
Get PDF - ResearchGate
Review
|
doi: 10.1111/j.1365-2796.2007.01892.x
Peroxisome proliferator-activated receptors – from active
regulators of macrophage biology to pharmacological
targets in the treatment of cardiovascular disease
M. A. Bouhlel, B. Staels & G. Chinetti-Gbaguidi
From the De´partement d’Athe´roscle´rose, Institut Pasteur de Lille; U545 INSERM; and Faculte´ des Sciences Pharmaceutiques
et Biologiques et Faculte´ de Me´decine, Universite´ de Lille 2; Lille, France
Abstract. Bouhlel MA, Staels B, Chinetti-Gbaguidi G.
(Institut Pasteur de Lille; U545 INSERM; and Universite´ de Lille 2; Lille, France). Peroxisome proliferator-activated receptors – from active regulators of
macrophage biology to pharmacological targets in the
treatment of cardiovascular disease (Review). J Intern
Med 2008; 263: 28–42.
Altered macrophage functions contribute to the pathogenesis of many infectious, immunological and
inflammatory disease processes. Pharmacological
modulation of macrophage activities therefore represents an important strategy for the prevention and
Introduction
Atherosclerosis is a chronic inflammatory disease and
a main cause of cardiovascular complications. Epidemiological studies have revealed environmental
(stress, smoking and alcohol consumption) and
genetic (dyslipidaemia, type 2 diabetes, insulin resistance and hypertension) risk factors predisposing to
atherosclerosis. This pathology is characterized by an
abnormal accumulation of lipids, necrotic cells and
fibrous elements in the medium and large arteries [1].
Activated endothelial cells (EC), smooth muscle cells
(SMC) and macrophages are amongst the major cells
contributing to atherosclerotic lesion formation and
development [2–4]. The endothelium, a monolayer of
EC, forms a selectively permeable barrier between the
blood and the vascular sub-endothelial space. Whenever mechanical or chemical effectors weaken this
barrier, a response is initiated, characterized by the
activation of EC, which acquire the ability to produce
28
ª 2007 Blackwell Publishing Ltd
treatment of inflammation-related diseases, such as
atherosclerosis. This review focuses on recent
advances on the role of the peroxisome proliferatoractivated receptor transcription factor family in the
modulation of lipid homeostasis and the inflammatory
response in macrophages and the potential participation of these actions in the modulation of metabolic
and cardiovascular disease.
Keywords: cardiovascular disease, gene regulation,
macrophages,
peroxisome
proliferator-activated
receptor.
several molecules that promote monocyte transmigration and lipoprotein particle entry and uptake in the
sub-endothelial space [1]. These events occur already
at an early stage of atherosclerosis. In subsequent
stages, SMC proliferate and produce extracellular
matrix components [5]. SMC proliferation is also a
primary mechanism underlying restenosis, an occlusive complication of corrective angioplasty procedures. Activation of SMC leads to the release of
proinflammatory cytokines, which combined with the
secretion of metalloproteinases and expression of procoagulant factors, results in a chronic inflammation
and plaque instability. This can subsequently evolve
in plaque rupture and acute occlusion by thrombosis,
resulting in myocardial or cerebral infarction and
stroke [1].
In addition to EC and SMC, monocyte-derived macrophages play a central role in the progression of
atherosclerosis. Circulating monocytes recruited by
M. A. Bouhel et al.
|
Review: PPARs
chemokines in the sub-endothelial space undergo
activation by cytokines and modified lipoproteins
that accumulate in the injured space. Thus, activated
monocytes differentiate into macrophages, which can
engorge huge amounts of lipids thus generating foam
cells, central contributors in atherosclerotic plaque
formation. The central process leading to foam cell
formation initially acts as a clearance pathway to
protect surrounding cells from harmful effects of
modified low-density lipoproteins (LDL) such as oxidized LDL (OxLDL). Atherosclerosis progresses to a
pathological condition when such clearance pathway
becomes inefficient and the presence of a large lipid
core in the atherosclerotic lesion correlates with the
severity of the pathology. The macrophages implicated in atherosclerotic lesion formation exhibit a
different pattern of gene expression than resting macrophages, notably with respect to genes involved in
the uptake and efflux of lipids and genes coding for
inflammatory mediators. The expression of such
genes can be modulated by transcription factors such
as the peroxisome proliferator-activated receptors
(PPARs).
Peroxisome proliferator-activated receptors are transcription factors activated by fatty acids and fatty
acid-derived eicosanoids, which modulate gene
expression and, as such, control cellular homeostasis.
Three different isotypes belong to this subfamily of
transcription factors, PPARa, PPARb ⁄ d, and PPARc.
PPARa (NR1C1) is expressed at high levels in tissues
exhibiting active fatty acid catabolism (liver, kidney,
heart and skeletal muscle). PPARc (NR1C3) is abundantly present in white and brown adipose tissue, and
to a lesser extent in cardiac and skeletal muscle,
whereas PPARb ⁄ d (NR1C2) is ubiquitously
expressed. PPARs are also expressed in cells of the
injured vascular wall (monocytes, macrophages, EC
and SMC) and are detected in the sub-endothelial
space and lipid core of atherosclerotic lesions [6]. In
addition to a distinct tissue distribution pattern,
PPARs exhibit distinct functions, whereas PPARa
controls lipid oxidation and clearance in hepatocytes,
PPARc is involved in lipid storage, exerts anti-inflammatory activities and promotes preadipocyte differentiation to adipocytes [7], whereas PPARb ⁄ d is
involved in fatty acid oxidation notably in skeletal
muscle [8, 9].
Much research has been directed towards the development of isotype-specific pharmacological compounds.
The best-characterized synthetic agonists are fibrates
and glitazones. Fibrates are PPARa ligands with lipidlowering properties and glitazones are PPARc ligands
used in the treatment of type 2 diabetes [10]. In addition, drugs that activate multiple PPAR isotypes are
considered for development: dual PPARa ⁄ c agonists
and pan-PPAR agonists (PPARa ⁄ c ⁄ d) [11]. Multiple
PPAR isotype activators should provide a combination
of the desired metabolic effects of each PPAR isotype
in only one compound. This unique molecule should
be free of side effects, which have so far hampered
successful clinical development of many compounds.
There is a different approach to activate PPARs based
on the concept of selective receptor–cofactor interactions and target gene regulation. Such selective PPAR
modulators (SPPARMs) activate the receptors in distinct ways leading to differential cofactor recruitment
and target gene expression [11]. Dual and pan-PPAR
agonists as well as SPPARMs constitute the new generation of therapeutic agents that should provide more
safety and efficacy.
The PPARs form a heterodimer with the retinoic X
receptor and acquire the capacity to recognize and
bind to specific PPAR-response elements in the promoter region of positive target genes. Moreover,
PPARs transrepress the expression of a number of
inflammatory response genes through interference with
proinflammatory transcription factor pathways such as
activator protein-1 and nuclear factor-kappa B (NFjB). PPAR activity is also determined by PPAR protein expression levels, the abundance and the nature of
their ligands, as well as coactivator and corepressor
availability [12]. Post-translational modifications, such
as phosphorylation and sumoylation of PPARs, and
their association with coactivators and corepressors
also modulate PPAR activity [13, 14].
In this review, we will describe how PPAR transcription factors may modulate different steps of atherosclerosis development and progression focusing on
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 29
M. A. Bouhel et al.
|
their role in macrophage biology. Finally, we will discuss the therapeutical potential of PPAR ligands as
evidenced in clinical trials.
PPARs and monocyte recruitment
The major conditions leading to the transmigration of
circulating monocytes to the neointimal sub-endothelial space is the inflammatory state of ECs and the
presence of OxLDL in the injured vessel [15]. Adhesion molecules and chemoattractant factors released
by EC promote monocyte recruitment. Thus, in the
presence of OxLDL, EC express at their surface selectins, like P-selectin and E-selectin, which promote the
adhesion and the ‘rolling’ of monocytes along the
endothelium [16]. Further, the presence of cytokines
stimulates EC to produce molecules like intercellular
and vascular cell-adhesion molecule-1 (ICAM-1 and
VCAM-1) [17]. EC also produce specific chemoattractant proteins, such as monocyte chemoattractant
protein-1 (MCP-1) that recognizes and binds to the
chemokine receptor (CCR) 2, expressed on monocytes. When MCP-1 interacts with CCR2, this leads
to monocyte recruitment by stimulating their migration to the intima of the arterial wall [18].
Experimental data provide evidences that the three
PPAR isotypes modulate monocyte recruitment and
retention. Indeed, activated PPARa inhibits cytokineinduced expression of ICAM-1 and VCAM-1 in EC
[19, 20] and PPARb ⁄ d activation results in decreased
expression of MCP-1 and ICAM-1 in the aorta of
treated LDL-receptor (LDLR)) ⁄ ) mice, an experimental model of atherosclerosis [21]. PPARc is also
involved in monocyte adhesion and transmigration.
On the one hand, glitazones inhibit the production of
MCP-1 in human EC [22, 23] and, on the other hand,
PPARc inhibits monocyte CCR2 expression and thus
blocks MCP-1-mediated chemotaxis [24, 25]. A study
performed in hyperlipidaemic rabbits indicates that
glitazones have a therapeutic potential for the treatment of vascular complications by suppressing acute
recruitment of monocytes [26].
Interestingly, the existence of crosstalk pathways
between PPARs and other modulators of the
30
Review: PPARs
inflammatory response, such as 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins),
angiotensin-converting enzyme (ACE) inhibitors and
angiotensin type 1 receptor (AT1R) blockers, have
been described with consequences on monocyte
recruitment. Simvastatin has been shown to affect
CCR2 gene expression and CCR2-dependent monocyte recruitment in response to MCP-1 in healthy
men by acting in a PPARc-dependent way [27]. Promoter analysis of CCR2 revealed that the effects of
simvastatin are mediated via PPARc activation. In
line, simvastatin-induced CCR2 repression by PPARc
was completely prevented by the synthetic PPARc
antagonist GW9662. In vivo experiments in hypercholesterolaemic rodents suggest that CCR2 downregulation by simvastatin may be sufficient to inhibit
vascular transmigration of monocytes [27]. In the
same line, Yano and colleagues have shown that inactivation of PPARc using a specific antagonist or
PPARc mRNA silencing, suppresses the inhibitory
effect of statins on LPS-induced TNFa and MCP-1
mRNA expression in mouse peritoneal macrophages
[28]. Statins are also able to activate PPARa and
enhance its transrepression activity by inhibiting the
protein kinase C signalling pathway in mice [29].
This provides evidence that at least part of the acute
anti-inflammatory actions of statins are mediated by
PPARs. Secondly, an unexpected PPAR-mediated
effect of ACE inhibitors has also been reported. ACE
converts angiotensin I to active angiotensin II, which
induces vascular inflammation by upregulating the
expression of the endothelial adhesion molecules
E-selectin, ICAM-1 and VCAM-1, as well as MCP-1
and macrophage-colony-stimulating factor (M-CSF).
Thus, in addition to their blood pressure-lowering
activity, ACE inhibitors have been reported to
decrease atherosclerosis via PPAR-independent pathways [30]. However, it has been shown that the ACE
inhibitor enalapril upregulates PPARa and PPARc
expression in the aorta of treated mice which may
contribute in preventing the angiotensin II-induced
overexpression of adhesion molecules and chemokines
[31]. In addition, Diep and colleagues reported that
the PPARc activators rosiglitazone and pioglitazone
prevent vascular inflammation induced by angiotensin
II in blood vessels of infused rats and could mediate
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
some of the anti-atherogenic effects of ACE inhibitors
[32]. Finally, the AT1R blockers telemisartan and irbesartan have been shown to be selective PPARc
modulators (SPPARM). The active metabolite of the
AT1R blocker losartan, EXP3179, has also been
described as a partial PPARc agonist able to induce
3T3-L1 adipocyte differentiation and to markedly
stimulate PPARc target gene expression [33, 34].
In addition to controlling monocyte recruitment in
early stages of atherogenesis, PPARa and PPARc also
control later steps of atherosclerosis. Upon vascular
injury, SMC migrate from the media to the neointima
where they proliferate and synthesize proteoglycans
thus leading to intima hyperplasia. In this context,
PPARa inhibits SMC proliferation by blocking G1 ⁄ S
cell cycle transition, through the induction of the cyclin-dependent kinase inhibitor p16. This results in
SMC growth inhibition and reduced neointima formation in a mouse model of carotid artery injury [35].
Similarly, PPARc agonists can also decrease both
SMC migration and proliferation [36, 37].
PPARs and macrophage cholesterol homeostasis
In early atherosclerosis, one of the main functions of
monocyte-derived macrophages is to scavenge modified LDL. Monocyte-derived macrophages can captate
infiltrated modified LDL in the intima, because they
express at their surface-specific lipoprotein receptors,
whose expression is not under negative feedback control by cellular cholesterol content, the scavenger
receptors [38]. The major members of the scavenger
receptor family are CD36 [39] and scavenger receptor
A (SR-A) [40, 41]. Macrophage accumulation of lipids, such as cholesterol and triglycerides (TG) originating from lipoproteins, leads to foam cell formation
and drives lipid deposition in atherosclerotic plaques.
The LDL-derived cholesteryl esters are hydrolysed in
the late endosomal ⁄ lysosomal compartment to free
cholesterol (FC). A fraction of FC is either integrated
in the cellular membrane, metabolized to cholesterol
derivatives or esterified by acyl-CoA cholesterol acyltransferase 1 (ACAT1) in the endoplasmic reticulum
[42]. Cholesterol esterification is an essential step in
the storage of unmetabolized cholesterol in lipid droplets. Lipid droplets are structures that function as
depots for neutral lipids-like TG, phospholipids and
sterol esters in the cytoplasm. Besides lipid storage,
macrophages are able to eliminate excess of cholesterol by specific efflux pathways. Effluxed cholesterol
is then carried by high density lipoproteins (HDL) to
the liver to be catabolized. This process is mediated
by specific membrane receptors, such as adenosine triphosphate (ATP)-binding cassette transporter (ABC)
A1, ABCG1, ABCG4 and CD36 and LIMPII-analogous 1 (CLA-1) ⁄ scavenger receptor B1 (SR-B1)
which interact with the principal actors of reverse
cholesterol transport, namely pre-b HDL, HDL and
their major apolipoproteins (apo), apoA-I and apoE
[43]. When lipid uptake and storage are dominant
over lipid efflux, lipid droplets enlarge and macrophages evolve to foam cells.
The modulation of the expression of genes involved
in lipid uptake, metabolism and efflux, might be a
means to prevent atherosclerosis development. Most
studies in the last decade suggest that PPAR activation could provide such regulation. We will present
below different observations implying a role for
PPARa, b ⁄ d and c to prevent foam cell formation.
Lipid uptake
The PPARc is the major actor in adipocyte differentiation by inducing lipid uptake and storage [44]. Hence,
PPARc has been initially presented as an activator of
the genes involved in cholesterol uptake in macrophages such as CD36, thus suggesting a promoting
role of PPARc in foam cell formation [45]. However,
PPARc activation also represses SR-A expression in
macrophages [46]. Moreover, no difference was
observed in term of cholesterol content in macrophages treated with PPARa or PPARc agonists in the presence of acetylated LDL [47]. In addition, activated
PPARa and PPARc are potent suppressors of apoB-48
receptor (apoB-48R) expression in human macrophages and they have been shown to reduce triglyceride
accumulation in macrophages incubated with triglyceride-rich lipoproteins [48]. Interestingly, cholesterol
content is reduced in human macrophages treated with
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 31
M. A. Bouhel et al.
|
PPARa or PPARc activators and incubated in medium
supplemented with glycated LDL (glyLDL), an abundant cholesterol carrier in diabetic patients [49]. Lipoprotein lipase (LPL) is required for the binding and
internalization of glyLDL [50] and through decreasing
LPL secretion and activity, PPARa and PPARc activation results in reduced cholesterol content in human
macrophages [49]. Taken together, these data show
that PPAR activation preferentially lowers lipid uptake
and storage in macrophages.
Intracellular cholesterol trafficking
The mobilization of cholesterol from intracellular
pools to the plasma membrane determines its availability for further storage in lipid droplets or efflux to
extracellular acceptors. Cholesterol trafficking from
the late endosome ⁄ lysosome to the plasma membrane
is a process controlled by a network of proteins that
includes at least two components, namely Niemann
Pick type C 1 and 2 (NPC1 and NPC2) [51, 52].
PPARa activation stimulates the postlysosomal
mobilization of cholesterol by inducing NPC1 and
NPC2 gene and protein expression. This results in an
enrichment of cholesterol in the plasma membrane
and a redistribution of the cholesterol in the external
cell surface domains, where it is more available for
efflux [53].
Cholesterol efflux
Macrophages are able to eliminate the excess of FC
by various mechanisms. PPARa and PPARc activators enhance the expression of the HDL receptor
CLA-1 ⁄ SR-BI [6]. By upregulating the expression of
the transcription factor Liver X Receptor a (LXRa),
PPARa and PPARc indirectly enhance the expression
of the ABCA1 transporter. Indeed, LXR induces
ABCA1 gene expression and thus promotes apoA-Imediated cholesterol efflux from macrophages [47,
54]. Expression of a second member of the ABC
transporter family, the ABC transporter G1
(ABCG1), is also induced by PPARc activation but
in an LXR-independent manner [55]. As a consequence, PPARa and PPARc clearly enhance the
apoA-I- and HDL-dependent cholesterol efflux in
32
Review: PPARs
macrophages [47, 55, 56]. PPARc is also able to
stimulate mobilization of cellular membrane cholesterol by activating caveolin-1 expression [57].
Because of its ability to bind cholesterol, caveolin-1
has been implicated in the regulation of cellular cholesterol metabolism in several cell types. Caveolin-1
is thought to stimulate cholesterol association with
lipid rafts, thus promoting its efflux in macrophages
[58]. Cholesterol oxidation products formed by the
action of cytochrome P450 enzymes are also
involved in cholesterol homeostasis. Cytochrome
P450, family 27 (CYP27) is a mitochondrial enzyme
that initiates the alternative bile acid synthesis pathway [59]. In human macrophages, CYP27 subfamily
A polypeptide 1 (CYP27A1) increases 27-hydroxycholesterol levels. The mRNA expression level and
the activity of CYP27A1 are both upregulated by
PPARc in human macrophages [60]. These data illustrate the major role of PPAR activators in the maintenance of macrophage cholesterol homeostasis.
The effects of PPARb ⁄ d in macrophage lipid metabolism remain controversial and particularly its function
in the efflux of cholesterol is not completely elucidated. Indeed, PPARb ⁄ d activation by the synthetic
agonist GW501615 has been shown to promote
apoA-I-specific cholesterol efflux and to induce
ABCA1 gene expression in THP-1 macrophages, suggesting an enhancement of reverse cholesterol transport [61]. In line with these observations, PPARb ⁄ d
activation in mice results in increased plasma HDL,
promoting reverse cholesterol transport from peripheral tissues to the liver [62]. Opposing to these data,
PPARb ⁄ d activation represses key genes involved in
lipid metabolism and efflux, such as CYP27A1 and
apoE and increases the expression of genes involved
in lipid uptake and storage like SR-A, CD36 and
adipophilin, observations obtained using THP-1 macrophages overexpressing PPARb ⁄ d [63]. Moreover,
recent data suggest a potential implication of
PPARb ⁄ d in the clearance of lipids by macrophages.
The activation of PPARb ⁄ d by VLDL-derived fatty
acids promotes mitochondrial b-oxidation, peroxisomal fatty acid oxidation and carnitine biosynthesis
thus resulting in increased fatty acid catabolism in
macrophages [8].
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
Cholesterol esterification and lipid storage
Cholesterol excess is directed to the endoplasmic reticulum where it is esterified by ACAT1 and stored as
lipid droplets. PPARa inhibits ACAT1 and enhances
cholesteryl ester hydrolase mRNA expression, thus
preventing cholesteryl ester accumulation in primary
human macrophages and thus foam cell formation
[64]. Similarly, an effect of PPARc ligands in the
reduction of cholesteryl ester accumulation in THP1macrophages has also been reported [65]. The availability of fatty acids in macrophages also contributes
to the efficiency of cholesterol accumulation. The activation of mitochondrial fatty acid b-oxidation could be
a way to reduce the level of free fatty acids in macrophages and thus to control the cholesterol esterification
rate. In primary human monocyte-derived macrophages different synthetic PPARa activators significantly
induced the gene expression of carnitine palmitoyltransferase 1 (CPT1), a key enzyme in mitochondrial
fatty acid beta-oxidation. The induction of CPT1 by
PPARa activation correlated with a reduction of cholesteryl ester levels. These observations provide one
mechanism by which PPARa controls cholesteryl ester
accumulation [64]. The lipid droplet-coating protein
adipophilin increases TG storage in human macrophages by stimulating their biosynthesis and inhibiting their
beta-oxidation and prevents lipid efflux from THP-1
macrophages [66, 67]. PPARb ⁄ d overexpression has
been reported to induce adipophilin expression [63].
PPARs and macrophage inflammation
Inflammation of the ECs is one of the primary events
in atherosclerotic plaque formation and leads to the
recruitment of monocytes to the neointima. Inflammatory activated monocyte-differentiated macrophages
release proinflammatory cytokines and chemoattractant molecules in the sub-endothelial space. Proinflammatory molecules, such as TNFa, IL-6, IL-12 or
IL-1b, are known to promote EC inflammation,
monocyte differentiation into macrophages and SMC
proliferation [68, 69].
The PPARs exert acute anti-inflammatory activities
via multiple molecular mechanisms. Transrepression
is a mechanism of negative interference of activated
PPARs with proinflammatory signalling pathways,
such as NF-jB and AP1 [70], thus inhibiting the
expression of proinflammatory genes, like VCAM1,
MMP9, TNFa or IL-6 [71, 72]. A recently identified
transrepression mechanism involves sumoylation of
the liganded-PPARc ligand-binding domain. This
SUMO–PPARc complex retains the corepressor complex NcoR ⁄ HDAC3 on promoter NF-jB sites, thus
preventing inflammatory gene activation by NF-jB in
macrophages [13, 73].
On the other hand, PPARc can also exert anti-inflammatory effects by inducing the expression of antiinflammatory genes, such as the IL-1 receptor
antagonist (IL-1Ra) [71, 72].
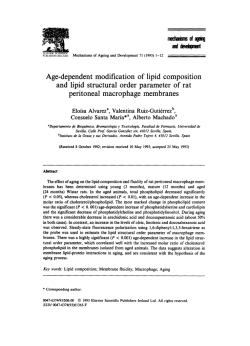
However, alternative pathways of inflammation control have been described recently. PPARc enhances
the alternative activation and differentiation of macrophages [74, 75]. Such alternatively differentiated
macrophages display a more pronounced anti-inflammatory phenotype (Fig. 1) [75]. IL-4, an anti-inflammatory cytokine and an activator of alternative
differentiation of macrophages in vitro, also stimulates
cellular generation of natural PPARc ligands by the
activation of the 12 ⁄ 15-lipoxygenase pathway in
macrophages thus enhancing the inhibition of iNOS
expression [76].
The PPARa activation also inhibits various proinflammatory molecules. Shu et al. have shown that PPARa
activation represses MMP9 gene expression in macrophages [77] and inhibits osteopontin expression, a
proinflammatory cytokine implicated in the chemoattraction of monocytes [78]. Moreover, PPARa activation inhibits LPS-induced expression and activity of
tissue factor in monocytes, a factor involved in thrombus formation [79, 80]. In mice, PPARa deficiency
provokes a chronic inflammatory response providing
genetic evidence for the anti-inflammatory activity of
this transcription factor [81]. In addition, PPARa
induces reactive oxygen species (ROS) in resting
human and murine macrophages. The ROS production
occurs via the NADPH oxidase pathway and leads to
a modification of LDL, which in turn act as PPARa
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 33
M. A. Bouhel et al.
|
Review: PPARs
M1 Macrophage
Classically activated macrophage
+ Pro-inflammatory cytokines production
+ Antigen presentation & microbicidal activity
IFN-γ, LPS
+ Expression of MHC class II molecules
Monocyte
Alternatively activated macrophage
IL-4, IL-13
+ Anti-inflammatory molecules production
+ Cell growth and tissue repair
Activated
PPARγ
M2 Macrophage
ligands to inhibit the induction of inflammatory
response genes, such as iNOS, in macrophages [82].
PPARb ⁄ d also modulates the inflammatory response
in macrophages by repressing subsets of LPS and
IFN-c target genes, including iNOS and COX2 [83].
However, Lee et al. reported that peritoneal macrophages from male LDLR) ⁄ ) mice transplanted with
PPARb ⁄ d-deficient bone marrow exhibit decreased
production of inflammatory mediators, including
MCP-1, IL-1b and MMP9, suggesting a proinflammatory role for PPARb ⁄ d [84]. Interestingly, pharmacological activation of PPARb ⁄ d by the GW501516
ligand inhibited the inflammatory response in the
same mice [84]. Other studies support the anti-inflammatory role of PPARb ⁄ d activation. Indeed, Li et al.
also demonstrated that PPARb ⁄ d agonist treatment of
LDLR) ⁄ ) mice decreased inflammatory cytokine
expression in atherosclerotic lesions [56]. Moreover,
PPARb ⁄ d activation by the agonist GW0742X has
been shown to decrease TNFa expression in peritoneal macrophages as well as the circulating serum
levels of proinflammatory proteins MCP-1, RANTES,
IL-12 and soluble TNFR1 in female LDLR) ⁄ ) mice
[21]. All together, these findings suggest an antiinflammatory function of activated PPARb ⁄ d in macrophages.
Biological marker modulation by PPAR agonists
Clinical trials using fibrates (fenofibrate, bezafibrate or
gemfibrozil) and glitazones (rosiglitazone or pioglitaz34
Fig. 1 Pathways of classical
and alternative macrophage
differentiation from monocytes.
+ Endocytic activity
one) also provide indications regarding the clinical
efficacy of PPAR agonists in the control of lipid and
glucose metabolism and inflammation. One means to
assess this activity is by measuring biomedical and
imaging markers of cardiovascular diseases (CVD).
Biochemical markers
Fenofibrate administration lowers the plasma levels of
inflammatory biomarkers, such as IL-6, fibrinogen
and C-reactive proteins (CRP) in patients with established atherosclerosis [85, 86] and significantly
reduces plasma levels of IFNc, TNFa, ICAM-1,
MCP-1, a2-macroglobulin and plasminogen in
patients with hyperlipoproteinaemia [86, 87]. In addition, in patients with impaired glucose tolerance,
1-month fenofibrate treatment reduced the plasma
concentrations of plasminogen activator inhibitor-1,
fibrinogen, factor VII as well as the circulating levels
of oxidized LDL [88]. Similar effects were observed
in hypertriglyceridaemic patients after bezafibrate
administration [89] and in obese patients with atherogenic dyslipidaemia after gemfibrozil treatment [90].
As fibrates, glitazones also modulate the expression of
cardiovascular biomarkers. In type 2 diabetes patients,
rosiglitazone administration rapidly reduces the levels
of inflammatory biomarkers, such as CRP, MMP-9,
SAA, sCD40L, MCP-1 or TNFa [91]. This effect
occurs 6 weeks earlier than the maximal glucose-lowering effect of rosiglitazone suggesting that glitazones
might directly affect these biomarkers independently
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
of their metabolic action [92]. In line with this
hypothesis, results from a study with rosiglitazone in
nondiabetic patients with symptomatic carotid artery
stenosis showed reduced CRP and SAA serum levels
associated with an increased atherosclerotic plaque
collagen content and a reduction of the expression of
MMP-3, MMP-8 and MMP-9 in the plaque [93].
Thus, short-term rosiglitazone treatment significantly
reduces vascular inflammation in nondiabetic subjects,
leading to a more stable type of atherosclerotic lesion.
Glitazone treatments also result in a significant reduction of endothelial dysfunction markers, such as endothelin-1, von Willebrand factor, PAI-1, adhesion
molecules (VCAM, ICAM and P-selectin) and circulating platelet activity [94–96]. A decreased number
or function of endothelial progenitor cell (EPC) also
leads to endothelial dysfunction. The beneficial effects
of glitazones on the endothelium may also be mediated by an increase in the number of circulating EPCs
and an improvement of their migratory response and
their adhesive capacity [97, 98].
Imaging markers
Fibrates and glitazones also influence surrogate markers of CVD, assessed by imaging technologies including coronary angiography or intravascular ultrasound
(IVUS), which allow the measurement of coronary
atherosclerosis and carotid intima ⁄ media thickness
(CIMT).
A decreased atherosclerosis progression was observed
upon treatment with gemfibrozil in the Lopid Coronary Angiography Trial, with bezafibrate in the Bezafibrate Coronary Atherosclerosis Intervention Trial and
with fenofibrate in the Diabetes Atherosclerosis Intervention Study [99–101].
In two recent studies in nondiabetic patients, pioglitazone treatment significantly reduced neointimal
hyperplasia, evaluated using IVUS, after coronary
stent implantation [102, 103]. In the CHICAGO (Carotid Intima-Media Thickness in Atherosclerosis using
Pioglitazone) trial enrolling type 2 diabetic patients
treated for 72 weeks, CIMT was reduced in the
pioglitazone when compared to the glimepiride group
(glimpepiride is a sulphonylurea used as an antihyperglycaemic agent for the therapy of type 2 diabetes mellitus) [104, 105]. Langenfeld and colleagues
reported similar results after a shorter treatment period
with pioglitazone (24 weeks) [105]. However, 12month rosiglitazone treatment in obese patients undergoing percutaneous coronary intervention did not
affect CIMT, although CRP levels were reduced
[106].
Cardiovascular outcome studies with PPAR agonists
The influence of fibrates on cardiovascular morbidity
and mortality was studied in primary (Helsinki Heart
Study [107] and Fenofibrate Intervention and Event
Lowering in Diabetes (FIELD) [108]) and secondary
[Bezafibrate Infarction Prevention [109], Veterans
Affairs High-density Lipoprotein Cholesterol Intervention trial [110] and FIELD [108]] cardiovascular prevention studies (Table 1). The results from these trials
suggest that fibrate therapy reduces coronary heart
disease (CHD) and is most efficacious in overweight
individuals with insulin resistance and chronic inflammation.
The most recent results come from the FIELD study
[108], which is a 5-year combined primary and secondary prevention study testing the effects of fenofibrate on CHD in 9795 patients with Type 2 diabetes.
The results of FIELD were somewhat unexpected.
After 5 years, fenofibrate reduced the primary combined end-point of nonfatal myocardial infarction
(MI) and CHD death by 11% compared to placebo,
an effect that was not significant (Table 1). Interestingly, the secondary end-point (MI, stroke, CVD
death, coronary and carotid revascularization) was significantly reduced by 11%. The observed benefit of
fenofibrate treatment was essentially due to fewer
nonfatal MI and coronary revascularizations. Moreover, fenofibrate treatment provides protective effects
on microvascular and peripheral vascular disease by
reducing the risk of nephropathy (measured as albumin excretion rate) by 15%, retinopathy needing laser
therapy by 30% and nontraumatic amputation by 38%
[108].
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 35
M. A. Bouhel et al.
|
Review: PPARs
Table 1 Peroxisome proliferator-activated receptor (PPAR)a and PPARc agonists in cardiovascular outcome trials
Absolute CVD risk
Clinical trial
Compound
Duration (years)
N
Gemfibrozil
5
4081
4.1
Control (%)
Drug (%)
Rel. RR (%)
P-value
Primary prevention
HHS
2.73
34
0.02
Secondary prevention
BIP
Bezafibrate
6
3090
15.0
13.6
VA-HIT
Gemfibrozil
5
2531
21.7
17.3
22
9.4
0.26
0.006
PROactive*
Pioglitazone
3
5238
23.5
21.0
10
0.095
11
Primary and secondary prevention
FIELD
9795
6.0
5.0
Primary prevention subgroup
Fenofibrate
5
7664
10.8
8.9
<0.001
0.16
Secondary prevention subgroup
2131
25.1
25.5
0.85
CVD, cardiovascular disease; N, number of patients; Rel. RR, relative risk reduction; HHS, Helsinki Heart Study; BIP, Bezafibrate Infarction
Prevention; FIELD, Fenofibrate Intervention and Event Lowering in Diabetes; PROactive, PROspective pioglitazone Clinical Trial in macroVascular Events; VA-HIT, Veterans Affairs High-density Lipoprotein Cholesterol Intervention trial.
*The PROactive principal secondary end-point (cardiovascular end-points of all-cause mortality, nonfatal MI and stroke) was significantly
(P = 0.027) reduced with a relative risk reduction of 16%.
During the course of the study, 17% of the placebo
and 8% of the fenofibrate group were initiated on statin therapy.
and the currently used glitazones may even be hepatoprotective against fatty liver disease and potentially
nonalcoholic steatohepatitis [114].
As statins decrease CVD in type 2 diabetic patients
[111], the actual benefit of fenofibrate may thus be
underestimated due to the higher use of statins in the
placebo group. The efficacy of fenofibrate, on top of
simvastatin therapy, will be addressed in the ongoing
Action to Control Cardiovascular Risk in Diabetes
study expected to terminate in 2 years. In this trial,
unlike in the FIELD study, fenofibrate is not being
used as monotherapy but only in combination with
simvastatin and compared to simvastatin monotherapy.
This design should largely avoid the problem of offtrial drug use encountered in FIELD and should thus
reveal the usefulness of fenofibrate as a specific
adjunct to statin therapy in the treatment of diabetic
dyslipidaemia and CVD.
The PROspective pioglitazone Clinical Trial in macroVascular Events (PROactive) [115] evaluated the
influence of pioglitazone on CVD in 5238 patients
with type 2 diabetes and prior macrovascular disease,
on top of current diabetes and cardiovascular medication. Although the primary end-point was not reached,
the principal secondary end-point composed of the
cardiovascular end-points of all-cause mortality, nonfatal MI and stroke was significantly reduced (16%
risk reduction; Table 1). Further post hoc analysis
showed that pioglitazone significantly lowered the risk
of recurrent fatal and nonfatal stroke in patients with
previous stroke but had no effect on subsequent
strokes in patients without prior stroke [116] as well
as recurrent MI and acute coronary syndrome in
patients with prior MI [117].
Glitazones were demonstrated to be efficient in the
management of insulin resistance and type 2 diabetes
in a number of prospective clinical trials [112, 113].
Although troglitazone was withdrawn, because of a
rare, but severe idiosyncratic hepatotoxicity, glitazones
are increasingly prescribed to patients with diabetes
36
Safety issues of PPAR activators
Fibrates are generally considered as safe drugs with
only few side effects [108]. However, a moderate
and reversible increase in plasma creatinine and
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
homocysteine levels in humans is a common side
effect of fibrates [118]. Novel generation, highly
active PPARa agonists, should also be monitored for
myopathy induction [118].
Glitazone administration is associated with a number
of adverse effects that have been categorized as
either unique to individual glitazones or common to
the class. For instance, hepatotoxicity is a side effect
specifically associated with troglitazone treatment
[119]. Class side effects include body weight gain
(because of an increase in adipose tissue and body
fluid expansion), haemodilution (decrease in haematocrit, red blood cell count and plasma haemoglobin),
peripheral oedema, which may precipitate congestive
heart failure, and increased risk of bone fractures
[120–122]. Hence, glitazone medication should be
avoided in patients with heart failure. However,
recent insights suggest that glitazones may be used
safely in individuals with stable heart failure. In an
ambulatory cohort of patients with established heart
failure and diabetes, glitazone use was not associated
with an increased risk of heart failure hospitalization
or death when compared with those not receiving
insulin-sensitizing medications [123]. Moreover, a
recent meta-analysis confirmed that glitazone treatment does not increase cardiovascular death,
although it increases the risk for congestive heart
failure (+72%) [124].
Recently, three independent studies reported results
from a meta-analysis suggesting that rosiglitazone
use may be associated with an increase in the risk of
MI from cardiovascular causes [125, 126]. This study
raises questions on the cardiovascular safety of rosiglitazone in the treatment of type 2 diabetes. However,
the increase in absolute cardiovascular risk after rosiglitazone treatment was very small in these studies
on low-risk patients, such as DREAM and ADOPT
[112, 113]. Intermediary safety analysis of a trial
assessing the cardiovascular effects of rosiglitazone
combined with metformin or sulfonylurea, the Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of Glycemia in Diabetes (RECORD) study,
reported nonsignificant changes in cardiovascular
morbidity and mortality after rosiglitazone treatment
[127]. These reports should be interpreted with caution and only the final outcome from the RECORD
study will provide evidences on the long-term cardiovascular effects of rosiglitazone in patients with type
2 diabetes. Meantime, it remains puzzling why rosiglitazone, in contrast to pioglitazone, does not
decrease the risk of CVD. Indeed, results from a
meta-analysis on the risk of cardiovascular events
after treatment with pioglitazone indicated that pioglitazone lowers the risk of death, MI or stroke in
patients with diabetes, whereas, as expected, the risk
of heart failure increases [128].
As a strategy to avoid glitazone side effects, research
should be focused on the elucidation of the mechanisms responsible for these adverse effects in T2D
patients to predict susceptibility and subsequently to
identify and exclude sensitive patients from glitazonebased medication.
Conclusions
Important progresses have been made in the understanding of the control of macrophage functions by
PPARs during the last years. Presently, a growing
body of evidence from in vitro and in vivo studies in
animals and, more importantly, in humans, indicates
that PPAR agonists have beneficial effects in the control of macrophage lipid metabolism and inflammatory status which may impact on atherosclerosis
development. Based on these findings the identification of novel molecules targeting these nuclear receptors provides exciting opportunities to reduce
atherosclerosis and its cardiovascular complications.
One strategy is to develop partial agonists of PPARc
with reduced side effects with selective PPAR modulator (SPPARM) activity [11]. We expect that future
treatment will be based on dual and pan SPPARM agonists with the aim to obtain the best benefit from the
activation of each PPAR isotype with fewer side
effects [11].
Conflict of interest statement
Bart Staels received speakers honorarium from Takeda, GSK and Solvay Pharma.
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 37
M. A. Bouhel et al.
|
Review: PPARs
Acknowledgements
We acknowledge grants from the Re´gion Nord-Pas de
Calais ⁄ FEDER, the Fondation Coeur et Arte`res and
the European Vascular Genomics Network. M.A.
Bouhlel is recipient of an unrestricted PhD thesis
grant from the Nouvelle Socie´te´ Franc¸aise d’Athe´roscle´rose ⁄ Sanofi-Aventis.
References
1 Lusis AJ. Atherosclerosis Nature (London) 2000; 407: 233–41.
2 Saxena U, Goldberg IJ. Endothelial cells and atherosclerosis:
lipoprotein metabolism, matrix interactions, and monocyte
recruitment. Curr Opin Lipidol 1994; 5: 316–22.
3 Nilsson J. Cytokines and smooth muscle cells in atherosclerosis. Cardiovasc Res 1993; 27: 1184–90.
4 Linton MF, Fazio S. Macrophages, inflammation, and atherosclerosis. Int J Obes Relat Metab Disord 2003; 27(Suppl. 3):
S35–40.
5 Katsuda S, Kaji T. Atherosclerosis and extracellular matrix.
J Atheroscler Thromb 2003; 10: 267–74.
6 Chinetti G, Gbaguidi GF, Griglio S et al. CLA-1 ⁄ SR-BI is
expressed in atherosclerotic lesion macrophages and regulated
by activators of peroxisome proliferator-activated receptors.
Circulation 2000; 101: 2411–7.
7 Duval C, Chinetti G, Trottein F, Fruchart JC, Staels B. The
role of PPARs in atherosclerosis. Trends Mol Med 2002; 8:
422–30.
8 Lee CH, Kang K, Mehl IR et al. Peroxisome proliferator-activated receptor delta promotes very low-density lipoproteinderived fatty acid catabolism in the macrophage. Proc Natl
Acad Sci U S A 2006; 103: 2434–9.
9 Lee CH, Olson P, Hevener A et al. PPARdelta regulates glucose metabolism and insulin sensitivity. Proc Natl Acad Sci U
S A 2006; 103: 3444–9.
10 Staels B, Fruchart JC. Therapeutic roles of peroxisome proliferator-activated receptor agonists. Diabetes 2005; 54: 2460–70.
11 Pourcet B, Fruchart JC, Staels B, Glineur C. Selective PPAR
modulators, dual and pan PPAR agonists: multimodal drugs
for the treatment of type 2 diabetes and atherosclerosis. Expert
Opin Emerg Drugs 2006; 11: 379–401.
12 Perissi V, Staszewski LM, McInerney EM et al. Molecular
determinants of nuclear receptor-corepressor interaction. Genes
Dev 1999; 13: 3198–208.
13 Pascual G, Fong AL, Ogawa S et al. A SUMOylation-dependent pathway mediates transrepression of inflammatory
response genes by PPAR-gamma. Nature (London) 2005; 437:
759–63.
14 Diradourian C, Girard J, Pegorier JP. Phosphorylation of
PPARs: from molecular characterization to physiological relevance. Biochimie 2005; 87: 33–8.
15 Han KH, Tangirala RK, Green SR, Quehenberger O. Chemokine receptor CCR2 expression and monocyte chemoattractant
38
16
17
18
19
20
21
22
23
24
25
26
27
28
29
protein-1-mediated chemotaxis in human monocytes. A regulatory role for plasma LDL. Arterioscler Thromb Vasc Biol
1998; 18: 1983–91.
Dong ZM, Brown AA, Wagner DD. Prominent role of P-selectin in the development of advanced atherosclerosis in ApoEdeficient mice. Circulation 2000; 101: 2290–5.
Albelda SM, Smith CW, Ward PA. Adhesion molecules and
inflammatory injury. FASEB J 1994; 8: 504–12.
Gerszten RE, Garcia-Zepeda EA, Lim YC et al. MCP-1 and IL8 trigger firm adhesion of monocytes to vascular endothelium
under flow conditions. Nature (London) 1999; 398: 718–23.
Marx N, Sukhova G, Collins T, Libby P, Plutzky J. PPARa
activators inhibit cytokine-induced vascular cell adhesion molecule-1 expression in human endothelial cells. Circulation
1999; 99: 3125–31.
Xu X, Otsuki M, Saito H et al. PPARalpha and GR differentially down-regulate the expression of nuclear factor-kappaBresponsive genes in vascular endothelial cells. Endocrinology
2001; 142: 3332–9.
Graham TL, Mookherjee C, Suckling KE, Palmer CN, Patel L.
The PPARdelta agonist GW0742X reduces atherosclerosis in
LDLR(- ⁄ -) mice. Atherosclerosis 2005; 181: 29–37.
Lee H, Shi W, Tontonoz P et al. Role of peroxisome proliferator-activated receptor alpha in oxidized phospholipid-induced
synthesis of monocyte chemotactic protein-1 and interleukin-8
by endothelial cells. Circ Res 2000; 87: 516–21.
Murao K, Imachi H, Momoi A et al. Thiazolidinediones inhibit the production of monocyte chemoattractant protein-1 in
cytokine-treated human vascular endothelial cells. FEBS Lett
1999; 454: 27–30.
Han KH, Chang MK, Boullier A et al. Oxidized LDL reduces
monocyte CCR2 expression through pathways involving peroxisome proliferator-activated receptor c. J Clin Invest 2000;
106: 793–802.
Chen Y, Green SR, Ho J, Li A, Almazan F, Quehenberger O.
The mouse CCR2 gene is regulated by two promoters that are
responsive to plasma cholesterol and peroxisome proliferatoractivated receptor gamma ligands. Biochem Biophys Res Commun 2005; 332: 188–93.
Tanaka T, Fukunaga Y, Itoh H et al. Therapeutic potential of
thiazolidinediones in activation of peroxisome proliferator-activated receptor gamma for monocyte recruitment and endothelial regeneration. Eur J Pharmacol 2005; 508: 255–65.
Han KH, Ryu J, Hong KH et al. HMG-CoA reductase inhibition reduces monocyte CC chemokine receptor 2 expression
and monocyte chemoattractant protein-1-mediated monocyte
recruitment in vivo. Circulation 2005; 111: 1439–47.
Yano M, Matsumura T, Senokuchi T et al. Statins activate peroxisome proliferator-activated receptor gamma through extracellular signal-regulated kinase 1 ⁄ 2 and p38 mitogen-activated
protein kinase-dependent cyclooxygenase-2 expression in macrophages. Circ Res 2007; 100: 1442–51.
Paumelle R, Blanquart C, Briand O et al. Acute antiinflammatory properties of statins involve peroxisome proliferator-activated receptor-alpha via inhibition of the protein kinase C
signaling pathway. Circ Res 2006; 98: 361–9.
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
30 Scholkens BA, Landgraf W. ACE inhibition and atherogenesis.
Can J Physiol Pharmacol 2002; 80: 354–9.
31 da Cunha V, Tham DM, Martin-McNulty B et al. Enalapril
attenuates angiotensin II-induced atherosclerosis and vascular
inflammation. Atherosclerosis 2005; 178: 9–17.
32 Diep QN, El Mabrouk M, Cohn JS et al. Structure, endothelial
function, cell growth, and inflammation in blood vessels of
angiotensin II-infused rats: role of peroxisome proliferator-activated receptor-gamma. Circulation 2002; 105: 2296–302.
33 Schupp M, Lee LD, Frost N et al. Regulation of peroxisome
proliferator-activated receptor gamma activity by losartan
metabolites. Hypertension 2006; 47: 586–9.
34 Schupp M, Clemenz M, Gineste R et al. Molecular characterization of new selective peroxisome proliferator-activated
receptor gamma modulators with angiotensin receptor blocking
activity. Diabetes 2005; 54: 3442–52.
35 Gizard F, Amant C, Barbier O et al. PPAR alpha inhibits vascular smooth muscle cell proliferation underlying intimal
hyperplasia by inducing the tumor suppressor p16INK4a.
J Clin Invest 2005; 115: 3228–38.
36 Miwa Y, Sasaguri T, Inoue H, Taba Y, Ishida A, Abumiya T.
15-Deoxy-Delta(12,14)-prostaglandin J(2) induces G(1) arrest
and differentiation marker expression in vascular smooth muscle cells. Mol Pharmacol 2000; 58: 837–44.
37 Gouni-Berthold I, Berthold HK, Weber AA, Seul C, Vetter H,
Sachinidis A. Troglitazone and rosiglitazone inhibit the low
density lipoprotein-induced vascular smooth muscle cell
growth. Exp Clin Endocrinol Diabetes 2001; 109: 203–9.
38 de Villiers WJ, Smart EJ. Macrophage scavenger receptors and
foam cell formation. J Leukoc Biol 1999; 66: 740–6.
39 Yamashita S, Hirano KI, Kuwasako T et al. Physiological and
pathological roles of a multi-ligand receptor CD36 in atherogenesis; insights from CD36-deficient patients. Mol Cell Biochem 2007; 299: 19–22.
40 Gough PJ, Greaves DR, Suzuki H et al. Analysis of macrophage scavenger receptor (SR-A) expression in human aortic
atherosclerotic lesions. Arterioscler Throm Vasc Biol 1999; 19:
461–71.
41 Herijgers N, de Winther MP, Van Eck M et al. Effect of
human scavenger receptor class A overexpression in bone marrow-derived cells on lipoprotein metabolism and atherosclerosis in low density lipoprotein receptor knockout mice. J Lipid
Res 2000; 41: 1402–9.
42 Chang TY, Chang CC, Lin S, Yu C, Li BL, Miyazaki A. Roles
of acyl-coenzyme A:cholesterol acyltransferase-1 and )2. Curr
Opin Lipidol 2001; 12: 289–96.
43 Jessup W, Gelissen IC, Gaus K, Kritharides L. Roles of ATP
binding cassette transporters A1 and G1, scavenger receptor
BI and membrane lipid domains in cholesterol export from
macrophages. Curr Opin Lipidol 2006; 17: 247–57.
44 Tontonoz P, Hu E, spiegelman BM. Stimulation of adipogenesis in fibroblast by PPARc2, a lipid-activated transcription
factor. Cell 1994; 79: 1147–56.
45 Nagy L, Tontonoz P, Alvarez JGA, Chen H, Evans RM. Oxidized LDL regulates macrophage gene expression through
ligand activation of PPARc. Cell 1998; 93: 229–40.
46 Moore KJ, Rosen ED, Fitzgerald ML et al. The role of PPARgamma in macrophage differentiation and cholesterol uptake.
Nat Med 2001; 7: 41–7.
47 Chinetti G, Lestavel S, Bocher V et al. PPARa and PPARc
activators induce cholesterol removal from human macrophage
foam cells through stimulation of the ABCA1 pathway. Nat
Med 2001; 7: 53–8.
48 Haraguchi G, Kobayashi Y, Brown ML et al. PPARalpha and
PPARgamma activators suppress the monocyte-macrophage
apolipoprotein B48 receptor. J Lipid Res 2003; 44: 1224–31.
49 Gbaguidi GF, Chinetti G, Milosavljevic D et al. Peroxisome
proliferator-activated receptor (PPAR) agonists decrese lipoprotein lipase secretion and glycated LDL uptake by human macrophages. FEBS Lett 2002; 512: 85–90.
50 Zimmermann R, Panzenbo¨ck U, Wintersperger A et al. Lipoprotein lipase mediates the uptake of glycated low density
lipoprotein in fibroblasts, endothelial cells, and macrophages.
Diabetes 2001; 50: 1643–53.
51 Garver WS, Heidenreich RA. The Niemann-Pick C proteins
and trafficking of cholesterol through the late endosomal ⁄ lysosomal system. Curr Mol Med 2002; 2: 485–505.
52 Watari H, Blanchette-Mackie EJ, Dwyer NK et al. NiemannPick C1 protein: obligatory roles for N-terminal domains and
lysosomal targeting in cholesterol mobilization. Proc Natl
Acad Sci U S A 1999; 96: 805–10.
53 Chinetti-Gbaguidi G, Rigamonti E, Helin L et al. Peroxisome
proliferator-activated receptor {alpha} controls cellular cholesterol trafficking in macrophages. J Lipid Res 2005; 46: 2717–25.
54 Chawla A, Boisver WA, Lee CH et al. A PPAR gamma-LXRABCA1 pathway in macrophages is involved in cholesterol
efflux and atherogenesis. Mol Cell 2001; 7: 161–71.
55 Akiyama TE, Sakai S, Lambert G et al. Conditional disruption
of the peroxisome proliferator-activated receptor gamma gene
in mice results in lowered expression of ABCA1, ABCG1,
and apoE in macrophages and reduced cholesterol efflux. Mol
Cell Biol 2002; 22: 2607–19.
56 Li AC, Binder CJ, Gutierrez A et al. Differential inhibition of
macrophage foam-cell formation and atherosclerosis in mice
by PPARalpha, beta ⁄ delta, and gamma. J Clin Invest 2004;
114: 1564–76.
57 Llaverias G, Vazquez-Carrera M, Sanchez RM et al. Rosiglitazone upregulates caveolin-1 expression in THP-1 cells
through a PPAR-dependent mechanism. J Lipid Res 2004; 45:
2015–24.
58 Gargalovic P, Dory L. Caveolins and macrophage lipid metabolism. J Lipid Res 2003; 44: 11–21.
59 Cali JJ, Russell DW. Characterization of human sterol 27hydroxylase. A mitochondrial cytochrome P-450 that catalyzes
multiple oxidation reaction in bile acid biosynthesis. J Biol
Chem 1991; 266: 7774–8.
60 Quinn CM, Jessup W, Wong J, Kritharides L, Brown AJ.
Expression and regulation of sterol 27-hydroxylase
(CYP27A1) in human macrophages: a role for RXR and
PPARgamma ligands. Biochem J 2005; 385: 823–30.
61 Oliver WRJ, Shenk JL, Snaith MR et al. A selective peroxisome proliferator-activated receptor delta agonist promotes
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 39
M. A. Bouhel et al.
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
40
|
reverse cholesterol transport. Proc Natl Acad Sci U S A 2001;
98: 5306–11.
van der Veen JN, Kruit JK, Havinga R et al. Reduced cholesterol absorption upon PPARdelta activation coincides with
decreased intestinal expression of NPC1L1. J Lipid Res 2005;
46: 526–34.
Vosper H, Patel L, Graham TL et al. The peroxisome proliferator-activated receptor promotes lipid accumulation in human
macrophages. J Biol Chem 2001; 276: 44258–65.
Chinetti G, Lestavel S, Fruchart JC, Clavey V, Staels B. Peroxisome proliferator-activated receptor alpha reduces cholesterol esterification in macrophages. Circ Res 2003; 92: 212–7.
Argmann CA, Sawyez CG, McNeil CJ, Hegele RA, Huff MW.
Activation of peroxisome proliferator-activated receptor
gamma and retinoid x receptor results in net depletion of cellular cholesteryl esters in macrophages exposed to oxidized lipoproteins. Arterioscler Throm Vasc Biol 2003; 23: 475–82.
Larigauderie G, Cuaz-Perolin C, Younes AB et al. Adipophilin
increases triglyceride storage in human macrophages by stimulation of biosynthesis and inhibition of beta-oxidation. FEBS J
2006; 273: 3498–510.
Larigauderie G, Furman C, Jaye M et al. Adipophilin
enhances lipid accumulation and prevents lipid efflux from
THP-1 macrophages: potential role in atherogenesis. Arterioscler Thromb Vasc Biol 2004; 24: 504–10.
Chomarat P, Banchereau J, Davoust J, Palucka AK. IL-6
switches the differentiation of monocytes from dendritic cells
to macrophages. Nat Immunol 2000; 1: 510–4.
Peppel K, Zhang L, Orman ES et al. Activation of vascular
smooth muscle cells by TNF and PDGF: overlapping and
complementary signal transduction mechanisms. Cardiovasc
Res 2005; 65: 674–82.
Delerive P, Fruchart JC, Staels B. Peroxisome proliferator-activated receptors in inflammation control. J Endocrinol 2001;
169: 453–9.
Marx N, Duez H, Fruchart JC, Staels B. Peroxisome proliferator-activated receptors and atherogenesis: regulators of gene
expression in vascular cells. Circ Res 2004; 94: 1168–78.
Meier C, Chicheportiche R, Juge-Aubry C, Dreyer M, Dayer
J. Regulation of the interleukin-1 receptor antagonist in THP-1
cells by ligands of the peroxisome proliferator-activated receptor gamma. Cytokines 2002; 18: 320–8.
Ohshima T, Koga H, Shimotohno K. Transcriptional activity of
peroxisome proliferator-activated receptor gamma is modulated
by SUMO-1 modification. J Biol Chem 2004; 279: 29551–7.
Odegaard JI, Ricardo-Gonzalez RR, Goforth MH et al. Macrophage-specific PPARgamma controls alternative activation and
improves insulin resistance. Nature (London) 2007; 447:
1116–20.
Bouhlel MA, Derudas B, Rigamonti E et al. PPARg activation primes human monocytes into alternative M2 macrophages with anti-inflammatory properties. Cell Metab 2007;
6: 137–43.
Huang JT, Welch JS, Ricote M et al. Interleukin-4-dependent
production of PPAR-c ligands in macrophages by 12 ⁄ 15 lipoxygenase. Nature (London) 1999; 400: 378–82.
Review: PPARs
77 Shu H, Wong B, Zhou G et al. Activation of PPARa or c
reduces secretion of matrix metalloproteinase 9 but not interleukin 8 from human monocytic THP-1 cells. Biochem Biophys Res Commun 2000; 267: 345–9.
78 Nakamachi T, Nomiyama T, Gizard F et al. PPARalpha agonists suppress osteopontin expression in macrophages and
decrease plasma levels in patients with type 2 diabetes. Diabetes 2007; 56: 1662–70.
79 Neve BP, Corseaux D, Chinetti G et al. PPARalpha agonists
inhibit tissue factor expression in human monocytes and
macrophages. Circulation 2001; 103: 207–12.
80 Marx N, Mackman N, Schonbeck U et al. PPARalpha activators inhibit tissue factor expression and activity in human
monocytes. Circulation 2001; 103: 213–9.
81 Devchand PR, Keller H, Peters JM, Vazquez M, Gonzalez FJ,
Wahli W. The PPARa-leukotriene B4 pathway to inflammation
control. Nature (London) 1996; 384: 39–43.
82 Teissier E, Nohara A, Chinetti G et al. Peroxisome proliferator-activated receptor alpha induces NADPH oxidase activity
in macrophages, leading to the generation of LDL with PPARalpha activation properties. Circ Res 2004; 95: 1174–82.
83 Welch JS, Ricote M, Akiyama TE, Gonzalez FJ, Glass CK.
PPAR{gamma} and PPAR{delta} negatively regulate specific
subsets of lipopolysaccharide and IFN-{gamma} target genes in
macrophages. Proc Natl Acad Sci U S A 2003; 100: 6712–7.
84 Lee CH, Chawla A, Urbiztondo N et al. Transcriptional
repression of atherogenic inflammation: modulation by PPARdelta. Science 2003; 302: 453–7.
85 Staels B, Koenig W, Habib A et al. Activation of human aortic
smooth-muscle cells is inhibited by PPARa but not by PPARc
activators. Nature (London) 1998; 393: 790–3.
86 Gervois P, Kleemann R, Pilon A et al. Global suppression of
IL-6-induced acute phase response gene expression after
chronic in vivo treatment with the peroxisome proliferatoractivated receptor-alpha activator fenofibrate. J Biol Chem
2004; 279: 16154–60.
87 Kowalski J, Okopien B, Madej A et al. Effects of fenofibrate
and simvastatin on plasma sICAM-1 and MCP-1 concentrations in patients with hyperlipoproteinemia. Int J Clin Pharmacol Ther 2003; 41: 241–7.
88 Okopien B, Krysiak R, Herman ZS. Effects of short-term fenofibrate treatment on circulating markers of inflammation and
hemostasis in patients with impaired glucose tolerance. J Clin
Endocrinol Metab 2006; 91: 1770–8.
89 Jonkers IJ, Mohrschladt MF, Westendorp RG, van der Laarse
A, Smelt AH. Severe hypertriglyceridemia with insulin resistance is associated with systemic inflammation: reversal with
bezafibrate therapy in a randomized controlled trial. Am J Med
2002; 112: 275–80.
90 Despres JP, Lemieux I, Pascot A et al. Gemfibrozil reduces
plasma C-reactive protein levels in abdominally obese men
with the atherogenic dyslipidemia of the metabolic syndrome.
Arterioscler Thromb Vasc Biol 2003; 23: 702–3.
91 Mohanty P, Aljada A, Ghanim H et al. Evidence for a potent
antiinflammatory effect of rosiglitazone. J Clin Endocrinol
Metab 2004; 89: 2728–35.
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42
M. A. Bouhel et al.
|
Review: PPARs
92 Raskin P, Rappaport EB, Cole ST, Yan Y, Patwardhan R,
Freed MI. Rosiglitazone short-term monotherapy lowers fasting and post-prandial glucose in patients with type II diabetes.
Diabetologia 2000; 43: 278–84.
93 Meisner F, Walcher D, Gizard F et al. Effect of rosiglitazone
treatment on plaque inflammation and collagen content in nondiabetic patients: data from a randomized placebo-controlled
trial. Arterioscler Thromb Vasc Biol 2006; 26: 845–50.
94 Sidhu JS, Cowan D, Tooze JA, Kaski JC. Peroxisome proliferator-activated receptor-gamma agonist rosiglitazone reduces
circulating platelet activity in patients without diabetes mellitus
who have coronary artery disease. Am Heart J 2004; 147: e25.
95 Sidhu JS, Cowan D, Kaski JC. The effects of rosiglitazone, a
peroxisome proliferator-activated receptor-gamma agonist, on
markers of endothelial cell activation, C-reactive protein, and
fibrinogen levels in non-diabetic coronary artery disease
patients. J Am Coll Cardiol 2003; 42: 1757–63.
96 Nakamura T, Ushiyama C, Shimada N, Hayashi K, Ebihara I,
Koide H. Comparative effects of pioglitazone, glibenclamide,
and voglibose on urinary endothelin-1 and albumin excretion
in diabetes patients. J Diabetes Complicat 2000; 14: 250–4.
97 Wang CH, Ting MK, Verma S et al. Pioglitazone increases the
numbers and improves the functional capacity of endothelial
progenitor cells in patients with diabetes mellitus. Am Heart J
2006; 152: 1051–e1.
98 Werner C, Kamani CH, Gensch C, Bohm M, Laufs U. The
PPAR-{gamma} agonist pioglitazone increases number and
function of endothelial progenitor cells in patients with coronary artery disease and normal glucose tolerance. Diabetes
2007; 56: 2609–15.
99 Frick MH, Syvanne M, Nieminen MS et al. Prevention of the
angiographic progression of coronary and vein-graft atherosclerosis by gemfibrozil after coronary bypass surgery in men
with low levels of HDL cholesterol. Circulation 1997; 96:
2137–43.
100 Ericsson C, Hamsten A, Nilsson J, Grip L, Svane B, de Faire
U. Angiographic assessment of effects of bezafibrate on progression of coronary artery disease in young male postinfarction patients. Lancet 1996; 347: 849–53.
101 Effect of fenofibrate on progression of coronary-artery disease
in type 2 diabetes: the Diabetes Atherosclerosis Intervention
Study, a randomised study. Lancet 2001; 357: 905–10.
102 Marx N, Wohrle J, Nusser T et al. Pioglitazone reduces neointima volume after coronary stent implantation: a randomized,
placebo-controlled, double-blind trial in nondiabetic patients.
Circulation 2005; 112: 2792–8.
103 Katayama T, Ueba H, Tsuboi K et al. Reduction of neointimal
hyperplasia after coronary stenting by pioglitazone in nondiabetic patients with metabolic syndrome. Am Heart J 2007;
153: 762–e1.
104 Mazzone T, Meyer PM, Feinstein SB et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes: a randomized trial. JAMA 2006; 296:
2572–81.
105 Langenfeld MR, Forst T, Hohberg C et al. Pioglitazone
decreases carotid intima-media thickness independently of
106
107
108
109
110
111
112
113
114
115
116
117
glycemic control in patients with type 2 diabetes mellitus:
results from a controlled randomized study. Circulation 2005;
111: 2525–31.
Bhatt DL, Chew DP, Grines C et al. Peroxisome proliferatoractivated receptor gamma agonists for the prevention of adverse
events following percutaneous coronary revascularization –
results of the PPAR study. Am Heart J 2007; 154: 137–43.
Frick MH, Elo O, Haapa K et al. Helsinki Heart Study: primary prevention trial with gemfibrozil in middle-aged men
with dyslipidemia. Safety of treatment, changes in risk factors,
and incidence of coronary heart disease. N Engl J Med 1987;
317: 1237–45.
Keech A, Simes RJ, Barter P et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with
type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet 2005; 366: 1849–61.
The BIP Study Group. Secondary prevention by raising HDL
cholesterol and reducing triglycerides in patients with coronary
artery disease: the Bezafibrate Infarction Prevention (BIP)
study. Circulation 2000; 102: 21–7.
Rubins HB, Robins SJ, Collins D et al. Gemfibrozil for the
secondary prevention of coronary heart disease in men with
low levels of high-density lipoprotein cholesterol. Veterans
Affairs High-Density Lipoprotein Cholesterol Intervention
Trial Study Group. N Engl J Med 1999; 341: 410–8.
Colhoun HM, Betteridge DJ, Durrington PN et al. Primary
prevention of cardiovascular disease with atorvastatin in type 2
diabetes in the Collaborative Atorvastatin Diabetes Study
(CARDS): multicentre randomised placebo-controlled trial.
Lancet 2004; 364: 685–96.
Gerstein HC, Yusuf S, Bosch J et al. Effect of rosiglitazone on
the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled
trial. Lancet 2006; 368: 1096–105.
Kahn SE, Haffner SM, Heise MA et al. Glycemic durability
of rosiglitazone, metformin, or glyburide monotherapy. N Engl
J Med 2006; 355: 2427–43.
Belfort R, Harrison SA, Brown K et al. A placebo-controlled
trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med 2006; 355: 2297–307.
Dormandy JA, Charbonnel B, Eckland DJ et al. Secondary
prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled
trial. Lancet 2005; 366: 1279–89.
Wilcox R, Bousser MG, Betteridge DJ et al. Effects of pioglitazone in patients with type 2 diabetes with or without previous
stroke: results from PROactive (PROspective pioglitAzone
Clinical Trial In macroVascular Events 04). Stroke 2007; 38:
865–73.
Erdmann E, Dormandy JA, Charbonnel B, Massi-Benedetti
M, Moules IK, Skene AM. The effect of pioglitazone on
recurrent myocardial infarction in 2,445 patients with type 2
diabetes and previous myocardial infarction: results from the
PROactive (PROactive 05) Study. J Am Coll Cardiol 2007;
49: 1772–80.
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42 41
M. A. Bouhel et al.
|
118 Rubenstrunk A, Hanf R, Hum DW, Fruchart JC, Staels B.
Safety issues and prospects for future generations of PPAR
modulators. Biochim Biophys Acta 2007; 1771: 1065–81.
119 Watkins PB, Whitcomb RW. Hepatic dysfunction associated
with troglitazone. N Engl J Med 1998; 338: 916–7.
120 Khan MA, St Peter JV, Xue JL. A prospective, randomized
comparison of the metabolic effects of pioglitazone or rosiglitazone in patients with type 2 diabetes who were previously
treated with troglitazone. Diabetes Care 2002; 25: 708–11.
121 Mudaliar S, Chang AR, Henry RR. Thiazolidinediones,
peripheral edema, and type 2 diabetes: incidence, pathophysiology, and clinical implications. Endocr Pract 2003; 9:
406–16.
122 Grey A, Bolland M, Gamble G et al. The peroxisome proliferator-activated receptor-gamma agonist rosiglitazone decreases
bone formation and bone mineral density in healthy postmenopausal women: a randomized, controlled trial. J Clin Endocrinol Metab 2007; 92: 1305–10.
123 Aguilar D, Bozkurt B, Pritchett A, Petersen NJ, Deswal A.
The impact of thiazolidinedione use on outcomes in ambulatory patients with diabetes mellitus and heart failure. J Am
Coll Cardiol 2007; 50: 32–6.
42
Review: PPARs
124 Lago RM, Singh PP, Nesto RW. Congestive heart failure and
cardiovascular death in patients with prediabetes and type 2
diabetes given thiazolidinediones: a meta-analysis of randomised clinical trials. Lancet 2007; 370: 1129–36.
125 Nissen SE, Wolski K. Effect of rosiglitazone on the risk
of myocardial infarction and death from cardiovascular causes.
N Engl J Med 2007; 356: 2457–71.
126 Singh S, Loke YK, Furberg CD. Long-term risk of cardiovascular events with rosiglitazone: a meta-analysis. JAMA 2007;
298: 1189–95.
127 Home PD, Pocock SJ, Beck-Nielsen H et al. Rosiglitazone
evaluated for cardiovascular outcomes – an interim analysis. N
Engl J Med 2007; 357: 28–38.
128 Lincoff AM, Wolski K, Nicholls SJ, Nissen SE. Pioglitazone
and risk of cardiovascular events in patients with type 2 diabetes mellitus: a meta-analysis of randomized trials. JAMA 2007;
298: 1180–8.
Correspondence: Bart Staels, UR 545 INSERM, Institut Pasteur de
Lille, 1, rue Calmette BP245, 59019 Lille, France.
(fax: 33 3 20 87 71 98; e-mail: [email protected]).
ª 2007 Blackwell Publishing Ltd Journal of Internal Medicine 263; 28–42






© Copyright 2026