
DAI en pacientes con función ventricular preservada: ¿cómo
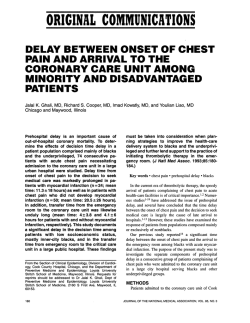
DAI en pacientes con función ventricular preservada: ¿cómo distinguir a la población en riesgo? Dr. Juan Ramón Fabregat Hospital Angeles Lomas 1 Consultar con nuevo miembro de SOMEEC 2 From: Indications for Implantable Cardioverter-Defibrillators Based on Evidence and Judgment J Am Coll Cardiol. 2009;54(9):747-763. doi:10.1016/j.jacc.2009.03.078 Figure Legend: Date of download: 10/18/2013 ICD Indications in Genetic Disorders Associated With SCD Risk Copyright © The American College of Cardiology. All rights reserved. 3 Fuera de las canalopatías confirmadas con fenotipo alterado: 4 The Class I recommendations for ICD Level of Evidence – A With LVEF ≤ 35% due to prior MI who are at least 40 days post-MI and are in NYHA Functional Class II or III With LV dysfunction due to prior MI who are at least 40 days post-MI, have an LVEF ≤ 30%, and are in NYHA Functional Class 1 Who are survivors of sudden cardiac arrest due to ventricular fibrillation (VF) after evaluation to define the cause of the event and to exclude any completely reversible causes Level of Evidence – B With nonischemic DCM who have an LVEF ≤ 35% and who are in NYHA Functional Class II or III With nonsustained ventricular tachycardia (VT) due to prior MI, LVEF < 40%, and inducible ventricular fibrillation or sustained ventricular tachycardia at electrophysiological study With structural heart disease and spontaneous sustained VT, whether hemodynamically stable or unstable With syncope of undetermined origin with clinically relevant, hemodynamically significant sustained VT or VF induced at electrophysiological study * Assuming patients are on chronic, optimal medical therapy and have a reasonable expectation of survival with good functional status for > 1 year. Recommendations for ICD Defibrillators 5 CMS determines that the evidence is adequate to conclude that an implantable defibrillator is reasonable and necessary for patients with 1) A documented episode of cardiac arrest due to ventricular fibrillation (VF), not due to a transient or reversible cause; 2) Documented sustained ventricular tachyarrhythmia, either spontaneous or induced by an electrophysiology (EP) study, not associated with myocardial infarction (MI) and not due to a transient or reversible cause; 3) Documented familial or inherited conditions with a high risk of life-threatening ventricular tachyarrhythmias, such as long QT syndrome or hypertrophic cardiomyopathy; 4) Coronary artery disease with a documented prior myocardial infarction, a measured left ventricular ejection fraction ≤ 0.35, and inducible, sustained ventricular tachycardia (VT) or VF at EP study. (The myocardial infarction must have occurred more than 4 weeks prior to implantable defibrillator insertion. The EP test must be performed more than 4 weeks after the qualifying myocardial infarction.) 6 Class II Recommendations for ICD Defibrillators Level of Evidence – B To reduce sudden cardiac death in patients with Long QT Syndrome who are experiencing syncope and/or ventricular tachycardia while receiving beta blockers Level of Evidence – C With unexplained syncope, significant LV dysfunction, and nonischemic DCM With sustained ventricular tachycardia and normal or near-normal ventricular function With catecholaminergic polymorphic VT who have syncope and/or documented sustained VT while receiving beta blockers For the prevention of sudden cardiac death in patients with ARVD/C who have one or more risk factors for sudden cardiac death With HCM who have one or more major risk factors for sudden cardiac death With Brugada syndrome who have had syncope or documented VT that has not resulted in cardiac arrest With cardiac sarcoidosis, giant cell myocarditis, or Chagas disease For nonhospitalized patients awaiting transplantation * Assuming patients are on chronic, optimal medical therapy and have a reasonable expectation of survival with good functional status for > 1 year. 7 5) CMS determines that the evidence is adequate to conclude that an implantable defibrillator is reasonable and necessary for patients with a documented prior myocardial infarction and a measured left ventricular ejection fraction ≤ 0.30 and a QRS duration of > 120 milliseconds. Patients must not have: New York Heart Association classification IV; Cardiogenic shock or symptomatic hypotension while in a stable baseline rhythm; have Had a coronary artery bypass graft (CABG) or percutaneous transluminal coronary angioplasty (PTCA) within past 3 months; Had an enzyme-positive MI within past month; Clinical symptoms or findings that would make them a candidate for coronary revascularization; or Irreversible brain damage from preexisting cerebral disease; Any disease, other than cardiac disease (e.g. cancer, uremia, liver failure), associated with a likelihood of survival less than one year; and patients must be able to give informed consent. Myocardial infarctions must be documented by elevated cardiac enzymes or Q-waves on an electrocardiogram. Ejection fractions must be measured by angiography, radionuclide scanning or echocardiography. CMS determines that the evidence is not adequate to conclude that an implantable defibrillator is reasonable and necessary for all patients with a prior myocardial infarction, a left ventricular ejection fraction ≤ 0.30, and a QRS ≤ 120 ms. All other indications are also noncovered. 8 9 El problema radica en la selección de riesgos 10 El problema Radica en que la mayor parte de los es en pacientes con FE baja 11 Selected Randomized, Clinical Trials of Implantable Cardioverter–Defibrillator (ICD)Therapy. DiMarco JP. N Engl J Med 2003;349:1836-1847. 12 From: Indications for Implantable Cardioverter-Defibrillators Based on Evidence and Judgment J Am Coll Cardiol. 2009;54(9):747-763. doi:10.1016/j.jacc.2009.03.078 Figure Legend: Date of download: 10/18/2013 Secondary Prevention Trials Copyright © The American College of Cardiology. All rights reserved. 13 From: Indications for Implantable Cardioverter-Defibrillators Based on Evidence and Judgment J Am Coll Cardiol. 2009;54(9):747-763. doi:10.1016/j.jacc.2009.03.078 Figure Legend: Date of download: 10/18/2013 Primary Prevention ICD Trials Copyright © The American College of Cardiology. All rights reserved. 14 From: Indications for Implantable Cardioverter-Defibrillators Based on Evidence and Judgment J Am Coll Cardiol. 2009;54(9):747-763. doi:10.1016/j.jacc.2009.03.078 Figure Legend: Date of download: 10/18/2013 Primary Prevention ICD Trials Copyright © The American College of Cardiology. All rights reserved. 15 16 Risk of Death or Heart Failure Moss AJ et al. N Engl J Med 2009;361:1329-1338 17 18 19 20 Complications of Implantable Cardioverter–Defibrillator Therapy. DiMarco JP. N Engl J Med 2003;349:1836-1847. 21 Baseline Demographic and Clinical Characteristics of the Patients Moss AJ et al. N Engl J Med 2009;361:1329-1338 22 Changes in Mean Echocardiographic Left Ventricular Volumes and Ejection Fraction between Baseline and 1-Year Follow-up Moss AJ et al. N Engl J Med 2009;361:1329-1338 23 24 Se solicita residente:















© Copyright 2026