
Angiomyofibroblastoma of the vulva occurring in a
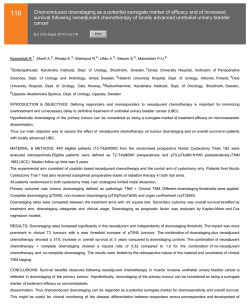
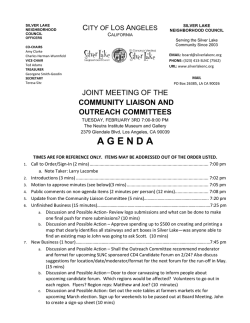
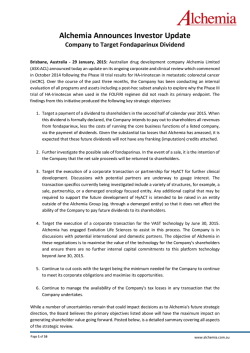
562 Gynaecology case reports References Donnez J., Donnez O., Squif et J. and Nisolle M. (2001) The concept of retroperitoneal adenomyotic disease is born, in: An atlas of operative laparoscopy and hysteroscopy, 2nd edn, edited by Donnez J. and Nisolle M., Chapter 12, pp. 113–117. London, Parthenon. Enatsu A., Harada T., Yoshida S., Iwabe T and Terakawa N. (2000) Adenomyosi s in a patient with the Rokitansky–Kuster–Hauser syndrome. Fertility and Sterility, 73, 862–683. Mitchell C.S., Goske M.J. and Applegate K. (1999) Imaging of Mullerian anomalies, in: Congenital malformations of the female genital tract—diagnosis and management , edited by Gidwani G. and Falcone T., Chapter 4, pp. 55–57. Philadelphia, Lippincott Williams and Wilkins. Angiomyo broblastoma of the vulva occurring in a teenaged girl H. S. QUBLAN,1 L. M. FAYYAD2 and A. S. AL-GHOWERI1 Departments of 1Obstetrics and Gynecology and 2Department of Histopathology, King Hussein Medical Center, Amman, Jordan Angiomyo broblastoma (AMFB) is an angiomyxoma that is related to a group of rare mesenchymal myxoid tumours (Ustun et al., 1998). This recently described benign tumour most commonly involves the soft tissue of the vulva and vagina (Fletcher et al., 1992; Vav Der Griend et al., 1994; Ockner et al., 1997). Patients are usually premenopausal and present with a vulval mass that is often diagnosed initially as a Bartholin’s cyst. This benign tumour should be distinguished from the aggressive angiomyxoma (AA) that has more in ltrative character and high recurrence rate (Hilgers et al., 1986). In this report, we describe a case of angiomyo broblastoma in a 17-year-old female patient. To our knowledge, this is the rst case of angiomyo broblastoma seen in a teenager. Case report A 17-year-old female patient, single, presented with a painless mass of the right vulva, which has been noticed rst by the patient 1 year previously. Menarche was at the age of 13, and cycles were regular. Examination revealed a well-circumscribed, mobile swelling located in the subcutaneous tissue of the right vulva. The preoperative clinical diagnosis was that of Bartholin gland cyst. The lesion was treated by simple excision. The postoperative coarse was uncomplicated, and follow-up for 3 years after excision revealed no recurrence of the tumour. Tumour description Macroscopically, the specimen was composed of an intact lobulated and encapsulated mass measuring 8 ´ 5 ´ 4 cm. Its cut surface was solid, rm and greyish in colour. Microscopically, the haematoxylin and eosin staining revealed an encapsulated neoplasm with a biphasic pattern of proliferating thin-walled blood vessels of variable diameters and of spindled and plump oval stromal cells arranged in hypocellular and hypercellular areas (Fig. 1). The tumour cells had bland nuclei with mitotic gures ranging from 0 to 1/10 HPF. Variable areas of intervening dense collagen bundles were noted as well as areas of oedematous and myxoid stroma. Scattered lymphocytes and mast cells were seen throughout the lesion. There was no evidence of nuclear atypia, adipocytes, histiocytes or necrosis. Immunohistochemicall y, the stromal Figure 1. Hypercellular and hypocellular areas of spindle cell proliferation with collagen bundles (H&E stain, ´ 24). Figure 2. Thin-walled vessels of variable diameters and positive immunstaining for muscle-speci c actin in the spindle cells using anti-muscle-speci c actin (HHF-35, Dakopatts) (´ 60). cells were positive for muscle speci c actin (Fig. 2), vimentin and desmin, but negative for S-100 protein, cytokeratin, CD34, oestrogen and progesterone receptors. The nal diagnosis was angiomyo broblastoma of the vulva. Discussion Angiomyo broblastoma is a rare benign tumour that involving most commonly the soft tissue of the vulva and vagina (Fletcher et al., 1992; Laskin et al., 1998), but rarely it may arises from the female urethra (Kitamura et al., 1999) and fallopian tube (Kobayashi et al., 1999). This tumour was also reported to involve adult men, where it arises from the scrotum or inguinal region (Laskin et al., 1998). Only about 73 cases were reported in the literature, and the patient’s age in these reports ranged from 23 to 86 years. The histogenesis of AMF is unknown. It is possible that these tumours originate from primitive mesenchyma l cells that may have potential for diverse lines of differentiation (Kobayashi et al., 1999), as some of these tumours have been reported to be mitotically active (Takeshima et al., 1998) to contain heterogeneous components, (Fokunaga et al., 1997) and, rarely, can undergo sarcomatous change (Neilsen et al., 1997). The slow-growth wellcircumscribed tumour usually presents as a painless vulval mass and is often misdiagnosed as a Bartholin’s gland cyst, hydrocele of the canal of Nuck or aggressive angiomyxoma (Fletcher et al., 1992; HernandezMonge et al., 2000). Some reports showed that 1–25 years after simple excision of the tumour there was no evidence of recurrence (Fletcher et al., 1992; Laskin et al., 1997). Vulval angiomyo broblastoma may be mistaken for myxoid epithelioid leiomyoma because of the presence of plump cells exhibiting desmin immunoreactivit y. However, these benign tumours are more cellular, lack prominent vascularity, and usually show positive staining for MSA. They have prominent myoid features ultrastructurally in the form of micro laments with focal densities and attachment plaques, which are poorly developed in AMFB (Fletcher et al., 1992). Angiomyo broblastoma should be distinguished from other soft-tissue tumours, most importantly aggressive angiomyxoma, because of the differences in clinical and pathological features, surgical management and follow-up. Gynaecology case reports Clinically, angiomyo broblastoma usually presents as a painless vulval mass measuring 0.5–12 cm (usually < 5 cm) noticed for periods ranging from 10 weeks to 8 years and often misdiagnosed as a Bartholin’s gland cyst. In contrast, the aggressive angiomyxoma is seen potentially over a wider anatomic spectrum, where it presents as a mass of the pelvic soft tissue, retroperitoneum, urinary bladder, vagina, vulva and perineum measuring 3–60 cm (usually > 5 cm) that is noticed for short period, usually a few months (Fletcher, 1992). Pathologically, both tumours contain myxoid stroma that is more uniform in aggressive angiomyxoma and do not demonstrate areas of hypercellularity or dense collagen deposition as in angiomyo broblastoma. Furthermore, the blood vessels of angiomyo broblastoma are thin-walled, venular or capillary-sized, whereas those of aggressive angiomyxoma are characterised by large and thick-walled vascular channels (Okner et al., 1997). Immunohistologically, Okner et al (1997) demonstrated strong similarities in the immunohistological and ultrasrtucural pro les of both aggressive angiomyxoma and angiomyo broblastoma. Comparing three cases of AA with 10 cases of AMFBs, they found that the stromal cells in both groups showed positivity for vimentin, desmin, speci c muscle actin (SMA) and oestrogen receptor protein. Contrary to these results, in a previous study Fletcher et al. (1992) found that the stromal cells of AMFB were positive for vimentin and desmin, negatively for SMA, while those of AA were positive for vimentin and negative for both desmin and SMA. However, immunohistochemical study in our case showed the positivity of stromal cells for SMA, vimentin and desmin, but was negative for oestrogen and progesterone receptor protein. These results suggest the limitation of immunohistochemical studies in differentiation between the two entities. Unlike AMFB which, treated by simple excision, resection of AA with wide tumour-free margins is the treatment of choice to prevent recurrence of the tumour. In conclusion, angiomyo broblastoma is a recently described benign soft tissue tumour that should be distinguished from the aggressive angiomyxoma . The differentiation between the two tumours should be based on clinical behaviour and histological studies. With this report, the patient’s age ranges from 17 to 86 years. 563 References Fletcher C.D., Tsang W.Y., Fisher C., Lee K.C. and Chan J.K. (1992) Angiomyo broblastoma of the vulva: a benign neoplasm distinct from aggressive angiomyxoma. American Journal of Surgical Patholog y, 16, 373–382. Fukunaga M., Nomura K., Matsumoto K., Doi K., Endo Y. and Ushigome S. (1997) Vulval angiomyo broblastoma: clinicopathologic analysis of six cases. Hernandez-Monge A., Estrada-Moscoso I., Alanis-Lopez P. and Villanueva L.A. (2000) Vulvar angiomyo broblastoma. Report of a case and review of the literature. Ginecologia Y Obstetricia de Mexico, 68, 31–34. Hilgers R.D., Pai R., Bartow S.A., Aisenbrey G. and Bowling M.C. (1986) Aggressive angiomyxoma of the vulva. Obstetrics and Gynecology, 68, 605–625. Kitamura H., Miyao N., Sato Y., Matsukawa M., Tsukamoto T. and Sato T. (1999) angiomyo broblastoma of the female urethra. International Journal of Urology, 6, 268–270. Kobayashi T., Suzuki K., Arai T. and Sugimura H. (1999) Angiomyo broblastoma arising from the fallopian tube. Obstetrics and Gynecology, 94, 833–834. Laskin W.B., Fetsch J.F. and Tavassoli F.A. (1997) Angiomyo broblastoma of the female genital tract: analysis of 17 cases including a lipomatous variant. Human Pathology , 28, 1046–1055. Laskin W.B., Fetsch J.F.A and Mosto F.K. (1998) Angiomyo broblastoma like tumor of the male genital tract: analysis of 11 cases with comparison to female angiomyo broblastoma and spindle cell lipoma. American Journal of Surgical Pathology , 22, 6–16. Nielsen G.P., Young R.H., Dickersin G.R. and Rosenberg A.E. (1999) Angiomyo broblastoma of the vulva with sarcomatous transformation. American Journal of Surgical Pathology, 21, 1104–1108. Ockner D.M., Sayadi H., Swanson P.E., Ritter J.H. and Wick M.R. (1997) Genital angiomyo broblastoma: comparison with aggressive angiomyxoma and other myxoid neoplasms of skin and soft tissue. American Journal of Clinical Pathology , 107, 36–44. Takeshima Y., Shinkoh Y. and Inai K. (1998) Angiomyo broblastoma of the vulva: a mitotically active variant? Pathology International, 48, 292–296. Ustun C., Malazgirt Z., Kandemir B., Kocak I., Bolat I. and Gumus S. (1998) Angiomyo broblastoma of the vulva: case report. Pathology Internationa l, 48, 964–966. Vav Der Griend M.D., Burda P. and Ferrier A.J. (1994) Case report. Angiomyo broblastoma of the vulva. Gynecologic Oncology, 54, 389–392. Correspondence to: Hussein S. Qublan, Irbid-Aidun, P.O. Box 97, Jordan. Fax: +962 2 7103268; E-mail: [email protected] Haemangiopericytoma of the sigmoid mesocolon. An unexpected nding during laparoscopic tubal evaluation R. GAZVANI, P. M. KING, W. D. THOMPSON, D. W. NOBLE and M. HAMILTON Grampian University Hospitals, Foresterhill, Aberdeen, UK Case report A 37-year-old healthy woman (Mrs P.S) and her husband were seen in the infertility clinic with a history of primary infertility of 18 months’ duration. Previous investigations of the couple con rmed regular ovulation and suboptimal semen quality. Abdominal examination as well as transvaginal ultrasonography of the pelvis revealed normal ndings and she was listed for a laparoscopic evaluation of her tubal patency (lap and dye) to be carried out as a day case. During laparoscopic examination a solid, vascular, red tumour measuring 6.5 ´ 5.5 ´ 5 cm was noted on the sigmoid colon. Several enlarged vessels could be made out on its surface, measuring up to 0.5 cm in diameter. On closer examination, it appeared to be arising from sigmoid mesocolon. It was partially mobile. During the investigation of the mass, possibly due to disturbance caused by instruments, active bleeding started from one of the vessels. A decision was made to proceed to laparatomy and the mass was removed. It was readily dissected off the colon without any bowel injury and appeared to be encapsulated. The histopathological investigation concluded that the tumour was highly vascular, which was con rmed by CD34 immunostaining. There was a regular pattern of uniform nuclei around these small blood vessels and the appearances were of those of a haemangiopericytoma. The presence of a sharp margin, scarcity of mitoses and lack of pleomorphism were suggested to be reassuring regarding a reduced malignant potential despite the presence of central necrosis (Fig. 1). No further treatment was indicated. A long-term follow-up was nevertheless advised as these lesions could be unpredictable. Further investigations including whole body computed tomography (CT) also found no evidence of further lesions elsewhere. The patient made an uneventful recovery and was discharged home 6 days after the operation to be reviewed in the outpatient clinic. In the management of her infertility, superovulation with intrauterine insemination was carried out 6 months after the initial operation. The patient conceived following one cycle of treatment and an intrauterine, triplet pregnancy was con rmed by ultrasound scan. Pregnancy progressed uneventfully and a caesarean section was carried out at 34 weeks gestation delivering three healthy infants. At the time of section, there was no evidence of recurrence of the tumour on the pelvic colon. Discussion Haemangiopericytoma is a rare and solitary vascular tumour that was rst identi ed and described by Zimmermann (1922) and accounts for less than 1 per cent of vascular tumours. It stems from capillary pericytes (Kuhn and Rosai, 1969), which are contractile pericapillary cells.



© Copyright 2026