
In Vivo Effect of Human Granulocyte-Macrophage Colony
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
In Vivo Effect of Human Granulocyte-Macrophage Colony-Stimulating Factor on
Megakaryocytopoiesis
By Massimo Aglietta, Clara Monzeglio, Fiorella Sanavio, Franco Apra; Silvia Morelli, Alessandra Stacchini,
Wanda Piacibello, Federico Bussolino, GianPaolo Bagnara, Giorgio Zauli, Angelika C. Stern, and F. Gavosto
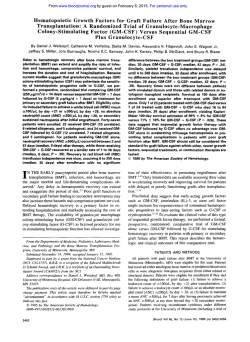
The effect of granulocyte-macrophage colony-stimulating
factor (GM-CSF) on megakaryocytopoiesis and platelet production was investigated in patientswith normal hematopoiesis. Three findings indicated that GM-CSF plays a role in
megakaryocytopoiesis. During treatment with GM-CSF (recombinant mammalian, glycosylated; SandozIScheringPlough, 5.5 p,g proteinlkgld, subcutaneously for 3 days) the
percentage of megakaryocyte progenitors (megakaryocyte
colony forming unit [CFU-Mk]) in S phase (evaluated by the
suicide technique with high JH-Tdr doses) increased from
31% & 16% to 88% f 11%; and the maturation profile of
megakaryocytes was modified, with a relative increase in
more immature stage 1-111 forms. Moreover, by autoradiogra-
phy (after incubation of marrow cells with 'Bl-labeled GMCSF) specific GM-CSF receptors were detectable on megakaryocytes. Nevertheless, the proliferative stimulus induced
on the progenitorswas not accompanied by enhanced platelet production (by contrast with the marked granulomonocytosis). It may be suggested that other cytokines are
involved in the regulation of the intermediate and terminal
stages of megakaryocytopoiesis in vivo and that their intervention is an essential prerequisite to turn the GM-CSFinduced proliferativestimulus into enhanced platelet production.
o 1991 by The American Society of Hematology.
H
(including differential) and platelet counts, and normal hemoglobin (Hb)levels. Liver and kidney functions were normal, and no
signs of abnormalities were present. No concomitant treatments
with corticosteroids, sulphonamides, H, antagonists, nonsteroid
anti-inflammatory drugs, or lithium were administered.
GM-CSF. Recombinant GM-CSF (mammalian, glycosylated;
Sandoz/Schering Plough) in purified lyophilized form was obtained
by the recombinant DNA technique from a mammalian cell system.
Study design. GM-CSF was administered to six patients by
subcutaneous route (2.8 pg of p r o t e i a g every 12 hours for 3 days).
Before and during the course of the study, the patients were
monitored daily by recording of vital signs, physical examination,
and determination of the complete blood counts with differential.
Bone marrow morphology. Megakalyocyte maturation was detined according to Williams and Levine.l6
finetic investigation of marrow-committed progenitors. The fraction of CFU-GM, BFU-E, and CFU-Mk in DNA synthesis (S
phase) was assessed, as previously described, by the suicide
technique after exposure to high-specific-activity tritiated thymidine (3H-Tdr) before culturing in semisolid media!
The marrow light-density fraction was collected after Ficoll
Hypaque (FH)separation (Lymphoprep; Nyegaard, Oslo, Norway), washed three times and resuspended in 0.5 mL of Iscove's
modified Dulbecco's medium (IMDM, Flow Laboratories, Imine,
UK) + 10% fetal calf serum (FCS; Flow Laboratories) at a
concentration of 2 x lo6 cells/mL. Five tubes were prepared and
UMAN GRANULOCYTE-macrophage colony-stimulating factor (GM-CSF) is a cytokine active on
hematopoietic cells. In vitro, it stimulates the proliferation
of all myeloid progenitors and, alone or in combination with
other growth factors, supports the formation of colonies
composed of mature cells.'-5
In vivo, in both normal subjects and patients with
hematopoietic disorders, GM-CSF stimulates the production of granulocytes and monocytes and activates mature
cells."" This finding confirms in vitro observations that the
molecule acts at all maturation levels of the granulomonopoietic differentiation pathway. Its effects on the
other myeloid lineages are less clear: in situations of
impaired hematopoiesis, increased production of erythrocytes and megakaryocytes has been reported incon~tantly.'*-'~
In a previous paper: we provided data to explain the
variable effects of GM-CSF on erythropoiesis: it increases
the proliferative activity of erythroid progenitors (erythroid
burst forming unit [BFU-E]), whereas it does not affect that
of erythroblasts, presumably as a consequence of a progressive loss of GM-CSF receptors during erythroid maturation. These data suggested that the endogenous levels of
other cytokines such as erythropoietin were crucial in order
that the proliferative stimulus induced on BFU-E resulted
in an increased production of erythrocytes.
We now extend our analysis to megakaryocytopoiesis to
demonstrate that, in subjects with normal hematopoiesis,
GM-CSF treatment increases the proliferative activity of
megakaryocyte progenitors (megakaryocyte colony forming
unit [CFU-Mk]) and modifies the maturation stages of
megakaryocytes. Moreover, we show that megakaryocytes
have receptors for GM-CSF. Accordingly, these findings
suggest that GM-CSF has an in vivo effect on megakaryocytopoiesis.
MATERIALS AND METHODS
Patients. Patients with histologicallyproven neoplasia not involving the myeloid system and with normal bone marrow participated
in the study. Each patient gave written informed consent, according to the Helsinki declaration. All patients had normal leukocyte
8/ood,Vol77,No6(March15),1991: pp1191-1194
From the Clinica Medica A, Dipadmento di Scienze Biomediche ed
Oncologia Umana, Universita di Torino; Istituto Di Istologia ed
Embriologia Generale, Univemith di Bologna; Divisione Ginecologia
C, Ospedale S. Anna, Torino; Dipaiiimento di Genetica, Biologia e
Chimica Medica, Universitri di Torino, Italy; and Clinical Research,
Sandoz Phanna Ltd, Basel, Switzerland.
Submitted May 23,1990; accepted November 8, 1990.
Suppoiied by grants from the Italian Association for Cancer
Research and from MPI 60%.
Address reprint requests to Massimo Aglietta, MD, Clinica Medica
A, via Genova 3,10126 Torino, Italy.
The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
"advertisement" in accordance with 18 U.S.C. section 1734 solely to
indicate this fact.
0 I 9 9 1 by The American Society of Hematology.
0006-4971/91/7706-ooO2$3.00/0
1191
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1192
AGLIETTA ET AL
incubated with: medium (in duplicate), 0.5 mg/mL cold thymidine
(Sigma Laboratories, St Louis, MO), 'H-Tdr (100 p,Ci/mL, specific
activity: 20 Ci/mmol/L; Amersham International, Buckinghamshire, UK, in duplicate). After 30 minutes of incubation at 3 7 T ,
the reaction was stopped by the addition of 5 mL ice-cold Hank's
balance salt solution (HBSS; Flow Laboratories) containing 0.5
mg/mL unlabeled thymidine. After three washes, the cells were
resuspended in IMDM: CFU-GM, BFU-E, and CFU-Mk cultures
were prepared with previously described procedures6." by seeding
1 X 105 cells/dish (for CFU-GM and BFU-E) and 3 x 10' cells/dish
(for CFU-Mk) of the original cell suspension. The following
medium and growth factors were used: 10% conditioned medium
of the 5637 cell line for CFU-GM; 10% human cord blood
endothelium supernatant and 1.5 IU erythropoietin (Toyobo,
Osaka, Japan) for BFU-E; and 10% conditioned medium of the
Mo cell line for CFU-Mk. After 7 and 14 days of incubation, the
number of clones was evaluated by two independent investigators.
CFU-GM and BFU-E were identified by their morphology,
CFU-Mk identification was performed by means of 515 (CD4lw), a
monoclonal antibody (MoAb) directed against the glycoprotein
(GP) IIb-IIIa complex: binding was shown by fluorescinated goat
antimouse IgG (Ortho-Diagnostic System, Raritan, NJ).
The percentage of progenitors in the S phase of the cell cycle
(Ns) was determined by applying the following formula: Ns = Nc Nt/Nc, where Nc is the number of colonies or bursts in the controls,
and Nt is the number of colonies or bursts in the samples treated
with high-dose 'H-Tdr.
Receptor studies. Marrow cells from normal donors were obtained with two separation techniques. In two cases (samples 1 and
2), buf€y coat cells were obtained by centrifugation for 10 minutes
at 80%. In one case (sample 3), enriched marrow megakaryocyte
populations were obtained by separation on Percoll gradient
(density 1.050).
Ten million cells per milliliter were incubated for 2 hours at
room temperature in a rotating system, with 1,000 pmol/L Y-GMCSF with and without a 1,000-fold excess of unlabeled GM-CSF.
They were then layered on a solution at 75% FCS. Cells were
centrifuged for 10 minutes at 4 Q , suspended in phosphatebuffered saline (PBS), and cytocentrifuge slides were prepared.
Slides were fixed for 30 seconds at room temperature in phosphate
buffer with 8% formaldehyde and 65% acetone, covered with
Kodak NTB2 emulsion (Eastman Kodak, Rochester, NY),and
incubated in the dark. After 4 weeks, slides were developed, fixed,
and cells were counterstained with May-Grunwald-Giemsa. The
degree of megakaryocyte labeling was evaluated under the light
microscope by counting the number of grains per cell and subtracting the background labeling. Specific labeling is equal to the
difference between the number of grains in specimens incubated
with '"I-GM-CSF only and those incubated with unlabeled GMCSF in excess.
Table 2. Effect of GM-CSF Treatment on the Percentage of S Phase
Marrow Progenitors
~~
Day of Study
Day 7 CFU-GM
Day 14 CFU-GM
BFU-E
CFU-Mk
6.7
4.5
0.16
0.34
11.7
291
1.5
1.0
+ 0.08
0.20
+ 0.4
? 49
?
+
+
36 ? 8
40 f 15
39 14
31 16
59 L 5 t
58 L 6'
71 + 1 8 t
88 ? 14t
+
+
RESULTS
Subcutaneous administration of GM-CSF resulted in a
marked granulo-monocytosis, whereas lymphocyte, erythrocyte, and platelet numbers were not affected (Table 1).
These results are similar to those previously observed after
continuous intravenous infusion in a similar group of
patients6
Table 2 shows that the percentage of myelopoietic
progenitors in S phase increased during treatment. A
particularly interesting new finding was the increment in
the proliferative activity of megakaryocyte progenitors (the
percentage of S phase CFU-Mk increased from 31% ? 16%
to 88% ? 14%). Moreover, the number of CFU-Mk per
milliliter of marrow increased from 299 ? 269 to 842 2 599.
Despite this proliferative stimulus induced by GM-CSF on
CFU-Mk, the number of circulating platelets was unchanged, suggesting that either megakaryocyte development or platelet release was not affected by the treatment.
To analyze the effect of GM-CSF treatment on morphologically recognizable megakaryocytes,two approaches were
used.
First, a morphologic analysis was performed to investigate whether GM-CSF treatment could modify the maturation profile of megakaryocytes (Table 3). A significant
decline in the percentage of mature (stage IV) megakaryocytes with a relative accumulation of the immature forms
occurred during treatment.
Second, a search for specific GM-CSF receptors on
megakaryocytes was made by incubating normal marrow
cells with '"I-GM-CSF and subsequent analysis of labeled
Table 3. Modifications in the Maturation Stages of Megakaryocytes
Induced by GM-CSF Treatment
Day of Study
Leukocytes (xlOg/L)
Neutrophils (xlOg/L)
Eosinophils (x109/L)
Monocytes (x109/L)
Hb (9%)
Platelets (x109/L)
3
Results are expressed as means f SD of the values obtained from six
patients (CFU-Mk data refer to four patients).
Absolute growth in controls (range of colony number per dish): day 7
CFU-GM: 40-273; day 14 CFU-GM: 21-104; BFU-E: 38-372; CFU-Mk:
20-131.
*P < .05 compared with data at day 0.
t P < .01 compared with data at day 0.
Table 1. Modificationsof Peripheral Blood Parameters Occurring
After Three Days of Treatment With GM-CSF
0
0
Day of Study
3
17.0 f 8.4*
13.0 f 7.0*
0.93 f 0.63'
0.78 + 0.20
11.4 f 0.9
301 76
+
Results are means ? SD of the values obtained from six patients.
* P < .01 compared with data at day 0.
Stage 1
Stage 2
Stage 3
Stage 4
0
3
7?3
21 + 7
5 3 + 15
19 5
7+4
30 9
58 + 13
5 + 3*
*
+
~
Results are expressed as means f SD of the values obtained from six
patients. At least 100 megakaryocytes were evaluated per each patient.
*P < .01 compared with data at day 0.
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
GM-CSF AND MEGAKARYOCYTOPOIESIS
1193
Table 4. Binding of "'OM-CSF (expressed as mean number of grains
per cells 2 SEI to Marrow MegakaryocytesFrom Normal Donors Not
Undergoing GM-CSF Treatment
Sample 1
Sample 2
Sample 3
Total GM-CSF
Bound
GM-CSF Binding
Specific
Binding
11 f 0.9
19 f 2.4
75 f 5.1
4.9 2 0.8
9.0 2 1.4
4425
56%
53%
40%
Nonspecific
Megakaryocytes were obtained from marrow buffy coat (samples 1
and 2) or after Percoll separation (sample 3). At least 50 megakaryocytes were counted for each point in samples 1 and 2 andmore than
150 in sample 3.
Fig 1. Autoradiographic preparation showing a megakaryocyte
labeled with '"I-GM-CSF. A megakaryocyte-enriched populationwas
obtained by Percoll separation of normal marrow cells.
cells. Megakaryocytes showed a significant labeling (Fig 1)
that was partially decreased by incubating marrow cells with
an excess of unlabeled GM-CSF (Table 4). This displacement of labeled GM-CSF, similar to that observed by
Fraser et a1," who studied the presence of erythropoietin
receptors on marrow megakaryocytes, strongly suggests the
presence of specific GM-CSF receptors on megakaryocytes.
DISCUSSION
These findings in subjects with normal hematopoiesis
throw some light on the effect of GM-CSF in thrombocytopoiesis in vivo.
Three observations suggest that GM-CSF plays a role in
megakaryocytopoiesis:
(1) There is a highly significant increase in the proliferative activity of CFU-Mk during subcutaneous GM-CSF
administration. Based also on in vitro evidence^'^^" showing
that GM-CSF alone supports the formation of megakaryocyte colonies, we suggest that GM-CSF stimulates CFU-Mk
by directly acting on progenitors. However, the possibility
of an indirect effect, caused by enhanced release of other
cytokines (ie, interleukin-6 [IG6], etc) can not be ruled
OUt.7,21-ZS
(2) GM-CSF treatment modifies the maturation profile
of megakaryocytes, inducing a relative increase in the more
immature forms.
(3) Incubation with labeled GM-CSF and autoradiography shows the presence of specific GM-CSF receptors on
megakaryocytes.
However, despite these observations, treatment with
GM-CSF did not alter the number of circulating platelets.
This finding contrasts with the marked proliferative stimulus induced by GM-CSF through the granulocyte-monocyte
line, resulting in a modulation in marrow composition with
a rapid and marked granulo-monocytosis (Table 1)?('
Seeking an explanation for this difference in effect, it
must be remembered that many cytokines promote (eg,
thrombopoietin, IL-6) or limit (eg, transforming growth
factor p) platelet p r o d ~ c t i o n . ' ~ "In~ subjects with normal
hematopoiesis, changes in marrow levels of these cytokines
could offset the proliferative stimulation of megakaryocyte
progenitors induced by pharmacologic doses of GM-CSF.
This hypothesis may also explain why GM-CSF has an
inconstant effect on the restoration of platelet production
when hematopoiesis has been affected (ie, by chemotherapy, marrow transplantation). In these situations the final
outcome of the proliferative stimulus of GM-CSF on early
phases of megakaryocytopoiesis is less predictable because
it depends on the number of residual progenitors and on
endogenous cytokine levels.
In conclusion, our data show that GM-CSF action is
restricted to early phases of megakaryocytopoiesis and does
not influence platelet production in subjects with normal
hematopoiesis. This result is presumably because of the fact
that other stimulating or inhibiting factors are of decisive
importance in the regulation of the intermediate and final
stages of platelet production in vivo. In perspective, a
sequential treatment with GM-CSF followed by cytokines
acting at a late stage (presumably thrombopoietin or IL-6)
might prove to stimulate platelet production in vivo.
ACKNOWLEDGMENT
We are indebted to M. Roland0 for secretarialassistance.
REFERENCES
1. Aglietta M, Piacibello W, Stem AC, Gavosto F Human
granulocyte-macrophage colony stimulating factor: Target cells
and kinetics of response, in Clark SC, Golde DW (eds): Hematopoiesis. New York, NY, Wiley-Liss, 1990, p 23
2. Groopman JE, Molina JM, Scadden D T Hematopoietic
growth factors: Biology and clinical applications. N Engl J Med,
321:1449,1989
3. Hoffman R: Regulation of megakaryocytopoiesis.Blood 7 4
1196,1989
4. Laver J, Moore MAS: Clinical use of recombinant human
hematopoietic growth factors. J Natl Cancer Inst 81:1370,1989
5. Morstyn G, Burgess A W Hemopoietic growth factors: A
review. Cancer Res 485624,1988
6. Aglietta M, Piacibello W, Sanavio F, Stacchini A, Apri F,
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1194
Schena M, Mossetti C, Carnino F, Caligaris Cappio F, Gavosto F
Kinetics of human hemopoietic cells after in vivo administration of
granulocyte macrophage colony stimulating factor. J Clin Invest
83:551,1989
7. Aglietta M, Monzeglio C, Apri F, Mossetti C, Stern AC,
Giribaldi G, Bussolino F In vivo priming of human normal
neutrophils by granulocyte macrophage colony stimulating factor:
Effect on the production of platelet activating factor. Br J Haemato1 75:333,1990
8. Baldwin GC, Gasson JC, Quan SG, Fleischmann J, Weisbart
R, Oette D, Mitsuyasu RT, Golde D W Granulocyte-macrophage
colony stimulating factor enhances neutrophil function in acquired
immunodeficiency syndrome patients. Proc Natl Acad Sci USA
85:2763, 1988
9. Groopman JE, Mitsuyasu RT, DeLeo MJ, Oette DH, Golde
D W Effect of recombinant human granulocyte-macrophage colony stimulating factor on myelopoiesis in the acquired immunodeficiency syndrome. N Engl J Med 317593,1987
10. Kaplan SS, Basford RE, Wing ET,Shadduck R K The effect
of recombinant human granulocyte-macrophage colony stimulating factor on neutrophil activation in patients with refractory
carcinoma. Blood 73:636,1989
11. Sullivan R, Fredette JP, Socinski M, Elias A, Antman K,
Schnipper L, Griffin JD: Enhancement of superoxide anion release
by granulocytes harvested from patients receiving granulocytemacrophage colony stimulating factor. Br J Haematol71:475, 1989
12. Antman KS, Griffin JD, Elias A, Socinski MA, Ryan L,
Cannistra SA, Oette D, Whitley M, Frei E, Schnipper L E Effect of
recombinant human granulocyte-macrophage colony stimulating
factor on chemotherapy induced myelosuppression. N Engl J Med
319:593,1988
13. Brandt SJ, Peters WP, Atwater SK, Kurtzberg J, Borowitz
MJ, Jones RB, Shpall EJ, Bast RC, Gilbert CJ,Oette DH: Effect of
recombinant human granulocyte-macrophage colony stimulating
factor on hematopoietic reconstitution after high dose chemotherapy and autologous bone marrow transplantation. N Engl J Med
318:869,1988
14. Vadhan-Raj S, Buescher S, LeMaistre A, Keating M, Walters R, Ventura C, Hittelman W, Broxmeyer HE, Gutterman JU:
Stimulation of hematopoiesis in patients with bone marrow failure
and in patients with malignancyby recombinant human granulocytemacrophage colony stimulating factor. Blood 72:134,1988
15. Vadhan-Raj S, Keating M, LeMaistre A, Hittelman WN,
McCredie K, Trujillo JM, Broxmeyer HE, Henney C, Gutterman
JU: Effects of recombinant human granulocyte-macrophage colony
stimulating factor in patients with myelodysplastic syndromes. N
Engl J Med 317:1545,1987
16. Williams N, Levine RF: The origin, development and
regulation of megakaryocytes. Br J Haematol52173,1982
17. Gugliotta L, Bagnara GP, Catani L, Gaggioli L, Guarini A,
Zauli G, Belmonte Mattioli M, Lauria F, Macchi S, Tura S: In vivo
AGLIETTA ET AL
and in vitro inhibitory effect of alpha-interferon on megakaryocyte
colony growth in essential thrombocytemia. Br J Haematol71:177,
1989
18. Fraser JK, Lin FK, Berridge MY: Expression of high affinity
receptors for erythropoietin on human bone marrow cells and on
the human erythroleukemic cell line HEL. Exp Hematol 162336,
1988
19. Bruno E, Miller ME, Hoffman R: Interacting cytokines
regulate in vitro human megakaryocytopoiesis. Blood 73:671, 1989
20. Lu L, Briddel RA, Graham CD, Brandt JE, Bruno E,
Hoffman R: Effect of recombinant and purified human haematopoietic growth factors on in vitro colony formation by enriched
populations of human megakaryocyte progenitor cells. Br J Haemato1 70:149, 1988
21. Sisson SD, Dinarello C A Production of interleukin 1-alpha,
interleukin 1-beta and tumor necrosis factor by human mononuclear cells stimulated with granulocyte-macrophage colony stimulating factor. Blood 721368,1988
22. Cicco NA, Lindemann A, Content J, Vandenbussche P,
Lubbert M, Gauss J, Mertelsmann R, Herrmann F Inducible
production of interleukin-6 by human polymorphonuclear neutrophils: Role of granulocyte-macrophage colony-stimulating factor
and tumor necrosis factor-alpha. Blood 75:2049,1990
23. Lindemann A, Riedel D, Oster W, Ziegler-Heitbrock HWL,
Mertelsmann R, Herrman F Granulocyte-macrophage colony
stimulating factor induces cytokine secretion by human polymorphonuclear neutrophils. J Clin Invest 83:1308,1989
24. Cannistra SA, Griffin JD: Regulation of the production and
function of granulocytes and monocytes. Semin Hematol 25:173,
1988
25. Bussolino F, Wang JM, Defilippi P, Turrini F, Sanavio F,
Edge11 U S , Aglietta M, Arese P, Mantovani A Granulocyte- and
granulocyte-macrophage colony stimulating factor induce human
endothelial cells to migrate and proliferate. Nature 337471,1989
26. Ishibashi T, Miller SL, Burstein SA: Type-beta transforming
growth factor is a potent inhibitor of murine megakaryocytopoiesis
in vitro. Blood 69:1737, 1987
27. Kishimoto T: The biology of interleukin 6. Blood 74:1, 1989
28. Lotem J, Shabo Y, Sachs L Regulation of megakaryocyte
development by interleukin 6. Blood 74:1545,1989
29. Renninck D, Jackson J, Yang G, Wideman J, Lee F, Hudak
S: Interleukin-6 interacts with interleukin-4 and other hematopoietic growth factors to selectively enhance the growth of megakaryocytic, erythroid, myeloid, and multipotential progenitor cells.
Blood 73:1828,1989
30. Mitaivila MT, Vinci G, Villeval JL, Kieffer N, Henri N,
Testa U, Breton Gorius J, Vainchenker W Human platelet alpha
granules contain a non specific inhibitor of megakaryocyte colony
formation: Its relationship to type beta transforming growth factor
(TGF-beta). J Cell Physiol143:93,1988
From www.bloodjournal.org by guest on February 6, 2015. For personal use only.
1991 77: 1191-1194
In vivo effect of human granulocyte-macrophage colony-stimulating
factor on megakaryocytopoiesis
M Aglietta, C Monzeglio, F Sanavio, F Apra, S Morelli, A Stacchini, W Piacibello, F Bussolino, G
Bagnara and G Zauli
Updated information and services can be found at:
http://www.bloodjournal.org/content/77/6/1191.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.









© Copyright 2026