPAIRED FASTING GLUCOSE/ TYPE 2 DIABETES There is evidence that RT can have a positive impact in improving glycemic control (4,5,20). A recent study showed that 10 weeks of resistance exercise was associated with significantly better glycemic control in adults with T2D compared with a treadmill exercise group (4). Additional studies have shown RT to be effective in improving glycemic control in older adults (5) and women (20). Muscle contraction-mediated glucose uptake and both increased intramuscular glucose transport (GLUT4) protein content and increased lean body mass have all been identified as mechanisms for enhanced glycemic control (11,14,20). Resistance exercise has been shown to improve ability to perform activities of daily living (18), and this is important to help increase daily physical activity, thus helping prevent or manage impaired fasting glucose, T2D, and MetS. DYSLIPIDEMIA Improvements in total cholesterol, lowdensity lipoproteins (LDL), and triglycerides have been observed from RT (16,20). The results of studies examining the effects of RT on various blood lipids (e.g., increases in HDL) have reported inconsistent findings, which may be partly because of varying RT programs used in the studies (e.g., different volumes of RT) (12,25). A reduction in abdominal adiposity is a proposed mechanism for these improvements observed in both T2D and dyslipidemia patients after RT (5,11,15,16,20,23). Healthy weight loss and weight maintenance is generally emphasized for persons with dyslipidemia. Although RT has been shown to reduce both resting and ambulatory blood pressure in persons with hypertension (19,21). The effects of RT on resting blood pressure are generally modest (3). A metaanalysis by Kelley and Kelley (17) indicates an approximate 2% reduction in resting systolic blood pressure and an approximate 4% reduction in resting diastolic blood pressure. This analysis looked at RT programs (circuit-training and a more conventional format [multiset, longer rest periods]) lasting at least 4 weeks. However, the majority of outcomes in this meta-analysis and a second one (10) were in subjects with resting blood pressures of ,140/90 mm Hg. More research is needed regarding the effects of RT on blood pressure in persons with hypertension. Recent data indicate that adults performing resistance exercise at least twice weekly may reduce the risk of developing prehypertension (9). Regular RT may have other benefits for persons with prehypertension/hypertension. Activities requiring physical exertion (e.g., physical activities involving lifting or carrying) may be safer to perform, because hemodynamic responses (e.g., increases in blood pressure and heart rate) may be less as a result of increased muscular strength and endurance from regular RT. Resistance exercise has been shown to decrease the blood pressure response to maximal exercise and improve heart rate and blood pressure recovery following cardiorespiratory exercise (26). ABDOMINAL OBESITY Although aerobic activities should be emphasized for weight loss and abdominal fat loss (2), RT has a demonstrated role with this component of MetS. Resistance training, performed Strength and Conditioning Journal | www.nsca-scj.com 65 Special Populations twice weekly, in the absence of a weight loss diet, has been shown to improve insulin sensitivity and fasting glycemia and decrease central adiposity in older men with T2D (15). In addition, a recent meta-analysis showed that RT could have a significant impact on reducing abdominal and total adiposity in individuals with abnormal glucose metabolism (24). Although RT should not be the primary mode of exercise for weight loss and total and abdominal fat loss, RT does expend calories and can result in increases in lean body mass, which can increase resting metabolic rate. In addition, increased muscular strength and endurance will likely enable overweight and obese individuals to be more physically active on a regular basis, thus expending more calories to assist with abdominal and total fat loss and the prevention of weight regain. SUMMARY More research is needed regarding the specific benefits of RT on the individual components of MetS. However, it is clear that RT, particularly when combined with aerobic exercise training, can help prevent and manage MetS. Conflicts of Interest and Source of Funding: The authors report no conflicts of interest and no source of funding. Paul Sorace is a clinical exercise physiologist for The Cardiac Prevention and Rehabilitation Program at Hackensack University Medical Center in Hackensack, NJ. Peter Ronai is a clinical associate professor in the exercise science department at Sacred Heart University in Fairfield, CT. James R. Churilla is an Assistant Professor of clinical exercise physiology and physical activity and the Graduate Program Director for the Exercise Science and Chronic Disease program in the Brooks College of Health at the University of North Florida in Jacksonville, FL. 66 REFERENCES 1. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, and Smith SC Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and international association for the Study of Obesity. Circulation 120: 1640–1645, 2009. 2. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription (8th ed). Baltimore, MD: Lippincott Williams & Wilkins, 2009, pp. 165–172, 232–237, 244–246, 248–256. 3. American College of Sports Medicine. Position stand: Exercise and hypertension. Med Sci Sports Exerc 36: 533–553, 2004. 4. Bweir S, Al-Jarrah M, Almalty AM, Maayah M, Smirnova IV, Novikova L, and Stehno-Bittel L. Resistance exercise training lowers HbA1c more than aerobic training in adults with type 2 diabetes. Diabetol Metab Syndr 1: 27, 2009. 5. Castaneda C, Layne JE, Munoz-Orians L, Gordon PL, Walsmith J, Foldvari M, Roubenoff R, Tucker KL, and Nelson ME. A randomized controlled trial of resistance exercise training to improve glycemic control in older adults with type 2 diabetes. Diabetes Care 25: 2335–2341, 2002. 6. Church TS, Blair SN, Cocreham S, Johannsen N, Johnson W, Kramer K, Mikus CR, Myers V, Nauta M, Rodarte RQ, Sparks L, Thompson A, and Earnest CP. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 304: 2253–2262, 2010. 7. Churilla JR, Fitzhugh EC, and Thompson DL. The metabolic syndrome: how definition impacts prevalence and risk among U.S. adults, NHANES 1999-2004. Metab Syndr Relat Disord 5: 331–341, 2007. 8. Churilla JR, Johnson TM, Magyari PM, and Crouter SE. Descriptive analysis of resistance exercise and metabolic syndrome. Diabetes Metab Syndr 6: 42–47, 2012. 9. Churilla JR, Magyari PM, Ford ES, Fitzhugh EC, and Johnson TM. Muscular strengthening activity patterns and metabolic health risk among US adults. J Diabetes 4: 77–84, 2012. VOLUME 35 | NUMBER 4 | AUGUST 2013 10. Cornelissen VA and Fagard RH. Effect of resistance training on resting blood pressure: A meta-analysis of randomized controlled trials. J Hypertens 23: 251–259, 2005. 11. Flack KD, Davy KP, Hulver M, Winett RA, Frisard ML, and Davy BM. Aging, resistance training, and diabetes prevention. J. Aging Res 2011: 127315, 2010. 12. Fletcher B, Berra K, and Ades P, et al. AHA scientific statement: Managing blood lipids a collaborative approach. Circulation 112: 3184–3209, 2005. 13. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, and Costa F; American Heart Association, National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome. An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Executive summary. Cardiol Rev 13: 322– 327, 2005. 14. Holten MK, Zacho M, Gaster M, Carsten J, Wojtaszewski JFP, and Flemming D. Strength training increases insulinmediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 53: 294–305, 2004. 15. Iban˜ez J, Izquierdo M, Argu¨elles I, Forga L, Larrio´n JL, Garcı´a-Unciti M, Idoate F, and Gorostiaga EM. Twice-weekly progressive resistance training decreases abdominal fat and improves insulin sensitivity in older men with type 2 diabetes. Diabetes Care 28: 662–667, 2005. 16. Iban˜ez J, Izquierdo M, Martinez-Labari C, Ortega F, Grijalba A, ForgaL Idoate F, Garcia-Unciti M, Fernandez-Real JM, and Gorostiaga EM. Resistance training improves cardiovascular risk factors in obese women despite a significant decrease in serum adiponectin levels. Obesity 18: 535–541, 2010. 17. Kelley GA and Kelley KS. Progressive resistance exercise and resting blood pressure: A meta-analysis of randomized controlled trials. Hypertension 35: 838– 843, 2000. 18. Levinger I, Goodman C, Hare D, Jerums G, and Selig S. The effect of resistance training on quality of functional capacity and quality of life in individuals with high and low numbers of metabolic risk factors. Diabetes Care 30: 2205– 2210, 2007. 19. Melo CM, Alencar Filho AC, Tinucci T, Mion D Jr, and Forjaz CL. Postexercise hypotension induced by low-intensity resistance exercise in hypertensive women receiving captopril. Blood Press Monit 11: 183–189, 2006. 20. Misra A, Alappan NK, Vikram NK, Goeli K, Gupta N, Mittal K, Bhatt S, and Luthra K. Effect of supervised progressive resistanceexercise training protocol on insulin sensitivity, glycemia, lipids, and body composition in Asian Indians with type 2 diabetes. Diabetes Care 31: 1282–1287, 2008. 21. Moraes MR, Bacurau RF, Casarini DE, Jara ZP, Ronchi FA, Almeida SS, Higa EM, Pudo MA, Rosa TS, Haro AS, Barros CC, Pesquero JB, Wu¨rtele M, and Araujo RC. Chronic conventional resistance exercise reduces blood pressure in stage 1 hypertensive men. J Strength Cond Res 26:1122–1129, 2012. 22. Pollex RL and Hegele RA. Genetic determinants of the metabolic syndrome. Nat Clin Pract Cardiovasc Med 3: 482– 489, 2006. 23. Stensvold D, Tjonna AE, Skaug EA, Aspenes S, Stolen T, Wisloff U, and Slordahl SA. Strength training versus interval training to modify risk factors of metabolic syndrome. J Appl Physiol 108: 804–810, 2010. 24. Strasser B, Siebert U, and Schobersberger W. Resistance training in the treatment of the metabolic syndrome: A systematic review and meta-analysis of the effect of resistance training on metabolic clustering in patients with abnormal glucose metabolism. Sports Med 40: 397– 415, 2010. 25. Tambalis K, Panagiotakos DB, Kavouras SA, and Sidossis LS. Responses of blood lipids to aerobic, resistance, and combined aerobic with resistance exercise training: A systematic review of current evidence. Angiology 60: 614–632, 2009. 26. Vincent KR, Vincent HK, Braith RW, Bhatnagar V, and Lowenthal DT. Strength training and hemodynamic responses to exercise. Am J Geriatr Cardiol 12: 97–106, 2003. Strength and Conditioning Journal | www.nsca-scj.com 67







© Copyright 2026