
L - Blood
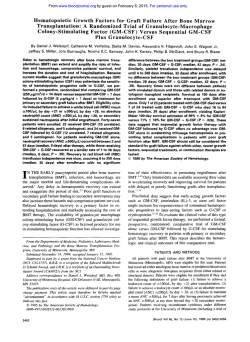
Relationship Between Patterns of Engraftment in Peripheral Blood and Immune Reconstitution After Allogeneic Bone Marrow Transplantation for (Severe) Combined Immunodeficiency By J.E.M. van Leeuwen, M.J.D. van Tol, A.M. Joosten, P.T.A. Schellekens, R . Langlois van den Bergh, J.L.M. Waaijer, N.J. Oudernan-Gruber, C.P.M. van der Weijden-Ragas, M.T.L. Roos, E.J.A. Gerritsen, H. van den Berg, A. Haraldsson, P. Meera Khan, and J.M. Vossen We report the outcome of allogeneic bone marrow transplantation (BMT) as treatment for severe combined immunodeficiency disease (SCID) in 31 patients grafted from 1968 until 1992. The patients received a graft froman HLA-identi(n = cal related (n = 10). anHLA-haplo-identicalrelated 19). or a closely HLA-matched unrelated (n = 2) donor that resulted in the long-term survival of 6 of IO, 9 of 19, and 0 of 2 children, respectively. Major complications included failure of engraftment and early death caused by respiratory failure. The chimerism pattern and immunologic remnstitution were evaluated in 15 children who survived more than 1 year with sustainedengraftment. The pattern of engraftment was investigated within flow-sorted peripheral blood (PB) T- and B-lymphoid, natural killer (NK), and myelomonocytic cell populations using the amplification of variable number of tandem repeats by the polymerase chain reaction. The immunologic reconstitution was assessed by various in vitro andin vivo parameters. Although thenum- ber of PB T cells and thein vitro T-cell proliferative response was in the lower region of normal in the majority of cases and even subnormal in some, in all cases donor T-cell engraftment and reconstitution of T-cell immunity was observed. Residual host-type T cells (1% t o 5%) were detected in eight cases at multiple occasions. All children showed normal serum IgM and IgG subclass levels and produced specific IgG antibodies after vaccination, irrespective of donor B-cell engraftment. However, three HLA haplo-identical cells graft recipients with host-type B lymphoid and myeloid have a persistent selective IgA deficiency. NK cells were either of donor, host, or mixed origin.Donor NK cell engraftment restored defective in vitroNK cell function of the recipient. We conclude that determination of lineage-specific engraftment patterns provides valuable information for the understanding of the immunologic reconstitution after allogeneic BMT for SCID. 0 1994 by The American Society of ffemato/ogy. S graftment of hematopoietic non-T-cell lineages and immunologic reconstitution. We have evaluated the outcome of 31 consecutive cases of allogeneic BMT for SCID performed at the Department of Pediatrics of the Leiden University Hospital. To define the basis of incomplete immune reconstitution after allogeneic BMT for SCID, we determined (1) the degree of engraftment of different hematopoietic cell lineages using fluorescence-activated cell sorting (FACS) and amplification of highly polymorphic variable number of tandem repeats (VNTRs) by the polymerase chain reaction (PCR),8.9and (2) the immunologic reconstitution by a variety of in vivo and in vitro parameters in 15 cases who showed sustained engraftment and survived more than 1 year after BMT. EVERE COMBINED immunodeficiency (SCID) is a heterogeneous group of congenital disorders, characterized by severe impairment of both cellular and humoral immunity, usually leading to death within 2 years of life.’.* Patients with SCID have been treated successfully with HLA identical allogeneic bone marrow transplantation (BMT) since 19683.4and with HLA haplo-identical T-cell-depleted (TCD) BMT since 1981.5 A European survey of the period 1968 to 1989 has shown a probability of survival of 76% and 52% after HLA identical and HLA nonidentical BMT for SCID, respectively.6 Moreover, SCID patients treated after 1983 with an HLA-identical graft showed a probability of survival of 97%: Unfortunately, HLA haplo-identical BMT was frequently associated with failure of engraftment or incomplete immune reconstitution. The use of more intensive conditioning regimens has resulted in a higher frequency of engraftment of B lymphoid and myelomonocytic lineages and improved immunologic reconstitution after HLA haploidentical BMT,6.7which suggests a relation between en- From the Department of Pediatrics, Leiden University Hospital; MGC- Department of Human Genetics, Leiden University, k i d e n ; and Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands. Submitted April 11, 1994; accepted July 27, 1994. Supported by a grant from the Dutch Cancer Society ( I K W 885). Address reprint requests to J.M. Vossen, PhD, MD, Department of Pediatrics, Leiden University Hospital, Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands. The publication costsof this article weredefrayed in part by page charge payment. This article must therefore behereby marked “adveaisement” in accordance with 18 U.S.C. section 1734 .solely to indicate this fact. 0 I994 by The American Society of Hematology. 0006-4971/94/8411-0017$3.00/0 3936 MATERIALS AND METHODS Patients. From December 1968 until July 1992, 47 infants and young children suffering from SCID were referred to the Department of Pediatrics of the Leiden University Hospital for treatment. Eleven of these patients died before transplantation could be performed. Five patients, who lacked a suitable donor and were treated with fetal liver cell transplantation before 1978, died without immunologic reconstitution.“’ The remaining 31 patients, included in this study, were treated by allogeneic BMT. Data were collected until July 1993, giving a minimum follow-up of I year for all children. This study was approved by the Institutional Review Board on Medical Ethics. Patients were classified according to criteria of the World Health Organization” into one of the following categories: SCID with a low number of T and B cells (T-B-), SCID with a low number of T cells, but a normal number of B cells (T-B’), SCID caused by adenosine deaminase deficiency (ADA-), Omenn’s syndrome (OS), and HLA class I1 deficiency (Table 1). Two patients (unique patient numbers [UPNs], 81 and 82) presented with atypical T-B- SCID characterized by a progressive decrease in T-cell function and an almost complete absence of pre-B and more mature B-cell stages, whereas Ig heavy- and light-chain genes of Epstein-Barr virus (EBV) Blood, Vol 84,No 1 1 (December l), 1994: pp 3936-3947 CHIMERISM AND IMMUNITY AFTER BMT FOR SCID 3937 Table 1. Patient Characteristics and Laboratory Findings at Presentation UPN Sex/ Age (mos) 2 5 17 26 50 74 92 105 131 139 4 28 41 53 56 59 81 82 93 94 96 108 112 114 118 126 167 168 183 189 199 M14 MI1 F115 F14 F15 F144 MI6 F182 MI1 F146 MI7 MI9 MI1 MI4 F13 M16 F156 F142 M Pl F114 F12 MI8 MI4 MI6 MP M18 F19 F16 F14 MI11 MP Lymphocytes (96) SCID Type Inheritance T-B' T-B' T-B' (N) T-BT-B' (N) XL Class 11- AR T-B' T-B' AR ADAT-B' T-B' T-B' T-BT-B' T-B+ (N) T-B' T-B" T-B-* Class IIClass IIADAT-B' T-B' T-B' OSt T-B' os T-B- ? AR AR AR AR AR AR ? XL AR ? AR ? AR AR AR AR AR ? ? ? AR ? AR AR os os AR T-B' XL AR Lymphocytes1 PL 600 1,584 1,300 1,650 615 2,888 532 234 96 294 357 1,430 338 248 1,800 532 147 248 1,066 504 300 576 402 1,400 2,886 1,900 1,200 338 5,304 6.31 8 5,375 Serum Ig lmg/dL) K56211 CD3' slg+ CD16' IgM W W 1 + ND ND ND ND ND 44 28 197 169$ 20 716 96* 1286 667* 563* 868 4346 362* ND 1 + 66 21 11 81 2 18 5 11 23 13 2 13 94 53 5 3 1 <l <l 6 43 43 40 30 71 54 <l <l 3 <l 21 <l 71 <l 84 86 <l + 99 <l 66 2 52 <l <l 12 38 54 49 89 92 77 78 <l <l <l 11 99 <l 6 20 58 66 ND ND ND ND ND 5 44 66 12 3 48 47 <l 7 1 13 24 56 25 4 <l <l 127 43 70 97 <l 25 5 59 <l 12 622 130 17 2 1 1 30 153 8 65 47 45 <l <l 4 109 58 8 185$ 9656 129 667 40* 515* 539$ 193$ 1454 338$ 8% 306$ 48 740* 56 257* 322$ 1616 402$ 64* <l 138 <l 126 13 1 132 <l 932 <l 18* <l 11* 54 <l 21 13 <l <l 47 <l <l 1 54 <l <l <l <l 7 <l Lysis -1 ND -1 ND Nll 1 N N - ND ND - N NI Nn - 1 1 N 1 ND ND - ND 1 ND ND N - ND ND Abbreviations: N, Nezelof type; XL, X-linked; AR, autosomal recessive; ND, not done; +, present. * Atypical T-B- SCID.'' t Atypical OS?' *After intramuscular or intravenous-globulin administration and/or transfusion with plasma. 6 IgG probably of maternal origin. 11 Absent (-1, below (C), or above (N) 10th percentile of normal controls.32 Presence or absence of NK activity confirmed using flow-sorted CD16+ NK cells. transformed B-lymphoblastoid cell lineages were retained in germline configuration." Three patients with T-B+ SCID showed Xlinked inheritance as evidenced by pedigree analysis (UPN 28 and 199) or nonrandom X-chromosome inactivation of maternal lymphocytes (UPN 2). Three patients presented with normal or increased serum Ig levels, cytoplasmic-Ig (cIg) containing plasma cells in the BM, and palpable lymph nodes, which are characteristic of Nezelof syndrome." Homogeneous Ig components were detected in the serum ofthe latter patients.I4 UPN 105 showed atypical late-onset T-B' SCID in combination with central deafness. She produced specific IgG antibodies in response to viral infections and vaccination before BMT. UPN 139 showed atypical T-B' SCID with absence of pre-B and B-cell stages, but presence of plasma cells in the BM and presence of IgA plasmacytosis. Three patients presented with HLA class I1 deficiency.15-" Three patients presented with diffuse erythrodermia, blood eosinophilia, hepatosplenomegaly, lymphadenopathy, failure to thrive, increased serum IgE, and recurrent infections, which are all characteristic of OS.'8,'9 Finally, UPN 118 presented with atypical OS; he had diffuse erythrodermia, hepatosplenomegaly, and an oligoclonal expansion of CD8+ T cells, but he showed no eosinophilia and lacked detectable levels of serum IgE.*' The majority of the patients presented with diarrhea, failure to thrive, and recurrent or persistent infections of the respiratory tract (eg, with Pneurnocystis carinii), digestive tract (eg, with rotavirus), mucosa, and/or skin (eg, with C albicans and Staphylococcus aurew). All patients showed an absent or severely decreased in vitro T-cell response towards phytohemagglutinin (PHA) (data not shown). BMT. Transplant-related variables are listed in Table 2. Patients received a BM graft from an HLA-identical related (n = lo), an HLA-haplo-identical related (n = 19) or a closely HLA-matched unrelated (n = 2) donor. Retransplantations were undertaken in six cases because of lack of engraftment and immune reconstitution after a previous attempt. The date ofthe most recent attempt of BMT is considered day 0. Conditioning ofthe patients was performed according to protocols formulated by the European Group for Immunodeficiency (EGID) and the European Group for Bone Marrow Transplantation (EBMT) (Table 2). Measures to prevent graft rejection included rabbit antithymocyte globulin (ATG), Cam- 3938 Table 2. Transplant-Related Variables and Outcome UPN SClD Type 2 5 17 T-B+ T- B T-B' (N) 26 50 T-BT-B' (NI 74 92 + Class 11T- B + 105 131 139 4 28 41 T-B+ ADAT-B+ T-B+ T- B T-B- 53 T-B+ 56 59 81 + T-B' (N) T-6' T-B- Age at BMT GVHD Proph. GVHD Grade (mod 5 4 26 33 5 13 18 M/F M/M F/M F/M F/M FIF F/F -, -,-, -, - 43 7 12 94 1 47 F/F M/M M/M F/M M/F F/F M/F M/M A,-, M/M -, -, -, -, -, -, -,-, -, -, -, -, -, -, A, -, DRt 1 1 1 1 1 1 1 1 2 M/M M/M F/F M/M F/M F/F F/F F/M F/M FIM M/M A, -, DR A, -, DR A,B,DR A, B. DR A,B, DR A,B, A,B, A,B, -t A, B, -t A,B, -t A,B, DR 2 2 2 2 2 3 3 2 2 2 3 A, DR B, 3 - CsA CsA CsA -t 2 2 2 3 3 -t 1 CsA Died?, +21 d, respiratory failure Engraftment failure Died?, +43 d, VOD AW. +6 yrs AW, + 4 yrs Diedll?, + l 2 d, respiratory failure Diedlln, + l 2 d. respiratory failure Died?, +71 d, acute GVHD Diedl, +3 mos, accidental cardiac tamponade Engraftment failure A, + 9 yrs A, +9 yrs, hypopigmentation AW, +9 yrs Engraftment failure Aplasia Died, +6 mos, aplasia Engraftment failure Aplasia Died, +6 mos, aplasia Autologous recovery, died +29 mos, intracranial lymphoproliferative syndrome Autologous recovery, died +2 mos, after second BMT at age 7 yrs, intracranial bleeding AW, +6 yrs, mental retardation AW, +5 yrs AW. +5 yrs Died, +l yr. GVHD + AdV Autologous recovery, died +20 mos. e.c.i. Died, +2 yrs, respiratory failure 2 2 2 2 CsA CsA CsA CsA Died//l, + l 2 d, respiratory arrest AW, t2.3 yrs AW, t1.7 yrs Diedlln, +l 1 d, cardiac arrest 2 CsA AW, +1.0 yr a 28 4 7 12 93 class II- 8 8 57 65 68 43 54 55 71 94 class II- 14 F/M a F/M MF M/F A, M/M 82 T-B- 96 108 112 114 118 ADAT-B+ T- B T-B+ 126 167 T-B+ os 168 183 189 199 T-B+ + 10 5 6 8 HLA Disp (A. B, DR) -, -,- -* -, B.A. -, DR 10 13 M/F B, A, F/M -,-, T-B- 7 os os 12 B,F/F A, F/M MIM DR B, A, 9 MIM B, A, 4 - M/M DRtt - - - MTX - CsA CsA CsA - CsA - CsA - CsA - - Acute Chronic Outcome, Follow-up, Main Cause of Death A, +24 yrs AW, +22 yrs, lost to FU Engraftment failure, AW. + l 6 yrs Diedllf, + l 4 d. respiratory failure Engraftment failure AW, + l 0 yrs. stunted growth -* DR -,-, Other 1 1 1 1 1 1 1 -, -, -, -, -,--,-, - B, A, B, A, os Conditioning TCD§ Regimen Sex R/D DRS DR Abbreviations: RID, recipient/donor; HLA disp, disparity for HLA A, B, and DR antigens on the noninherited haplotype; ATG, 2 mg/kg body weight (BW) x 3 (days -6 through -4); Camp, Campath-IG MoAb at 0.2 mg/kg BW x 2 (days -5 and +3) plus Campath-IM MoAb at 0.2 mg/ kg BW x 1 (day 0); LFA1, 0.2 mg/kg BW x 13 (days -3 through +lo); CD2, 0.2 mglkg BW x 11 (days -2 through +8); VPlGW0, total dose of etoposide in mg/m2; Buwlsno, total busulfan dose in mg/kg BW; Cy~ow12ww, total dose of cyclophosphamide in mglkg BW;TBIw, total-body irradiation dose in Gy; na, not applicable; A(W), alive (and well); FU, follow-up; VOD, veno-occlusive disease; AdV, adenovirus; MTX, methotrexate; CsA, cyclosporin A; Propho, prophylaxis; TCD, T-cell depletion. 1 Ag mismatched (UPN 281 or matched (UPN 167) unrelated donor. t S Patient is homozygous for A t or DRS antigens shared by the donor. 5 TCD protocol: 1, albumin gradient; 2, albumin gradient E-rosetting; 3, Campath-IM plus human complement. I/ Engraftment not evaluable. ll Immune reconstitution not evaluable. + CHIMERISM AND IMMUNITY AFTER BMT FOR SCID 3939 and 11 to14 months of age. Data of these infants were kindly path monoclonal antibody (MoAb) (supplied by the Department of provided by Dr H. RUmke (NIPHEP). Leukemia patients received Pathology, University of Cambridge, Cambridge, UK),” antilymDT-IPV vaccine (I through IV) at 2, 3, 4, and 6 to 24 months after phocyte function-associated antigen-l (LFA1) MoAb?’ or anti-CD2 HLA-identical BMT. Data of leukemic graft recipients were kindly MoAb (Table 2). HLA-identical graft recipients received albumin provided by Dr J. Labadie (Department of Pediatrics, Leiden Univergradienvstem cell-enriched l-log TCD BM.23 The majority of sity Hospital, Leiden, The Netherlands). HLA-non-identical allograft recipients received more than 2-log TCD BM cells after albumin gradient and E-rosette ~eparation?~ or after treatment with Campath-1M MoAb plus human complement.2s RESULTS Additional graft-versus-host disease (GVHD) prophylaxis consisted of cyclosporin A (CsA), 2 m&g/d intravenously (day -5 to +30, MaternoTfetal T-cell engraftment. Materno-fetal T-cell followed by 6 mg/kg/d orally through day +l201 and tapered off engraftment was only looked for in typical SCID patients until discontinuation at day + 180, or methotrexate (Mtx) intrave(ie, with T-B-, T-B+, or ADA-type SCID) in case the absonously at weeklyintervals up to day + 102.26All patients were nursed lute PB CD3+ T-cell count was more then 200/pL at admiswithin the environment of a laminar flow isolator and received prosion (n = 4). This was performed by HLA class I serotyping phylactic antimicrobial medication to suppress their intestinal miof E-rosette-positive T cells and by FPV analysis of ~roflora.’~ PBMCs. Maternal T cells were detected by both techniques Chimerism analysis. Chimerism analysis of fractionated periphin two patients (UPN 56 and 59) who also showed clinical eral blood mononuclear cells (PBMCs), obtained after Ficoll-Isosigns of GVHD at diagnosis. Maternal T cells were absent paque (Pharmacia, Uppsala, Sweden) density-gradient centrifugain one other patient (UPN 17), and no material was available tion, was performed after cell sorting followed by amplification of VNTRs by PCR, so called FACS/PCR-INTR or FPV a n a l y ~ i s . ~ , ~ for analysis in the fourth case (UPN 26). Using FPV chimeCD3+CD4+ and CD3+CD8+ T cells, CD20TD19’ B cells, rism analysis, we also excluded the presence of circulating CD16+CD14- natural killer (NK) cells and CD14+CD16- myelomaternal T cells in one patient with OS (UPN 183). monocytic cell populations were investigated. Two children could Transplant outcome. Transplant-related variables and not be evaluated by FPV analysis either because of technical reasons clinical outcome are listed in Table 2. Engraftment could (UPN 108) or because none of the 5 VNTR markers yielded patient not be evaluated in five children who died within 21 days and/or donor-specific alleles (UPN 131). In these cases, a sex misafter BMT. Successful engraftment after the first BMT was match between the donor and the recipient permitted analysis by obtained in 17 of 26 evaluable children. In 4 of 9 cases with fluorescent in situ hybridization with a Y-chromosome-specific primary graft failure, sustained engraftment was obtained probe (Y-FISH) in combination with simultaneous fluorescent labelafter a second transplant (following intensification of the ing of cell surface antigens.” Ig allotypes were determined in a hemagglutination inhibition assay?9 conditioning regimen). These cases included three patients Immunologic teesrs. Immunophenotypic analysis of PBMCs was who did not receive cytoreductive treatment before the first performed by two-color immunofluorescencemicroscopy or by flowBMT (UPN 17,50 and 53), and one patient (UPN 92) who cytometric analysis using a FACStar flow cytometer and commershowed residual alloreactivity and expressed no adverse clincially available MoAb in appropriate dilutions. From 1 year after ical symptoms after BCG vaccination and transfusion with BMT onwards, investigations were performed at irregular time internonirradiated blood products before BMT. The other 5 cases vals. Age-matched reference values for PB counts of lymphocytes, of primary graft failure were observed after HLA-haploCD3’ T cells, surface Ig+ (sIg+), or CD20+ B cells and CD16+ NK identical TCD BMT, despite the use of high-dose myeloablacells (5% to 95% confidence intervals) were kindly provided by tive conditioning. Strikingly, the children with atypical T-BProfessor Dr J.J.M. van Dongen (Erasmus University Rotterdam, The Netherlands). Serum Ig isotype and IgG subclass levels were SCID (UPN 81 and 82) showed repeated graft failure, even determined by radial immunodiffusion and dot immunobinding after infusion of Campath MoAbs in vivo and conditioning assay, respectively, and compared with age-matched reference valwith total-body irradiation. Additional attempts of grafting ues ( 2 2 SD).30 in vitro T-cell proliferative capacity was assessed were not undertaken in the remaining cases of graft failure, either in whole blood or in standard PBMCs using microculture ie, in two siblings with HLA class I1 deficiency (UPN 93 techniques following mitogenic (PHA and/or antilymphocyte serum and 94) and in one infant with atypical OS who showed a [ALS]), allogeneic (mixed lymphocyte culture [MLC]), or pseudonormal response in MLC before BMT (UPN 118), either antigenic (anti-CD3) stimuli and compared with normal reference because of parental refusal (UPN 93 and 94) or because the values (5% to 95% confidence intervals)?’ In vitro NK cell function patient had suffered from severe veno-occlusive disease after was measured by spontaneous cytotoxicity towards the K562 erythBMT (UPN 118). UPN 94 ultimately died after a second roleukemia cell line in standard 4-hour 5’Crrelease assays and compared with reference values (10% to 90% confidence intervals).” transplant performed elsewhere. Specific IgG antibody production was determined in serum taken 2 The actual survival percentage after HLA-identical reto 4 weeks after in vivo immunization with diphtheria toxoid (D), lated, HLA-haplo-identical related, and closely HLAtetanus toxoid (T), andheat-inactivated poliomyelitis (P) virus type I, matched unrelated BMT was 60% (6/10), 47% (9/19), and 11, and 111(DT-IPV) vaccine using routine techniques at the National 0% (0/2), respectively. As seen in Table 2, major causes of Institute of Public Health and Environmental Protection (NIPHEP, death were primary graft failure (n = 5) and respiratory Bilthoven, The Netherlands). The children received the DT-IPV infailure (n = 5). All children who died from respiratory failure jections at irregular time intervals after BMT. Data obtained within presented with severe and progressive lung infection (Pcari1 month after discontinuation of daily plasma infusions or biweekly nii, Aspergillus or cytomegalovirus) before BMT. intravenous immunoglobulin (IVIG) therapy were excluded from With the exception of three cases (UPNs 2, 53, and 56), analysis. Control groups consisted of 20 healthy infants and 20 children who received an HLA-identical BM graft for leukemia. all long-term survivors are alive and well (Kamofski score, Healthy infants received DT-IPV vaccine (I through IV) at 3, 4, 5 , 100%; Table 2). UPN 2 suffered from recurrent skin infec- VAN LEEUWEN ET AL 3940 Table 3. Cell Lineage-Specific Patterns of Engraftment After BMT Time UPN 2 17 50 105 131 53 56 59 96 108 112 126 168 183 199 Diagnosis T-B+ (N)T-B+ (N)T-B+ T-B' ADAT-B' T-B' (N) T-B+ ADAT-B' T-B+ T-B' T-B- os T-B+ Conditioning Regimen CylzoTBI, B~16cV200 BUSCYZOO ATGlCVloo ATGICVZOO ATG ATGlB%Cyzoo B~lscYzoo B~sCy,oo ATGJCymc BUSCYZOO LFAl/Bu&mo BU&ZOO TCD 1 1 1 l 1 2 2 2 2 Chimerism* (vs) Post-BMT +22.9 +15.4 +8.8 +5.1 +2.2 +8.1 +8.4 +8.1 +5.7 2 +2.7 2 +4.0 +1.0 +1.0 +1.0 +1.0 1 2 2 2 VNTR r/D 33.6 HRAS r/D D r/D D r/D r/D APOB D YNZ22 Y-FISH* D APOB 33.6 D YNZ22 YNZ22 YNZ22 D D D D D rlD r/D r/D YNZ22t APOBS Y-FISH* 33.6 B NK R/d RID RID D r/D RID R r/D RID D r/D D R R/d R/d RID D R D D R/d R/d RID T APOB R/d D R D D r/D r/D R/d MM R/d D r/D R R R/d R R R/d R/d R/d Abbreviations: TCD, T-cell depletion; MM, myeloid/monocytic cells; TBI. total-body irradiation; Bu, busulfan; Cy, cyclophosphamide; ATG, antithymocyte globulin; APOB, apolipoprotein B; HRAS, Harvey RAS. *The predominant origin, either recipient (R) or donor (D), of the cell populations is given uppercase, in whereas a minor population( ~ 1 0 % ) is indicated in lowercase (r or d. respectively); If donor and recipient derived cells were present in near equal amounts, both populations are given in uppercase (ie. R/D). t The presence of recipient-derived cells cannot be excluded. Determined by Y-FISH analysis. * tions caused by S aureus in association with acne and warts, and experienced a severe S aureus sepsis and pneumonia once, at the age of 7 years; he is now under flucloxacillin prophylaxis. UPN 53 suffered from recurrent upper respiratory tract infections (URTI) with encapsulated bacteria until the age of about 10 years; he is now scheduled for tympanoplasty of both ears; he still suffers from warts on feet and hands. UPN 56 recovered from her extensive chronic GVHD of the skin, except for persisting hypopigmentation of skin and hair. Chimerism patterns. Lineage-specific patterns of engraftment and immune reconstitution were evaluated in 15 of 16 children who survived more than 1 year after BMT with sustained engraftment. UPN 5, who showed complete immune reconstitution, but lacked engraftment in B lymphoid and erythroid lineages,33was lost to follow-up and could not be evaluated. PB T cells were exclusively or predominantly of donor origin in all children, whereas B -, NK- and myeloid cell populations were either of recipient, donor, or mixed origin (Table 3 and Fig l, A through C, last follow-up). Surprisingly, residual (1% to 5 % ) host T cells were detected in eight cases up to 23 years after BMT. Except for UPN 2 and 105, these residual host-type T cells were detected at multiple occasions. In three cases who received no conditioning before BMT, engraftment of the myeloid cell lineage was absent or extremely limited. In addition, myeloid cells remained predominantly of host origin in 7 of 12 children who received prior cytoreductive treatment. Five children showed (complete) engraftment in all cell lineages. The origin of serum Igs after BMT was evaluated by Ig allotyping. Unfortunately, a discriminating Ig allotype marker was not available in 12 of 15 donorhecipient pairs. Both donor and recipient Ig allotypes were detected in the serum of UPN 17, and recipient Ig allotypes were found in the serum of UPN 53 and 59 (data not shown), in agreement with the results obtained by FPV analysis. PB lymphocyte numbers. Longitudinal analysis of the absolute numbers of various PB lymphocyte subsets showed considerable fluctuations of cell counts in the children who were frequently investigated. Results of the last follow-up are summarized in Table 4. We repeatedly observed subnormal absolute lymphocyte and CD3' T-cell counts in five cases (UPN2, 53, 56, 131, and 168), although they were incidentally within normal range for UPN 2 and 56 at the last follow-up. In general, decreased counts were observed in both CD4' and CD8' T-cell subsets in graft recipients with a diminished number of CD3' T cells. Three children (UPN 2, 56, and 105) showed an increased percentage of y6 T lymphocytes at the last evaluation (40%, 17%, and 19%, respectively). Although UPN 168 and 183 repeatedly showed a decreased number of circulating B cells, the absolute numbers of CD16+ NK and CD20' and/or sIg+ B cells were within the normal range in the majority of cases. In vitroT-cellproliferation. Analyses were performed at irregular time intervals after BMT. The results of the last investigation are summarized in Table 4. The in vitro proliferative T-cell response towards PHA, ALS, and antiCD3 MoAb in whole blood cultures and the response towards PHA in standard PBMC cultures was repeatedly decreased in three children (UPN 2, 53, and 131). The in vitro T-cell response towards alloantigens, as determined in the MLC, wasdecreased at multiple occasions in one case (UPN 53). B-cell immune reconstitution. Longitudinal analysis of serum Ig classes and IgG subclasses was performed from 1 CHIMERISM AND IMMUNITY AFTER BMT FOR SCID 3941 All evaluable children (n = 14) who survived more than 1 year after BMT with sustained engraftment showed a posi- LC, 872 bp -603 bp I Fig 1. Cell lineage-specific patterns of engraftment after allogeneic BMT for SCID.(A) UPN 2,23 years after HLA-identicalBMT (APOB VNTR); (B) UPN 53, 8 years after HLA-haplo-identical BMT (33.6 VNTR); and (C) UPN 168, 1 year after HLA-haplo-identical BMT (YNZ22 VNTR). Pre-BMT patient (PI- and donor (D)-specificbands are indicated. PCR-VNTR analysiswas performed on DNA obtained from the cell populationsindicatedabove each lane. Negative control samples were included in each amplification experiment and found to be negative (not shown in Fig 1A). Although a faint (+Yo) recipient-typespecific band was visible in the CD3'CD4' and CD3TD8' T-cell fractions on the autoradiogram of Fig 1C. this could not be visualized on the photograph. year after BMT onwards. Three children (UPN 53, 59 and 199) showed a persistent selective IgA deficiency (IgA-D) after BMT. Some secretory IgA was detected in the tears of UPN 53, but not in those of UPN 59. In several of the other cases, serum levels of total IgG,IgG subclasses and IgA occasionally dropped below the lower confidence limit (-2 SD) of age-matched controls, but none of them showed a persistent deficiency in these subclasses (Table 5). tive IgG antibody response towards at least one T-cell-dependent recall antigen after repeated DT-IPV immunizations posttransplant (Table 5). UPN 199 was considered nonevaluable because he received only two injections of DT-IPV vaccine and has notyetproduced specific IgG antibodies towards any of the DT-IPV antigens. Although UPN 59 did not respond to D or IPVI.IIIantigens, even after 6 DT-IPV injections, he produced specific IgG antibodies toward tetanus, and toward rubella after natural infection (data not shown). As seen in Table 6, the cumulative response rates of the grafted SCID patients towards DT-IPV antigens, as observed within 6 months after BMT, are inferior to those of healthy infants, but comparable to those observed after BMT for leukemia. In this context, it should be noted that the majority of graft recipients received immunosuppressive therapy up to 6 months posttransplant, which may explain the poorer specific antibody responses when compared with healthy infants. Additional immunization with DT-IPV vaccine more than 6 months after BMT for SCID further increased the cumulative response rate: graft recipients who received at least a total of four injections of DT-IPV vaccine or showed a positive antibody response after previous vaccination showed a cumulative response rate towards D, T, IPV,, IPVII, and IPVlllof 75% (9/12), 100% (l3/13), 92% (l2/13), 85% (1 1/13), and 75% (9/12), respectively (Table 5 ) . In comparison, healthy infants exhibit a 100% cumulative response rate toward DT-IPV antigens from DT-IPV IV onward, and children grafted for leukemia exhibit a 100% cumulative response rate toward tetanus toxoid from DT-IPVIV onward.23a In vitro NK cell function. The in vitro NK cell function of the children after BMT is summarized in Table 4 and Fig 2. Engraftment of donor NK cells was associated with restoration of NK cell activity in two graft recipients with a defective NK cell function before BMT (UPN 1 12 and 131). Although NK cells were completely of donor origin, UPN 126 showed decreased in vitro NK cell activity. The in vitro NK cell function of this patient before BMT was not determined. The N K cell function was only partially restored in three graft recipients (UPN 2, 17, and 59), perhaps because in these children, a mixture of functionally defective recipient NK cells and normal donor NK cells was present after BMT. None of the latter cases received cytoreductive treatment before BMT. We also observed normal NK cell activity in transplant recipients without or with only marginal NK cell engraftment (UPN 53, 56, 168, and 183). This finding is in agreement with the normal NK cell activity observed before BMT in three of these cases (UPN 53, 56, and 168). For unknown reasons, NK cell activity could not be detected in cryopreserved samples obtained before BMT in the fourth case (UPN 183). DISCUSSION From December 1968 until July 1992,31infantsand young children with SCID were treated by allogeneic BMT at the Department of Pediatrics in Leiden, The Netherlands. 3942 ET LEEUWEN VAN Table 4. Immunologic Reconsitution After BMT for SClD Proliferation T-cellIn Vitro PBMC Counts UPN 2 Diagnosis Time (yrsl PostBMT T-B+ +22.9 Standard Lymphocytes/ CD3'1 /JL @L pL 2,604 CD20+/ pL CD%+/ K562 PHA ALS Infections z1 yr Post-BMT a-CD3 Lysis11MLCO PHA i 103 5,120t 2,422 6,630 10,900t 5,400t 130 130 HPV (warts), S aureus (sepsis. pneumonia) 17 50 105 131 53 T-B'(N) T-B' (N) T-B' ADAT-B' +15.4 +8.8 +5.1 +2.7 +8.1 1,846 3,280 2,100 1,280' 1,100' 1,403 2,296 1,176* 755' 495' 158 222 22,415 10,900 37,900 11,500 203 426 459 357 357 90' 358 242 297 56 59 96 108 112 126 168 183 199 T-B+ (N) T-B' ADAT-B' T-B' T-BT-B- +8.4 f8.1 +5.7 +4.7 +4.0 +1.8 +2.5 +1.0 +1.0 2,262 1,260* 2,130 1,911' 2,508 884' 504* 2,000 7,410 1,312 1,134 1,065 975* 1,956 339 88* 490 363 426 OS T-B+ ND ND 151* 1,500 4,668 45* 20' 2,742 452 25' 554 554 125 ND 111 280 222 53,700 15,100 1 N N N 4,810 146 34,689 ~ 15,000 1,400t 300t 27,700 9,700t 5,300t 11,200 1,060t 150t 14,330 4.592$ 287t 59 132 29 2,900t 8,900 19,500 16,400 14,000 11,300 1,900t 26,500 24,900 6,800t 37,100 33.700 29,100 45,800 14,500 10,100t 36,000 49,200 890t 1,760 20,553 12,619 29,590 19,214 28,436 11,965 7,578t 33,469 51,194 166 24 N l - ND NE ND N - ND ND 9,360 2,140 3,800 12,100 6,220 ~ - N 166 117 151 59 252 84 HPV (warts), URTl ~ - l ~ N N ND ~ Abbreviations: HPV, human papilloma virus; ND, not done; NE, not evaluable. * Below fifth percentile of age-matched controls. t Below fifth percentile of control values, ie <6,000 counts per minute (cpm) for PHA, <14,000 cpm for ALS, and <l600 cpm for a-CD3." Below 2.5 percentile of control values, ie, <8,400 c p ~ n . ~ ' § Response capacity, percent of two controls (250% is considered normal). /I Above (N) cq below (1)10th percentile of controls32(see also Fig 2, A through D). * The actual survival is 60% after HLA-identical BMT (n = lo), 47% after HLA-haplo-identical BMT (n = 19) and 0% after closely HLA-matched unrelated BMT (n = 2). If patients with HLA class I1 deficiency or OS, disorders associated with a poor prognosis,34are excluded from our report, the actual survival after HLA identical and HLA non-identical BMT for SCID is 67% and 53%, respectively. Similar probabilities of survival have been reported by the EBMT in the 1968-1989 survey (ie, 76%and 52% after HLA-identical and HLA-nonidentical BMT, respectively).6Major obsta- Table 5. Humoral Immune Reconstitution After BMT for SClD Serum Ig UPN Time (yrs) Post-BMT IgM IgG No. of DT-IPV Vaccinationst Levels (mg/dL) Total IgA lgGl lgG2 lgG3 71* 421 167 262 25 29 73 lgG4 Specific IgG Antibody Productiont D+ TS IPV,,,§ IPV,,§ IPV,§ 111 II I 111 111 Ill ___~ _ ~ 2 1,190 173 +15.4 17 50 105 131 53 56 +8.1 59 085 109 +5.7 96 108 97 112 663 126 04 101 +1.6 168 f1.5 183 199 +22.9 667 110 +8.8 +3.1 +2.7 +8.3 +8.4 194 134 119 398 128 73 1,311 56 57 88 294 1,106 635 162 651 186 877 1,110 917 4' 974 909 44' 1,011 507* <l* 327* +4.7 78 933 163 89 +4.0 571 137 +2.2 4,028 369 50 71136 402 350 f 1 . 0 1,769 136 158 80* 87 302 106 82 620 141 2,395 51274 746 125 < l59 * 1,558 417 28 124 71 100 46 14 VI 31 15 11 16 4* 86 50 20 59 127 47 33 20 3 11 9 37 XI VI IV 111 IV VI Vlll VI V V IV V VI Ill Ill I1 Humoral Immune Reconstitution - IVIV ~ 111 ~ V IV ~ V 111 IV I II II IV I Ill " - - VI1 II 111 - IV IV II - V 111 IV I 111 111 - _ IX I1 111 111 _ ~ ~ VI1 II It1 - - - IV II IV Ill ~ V v - V - V I Ill V I 111 - - - - _ ~ * Below mean -2 SD of age-matched controls." t The number of the DT-IPV immunization after which the positive response occurred is indicated (-, no positive response). * Positive if the postimmunization titer wasat least twice thepreimmunization titer. § Positive if the postimmunization titer was at least 4 times the preimmunization titer. _ _ ~ Complete Complete Complete Complete Complete Selective IgA-D Complete Selective IgA-D Complete Complete Complete Complete Complete Complete Selective IgA-D ~ AND CHIMERISM FOR SCID 3943 Table 6. Cumulative Response RatesToward DT-IPV Antigens After Three Vaccinations of Healthy Infants. and of Pediatric Graft Recipients Within 6 Months After BMT D 60% Healthy infants (n = 20) Pediatric BMT recipients Leukemia (n = 20) 60% SCID IWm IPV,, IPV, T ~PVI-III* 83% 89% 90% 90% 90% 25% (2/8)t 64% (7/11) 56% (5/9) 44% (4/9) 25% (2/8) 100% 67% (6/9) Response to either IPV,, IPV,,, or IPV,,,. t Number of patients who showed a positive response among those who either received three DT-IPV injections or showed a positive response after previous vaccination within 6 months after BMT. cles for short-term success were early death caused by respiratory failure (n = 5), and primary graft failure (n = 9) ultimately leading to death in five cases. The children who died from respiratory failure all presented with progressive lung infection before BMT, an important adverse risk factor in the EBMT survey: Graft failure was observed after unconditioned BMT (n = 3) and, despite prior cytoreductive treatment, in patients with T-B+ SCID (n = l), atypical OS (n = 1)'; atypical T-B- SCID (n = 2),12and HLA class I1 deficiency (n = 2). Successful engraftment was obtained in four of six patients who received a second transplant. Sixteen graft recipients were alive for more than 1 year after BMT, and data on these cases are included in this evaluation (except for UPN 5, who was lost to follow-up). With the exception of an episode of severe S aureus infection in UPN 2, recurrent URTI in UPN 53, and persistenthecurrent warts in both cases, no signs or symptoms of a subnormal immunologic defense capacity were present in the long- A. B. '"1 0 5 10 15 20 0 25 5 10 15 20 25 EK mtlo ratio D. C. ap 10 / l 0 15 5 20 10 ratio 25 , , n 0 5 10 1s 20 26 E/T mtlo Fig 2. in vitro NK c e l l activity after BMT for SCID.PBMCs of the children were collected M o r e (pre) or after (post) BMT. Testa were lines represent 10% and 90% confidence intervals of fresh performed using either fresh (A andB) or cryopreserved IC and D) material. Dashed (n = 66;A and B) or cryopreserved In = 33; C and D) control samples. Posltransplant NK cells of the children were either of rmlpient origin (A and C), donor and recipient origin (B), or donor origin (D). 3944 VAN LEEUWEN ET AL term survivors at a median (range) follow-up of 6 (1 to 24) sponses for many years after BMT, in contrast to the obseryears after BMT. Noneof the childrenreceived Ig suppletion vations of Wijnaendts et al.37 more than 6 months after BMT. Except for UPN 2 , who is Defective in vitro NK cell function in SCID patients before BMT32.38.39 and nonrandom X-chromosomeinactivation on flucloxacillin prophylaxis for his tendency to develop S aureus skin infection, none of the long-term survivors rein NK cells of female obligate XSCID carriers4" has been ceived antimicrobial prophylaxis more than 6 months after described, suggesting that NK cells are intrinsically defective BMT. in a subset of patients with SCID. Here, we show that NK In 15 children and young adults, weinvestigated the relacells can be either of recipient, donor, ormixed origin. Donor tionship between engraftment of different cell lineages and T- and B-cell engraftment was not always associated with immune reconstitution. In the majority of cases, FPV chimedonor NK cell engraftment, supporting the ideathat NK cells rism analysis showed the presence of complex, cell lineage belong to a separate lymphoidlineage. All evaluable children specific patterns of engraftment, which are not observedafter showed in vitro NK cell activityafter BMT. Importantly, high-dose conditioning andallogeneic BMT for le~kemia.'.'~ engraftment of NK cells was associated with increased in Interestingly, conditioning withbusulfan (8 to 16 mgikg vitro NK cell function in children who showed defective in BW) plus cyclophosphamide was not sufficiently myeloablavitro NK cell activity before BMT. Accordingly, incomplete NK cell engraftmentresulted in partial restoration of in vitro tive inthe majority of children to eradicate host-type hematopoiesis. In a previous study, we noted a high incidence of NK cell function in such cases. All children with sustained engraftment showed evidence persistent host-type hematopoiesisinchildren less than2 of humoral immune reconstitution after BMT. None of the yearsof age grafted for leukemia afterconditioningwith busulfan (16 to24mgikgBW)plus cy~lophosphamide.~~ children showed apersistentIg isotype deficiency, except for three cases (UPN 53, 59, and 199) who lacked B-cell These findings may be explained by altered pharmacokinetengraftmentand displayedalong-lastingselective IgA-D ics of busulfan in children as compared with adults leading after BMT for T-B' SCID. Selective IgA-D after HLAto decreased drug exposure in children? Thus, the use of haplo-identical BMT for SCID hasbeenreported also by either no or arelativelymildpreparative regimenbefore other investigator^."^^' Importantly, specific IgG antibodies BMT for SCID leads to the persistence of host-type stem were detected in all evaluable children after repeated DTcells. In turn, these may occupy the space in the BM necesIPV immunization (and after natural infection), irrespective sary for engraftmentof donor stem cells. Under these circumstances, donor cells may be detectable only at the maturaof donor B-cell engraftment. However, the recovery of specificantibodysynthesisafter BMT for SCID may not be tional stage of thehematopoieticcelllineages inwhich complete in all cases as suggested by holes in the antibody recipient cells have defectsin their development andor funcresponses after repeated vaccination (eg, in the case of UPN tion as a result of a selective growth advantage. 59; Table 5). Interestingly,the cumulative responserates Surprisingly, we detected residual (1% to 5%) host-type towards DT-IPV antigens of the group of grafted SCID paT cells in eight of the graft recipients, even more than 23 tients were similar to those observed in children after HLAyears after BMT. Although we cannot formally exclude the identical BMT for leukemia (Table 6). possibility that purified T cells might have been contamiAEuropeansurveyhasshownthatincompletehumoral nated with recipientnon-T cells, we believe that this explanaimmune reconstitution (ie, lack of specific antibody production is unlikely for several reasons. First, all T-cell population or Ig isotype deficiency) after HLA nonidentical BMT tionsthat were purified by cell sorting showed aclearly for SCID is stronglyassociatedwith failure of B-cell endistinct stainingpattern in fluorescence diagrams (results not graftment.'j In agreement with these data, we only observed shown). Second, residual host-type T cells were observed in incompletehumoral immune reconstitution(ie,selective some, but not all children withcelllineage-specific enIgA-D) inchildren who showedno or onlymarginalBgraftment patterns; these host-type T cells were detected on cell engraftment after HLA-haplo-identical BMT for T-B' several occasions in all six children who were investigated SCID. Several mechanisms, which are not mutually exclumore than once. Moreover, residual host-type T cells were sive,may explain the above findings.First,lack of B-cell detected in one childwith predominantly donor cells innonengraftment may lead to incomplete humoral immunereconT-cell lineages (UPN 105). It seems unlikely that the persisstitution after BMT for T-B' SCID, because subtle defects tence of residual host-type T cells can beconfirmed by stanin in vitro B-cell function have been described in a subset dardmetaphasecytogeneticsbecause, in ourexperience, of T-B+ SCIDpatients42and because nonrandom X-chromoFPVchimerismanalysis ismoresensitive andbecause some inactivation has been observed in B lymphocytes obthese host-type T cells most likely do not respond to polytained from female obligate XSCID carriers, suggesting an clonal activators (eg, PHA) used to obtain metaphases for intrinsic B-cell defect.47 More recently, it has been shown karyotyping. In addition,informative cytogenetic markers that XSCID is caused by mutations in the common y ( y J were not available in several of these cases. chain,44 a functionally important component of the IL-2, ILAll children who showed sustained engraftment and sur4, and IL-7receptors.ds-4RThus, we cannot excludethe possivived for more than 1 yearafter BMT showed significant bility that the persistent host-type B cells of children with improvement of T-cell immunity as evidenced by several in incomplete humoral immune reconstitution (UPN 53, 59, vivo andin vitro parameters. However,wefound thata and 199) are intrinsically defective for some, but not all, Bnumber of long-term survivors continued to have low absocellfunctions. However, thehypothesisdescribed above lute T cell counts and low in vitro proliferative T-cell re- CHIMERISM AND IMMUNITY AFTER BMT FOR 3945 SCID does not explain the general finding that incomplete humoral immune reconstitution is observed almost exclusively after HLA nonidentical BMT.6.7.37,49 Second, incomplete humoral immune reconstitution after HLA-nonidentical BMT may be caused by the inability of donor T cells to cooperate with host B cells across major histocompatability complex (MHC) barriers. This model seems unlikely for several reasons: (1) postthymic T cells of murine radiation BM chimeras display MHC restriction patterns towards host MHC antigens5's5' because positive selection is mediated by thymic epithelial cells of host MHC (2) T-B-cell cooperation across MHC barriers gen~type~'-'~; has been shown in several SCID patients after HLA-nonidentical BMT, even at the clonal l e ~ e l ~ ~and . ~ '(3) ; T-B-cell cooperation after HLA-haplo-identical BMT can always occur via the shared HLA haplotype. Third, lack of self-tolerance towards donor-specific HLA class I1 antigens has been observed in SCID patients with incomplete humoral immune reconstitution after HLAhaplo-identical BMT.62" Various studies in mice have indicated that clonal deletion of self-reactive thymocytes is mediated by BM-derived antigen presenting cells in the thymus.65-68 Thus, graft recipients with split chimerism may fail to delete donor thymocytes reactive towards the nonshared donor-specific HLA antigens. Indeed, T-cell-mediated donor-antidonor reactivity towards donor-specific HLA class I1 antigens has been observed in split ~hirneras,6*".~~."but not in complete chimera^.^' In our study, 7 of 10 HLA haploidentical allograft recipients showed split chimerism. Complete humoral immune reconstitution was observed in split chimeras with B-cell engraftment (UPN 56, 168, and 183). Interestingly, studies performed by De Villartay et a16' and Keever et a163 suggest a relation between lack of B-cell engraftment and the presence of donor-antidonor HLA class I1 reactivity. It is tempting to speculate that resting donor B cells, which constitutively express HLA class I1 antigens, but lack costimulatory activity (ie, B7 expression):'may play a role in the functional inactivation of naive donor T cells that recognize donor-specific HLA class Wpeptide complexes. The remaining children with split chimerism (UPN 53, 59, 108, and 199) lacked B lymphoid and myeloid engraftment. Strikingly, LJPN 108 received BM from an HLA class I1 phenotypically identical, MLC-negative, related donor (which was also identical at the HLA DR and DP loci as determined by oligotyping) and showed complete humoral immune reconstitution, whereas the other three graft recipients showed selective IgA-D after HLA class I1 haplomismatched BMT. In these children, expression of donor HLA class I1 antigens is restricted to activated T cells. Although there is no direct evidence showing a causal relationship between the presence of donor-antidonor class I1 reactivityand incomplete humoral immune reconstitution, it seems possible that the presence of donor-antidonor HLA class 11 reactivity in these cases may interfere with T-cell activation, leading to a reduced efficiency of T-B-cell cooperation and incomplete humoral immune reconstitution?* Importantly, such a model provides an explanation for the finding that incomplete humoral immune reconstitution is found almost exclusively after HLA-nonidentical BMT and is restricted to graft recipients who lack B lymphoid and myeloid engraftment. ACKNOWLEDGMENT We thank M. van der Keur and J. Slats for technical assistance in cell sorting experiments and Professor Dr D.W. van Bekkum for critical review of the manuscript. REFERENCES 1. Fischer A: Severe combined immunodeficiencies. Immunodef Rev 3:83, 1992 2. Dooren LJ, Vossen JM: Severe combined immunodeficiency: Reconstitution of the immune system following bone marrow transplantation, in van Bekkum DW, Ewenberg B (eds): Bone Marrow Transplantation. Biological Mechanisms and Clinical Practice. New York, NY, Dekker, 1985, p 351 3. Gatti RA, Allen HD, Meeuwissen H J , Hong R, Good RA: Immunological reconstitution of sex-linked lymphopenic immunological deficiency. Lancet 21366, 1968 4. de Koning J, Dooren LT, van Bekkum DW, van Rood JJ, Dicke K A , Rad1 J: Transplantation of bone marrow cells and fetal thymus in an infant with lymphopenic immunological deficiency. Lancet 1:1223, 1969 5. Reisner Y, Kapoor N, Kirkpatrick D, Pollack MS, Cunningham-Rundles S, Dupont B, Hodes MZ, Good RA, O'Reilly RJ: Transplantation for severe combined immunodeficiency with HLAA,B,D,DR incompatible parental marrow cells fractionated by soybean agglutinin and sheep red blood cells. Blood 61:341, 1983 6. Fischer A, Landais P,Friedrich W, Morgan G, Genitsen ETA, Fasth A, Porta F, Griscelli C, Goldman SF, Levinsky RJ, Vossen JM: European experience of bone marrow transplantation for severe combined immunodeficiency. Lancet 3362350, 1990 7. O'Reilly RJ, Keever CA, Small TN, Brochstein JA: The use of HLA-non-identical T-cell-depleted marrow transplants for correction of severe combined immunodeficiency disease. Immunodef Rev 1:273, 1989 8. van Leeuwen JEM, van To1 MJD, Bodzinga BG, Wijnen JT, van der Keur M, Joosten AM, Tanke HJ, Vossen JM, Meera Khan P Detection of mixed chimaerism in flow sorted cell subpopulations by PCR-amplified VNTR markers after allogeneic bonemarrow transplantation. Br J Haematol 79:218, 1991 9. van Leeuwen JEM, vanTo1 MJD, Joosten AM, Wijnen JT, Meera Khan P, Vossen JM: Mixed T lymphoid chimerism following allogeneic bone marrow transplantation for hematologic malignancies of children is not correlated with relapse. Blood 82:1921, 1993 10. Lowenberg B, Vossen JM, Dooren LJ: Transplantation of fetal liver cells in the treatment of severe combined immunodeficiency disease. Blut 34:181, 1977 11. Rosen FS, Wedgwood RJ, Eibl M, Griscelli C, Seligmann M, Aiuti F, Kishimoto T, Matsumoto S, Khakhalin LN, Hanson LA, Hitzig WH, Thompson R A , Cooper MD, Good RA, Waldmann TA: Primary immunodeficiency diseases. Report of a WHO scientific group. Immunodef Rev 3:195, 1992 12. Thompson A, Hendriks RW, Kraakman MEM, KoningF, Langlois van den Bergh R, Vossen JM, Weemaes CMR, Schuurman RKB: Severe combined immunodefiency in man with an absence of immunoglobulin gene rearrangements butnormal T cell receptor assembly. Eur J Immunol 20:2051, 1990 13. Nezelof C: Thymic dysplasia with normal immunoglobulins and immunologic deficiency: Pure alymphocytosis, in Bergsma D, Good RA (eds): Birth Defects. Original Article Series. Immunological Deficiency Diseases in Man (ed 4). New York, NY, Liss, 1968, P 104 14. Genitsen ETA, Vossen JM, van To1 MJD, Jol-van der Zijde 3946 CM, van der Weijden-Ragas CPM, Radl J: Monoclonal gammopathies in children. J Clin Immunol 9:296, 1989 15. Kuis W, Roord JJ, Zegers BJM, Schuurman RKB,Heijnen CJ, Baldwin WM, Goulmy E, Claas F, van de Griend RJ, Rijkers GT, van Rood JJ, Vossen JM, Ballieux RE, Stoop JW: Clinical and immunological studies in a patient with the “bare lymphocyte” syndrome, in Touraine JL, Gluckman E, Griscelli C (eds): Bone Marrow Transplantation in Europe, v01 2. Amsterdam, The Netherlands, Excerpta Medica, 1981, p 201 16. Schuurman HJ,van de Wijngaert FP, Huber J, Schuurman RKB, Zegers BJM, Roord JJ, Kater L: The thymus in “bare lymphocyte” syndrome: Significance of expression of major histocompatibility complex antigens on thymic epithelial cells in intrathymic Tcell maturation. Hum Immunol 13:69, 1985 17. Griscelli C, Lisowska-Grospierre B, Mach B: Combined immunodeficiency with defective expression in MHC class I1 genes. Immunodef Rev 1:135, 1989 18. Omenn GS: Familial reticuloendotheliosis with eosinophilia. N Engl J Med 273:427, 1965 19. Barth RF, Vergara VE, Khurana SK, Lonman JT: Rapidly fatal familial histiocytosis associated with eosinophilia and primary immunological deficiency. Lancet 1:503, 1972 20. Kuijpers KC, van Dongen JJM, van der Burg P, Roos MT, Vonk J, de Abreu R, de Korte D, van Noesel CJM, Weening RS, van Lier RAW: A combined immunodeficiency with oligoclonal CD8’. VP3-expressing, cytotoxic T lymphocytes in the peripheral blood. J Immunol 149:3403, 1992 21. Fasth A, Porras 0, Friedrich W, Morgan G, Levinsky RJ, Hale G: Haploidentical bone marrow transplantation for immunodeficiency. Invivo conditioning with monoclonal antibodies. J Cell Biochem 12:99,1988 (abstr) 22. Fischer A, Friedrich W, Fasth A, Blanche S , Le Deist F, Girault D, Veber F,Vossen JM, Lopez M, Griscelli C, Him M: Reduction of graft failure by a monoclonal antibody (anti-LFA1 CD1 la) after HLA nonidentical bone marrow transplantation in children with immmunodeficiencies, osteopetrosis, and Fanconi’s anemia: A European Group for ImmunodeficiencylEuropean Group for Bone Marrow Transplantation report. Blood 77:249, 1991 23. Dicke KA, van Bekkum DW: Allogeneic bone marrow transplantation after elimination of immunocompetent cells by means of density gradient centrifugation. Transplant Proc 3:666, 1971 24. Wagemaker G, Heidt PJ, Merchav S , van Bekkum DW: Abrogation of histocompatibility barriers to bone marrow transplantation in rhesus monkeys, in Baum SJ, Ledney GD, Thierfelder S (eds): Experimental Hematology Today. Basel, Switzerland, Karger, 1982, p 111 25. Waldmann H, Polliak A, Hale G, Or R, Cividalli G, Weiss L, Weshler Z, Samual S , Manor D, Brautbar C, Rachmilewitz EA, Slavin S: Elimination of graft-versus-host disease by in-vitro depletion of alloreactive lymphocytes with a monoclonal rat anti-human lymphocyte antibody (Campath-l). Lancet 2:483, 1984 26. Storb R, Epstein RB, Graham TG, Thomas ED: Methotrexate regimens for control of graft-versus-host disease in dogs with allogeneic marrow grafts. Transplantation 9:240, 1970 27. Vossen JM, Heidt PJ, van den Berg H, Gemtsen EJA, Hermans J, Dooren LJ: Prevention of infection and graft-versus-host disease by suppression of intestinal microflora in children treated with allogeneic bone marrow transplantation. Eur J Clin Microbiol Infect Dis 9: 14, 1990 28.van den Berg H, Vossen JM, Langlois vandenBergh R, Bayer J, van To1 MJD: Detection of Y chromosome by insitu hybridization in combination with membrane antigens by two color immunofluorescence. Lab Invest 64:623, 1991 29. Korver K, de Lange G, Langlois van den Bergh R, Schellekens PTA, van Loghem E, van Leeuwen F, Vossen JM: Lymphoid VAN LEEUWEN ET AL chimerism after allogeneic bone-marrow transplantation: Y-chromatin staining of peripheral T and B lymphocytes and allotyping of serum immunoglobulins. Transplantation 44:643, 1987 30. Gemtsen EJA, van To1 MJD, Lankester AC, vander WeijdenRagas CPM, Jol-van der Zijde CM, Oudeman-Gruber NJ, Rad1 J . Vossen JM: Immunoglobulin levels and monoclonal gammopathies in children after bone marrow transplantation. Blood 82:3493. 1993 31. Bloemena E, RoosMTL,van Heyst JLAM, Vossen JM, Schellekens PTA: Whole-blood lymphocyte cultures. J Immunol Methods 122:161, 1989 32. ten Berge RJM, Schellekens PTA, Budding-Koppenol A, Dooren LJ, Vossen JM: Natural killer (NK)-cell activity in sorted subsets of peripheral blood mononuclear cells from patients with severe combined immunodeficiency. J Clin Immunol 7:198, 1987 33. Vossen JM, de Koning J, van Bekkum DW, Dicke KA, Eysvoogel VP, Hijmans W, van Loghem E, Radl J, van Rood JJ, van der Waay D, Dooren LJ: Successful treatment ofan infant with severe combined immunodeficiency by transplantation of bone marrow cells from an uncle. Clin Exp Immunol 13:9, 1973 33a. Gemtsen EJA, vanTo1 MJD, van’t Veer MB, Wels JMA, Khouw IMSL, Touw CR, Jol-van der Zijde CM, Hermans J, R u d e HC, Rad1 J, Vossen JM: Clonal disregulation of the antibody response to tetanus-toxoid after bone marrow transplantation. Blood (in press) 34. Fischer A, Landais P, Friedrich W, Gemtsen EJA, Fasth A, Porta F, VellodiA, Benkerrou M, Jais JP, Cavazzana-Calvo M, Souillet G, Bordigoni P, Morgan G, van Dijken P,Vossen JM, Locatelli F, Di Bartolomeo P: Bone marrow transplantation (BMT) in Europe for primary immunodeficiencies other than severe combined immunodeficiency: A report from the European Group for BMT and the European Group for Immunodeficiency. Blood 83: 1149, 1994 35. van Leeuwen JEM, vanTo1 MJD, Joosten AM, Wijnen JT, Verweij PJM, Meera Khan P, Vossen JM: Persistence of host-type hematopoiesis after allogeneic bone marrow transplantation for leukemia is related to the intensity of the conditioning regimen and/or the recipient age, but not associated with an increased risk of relapse. Blood 83:3059, 1994 36. Grochow LB, KrivitW, Whitley CB, Blazar B:Busulfan disposition in children. Blood 75:1723, 1990 37. Wijnaendts L, Le Deist F, Griscelli C, Fischer A: Development of immunologic functions after bone marrow transplantation in33 patients with severe combined immunodeficiency. Blood 74:2212, 1989 38. Buckley RH, Schiff SE, Sampson HA, Schiff RI, Markert ML, Knutsen AP, HershfieldMS, Huang AT, Mickey GH, Ward FE: Development of immunity in human severe primary T cell deficiency following haploidentical bone marrow stem cell transplantation. J Immunol 136:2398, 1986 39. Peter HH, Friedrich W, Dopfer R, Muller W, Kortmann C, Pichler WJ, Heinz F, Rieger CHL: NK cell function in severe combined immunodeficiency (SCID): Evidence of a common T and NK cell defect in some but not all SCID patients. J Immunol 131:2332, 1983 40. Wengler GS, Allen RC, Parolini 0, Smith H, Conley ME: Nonrandom X chromosome inactivation in natural killer cells from obligate carriers of X-linked severe combined immunodeficiency. J Immunol 150:700, 1993 41. Fischer A, Durandy A, De Villartay JP, Vilrner E, Le Deist F, Gerota I, Griscelli C: HLA-haploidentical bonemarrow transplantation for severe combined immunodeficiency using E rosette fractionation and cyclosporin. Blood 67:444, 1986 42. Gougeon ML, Drean G, Le Deist F, Dousseau M, Fevrier M, Diu A, Theze J, Griscelli C, Fischer A: Human severe combined CHIMERISM ANDIMMUNITY AFTER BMT FOR SClD immunodeficiency disease. Phenotypical and functional characteristics of peripheral B lymphocytes. J Immunol 145:2873, 1990 43. Conley ME, Lavoie A, Briggs C, Brown P, Guerra C, Puck JM: Nonrandom X chromosome inactivation in B cells from carriers of X chromosome-linked severe combined immunodeficiency. Proc Natl Acad Sci 85:3090, 1988 44. Noguchi M, Yi H, Rosenblatt HM, Filipovich AH, Adelstein S , Modi WS, McBride OW, Leonard WJ: Interleukin-2 receptor y chain mutation results in X-linked severe combined immunodeficiency in humans. Cell 73:147, 1993 45. Noguchi M, Nakamura Y, Russell SM, Ziegler SF, Tsang M, Cao X, Leonard WJ: Interleukin-2 receptor y chain: A functional component of the interleukin-7 receptor. Science 262:1877, 1993 46. Russell SM, Keegan AD, Harada N, Nakamura Y, Noguchi M, Leland P, Paul WE, Leonard WJ: Interleukin-2 receptor y chain: A functional component of the interleukin-4 receptor. Science 262:1880, 1993 47. Kondo M, Takeshita T, Ishii N, Nakamura M, Watanabe S , Arai KI, Sugamura K: Sharing of the interleukin-2 (IL-2) receptor y chain between receptors for IL-2 and L-4. Science 262:1874, 1993 48. Kondo M, Takeshita T, Higuchi M, Nakamura M, Sudo T, Nishikawa SI, Sugamura K: Functional participation of the IL-2 receptor y chain inIL-7 receptor complexes. Science 263:1453, 1994 49. Friedrich W, Knobloch C, Greher J, Hartmann W, Peter HH, Goldmann SF, KIeihauer E Bone marrow transplantation in severe combined immunodeficiency: Potential and current limitations. Immunodef Rev 4:315, 1993 50. Singer A, Hathcock KS, Hodes RJ: Self recognition in allogeneic radiation bone marrow chimeras. J Exp Med 153:1286, 1981 51. Sprent J, Lo D, Gao EK, Ron Y: T cell selection in the thymus. Immunol Rev 101:173, 1988 52. Lo D, Sprent J: Identity of cells that imprint H-2-restricted T-cell specificity in the thymus. Nature 319:672, 1986 53. Blackman MA, Marrack P, Kappler JW: Influence of the major histocompatibility complex on positive thymic selection of VP17a+ T cells. Science 244:214, 1989 54. Benoist CO, Mathis D: Positive selection of the T cell repertoire: Where and when does it occur. Cell 58:1027, 1989 55. Hugo P, Kappler JW, Godfrey DI, Marrack PC: A cell line that can induce thymocyte positive selection. Nature 360:679, 1992 56. Vukamanovic S, Grandea AG, Faas SJ, Knowles BB, Bevan MJ: Positive selection of T-lymphocytes induced by intrathymic injection of a thymic epithelial cell line. Nature 359:729, 1992 57. Chu E, Umetsu D, Rosen F, Geha RS: Major histocompatibility restriction of antigen recognition by T cells in a recipient of haplotype mismatched human bone marrow transplantation. J Clin Invest 72: 1124, 1983 3947 58. Roncarolo MG, Touraine JL, Banchereau J: Cooperation between major histocompatibility complex mismatched mononuclear cells from a human chimera in the production of antigen-specific antibody. J Clin Invest 77:673, 1986 59. Roncarolo MG, Yssel H, Touraine JL, Bachetta R, Gebuhrer L, de Vries JE, Spits H: Antigen recognition by MHC-incompatible cells of a human mismatched chimera. J Exp Med 158:2139, 1988 60. Roberts JL, Volkman DJ, Buckley RH:ModifiedMHCrestriction of donor-origin T cells in humans with severe combined immunodeficiency transplanted with haploidentical bonemarrow stem cells. J Immunol 143:1575, 1989 61. Geha RS, Rosen FS: The evolution of MHC restrictions in antigen recognition by T cells in a haploidentical bone marrow transplant recipient. J Immunol 143:84, 1989 62. De Villartay JP, Griscelli C, Fischer A: Self-tolerance to host and donor following HLA-mismatched bone marrow transplantation. Eur J Immunol 16:117, 1986 63. Keever CA, Flomenberg N, Small T, Brochstein JA, Collins N, Young-Yang S, Insel R,Dupont B, O’Reilly RJ: Loss of tolerance associated with disappearance of B cells in a patient sequentially transplanted with paternal and maternal bone marrow for the treatment of severe combined immunodeficiency. Hum Immunol 26:27, 1989 64. Keever CA, Flomenberg N, Gazzola MV, Pekle K, Yang SY, Small TN, Collins NH, O’Reilly RJ: Cytotoxic and proliferative Tcell clones with antidonor reactivity from a patient transplanted for severe combined immunodeficiency disease. Hum Immunol 29:42, 1990 65. Ramsdell FJ, Lantz T, Fowlkes BJ: A nondeletional mechanism of thymic self tolerance. Science 246:1038, 1989 66. Speiser DE, Lees RK, Hengartner H, Zinkernagel RM, MacDonald HR: Positive and negative selection of T cell receptor VD domains controlled by distinct cell populations in the thymus. J Exp Med 170:2165, 1989 67. Yoshikai Y, Ogimoto M, Matsuzaki G, Nomoto K: Bone marrow-derived cells are essential for intrathymic deletion of selfreactive T cells in both the host- and donor-derived thymocytes of fully allogeneic bone marrow chimeras. J Immunol 145:505, 1990 68. Matzinger P, Guerder S: Does T-cell tolerance require a dedicated antigen-presenting cell? Nature 338:74, 1989 69. Schiff SE, Buckley RH: Modified responses to recipient and donor B cells by genetically donor T cells from human haploidentical bone marrow chimeras. J Immunol 138:2088, 1987 70. Keever CA, Flomenberg N, Brochstein JA, Sullivan M, Collins NH, Bums J, Dupont B, O’Reilly RJ: Tolerance of engrafted donor T cells following bone marrowtransplantation for severe combined immunodeficiency.Clin Immunol Immunopathol48:261, 1988 71. Jenkins MK, Johnson JG: Molecules involved in T-cell costimulation. Curr Opin Immunol 5:361, 1993






© Copyright 2026