
PDF Links
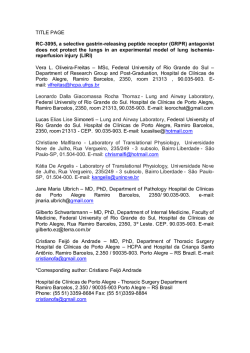
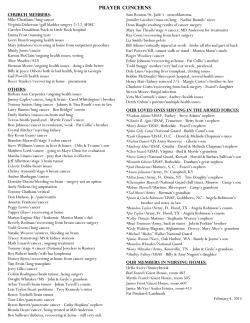
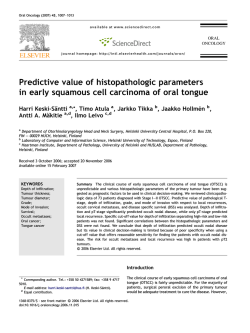
대한내과학회지: 제 88 권 제 2 호 2015 http://dx.doi.org/10.3904/kjm.2015.88.2.202 간세포암종에서 발생한 공동 형태의 폐 전이 서울대학교 의과대학 서울대학교병원 호흡기내과 조용숙·배 원·김주혜·이하연·곽낙원·고성준·이창훈 Cavitary Form of Lung Metastasis from Advanced Hepatocellular Carcinoma Yong Suk Jo, Won Bae, Joo Hae Kim, Ha Youn Lee, Nak Won Kwak, Sung Jun Ko, and Chang-Hoon Lee Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea The most common site of extrahepatic metastasis in cases of advanced hepatocellular carcinoma is the lung. A 60-year-old Korean male had been previously diagnosed with hepatocellular carcinoma and was treated several times with transcatheter arterial chemoembolization prior to a regime of sorafenib after multiple bone metastases were detected. Despite 2 months of systemic treatment, the disease progressed, and newly developed cavitary nodules and ground glass opacities were observed on a chest computed tomography scan. Initially the patient was diagnosed with septic pneumonia and was subsequently treated with antibiotics over 2 weeks, with no observable improvement. A percutaneous transthoracic needle aspiration biopsy was performed to ascertain the noninfectious origin of the lung lesions. As a result, a rare form of pulmonary metastasis from hepatocellular carcinoma was discovered. Unfortunately, there were no available treatment options for the patient and so end-of-life care was recommended. (Korean J Med 2015;88:202-206) Keywords: Hepatocellular carcinoma; Infection; Metastasis INTRODUCTION nodules, generally in the peripheral parenchyma, combined with diffuse interstitial thickening [2]. In advanced hepatocellular carcinoma, metastasis is most of- Because multiple cavitary pulmonary nodules can have di- ten seen intrahepatically, while the lung is the most common verse etiologies such as septic pneumonia, fungal infections, site of extrahepatic metastasis [1]. The typical radiologic find- Mycobacterium tuberculosis infection, vasculitis, and lung meta- ings of pulmonary metastases are multiple, round,variously sized stasis, identifying their origin can be difficult. Received: 2014. 6. 17 Revised: 2014. 7. 22 Accepted: 2014. 8. 28 Correspondence to Chang-Hoon Lee, M.D. Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul 110-744, Korea Tel: +82-2-2072-4743, Fax: +82-2-762-9662, E-mail: [email protected] *Conflict of Interest: The authors disclose no potential conflicts of interest. Copyright ⓒ 2015 The Korean Association of Internal Medicine This is an Open Access article distributed under the terms of the Creative Commons Attribution - 202 - Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited. - Yong Suk Jo, et al. Atypical lung metastasis - Figure 1. Transaxial chest computed tomography scan demonstrating multiple cavitary lesions and ground glass opacities in both lung fields. This case highlights the importance of considering pulmonary metastasis of a hepatocellular carcinoma, even when disease Figure 2. Transaxial chest computed tomography scan demonstrating percutaneous transthoracic needle aspiration biopsy of the left upper lung cavitary lesion. vealed no abnormal pulmonary parenchymal lesions, which would suggest emphysema. The patient underwent a complete work-up, including com- symptoms present with unusual or novel features. puted tomography of the chest. The CT revealed multiple cavitary lesions, patchy consolidation, and ground glass opacities in CASE REPORT both lungs (Fig. 1). At this time, serum levels of acute phase A 60-year-old Korean male was diagnosed 7 years previously proteins were high (C-reactive protein [CRP], 21.45 mg/dL), fe- with chronic hepatitis B with related liver cirrhosis and hep- ver was sustained, and radiological findings supported an in- atocellular carcinoma, which was diagnosed 3 years ago. He had fectious condition. Metastasis was not immediately suspected, undergone transcatheter arterial chemoembolization five times despite a marked increased in tumor marker expression (alpha- because of intrahepatic recurrences and metastases. When bone fetoprotein [AFP], 379.8 ng/mL), as cavitary nodular lung meta- metastases were detected after a work-up to investigate back stases are rarely encountered in hepatocellular carcinoma. Septic and chest pain, he underwent palliative radiation therapy to his pneumonia appeared to be a more likely diagnosis based on the sternum and his cervical and thoracic spine to alleviate bone fever, high CRP levels, and multiple peripheral nodules with pain. Subsequently, sorafenib, a tyrosine kinase inhibitor, was cavitation. Despite our efforts to uncover a septic cause, none prescribed. After 2 months on sorafenib, he was admitted to our could be determined. However, during CT scan and echocardio- hospital with a fever, progressive dyspnea upon exertion, and gram of the abdomen we observed progression of the hepato- general weakness. A chest radiograph identified multiple periph- cellular carcinoma with portal vein tumor thrombus. After sev- eral nodules with cavitation in both lungs. The patient had never eral days of antibiotic treatment, the patient’s fever did not sub- smoked and his baseline lung function was normal. A chest side and radiographic findings showed no improvement. No computed tomography (CT) scan performed 3 years prior re- causative microbiological factors were identified despite a multi- - 203 - - 대한내과학회지: 제 88 권 제 2 호 통권 제 654 호 2015 - A B C D Figure 3. Histopathological findings of the lung. (A) Hematoxylin and eosin staining; original magnification 200×. (B) Immunonegativity for thyroid transcription factor-1 (immunohistochemistry [IHC], 400×). (C) Immunopositivity for cytokeratin 7 (IHC, 400×). (D) Immunopositivity for alpha-fetoprotein (IHC, 400×). disciplinary approach culturing sputum, blood, and urine as well atin 7, and AFP (Fig. 3C and 3D, respectively) and negative for as bronchoscopic alveolar lavage fluid. Considering the possi- thyroid transcription factor-1 (Fig. 3B). Subsequently, the multi- bility of combined radiation pneumonitis, a short-term systemic ple cavitary lung lesions were identified as metastasis from the steroid was administered intravenously, and the patient’s fever primary hepatocellular carcinoma. At this time antibiotic treat- subsequently subsided. However, his condition still showed no ment was terminated. Unfortunately, there were no further treat- clinical or radiographic improvements. His continued lack of re- ment options for the patient and end-of-life care was recommended. sponse to treatment for pneumonia suggested a noninfectious con- Administration of sorafenib was also discontinued. Although the dition. Therefore, a percutaneous transthoracic needle aspiration patient had been taking it regularly, the drug had no effect on biopsy of the lung was performed to ascertain the etiology of the progression of the disease. After discontinuation of the sys- the cavitary lesions (Fig. 2). Histological examination of the spe- temic steroid, the patient’s fever returned; however, there were cimen revealed a poorly differentiated carcinoma (Fig. 3A). Im- no other signs or symptoms suggestive of an infection. The pa- munohistochemistry identified tumor cells positive for cytoker- tient was sent to a convalescent hospital for supportive care, and - 204 - - 조용숙 외 6인. 공동성 결절로 발생한 간세포암 폐 전이 - piration pneumonia. Noninfectious causes of cavitary lesions in- did not return to the outpatient clinic. clude primary tumors and metastasis, various granulomatous diseases, such as sarcoidosis and Wegener’s granulomatosis, arte- DISCUSSION riovenous malformation, pneumoconiosis, and rheumatoid arthriHepatocellular carcinoma is the sixth most common form of tis [6]. Cavitary lesions are detected in only 4% of metastatic cancer worldwide, with predominance in Asia over other regions. nodules, of which approximately 70% are metastatic squamous While it can be successfully treated if diagnosed at an early cell carcinoma [7]. To our knowledge, this is the first report of stage, it remains the third-leading cause of cancer-related deaths cavitary pulmonary metastasis from hepatocellular carcinoma. globally [3]. Although intrahepatic recurrence and metastasis of We believe that central necrosis may have occurred in the rap- hepatocellular carcinoma occur frequently, they can be managed idly growing metastatic nodules or that intratumoral necrosis successfully through various multidisciplinary modalities includ- may have been the cause of cavitary lung metastasis in our ing surgical resection, transcatheter arterial chemoembolization patient. These atypical findings may aid clinicians in cases in and percutaneous ablation or alcohol injection [4]. Therefore, in- which a pulmonary metastasis is difficult to distinguish from an trahepatic recurrence and metastasis can be reasonably managed, infectious condition or where the appropriate treatment plan is prolonging patient survival. Due to the development of new di- unclear. Furthermore, while early lung metastasis is relatively agnostic techniques extrahepatic metastasis is now more fre- asymptomatic, severe respiratory difficulties could develop as quently diagnosed than previously, making it an important in- disease progresses [8]. Additional confounding factors, specifi- dicator of prognosis. The most commonly observed site of ex- cally in our case, included elevated CRP levels, which can be trahepatic hepatocellular carcinoma metastasis is to the lung. related to tumor burden; and fever, which can be triggered by Hepatocellular carcinoma with extrahepatic metastasis is re- pyrogenic cytokines produced by the liver in cases of hep- garded as a terminal condition as there are currently no standard atocellular carcinoma [9,10]. In conclusion, pulmonary metastasis from an advanced hep- treatment courses available [1]. In most cases of pulmonary metastasis from hepatocellular atocellular carcinoma should be considered even if typical pul- carcinoma, the classic radiologic findings include multiple, round monary features are observed. Careful analysis of tumor markers nodules of various size, usually in the peripheral parenchyma, is recommended in these cases. combined with diffuse interstitial thickening [2]. Previously, Assed et al. reported a case of a 26-year-old female, with no history 중심 단어: 간세포암; 감염; 전이 of disease, who presented with multiple nodules, of various size, in both lungs by CT and multiple hyperechoic nodules in the REFERENCES liver, as shown by abdominal ultrasonography. Liver and pleural 1. Ikai I, Arii S, Kojiro M, et al. Reevaluation of prognostic factors for survival after liver resection in patients with hepatocellular carcinoma in a Japanese nationwide survey. Cancer 2004;101:796-802. 2. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma. Radiology 2000;216:698-703. 3. Song MJ, Bae SH. Newer treatments for advanced hepatocellular carcinoma. Korean J Intern Med 2014;29:149155. 4. Uchino K, Tateishi R, Shiina S, et al. Hepatocellular carcinoma with extrahepatic metastasis: clinical features and biopsies were performed, and she was diagnosed with primary hepatocellular carcinoma with multiple pulmonary metastases. The patient died 3 months later despite receiving systemic chemotherapy. Typical pulmonary metastases were reported in this case [5]. Multiple cavitary pulmonary lesions can have various causes, which may be of infectious or noninfectious etiology. Infectious causes are diverse and include bacterial (e.g., Mycobacterium tuberculosis), fungal, parasitic, septic embolism, abscesses, and as- 205 - - The Korean Journal of Medicine: Vol. 88, No. 2, 2015 - prognostic factors. Cancer 2011;117:4475-4483. 5. Assed C, Marchiori E, Zanetti G, et al. Pulmonary metastases from primary hepatocellular carcinoma in a 26-yearold patient: a case report. Cases J 2009;2:6256. 6. Heller I, Biner S, Isakov A, et al. TB or not TB: cavitary bronchiolitis obliterans organizing pneumonia mimicking pulmonary tuberculosis. Chest 2001;120:674-678. 7. Seminara P, Manna G, Emiliani A, Iannace A, Losanno T. An unusual presentation of multiple cavitated lung metastases from colon carcinoma. BMC Med Imaging 2011;11: 13. 8. Natsuizaka M, Omura T, Akaike T, et al. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J Gastroenterol Hepatol 2005;20:1781-1787. 9. Dufour JF. C-reactive protein, a prognostic marker in hepatocellular carcinoma. Hepatology 2013;57:2103-2105. 10. Harimoto N, Shirabe K, Abe T, et al. Interleukin-8 producing hepatocellular carcinoma with pyrexia. HPB Surg 2009; 2009:461492. - 206 -





© Copyright 2026