
p53 Gene Mutations and Protein Overexpression Are
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
p53 Gene Mutations and Protein Overexpression Are Associated With
Aggressive Variants of Mantle Cell Lymphomas
By Luis Hernandez, Thierry Fest, Maite Cazorla, Julie Teruya-Feldstein, Francesc Bosch, Miguel A. Peinado,
Miguel A. Piris, Emilio Montserrat, Antonio Cardesa, Elaine S.Jaffe, Elias Campo, and Mark Raffeld
Mantle cell lymphoma (MCL) is molecularly characterizedby
bcl-1 rearrangement and cyclin DlIPRAD-1 gene overexpression. Some aggressive variants have been recognized
with a blastic or large cell morphology, higher proliferative
activity, and shorter survival. p53 gene mutations in
lymphoid neoplasms have been detected mainly in high
grade lymphomas and have been associatedwith tumor progression in follicular and small lymphocytic lymphomas. To
determine the role of p53 alterations in MCL, we examined
35 typical and 8 aggressive variants (5 blastic and 3 large
cell) of MCLs by a combination of immunohistochemistry,
single-strand conformational polymorphism analysis of genomic DNA and/or cDNA obtained by reverse transcriptasepolymerase chain reaction, denaturing gradient gel electrophoresis, and sequencing. Of the 8 aggressive MCLs, 3 (38%)
contained missense point mutations in exon 8 codon 278
(Pro -+ Leu), exon 8 codon 273 (Arg His), and exon 5 codon
151 (Pro + Ser), respectively. A diffuse p53 protein overexpression was observed in more than 50% of the tumor cells
in these 3 cases. A fourth blastic MCL also showed strong
p53 immunoreactivity. However, no mutations were de-
tected in exons 5-9 in this case. p53 expression was also
detected in 10% of the cells in an additional large cell type
of MCL and in less than 1% of the cells in 6 typical cases.
No mutations were detected in any of these cases or in the
remaining cases with no expression of the protein. Four nucleotide changes were observed by single-strand conformational polymorphism analysis in 4typical MCLs with no overexpression of the protein. Direct sequencing showed that
these nucleotide changes were located at exon 6 (1case),
intron 7 (2 cases), and intron 8 (1case). The changes in exon
6 and intron 7 were known polymorphisms. The nucleotide
change in intron 8 was outside splicing sites of the neighboring exons. The overall survival of the 3 patients with p53
mutations (median, 18.3 months) was significantly shorter
than that of pateints with the nonmutated MCLs (median,
49 months; P < .01). These findings indicate that p53 gene
mutations are an infrequent phenomenon in MCLs and are
associated with a subset of aggressive variants.
This is a US government work. There are no restrictions on
its use.
M
classic variants with bcl-1 rearrangements and cyclin D1
overexpression.”.” However, the proliferative activity of
MCLs seems to be independent of the levels of cyclin D1
expression. We have recently shown that the mRNA levels
are similar in the classic and aggressive variants of MCLs.”
These findings indicate that other mechanisms may be implicated in the control of cell cycle progression in MCLs.
p53 is a nuclear phosphoprotein that plays an important
role in the regulatory control of the cell cycle. This protein
-+
ANTLE CELL LYMPHOMA (MCL) is a malignant
lymphoproliferative disorder probably derived from
naive pregerminal center B-cells. Several studies have identified the t(l1; 14)(q13;q32) translocation and bcl-1 rearrangement as cytogenetic and molecular abnormalities highly
characteristic of this lymphoma.’4 This translocation activates the cyclin D1 (PRAD-l/BCL-I/CCNDl) gene located
110- to 130-kb downstream from the major breakpoint of
this rearrar~gement.~.’We and others have recently shown
that cyclin D1 overexpression occurs in virtually all MCLs
independently of the detection of t(l1; 14) translocation or
bcl- 1 rearrangements.6.8-’0
In addition, overexpression of this
gene is a highly specific phenomenon of this type of
lymphoma, although it may also occur infrequently in other
lymphoproliferative disorders with 1lq13 translocations.6*8”o
Cyclin D1 is a G1 cyclin that participates in the control
of the cell cycle progression at the G1- to S-phase transition.
Overexpression of this cyclin induces a shortened G 1 phase
and less dependence on growth
Conversely, the
inhibition of cyclin D1 function arrests the cells in Gl.’2-’5
Transfection and transgenic mice experiments have also
shown that cyclin D1 may function as an oncogene cooperating with other oncogenes in cellular transf~rmation.’~.’’
However, the tumorigenic and transforming properties of
cyclin D1 seem to be less effective than those of the conventional oncogenes. The possible additional oncogenic factors
cooperating with cyclin D l in the development and progression of MCLs are unknown.
MCLs may present with a heterogeneous proliferative activity that is considered to be of prognostic significance. In
particular, some aggressive variants have been recognized
with a blastic or large cell morphology, a high proliferative
fraction, and a more aggressive behavior.’8-20Aggressive
variants of MCLs have the same molecular alterations as the
Blood, Vol 87, No 8 (April 15). 1996: pp 3351-3359
From the Departments of Anatomic Pathology and Postgraduate
School of Hematology “Farreras Valent( Hospital Clinic Provincial, University of Barcelona, Barcelona, Spain; the lnstitut Recerca
Oncologica, Barcelona, Spain; the Depament of Anatomic Pathology, Hospital “Virgen de la Salud, ” Toledo, Spain: the Department
of Basic Medical Sciences, School of Medicine, University of Lleida,
Lleida, Spain; and the Hematopathology Section, Laboratory of Pathology, National Cancer Institute, National Institutes of Health,
Bethesda. MD.
Submitted July 27, 1995; accepted November 24, 1995.
Supported in part by Grant No. SAF I I95/93 from CICU, Ministerio de Educacidn y Ciencia (E.C.), and CIRIT (Generalitat de
Catalunya, Spain). L.H. was a fellow supported by a grant from the
European Union, and M.C. was a fellow from the Spanish Ministerio
de Educacidn y Ciencia. T.F. was a fellow supported by the Asociation pour la Recherche contre le Cancer (ACR: Paris, France}. The
j r s t and second authors contributed equally to this study.
Address reprint requests to Elias Campo, MD, Laboratory of
Anatomic Pathology, Hospital Clinic Provincial, Villarroel 170,
08036-Barcelona, Spain.
The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with 18 U.S.C. section 1734 solely to
indicate this fact.
This is a US govemment work There are rw resrricrions on its use.
0006-4971/96/8708-04$0.00/0
3351
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
3352
HERNANDEZ ET AL
participates in a GI arrest checkpoint that would allow the
cell to repair DNA damage before progression in the cell
Somatic allelic deletions and point mutations of
this gene are considered to be the most frequent genetic
alterations in human neoplasm^.'^ p53 mutations have been
associated with progression to more aggressive forms of the
disease in several hematologic malignancies. Particularly,
in non-Hodgkin's lymphoid neoplasms, p53 gene mutations
have been mainly detected in high grade lymphoma^.^^.^' In
addition, they are associated with the histological and clinical
progression of f o l l i c ~ l d and
~ ~ 'small
~
lymphocytic lymphomaS,24.2h.27
The aim of this study was to determine the role of p53
alterations in MCL and their possible involvement in the
pathogenesis of the more aggressive variants. For this purpose, we have examined a series of classic and aggressive
MCLs by a combination of immunohistochemistry, singlestrand conformational polymorphism (SSCP) analysis of genomic DNA and cDNA obtained by reverse transcriptasepolymerase chain reaction (RT-PCR), denaturing gradient
gel electrophoresis (DGGE), and sequencing. The findings
indicate that p53 mutations and protein expression are rare
in typical MCLs but may be involved in the pathogenesis
of a subset of aggressive variants of this lymphoma.
MATERIALS AND METHODS
Case selection. Tumor specimens from 43 MCLs were included
in the study. A total of 25 cases were obtained from the Anatomic
Pathology Department of the Hospital Clinic Provincial (HCP; University of Barcelona, Barcelona, Spain), and 18 were obtained from
the Laboratory of Pathology, National Cancer Institute (NCI; National Institutes of Health, Bethesda, MD). A total of 35 cases were
classified as typical MCLs (20 from HCP, 15 from NCI),3'.'2 and 8
cases were classified as aggressive variants of MCLs ( 5 from HCP,
3 from NCI). These aggressive variants included 5 blastic MCLs
and 3 large cell ("anaplastic") type of MCLs defined according to
criteria previously
All the cases were reviewed and
classified by two pathologists (E.C. and E.S.J.) together. Immunophenotype was analyzed in all cases using immunohistochemistry
on frozen tissue sections andor cell suspensions by flow cytometry.
These studies included Ig light and heavy chains, several of the Bcell (CD19, CD20, CD22, CD45RA) and T-cell (CD2, CD3, CD5,
CD7, CD4, CD8, CD45R0, CD43) markers, and CDlO and CD23.
Cyclin D1 expression was examined in 25 cases, including 5 aggressive variants, by Northern blot analysis, and it was overexpressed
in all of them."' All patients had advanced stage disease (111 or IV)
and were treated with systemic chemotherapy according to protocols
at the respective institutions. Actuarial survival analysis was performed according to the method described by Kaplan & Meier, and
the curves were compared by the log-rank test.
RNA and DNA extraction. Total RNA was isolated from frozen
tissues in the 25 cases from HCP by guanidine isothiocyanate extraction and cesium chloride gradient centrifugation." High molecular
weight DNA was extracted from the 18 cases from NCI and from
additional frozen material available in 19 cases from HCP, using
Proteinase WRNAse treatment and phenol-chloroform extraction.
DNA and RNA were also extracted from the following cell lines
and used as positive controls for p53 mutations during the SSCP,
DGGE, and sequencing analysis: MDA-MB-468 breast carcinoma
cell line (mutated at codon 273), obtained from the American Tissue
Culture Collection (Rockville, MD); the KM12SM colorectal cancer
cell line (mutated at codon 179), kindly provided by Dr I.J. Fidler
Table 1. Primer Sets Used for the RT-PCR, PCR, SSCP Analysis, and
Sequencing Analysis of p53 Gene
10D
1UR
10DN
126U
331DB2
1297911
14875D
13463D
13966U
22511
5DN
5'
5'
5'
5'
5'
5'
5'
5'
5'
5'
5'
TGTCAGTCTGAGTCGGGCCTCTG 3'
AGACTGCCTTCCGGGTCACT 3'
ATGGCGGGAGGTAGACTGAC 3'
TACTCCCCTGCCCTCAACAAG 3'
ACAGATCTGAAGGGTGAAATATTCTCC 3'
GCTGCCGTGTTCCAGTTGCT 3'
AGGCATCACTGCCCCCTGAT 3'
CTCCTCCCAGAGACCCCAGT 3'
CTGGCCTCATCTTGGGCCTG 3'
TTGGCTCTGACTGTACCACCA 3'
CATAGGGCACCACCACACTA 3'
(M.D. Anderson Cancer Center, Houston, TX); and the T-cell line
CEM (mutated at codons 175 and 248), obtained from American
Tissue Culture Collection.
RT-PCR ofp.53 gene. p53 cDNA was obtained in 25 cases using
RT and the antisense primer 10D (Table 1) located at the 5' end of
the 11th exon. The RT reaction was performed with I .5 p g of total
RNA, 200 U of Moloney murine leukemia virus RT (GIBCO-BRL.
Gaithesburg, MD), 0.5 pmollL of primer, 0.5 mmol/L of each deoxynucleotide triphosphate (dNTP), 20 U of RNAsin, I O mmoliL dithiothreitol, and RT buffer (50 mmolfl, Tris HCl, pH 8.3: 75 mmol/L
KCI; 3 mmol/L MgCIJ in a final volume of 20 pL. The reaction
was incubated for 1 hour at 37°C and for 5 minutes at 95°C
Ampl@ution of the p53 gene. For the RNA samples, a nested
PCR was used to amplify a fragment of p53 gene including exons
5 through 9. The primers used in PCR procedures are described in
Table 1. The first PCR reaction was performed by mixing 5 p L of
the RT reaction product with I U of Taq polymerase (GIBCO-BRL),
0.4 m m o l n each primer (1UR and lODN), and PCR buffer ( I O
mmoliL Tris-HCI, pH 7.8; SO mmol/L KCI; 1.5 mmollL MgCI,; and
0.018 gelatin) in a final volume of 25 mL. The reaction was performed for 15 cycles in a thermal cycler (Perkin-Elmer Cetus, Norwalk, CT) at 94°C for 1 minute, at 53°C for 45 seconds, and at 72°C
for 1 minute. The second PCR was performed with 0.5 pL of the
first reaction in the same conditions but with 120 mmol/L dNTPs
and 2 mmol/L of each primer ( 1 26U and 33 I DB2), at an annealing
temperature of 5 5 T , and for 35 cycles.
For the DNA samples, 0.5 pg of DNA was added to I U of Tdq,
2 mmoVL each primer (1 2979U and 14875D), I20 mmol/L dNTPs,
and PCR buffer in a final volume of 25 pL. The reaction was
performed for 25 cycles at 94°C for 45 seconds, at 63°C for 35
seconds, and at 72°C for I minute and 15 seconds. Two nested PCRs
were performed on I pL of 1/1,000 dilution of the first PCR product.
with two pairs of primers (126U/13463D for exons 5 to 6, and
13966U/331DB2 for exons 7 to 9). The reactions were performed
for 3.5 cycles at 94°C for 45 seconds, at 63°C for 35 seconds, and
at 72°C for 1 minute.
SSCP anu1ysi.r. SSCP analysis was used to screen for p53 mutations according to a modified protocol of a previously described
Nested PCRs were performed as described above in the
presence of 2 pCi "P deoxycytidine triphosphate per PCR. For the
37 genomic DNA samples and for the 25 cDNA samples, 5 p L and
9 pL. respectively, of the radioactive PCR product were digested
with Hpa 11. Samples were diluted 20-fold in formamide-dye loading
buffer,36incubated for 3 minutes at 95°C. and immediately cooled
on ice; 2 pL were loaded on a 6% polyacrylamide nondenaturing
gel with or without 10% glycerol. Electrophoresis was performed at
room temperature at 30 W for 12 minutes followed by 6 W for 14
hours for IO% glycerol gels and at 30 W for 12 minutes followed
by 6 W for 6 hours for the gels without glycerol. The gels were
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
~ 5 IN
3 MANTLE CELL LYMPHOMAS
3353
Table 2. Primer Sets Used for the PCR Reaction and Conditions for DGGE for p53 Mutations
p53 Exon
Primers
Fragment Size
DGGE Conditions*
5
Forward 5'(GC)lTCCTClTCCTGCAGTACTC-3't
Reverse S'-CTGGGCAACCAGCCCTGTCGT-3'
Forward 5'(GC)ACGACAGGGCTGGlTGCCCA-3'
Reverse 5'-AGlTGCAAACCAGACCTCAG-3'
Forward 5'(GC)TCTCCTAGGlTGGCTCGACTG-3'
Reverse 5'-GCAAGTGGCTCCTGACCTGGA-3'
Forward S'CCTATCCTGAGTAGTGGTAATC-3'
Reverse 5'-(GC)AAGTGAATCTGAGGCATAAC-3'
Forward 5'CCTATCCTGAGTAGTGGTAATC-3'
Reverse 5'-(GC)GTCCCAAGAClTAGTACCTGAAG-3'
Forward 5'CACCllTCClTGCCTCllTCCTAG-3'
Reverse 5'-(GC)GTCCCAAGAClTAGTACCTGAAG-3'
282
50%-65% for 5 h
227
35%-60% for 8 h
174
35%-65% for 7 h
260
35%-65% for 8 h
375
35%-65% for 7 h
156
35%-65% for 8 h
6
7
8
8&9
9
*The percentage of denaturant range and electrophoresis run time at 150 V and 60°C.
t (GC) is 5'-CGCCCGCCGCGCCCCGCGCCCGGCCCGCCGCCCCCGCCCG9'.
dried under vacuum at 85°C and exposed to an x-ray film at room
temperature for 3 days.
DGGE analysis. DGGE analysis was performed in the 37 cases
in which genomic DNA was available. Primers flanking p53 exons
5-9 were the same as those described by Beck et
except for the
exon 8 and 9 primers, and are listed in Table 2. One primer of each
pair was synthesized with an added 40-bp GC-rich sequence (GC
clamp) at the 5' end. This results in a high temperature melting
domain at one end of each PCR product and renders the remainder
of the exon sequence accessible to analysis by DGGE." PCRs were
performed using a previously reported protocol with minor modification~.~'
Briefly, 200 ng of genomic DNA was mixed with 40 pmol
of each primer and 75 nmol of each dNTP in 50 pL of PCR buffer
(10 "OK Tris HCI, pH 8.3; 50 "OK KCI; 1.5 "OK MgC12;
0.01% gelatin). A total of 1.5 U of Taq was added to each sample,
and PCR was performed at 94°C for 1 minute and 15 seconds, at
58°C for 1 minute and 15 seconds, and at 72°C for 35 seconds plus
a I-second extension per cycle for 40 cycles.
The PCR products were analyzed using a D-gene gel electrophoresis apparatus (Bio-Rad Laboratories, Hercules, CA). Gels were cast
using the Model 475 Gradient delivery System (Bio-Rad). Electrophoresis of 40 pL of the PCR product was performed at 150 V at
60°C in 7.5% polyacrylamide gel under the appropriate predetermined denaturing conditions. Except for the gradient conditions for
exon 5 (see Table 2), all other p53 exons were analyzed under the
same gradient conditions described by Beck et al?'
Sequencing of the SSCP+ and DGGE+ fragments. To confirm
the possible p53 mutations the samples of DNA with altered migration by SSCP or DGGE were sequenced. Sequences were performed
using a commercial cycle sequencing kit (Perkin-Elmer Cetus) and
33P deoxyadenosine triphosphate. A total of 0.5 pL of the nested
PCR product was used as template for sequencing. Several internal
primers (126U, 331DB2, 13463D, 13966U, 225U, and 5DN) were
used for the sequencing reaction at a final concentration of 14 nmol/
L. The reaction was performed according to the instructions of the
manufacturer. The reaction was performed for 30 cycles at 94°C for
45 seconds, at 60°C for 30 seconds, and at 72°C for 1 minute and
30 seconds. The final product was diluted twofold in formamidedye loading buffer. Samples were denatured for 3 minutes at 95"C,
and 2 pL was analyzed in a denaturing 6% polyacrylamidel8 mol/
L urea sequencing gel for 2 or 3 hours at 55 W. The gels were
dried under vacuum at 85°C and exposed to an x-ray film at room
temperature for 3 days without an intensifier screen. The presence
of a mutation was confirmed by sequencing both the genomic DNA
and cDNA of each mutated case, when available, and by sequencing
the other DNA strand.
Immunohistochemical analysis. p53 protein expression was immunohistochemically assessed in all cases on formalin-fixed-paraffin-embedded material using the DO-7 (Dako Corp, Carpinteria,
CA). In addition, the 25 cases from the HCP were assessed on frozen
sections using the anti-p53 monoclonal antibodies (MoAbs) Pab
1801 and Pab 240 (Oncogene Science, Cambridge, MA). The results
with the paraffin-embedded material and with the frozen sections in
these cases were concordant. Before the application of the primary
antibodies on the fixed and paraffin-embedded sections, an antigen
retrieval technique was performed. The deparaffinized and rehydrated slides were placed in 10 mmol/L citrate buffer (pH 6) and
were heated in the microwave oven for 15 minutes at 700 W. The
frozen sections were air-dried, fixed in cold (4°C) acetone for 10
minutes, hydrated, and incubated with the MoAbs. The MoAbs were
incubated overnight at 4°C. The immunoreaction was detected by
means of the streptavidin-biotin-alkaline phosphatase (Biogenex,
San Ramon, CA) technique using Fast-Red as chromogen and levamisole to inhibit endogenous alkaline phosphatase or, alternatively,
using the avidin-biotin-peroxidase complex technique (Vectastain
ABC kit; Vector Laboratories, Burlinghame, CA) and 3-3' diaminobenzidine tetrahydrochloride (Sigma Chemical Co, St Louis, MO)
dissolved in 10 mL of Tris buffer 0.05 mom, pH 7.6, and 0.03%
of HzOzas developer. The slides were counterstained with hematoxylin. The cases were evaluated as negative when no positive cells
were observed, and p53 was scored as 1+ (weak), 2+ (moderate),
and 3+ (strong), when less than 1%, less than 20%, or greater than
20% of the tumor cells, respectively, showed nuclear immunoreactivity.
RESULTS
SSCP and DGGE analysis. A series of 35 typical and 8
aggressive variants of MCLs were analyzed for the presence
of p53 mutations using SSCP of genomic DNA and/or cDNA
samples and DGGE of genomic DNA. The results are summarized in Tables 3 and 4 and in Figs 1, 2, and 3. Only 4
of the 35 typical MCLs and 3 of the 8 aggressive cases
showed altered electrophoretic mobility. Two of these aggressive variants (cases no. 10 and 31) had a blastic morphology (Fig 4), and the third case (case no. 15) was a large cell
MCL variant (Fig 5). In cases no. 10 and 15, the anomalous
mobility was found within the fragments encompassing exon
8 using all three techniques,ie, SSCP and DGGE of genomic
DNA and SSCP of cDNA. In case no. 31, an abnormally
migrating band was identified in exon 5 by SSCP and DGGE
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
3354
HERNANDEZ ET AL
Table 3. Frequency of p53 Gene Alteration and Protein
Overexpression in MCLs
__
~
Diagnosis
(MCL variant)
No of
Cases
Typical
Aggressive*
35
8
0
4 (50)
3 (38)
Ot
3 (38)
Total
43
4 (9)
7 (16)
3 (7)
IHC
I%)*
Mutation
SSCP/DGGE
1%)
(70)
4 (11)
Abbreviation: IHC, immunohistochemistry.
* O n l y cases with strong p53 immunostaining (>20% of cells
stained) were scored positive.
t One case with anomalous mobility in the SSCP analysis was the
known polymorphism in codon 213. Two cases had a known polymorphism in intron 7, and one case showed a nucleotide change in intron
8 away from splicing sites.
Histologically aggressive variants defined as blastic (5 cases) or
large-cell ("anaplastic"; 3 cases).
*
of genomic DNA. SSCP analysis of cDNA was not performed in this case because of the unavailability of RNA.
Of the 4 abnormalities found in typical MCLs, 3 occurred
only in the SSCP analysis of genomic DNA (cases no. 2, 9,
and 38). The anomalous mobility was observed in the fragment containing exons 7-9. This genomic SSCP fragment
also contains introns 7 and 8; whereas the other methods
used, ie, DGGE and SSCP of cDNA, do not include intronic
sequences, suggesting that the abnormalities present were
caused by changes in introns 7 or 8. One typical MCL (case
no. 4) showed an anomalous band in the exon 6 fragment
using all three techniques in a pattern suggestive of the
known polymorphism at codon 213.
DNA sequencing. All the fragments with anomalous
SSCP and DGGE were subsequently sequenced. The results
are summarized in Table 4 and in Figs 2 and 3. The 3 high
grade MCLs showed a missense mutation in exon 8 codon
278 (Pro
Leu; case no. lo), exon 8 codon 273 (Arg +
His; case no. 15), and exon 5 codon 151 (Pro Ser; case
no. 31), respectively. In cases no. 10 and 15, the mutation
was confirmed in both genomic DNA and cDNA.
The altered mobility detected in exon 6 in 1 typical MCL
(case no. 4) by SSCP and DGGE was shown to be the result
of the known polymorphism at codon 213, with the neutral
change CGA (Arg) CGG (Arg). This nucleotide change
was confirmed in both genomic DNA and cDNA. The anom+
-+
-+
alous SSCP detected at the genomic level in 2 typical MCLs
(cases no. 2 and 38) were caused by a known polymorphism
in intron 7 characterized by C + T and T G changes at
71-bp and 91-bp downstream of exon 7, respectively.''' The
fourth typical MCL (case no. 9) with an altered mobility
detected at genomic level was a nucleotide change in intron
8 (G A), 32-bp downstream of exon 8 (Table 4 and Fig
2). This nucleotide change was outside splicing sites of the
neighboring exons. No DNA from normal tissues of this
case was available to rule out the possibility that this change
was an intronic polymorphism.
Immunohistochemical analysis of'p53 protein. Expression of p53 protein was examined in the 43 cases by immunohistochemistry. The 3 aggressive cases with a missense
p53 mutation showed strong nuclear immunostaining in a
high proportion of the tumor cells (>SO%; see Figs 4 and
5 ) . The positive cells were diffusely distributed throughout
the tumor. In 1 of these cases, a paraffin block of a previous
biopsy performed 2 years before was also available. This
sample was obtained at the time of presentation of the tumor
and was interpreted as a large-cell type of MCL with a
nodular growth pattern. Comparing both samples, the second
specimen showed a progression to a more aggressive morphology with a diffuse growth pattern and larger and more
irregular cells that contained nuclei with blastic chromatin
and occasional nucleoli. The mitotic index in the first biopsy
specimen was lower (2 mitoses X high power field [HPF])
than that in the second specimen (6.5 mitoses X HPF). The
patient died 2 months after the second biopsy was performed.
In spite of the morphological progression between the first
and second biopsy specimens, the p53 expression was similar
in both samples, with a strong immunoreactivity in more
than 70% of the tumor cells.
In addition to the 3 mutated cases described above, 1
blastic MCL (case no. 29) showed strong (3+) p53 overexpression, with nuclear immunoreactivity in more than 50%
of cells. However, no gene mutations were detected in exons
5-9 in this case. An additional large-cell type of MCL (case
no. 42) showed p53 immunostaining in 10%of the cells. No
gene alterations were detected in this case.
None of the remaining nonmutated cases showed overexpression of the protein, including the case with the codon213 polymorphism and the 3 cases with nucleotide changes
in intronic regions. In 6 typical MCLs with no DNA alter+
+
Table 4. p53 Gene Alterations and Protein Expression in Typical and Blastic MCLs
DNA'
Case
No.
10
15
31
4
2
9
38
MCL Variant
IHC
RNNcDNA SSCP
SSCP
DGGE
Mutation
Blastic
Large cell
Blastic
Typical
Typical
Typical
Typical
+
+
+
+
+
+
+
+
+
+
+
t
Codon 278 CCT CTT
Codon 273 CGT CAT
Codon 151 CCC TCC
Codon 213 CGA 4 CGG
Intron 7
Intron 8
Intron 7
-
+
-
-
-
-
-
+
+
+
+
-
-
AA
+
+
+
~
Abbreviations: IHC, immunohistochemistry; AA, amino acid.
* SSCP analysis of the genomic DNA included exonic and intronic regions, whereas DGGE examined only exonic areas.
Pro + Leu
Arg His
Pro Ser
Arg Arg
+
+
+
-
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
3355
~ 5 IN
3 MANTLE CELL LYMPHOMAS
c
Fig 1. SSCP analysis of p53
cDNA (A, B, and C) and genomic
DNA (D) in MCLs. cDNA fragments corresponding t o exons 56 (A) and exons 7-8 (B and CI of
p53 gene run in a nondenaturing
6% acrylamide gel containing
10% (A and B)or no (C) glycerol.
Genomic DNA fragment corresponding t o exon 5 (DI of p53
gene run in a nondenaturing 6%
acrylamide gel with no glycerol.
Lane numbers indicate the different MCLs. Lane C1 in (A) contains cDNA from the positive
control cell line KMl2SM mutated at codon 179. Three aggressive MCLs (cases no. 10, 15,
and 31) showed an abnormal migration in exon 8 (B and C) and
exon 5 (D), respectively. Case no.
4 was a typical MCL, with a polymorphism in exon 6 codon 213
(A).
1
1
2
3
~
15
.
16
.
4
17
29
18
30
31
32
I
'.
EXONS
T
A
T
C
--
C
w
'1
WILD
CODON 278
8 9 10 I 1 12 13 14
**.'.
--w IO w IO w IO w IO
A
6 7
~~
EXONS
G
4 5
CASE lo
G
IS
w
IS
w
IS
w
IS
WILD
CODON 273
ARG
c\
GT'
PRO
INTRON7
G
A
T
C
w 2 w 2 w 2 W 2
INTRONS
C
T
A
G
9 w 9 w 9 w 9
w
CASE 9
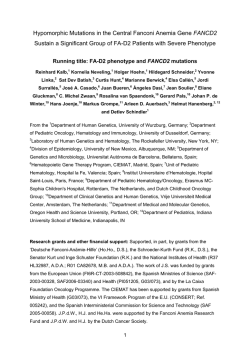
Fig 2. Sequence analysis of
SSCP' cases. The p53 gene regions amplified by PCR were sequenced by a direct cycle reaction. (A), (6). (CI, and (D) show
the sequences of cases no. 10,
15, 2, and 9, respectively. Cases
no. 10 and 15 were mutated in
codon 278 and 273. whereas
cases no. 2 and 9 showed a nucleotide change in intron 7 and 8
in distant regions of the splicing
sites.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
HERNANDEZ ET AL
3356
A
i
2
3
4
A
Codon151
Fig 3. DGGE and sequence analysis of case no. 31. (A) 200 ng of genomic DNA was amplified with the exon 5 primers and was analyzed
by DGGE. Lane 1 is a normal placental control showing the normal homoduplexpattern. Lane 2 is case no. 31 showing an abnormal homoduplex.
Lane 3 is an equal mixture of control DNA with case no. 31 DNA. The resulting complex band pattern is caused by the formation of normal
and mutant heteroduplex species, in addition to the two homoduplex species, allowing a clearer evaluation of the abnormality present. Lane
4 is a positive control cell line ICEM). Bands labeled "1" represent abnormal homoduplexes; bands labeled "2" reDresent heterodudexes.
(B) Sequence analysis of case no. 31 showing a C T transition in codon 151 that results in the substitution of serine for the normal proline
(CCC TCCI.
-
-
ations, isolated positively stained cells (<1%) were also
observed.
p53 Alterations and survival qf the patients. The median
overall survival of this series of MCL patients was 42 months
(range, 2 to 132 months). Patients with aggressive variants
of MCLs had an overall survival (median, 18.3 months; n
= 8) significantly shorter than that of patients with typical
mantle cell lymphomas (median, 49.8 months; n = 30; P <
.02). No follow-up was available in 5 patients with typical
MCL. The survival of the 3 patients with p53 mutations
(median, 18.3 months) was significantly shorter than that of
the pateints with nonmutated MCLs (median, 49 months;
95% confidence interval, 24 to 69 months; P < .01; see (Fig
6). However, the survival of 5 aggressive MCLs with no
detectable p53 mutations was similar to the survival of the
mutated aggressive cases (median, 14 and 18.3 months, respectively). The blastic MCL with strong p53 immunostain-
Fig 4. Histological section of a blastic MCL (case no. 31) with
p53 mutation (hematoxylin and eosin [H&El; original magnification
x 630).
ing in which no mutations were detected also had a short
survival of 18 months.
DISCUSSION
In this study we have examined 35 typical and 8 aggressive variants of MCLs for the presence of p53 mutations
and protein expression. Only 3 of 43 (7%) MCLs showed
p53 gene mutations and strong overexpression of the protein.
However, all 3 were in the histologically aggressive subgroups, further classified as either blastic or large-cell variants of MCL. None of the typical MCLs with low proliferative fraction and more indolent behavior showed p53
mutations. Protein expression in these cases was negative or
negligible. These findings indicate that p53 gene mutations
in MCLs are a relatively infrequent phenomenon (7% of all
the MCLs examined). However, the presence of mutations
in 3 of the 8 histologically aggressive cases (38%) with
shortened survival indicates that p53 may be involved in the
pathogenesis of a subset of aggressive MCLs.
One of the two mutations found was a G + A transition
in codon 273. This is a known hot-spot codon with a CpG
dinucleotide. Most of the mutations occurring in this codon,
including the one detected in our study, lead to a loss of
the biological functions of p53 pr~tein.~"
p53 mutations in
leukemiadlymphomas, as in other tumors, occur frequently
at CpG sites that are considered to be particularly susceptible
to spontaneous mutations.24The other two mutations were
C 4 T transitions in codon 278 and 151. Mutations in these
codons are rare in lymphomas but have been detected in
several lymphomas and hematologic d i s ~ r d e r s . ~Three
~~~~~~"~~'
other nucleotide changes were detected in intronic regions
of the gene. Two of them were a known polym~rphism,~~
and, in the third case, the change was distant from splicing
sites.
The immunohistochemical detection of p53 protein in a
high number of cells (>50%) was relatively concordant with
the presence of gene mutations in this series of MCLs because strong p53 immunostaining was observed in the 3
cases with p53 gene mutations, whereas all typical MCLs
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
~ 5 3
IN MANTLE CELL LYMPHOMAS
3357
Fig 5. Histologicalsection and p53 immunohistochemicalstaining
of case no. 15. (A) Biopsy specimen obtained at the time of diagnosis
shows a large-cell (anaplastic) MCL. (H&E; original magnification x
630). (B) Histological section of the biopsy specimen obtained 2 years
later in the same patient. The cells are larger with irregular nuclei,
disperse chromatin, and occasional nucleoli (H&E; original magnification x 6301. (C) p53 immunostaining shows nuclear positivity in
more than 50% of the cells. Sequencing analysis showed a p53 gene
mutation in codon 273 (p53 immunostaining;original magnification
x 400).
were negative or weakly positive. However, no mutations
were detected in exons 5-9 in 2 blastic MCLs with strong
(case no. 29) and moderate (case no. 42) pS3 overexpression,
respectively. Immunohistochemical detection of pS3 protein
in human tumors has been considered to be a consequence
of the gene mutation and protein stabilization with a longer
half-life. However, several studies have now shown that in
some high grade non-Hodgkin's lymphomas (NHLs), p53
overexpression is not always associated with detectable gene
mutations.'X.J'.." Although we can not completely rule out
the existence of mutations in our 2 blastic MCLs overexpressing the protein. mutations in regions outside of exons
5 to 9 in NHL seem to be rare." The increased expression
of the protein in these cases may be caused by nondetected
mutations or by the stabilization of the protein by other
mechanisms, or, alternatively, it may be related to the high
proliferative activity of tumor cells. Overexpression of wildtype p53 has been observed in highly proliferating cells and
reactive tissues in which it may represent a normal expression related to its function in the control of cell proliferation.?x.41.15
The presence of pS3 mutations in aggressive MCLs is
consistent with the observations in other hematopoietic disorders and NHLs in which pS3 mutations mainly occur in
high grade tumors and in association with progression of the
disease. In particular, pS3 alterations are rarely found in low
grade lymphomas and indolent chronic lymphocytic leukemias. However, mutations are detected in high grade
lymphomas evolving from B-cell chronic lymphocytic leukemia (Richter's syndrome) and in transformed follicular
lymphomas, suggesting that pS3 mutations may be implicated in the histological progression of these tumors.25.~s.'0ac'
Similar to those in follicular lymphomas, pS3 mutations were
only present in less than half of the blastic and large-cell
types of MCLs, indicating that other mechanisms may also
be implicated in the pathogenesis of these aggressive variants.
MCLs are considered indolent lymphomas with frequent
relapses and an intermediate overall survival (median, 3 to
5 years) between low and high grade NHL." Histological
progression from typical MCLs to more aggressive variants
may occur in tumor relapses. with an increase in the mitotic
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
3358
HERNANDEZ ET AL
PROBABILITY
REFERENCES
pso.01
NON-MUTATED
......
1
index, nuclear size, and chromatin dispersal.47 However,
most aggressive variants of MCL are recognized at diagnosis, indicating that they may arise de novo as primary aggressive MCLs." In our series, the 8 aggressive cases were diagnosed at presentation. In 1 of these cases, a further
morphological progression was observed at relapse after an
interval of 24 months. In this tumor, the p53 mutation was
found in the second biopsy specimen. Although no molecular
studies could be performed in the first biopsy specimen of
this patient, the strong overexpression of the protein with an
intensity similar to that of the second sample suggests that
p53 was already mutated at presentation. Similarly, the p53
mutations observed in the other 2 blastic MCLs were also
detected during biopsies performed at diagnosis. These findings suggest that p53 mutations in MCLs may occur in an
early stage of the development of these aggressive variants
of the tumors. This model seems to be different from that
observed in follicular lymphomas, in which p53 mutations
appear during the evolution of the tumor and are closely
associated with its histological transformation to a high grade
lymphoma.29
The mechanisms by which p53 mutations may lead to the
higher proliferative activity and more aggressive behavior
of this subset of MCLs are not clear. Wild-type p53 participates in the control of cell cycle progression, particularly in
a G1 checkpoint that allows the cell to repair DNA damage
before progression in the cell cycle.2',22Inactivation of p53
may favor the accumulation of other genetic lesions that
would confer to the cells a selective growth advantage.
In conclusion, our findings indicate that p53 gene alterations are an infrequent phenomenon in MCLs, but that they
are associated with a subset of aggressive variants and short
survival. Further studies are needed to clarify other possible
molecular mechanisms implicated in the pathogenesis of the
aggressive MCLs in which no p53 mutations are detected.
ACKNOWLEDGMENT
The authors thank Irazema Nayach and Nerea Peird for excellent
technical assistance.
1. Weisenburger DD, Sanger WG, Armitage JO, Purtilo DT: Intermediate lymphocytic lymphoma: Immunophenotypic and cytogenetic findings. Blood 69:1617, 1987
2. Vandenberghe E, de Wolf-Peters C, van den Oord J, Wlodarska
I, Delabie J, Stul M, Thomas J, Michaux JL, Mecucci C, Cassiman
JJ, van den Berghe H: Translocation (1 1; 14): A cytogenetic anomaly
associated with B-cell lymphomas of non-follicle centre cell lineage.
J Pathol 163:13, 1991
3. Williams ME, Westermann CD, Swerdlow SH: Genotypic
characterization of centrocytic lymphoma: Frequent rearrangement
of the chromosome 11 bcl-1 locus. Blood 76:1387, 1990
4. Medeiros LJ, Van Krieken JH, Jaffe ES, Raffeld M: Association of bcl-1 rearrangements with lymphocytic lymphoma of intermediate differentiation. Blood 76:2086, 1990
5. Withers DA, Harvey RC, Faust JB, Malynk 0, Carey K,
Meeker TC: Characterization of a candidate bcl-1 gene. Mol Cell
Biol 11:4846, 1991
6. Rosenberg CL, Wong E, Petty EM, Balf AE, Tsujimoto Y,
Harris NL, Arnold A: PRADl, a candidate BCLI oncogene: Mapping and expression in centrocytic lymphoma. Proc Natl Acad Sci
USA 88:9638, 1991
7. Motokura T, Bloom T, Kim HG, Juppner H, Ruderman JV,
Kronenberg HM, Arnold A: A novel cyclin encoded by BCLI -linked
candidate oncogene. Nature 350:512, 1991
8. Rimokh R, Berger F, Delsol G, Charrin C, Bertheas MF,
French M, Garoscio 0, Felman P, Coiffier B, Bryon PA, Rochet
M, Genthilhomme 0, Germain D, Magaud JP: Rearrangement and
overexpression of the BCL-IPRAD- 1 gene in intermediate lymphocytic lymphomas and in t(l lql3)-bearing leukemias. Blood 81:3063,
1993
9. Oka K, Ohno T, Kita K, Yamaguchi M, Takakura N, Nishi K,
Miwa H, Shirakawa S: PRAD-1 gene overexpression in mantle cell
lymphoma but in not in other low grade B-cell lymphomas, including
extranodal lymphoma. Br J Haematol 86:786, 1994
IO. Bosch F, Jares P, Campo E, Lopez-Guillermo A, Pins MA,
Villamor N, Tassies D, Jaffe ES, Montserrat E, Rozman C, Cardesa
A: PRAD-lkyclin DI gene overexpression in chronic lymphoproliferative disorders: A highly specific marker of mantle cell
lymphoma. Blood 84:2726, 1994
1 1. Jiang W, Zhang Y-J, Kahn SM, Hollstein MC, Santella RM,
Lu S-H, Hams CC, Montesano R, Weinstein IB: Altered expression
of the cyclin D1 and retinoblastoma genes in human esophageal
cancer. Roc Natl Acad Sci USA 90:9026, 1993
12. Quelle DE, Ashmun RA, Shurtleff SA, Kat0 J, Bar-Sagi D,
Roussel M, Sherr CJ: Overexpression of mouse D-type cyclins accelerates GI phase in rodent fibroblasts. Genes Dev 7:1559, 1993
13. Baldin V, Lukas J, Marcote MJ, Pagano M, Draetta G: Cyclin
D1 is a nuclear protein required for cell cycle progression in G1.
Genes Dev 7:812, 1993
14. Bartkova J, Lukas J, Muller H, Lutzhoft D, Strauss M, Bartek
J: Cyclin D1 protein expression and function in human breast cancer.
Int J Cancer 57:353, 1994
15. Tam SW, Theodoras AM, Shay JW, Draetta GF, Pagano M:
Differential expression and regulation of cyclin D1 protein in normal
and tumor human cells: Association with cdk4 is required for cyclin
D1 function in G1 progression. Oncogene 9:2663, 1994
16. Hinds PH, Dowdy S, Eaton EN, Arnold A, Weinberg RA:
Function of a human cyclin gene as an oncogene. Proc Natl Acad
Sci USA 91:709, 1994
17. Lovec H, Grzeschiczek A, Kowalski M-B, Moroy T: Cyclin
Dlhcl-1 cooperates with myc genes in the generation of B-cell
lymphomas in transgenic mice. EMBO J 13:3487, 1994
18. Lardelli P, Bookman MA, Sundeen J, Longo DL, Jaffe ES:
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
~ 5 3
IN MANTLE CELL LYMPHOMAS
Lymphocytic lymphoma of intermediate differentiation: Morphologic and Immunophenotypic spectrum and clinical correlations. Am
J Surg Path01 14:752, 1990
19. Lennert K, Feller AC: Histopathology of Non-Hodgkin’s
Lymphomas. New York, NY, Springer-Verlag, 1992
20. Ott MM, Ott G, Porowski P, Gunzer U, Feller AC, MullerHermelink HK: The anaplastic variant of centrocytic lymphoma is
marked by frequent rearrangements of the bcl- 1 gene and high proliferation indices. Histopathology 24:329, 1994
21. Lane D P p53, guardian of the genome. Nature 358:15, 1992
22. Kastan MB, Zhan Q, El-Deiry WS, Carrier F, Jacks T, Walsh
WV, Plunkett BS, Vogelstein B, Fomace AJ Jr: A mammalian cell
cycle checkpoint pathway utilizing p53 and GADD45 is defective
in ataxia-telangiectasia. Cell 71:587, 1992
23. Hollstein M, Sidransky D, Vogelstein B, Harris CC: p53 mutations in human cancers. Science 253:49, 1991
24. Gaidano G, Ballerini P, Gong JZ, Inghirami G, Neri A, Newcomb EW, Magrath IT, Knowles DM, Dalla-Favera R: p53 mutations
in human lymphoid malignancies: Association with Burkitt
lymphoma and chronic lymphocytic leukemia. Proc Natl Acad Sci
USA 88:5413, 1991
25. Ichikawa A, Hotta T, Takagi N, Tsushita K, Kinoshita T,
Nagai H, Murakami Y, Hayashi K, Saito H: Mutations of p53 gene
and their relation to disease progression in B-cell lymphoma. Blood
79:2701, 1992
26. Imamura J, Miyoshi I, Koeffler H P p53 in hematologic malignancies. Blood 84:2412, 1994
27. Prokocimer M, Rotter V: Structure and function of p53 in
normal cells and their aberrations in cancer cells: Projection on the
hematologic cell lineages. Blood 84:2391, 1994
28. Villuendas R, Piris MA, Algara P, Sanchez-Beato M, Sanchez-Verde L, Martinez JC, Omadre JL, Garcia P, Lopez C, Martinez
P The expression of p53 protein in non-Hodgkin’s lymphomas is
not always dependent on p53 mutations. Blood 82:3151, 1993
29. Sander CA, Yano T, Clark HM, Harris C, Longo DL, Jaffe
ES, Raffeld M: p53 mutation is associated with progression in follicular lymphomas. Blood 82:1994, 1993
30. LoCoco F, Gaidano G,Louie DC, Offit K, Chaganti RSK,
Dalla-Favera R: p53 mutations are associated with histologic transformation of follicular lymphoma. Blood 82:2289, 1993
31. Banks PM, Chan J, Clearly ML, Delsol G, de Wolf-Peeters
C, Gatter K, Grogan TM, Harris NL, Isaacson PG, Jaffe ES, Mason
D, Pileri S, RalflciaerE, Stein H, Wamke RA: Mantle cell lymphoma:
A proposal for unification of morphologic, immunologic, and molecular data. Am J Surg Pathol 16:637, 1992
32. Zucca E, Stein H, Coiffier B: European lymphoma task force
(ELTF): Report of the workshop on mantle cell lymphoma (MCL).
Ann Oncol 5:507, 1994
33. Glisin V, Crkvenjakov R, Byus C: Ribonucleic acid isolated
by cesium chloride centrifugation. Biochemistry 13:2633, 1974
3359
34. Orita M, Iwahance H, Kanazawa H, Hayashi K, Sekiya T:
Detection of polymorphisms of human DNA by gel electrophoresis
as single-stranded conformation polymorphisms. Proc Natl Acad Sci
86:2766, 1989
35. Peinado MA, Femandez-Renart M, Capella G, Wilson L,
Perucho M: Mutations in the p53 suppressor gene do not correlate
with c-K-rus oncogene mutations in colorectal cancer. Int J Oncol
2:123, 1993
36. Sambrock J, Fritsch EF, Maniatis T (eds): Molecular Cloning:
A Laboratory Manual. Cold Spring Harbor, NY, Cold Spring Harbor
Laboratory, 1989
37. Beck JS, Kwitek AE,Cogen PH: A denaturing gradient gel
electrophoresis assay for sensitive detection of p53 mutations. Hum
Genet 91:25, 1993
38. Sheffield VC, Cox DR, Lerman LS, Myers RM: Attachement
of a 40-base-pair G+C-rich sequence (GC-clamp) to genomic DNA
fragments by the polymerase chain reaction results in improved
detection of single-base changes. Proc Natl Acad Sci USA 86:232,
1989
39. Prosser J, Condie A: Biallelic ApaI polymorphism of the
human p53 gene (TP53). Nucleic Acid Res 19:4799, 1991
40. Ory K, Legros Y, Auguin C, Soussi T: Analysis of the most
representative tumour-derived p53 mutants reveals that changes in
protein conformation are not correlated with loss of transactivation
or inhibition of cell proliferation. EMBO J 13:3496, 1994
41. Wattel E, Preudhomme C, Hecquet B, Vanrumbeke M, Quesne1 B, Dervite I, Morel P, Fenaux P p53 mutations are associated
with resistance to chemotherapy and short survival in hematologic
malignancies. Blood 843148, 1994
42. Inghirami G, Macri L, Cesarman E, Chadbum A, Zhong J,
Knowles DM: Molecular characterization of CD30+ anaplastic largecell lymphoma: High frequency of c-myc proto-oncogene activation.
Blood 83:3581, 1994
43. Matsushima AY, Cesarman E, Chadbum A, Knowles DM:
Post-thymic T cell lymphomas frequently overexpress p53 protein
but infrequently exhibit p53 gene mutations. Am J Path01 144:573,
1994
44. Matsushima AY, Cesarman E, Knowles DM: Mutations are
not detected outside p53 gene exons 5 to 9 in lymphoid tumors. Lab
Invest 70:115, 1994 (abstr)
45. Danova M, Giordano M, Mazzani G, Ricardi A: Expression
of p53 protein during the cell cycle measured by flow cytomety in
human leukemia. Leuk Res 14:417, 1990
46. Chang H, Benchimol S, Minden MD, Messner HA: Alterations of p53 and c-myc in the clonal evolution of malignant
lymphoma. Blood 83:452, 1994
47. Swerdlow SH, Habeshaw JA, Murray LJ, Dhaliwal HS, Lister
TA, Stansfeld AG: Centrocytic lymphoma: A distinct clinicopathologic and immunologic entity. A multiparameter study of 18 cases
at diagnosis and relapse. Am J Pathol 113:181, 1983
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1996 87: 3351-3359
p53 gene mutations and protein overexpression are associated with
aggressive variants of mantle cell lymphomas
L Hernandez, T Fest, M Cazorla, J Teruya-Feldstein, F Bosch, MA Peinado, MA Piris, E
Montserrat, A Cardesa, ES Jaffe, E Campo and M Raffold
Updated information and services can be found at:
http://www.bloodjournal.org/content/87/8/3351.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.









© Copyright 2026