
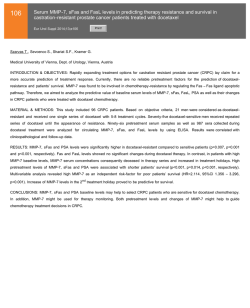
Serum Levels of Soluble Intercellular Adhesion Molecule 1
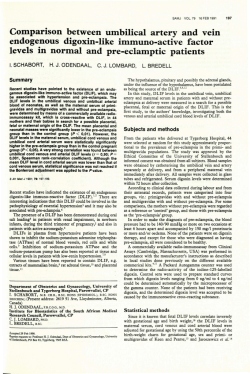
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Serum Levels of Soluble Intercellular Adhesion Molecule 1 Are Increased in Chronic B-Lymphocytic Leukemia and Correlate With Clinical Stage and Prognostic Markers By llse Christiansen, Cecilia Gidlof, AnnaCarin Wallgren, Bengt Simonsson, and Thomas H. Totterman The serum levels of soluble intercellular adhesion molecule 1 (ICAM-1) were significantly elevated ( P < .001) in patients with chronic B-lymphocytic leukemia (B-CLL, n = 113) compared with healthy controls (n = 31). SICAM-llevels in B-CLL were positively correlated to thetumor mass asreflected by the modified Rai and the Binet staging systems, lymphocyte counts, and isolated spleno/hepatomegaly. During disease progression or regression on cytoreductive therapy, the circulating SICAM-l levels changed accordingly. SICAM-l was also correlated to a kinetic parameter such as the lymphocyte doubling time. Furthermore, the serum SICAM-l levels were inversely correlated to hemoglobin levels in patients with earlyclinicalstage, and this may turn out to be of prognostic value. SICAM-l wascompared with other serum markers said to reflect disease activity in B-CLL, ie, soluble CD23, thymidine kinase, lactate dehydrogenase (LDH), and P,-microglobulin. SICAM-l wasequally well or better correlated toclinical stage and lymphocyte doubling time. Inunivariate regression analysis,all serum markers but LDH correlated with survival, and in multivariate analysis, SICAM-l was theonly marker approaching significance foradditional prognostic information when included after clinicalstage and lymphocyte doubling time. Based on the present observations, it appears that prospective studies repeatedly monitoring serum SICAM-l in B-CLL are justified. 0 1994 by The American Societyof Hematology. C and regulate important cell-stromal and cell-cellinteractions" such as leukocyte adhesion and migration, mitogenand alloantigen-induced T-cell proliferation, T/natural killer (NK) cellkilling,and meta~tasis.'"~' Recently, an 82-kD soluble form of ICAM-I (SICAM-l) was detected in serum of normalsubjects as well as patientswithinflammatory conditions such as allograft rejection, rheumatoid arthritis. systemic lupus erythematosus, and Wegener's granulomatosis. .zx-32 Elevated levels of SICAM-lwere also reported in malignant disorders including melanoma, Hodgkin's disease (HD), and childhood acute lymphoblastic leukemia (ALL)?" We report here that serum sICAM-I levels are elevated in B-CLL and correlate with the clinical stage, lymphocyte doubling time (LDT),isolated hepato/splenomegaly, and Hb level. The prognostic value of SICAM-l was further compared with known serum markers of disease activity such as sCD23, TK, LDH, and P2m. HRONICB-LYMPHOCYTICleukemia (B-CLL)the most common type of leukemia in Western countries -represents a monoclonal expansion of phenotypically small,slightly immature,and activatedCD5'B cellsexpressing surface IgMfrequently specific for autoantigen. The clinical course of B-CLL is quite variable, and consequently, attempts have been made to find methods for the prediction of prognosis and timing of therapy. Critical reviews"' of these methods have clearly established the value of clinical staging systems'". However, among B-CLL patients reprewill senting low-risk stages (Rai 0, Binet A),some20% progress more rapidly, and other methodspredicting progression are needed.' Additional independent prognostic information may be obtained by determination of the blood lymphocyte doubling time,"' hemoglobin (Hb) level," marrow histopathology," lymphocyte morphology," cytogenetic patterns,'$ and probably also the blood lymphocyte count." A number of serum markers including lactate dehydrogenase (LDH)," /?,-microglobulin (,&m)," thymidine kinase (TK),lX soluble CD23 (sCD23)," and recently, soluble CD27 ( s C D ~ ~were ) ~ " reported to be positively correlated to clinical stage, but need to be evaluated further. The intercellular adhesion molecule 1 (ICAM-1, CD54), a 90-kD member of the Ig supergene family, is the ligand forthe integrin lymphocyte function-associatedantigen 1 (LFA- I , CD 11a/CD 1 ICAM- ULFA- 1 are widelydistributed among hematopoietic and nonhematopoietic cells From the Department of Clinical Immunology and Transfusion Medicine and the Department of Medicine. UniversiQ Hospitul, Uppsala, Sweden. Submitted April 19, 1994; uccepted July S, 1994. Supported by grants from the Swedish Cancer Society and the Lion's Cancer Fund at the University Hospital, Uppsala, Sweden. Addressreprintrequests to Thomas H . Tiitterman,MD,PhD, Department of Clinical Immunology. University Hospital, S-751 8.5 Uppsala, Sweden. The publication costs of this article were defrayedin part by page chargepayment. This article must thereforebeherebymarked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate thi.y ,fact. 0 1994 by The American Society of Hematology. 0006-497//94/8409-0013$3.00/0 3010 MATERIALS AND METHODS Patients and Control Subjects We studied 1 13 B-CLL patients (75 men and 38 women, mean age, 69; range, 44 to 88). all fulfilling the diagnostic criteria of the International Workshop on CLL (IWCLL)." Serum samples were ( I 2 to 460 months) and collected at varying intervals after diagnosis stored at -70°C until use. Seventy-one patients were untreated, five patientsweresplenectomized only (91,76, 18, 6,and 4 months before study), and 1S patients had received chemotherapy, but were off treatment (3 to 240 months). Two of the latter patients had been splenectomized(39and48monthsearlier).Twenty-two patients were on chemotherapy (nine chlorambucil-prednisolone, five COP, two CHOP, two prednisolone. one cyclosporine-A, one teniposide, and one prednimustine). Three of these cases had been splenectomized (60, 12, and 2 months before study). At the time of serum sampling, all I 1 3 patients were restaged according to the systems of Rai et and Binet et al.' The LDT's were calculated retrospectively in the 76 untreated patients all having observation times in excess of l year. All 22 patientsundergoingchemotherapyhad LDT's 5 1 year before treatment, and were classified accordingly. LDT's were In the IS casesreceivingintermittentchemotherapy, estimated a minimum of 3 months after treatment. At the time of serum sampling, analysis of routine hematologic variables including determination of serum LDH (n = 95) and serum TK (n = 74) were performed, Repeated sampling of sera was done in I O patients with disease progression (n = X ) or regression (n = 2). Blood, Vol 84,No 9 (November l), 1994: pp 3010-3016 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. SICAM-1 3011 IS ELEVATED IN B-CLL Serum samples from 31 healthy elderly blood donors (mean, 51 years; range, 40 to 60 years) were analyzed for comparison. Assays SICAM-l. The SICAM-l levels in serum were determined by enzyme immunoassay (EIA) kits purchased from British Biotechnology Products Ltd (Oxon. UK). The assay is based on two monoclonal antibodies (MoAbs) directed against different epitopes on the SICAM-l molecule. The capture MoAb is bound to solid phase and the detection MoAb is conjugated to horseradish peroxidase (HRP). 3, 3, 5 , 5-tetramethylbenzidine (TMB) is used as substrate. The colored product was quantified photometrically using a spectrophotometer (Titertek Multiskan MCC1340, Solna, Sweden) set at 450 nm with a correction wavelength of 620 nm. Data were evaluated by Deltasoft 3.3 MCC software for the Macintosh (both from Apple Computers, Cupertino, CA). The sensitivity of the assay was 0.35 ng/mL, the interassay coefficient of variance (CV) was less than 7.4% and the intra-assay CV varied between 3.3% and 4.8%. Serum samples from IO patients were tested fresh and after freeze thawing. The SICAM-l levels were unaltered. µglobulin. Soluble pzm levels in serum were determined by EIA kits (T Cell Diagnostics, Inc, Cambridge, UK) based on a competitive assay in which HRP-labeled Pzm competes with cold serum ligand for binding to solid phase antiserum. After incubation with TMB, the colored product was measured using the spectrophotometer set at 450 nm. The sensitivity of the assay was 0.25 pg/mL, the intra-assay CV was less than 6% and the interassay CV was less than 13%. sCD23. sCD23 EIA kits (The Binding Site, Birmingham, UK). were based on three antibodies. The capture MoAb is bound to solid phase, and detection involves sheep-antihuman sCD23 followed by HRP-conjugated antisheep IgG. TMB is used as substrate and the colored product is measured by spectrophotometry. The intra-assay precision CV was 4.2% and the interassay CV was 18.9%. Thymidine kinase. TK is a routine analysis at our institution. In a radioenzymatic technique (Prolifigen assay; Sangtec Medical, Bromma, Sweden), TK converts ['251]deoxyuridine into ["'I] deoxyundine monophosphate, and the reaction product, but not the unconverted substrate, is absorbed to a granulate. The radioactivity of the granulate is then measured after several washings. The mean serum TK level in healthy adults was 2.4 1.3 U L . TK values above 5 U/L (mean + 2 SD) were considered elevated. Lactate dehydrogenase. LDH is a routine analysis at our institution. LDH (EC 1.1.l .27) was analyzed on a Hitachi 7 17 spectrophotometer (Boehringer Mannheim Diagnostica, Titzing, Germany) using an LDH reagent from the same manufacturer (Catalogue No. 191 353 ). In short, LDH catalyzes pyruvate to lactate + nicotinamide adenine dinucleotide (NAD) in the presence of reduced NAD (NADH) + H+. Kinetic measurement of NAD at 340 nm proportionally reflects the concentration of LDH. The serum levels in healthy subjects ranged from 3.8 to 6.7 pkat/L. RESULTS Serum SICAM-I Is Elevated in B-CLL All 113 B-CLL patients and 31 control subjects had detectable serum sICAh4-1 (Fig l). Circulating SICAM-l levels were significantly elevated ( P = , 0 0 0 9 ) in the patient group (533 2 293 ng/mL, mean 2 SD) compared with the control group (329 t 132 ng/mL),althoughvalueswerewidely scattered in B-CLL. The sICAh4-1 levels in patients representing the lowest Rai stage 0 (395 -C 169 ng/mL) were not different from controls ( P = .06). However, whenComparing Binet stage A patients (412 5 205 ng/mL) with controls, a significant difference was found ( P = .03) (see below). SICAM-I in Relation to Clinical Staging Systems When applying the modifiedRai classification system(Fig 2), B-CLL patients representing high-risk stages had significantly higher ( P < .0001) serum levels of SICAM-l (71 1 5 336 ng/mL) compared with intermediate-risk (443 t 217) 1500 1250 Q 1o00, Q 750 500, 250 Statistical Methods Data are presented as mean 2 SD. P values less than .05 were considered significant. Analysis of variance was used to compare serum SICAM-l levels with the clinical classification systems of Rai and Binet. The paired Student's t-test was used to compare serum SICAM-I levels to lymphocyte counts, LDT, and Hb levels. Spearman's correlation coefficient was used to determine the association between SICAM-land other serum markers,and the association between lymphocyte count and serum markers. The Cox proportional hazard regression model was used in univariate and multivariate analyses. r *1 ** 0 8 CI 8 0 0, Q0 I I Controls B-CLL (n=31) (n=113) Fig 1. Serum slCAM-1 levels in B-CU patients and healthy controls (P= .OOOS). Horizontal bars indicate mean values. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3012 CHRISTIANSEN ET AL 1500 7 *** l r *** l I n s , 0 1250 !l 0 0 8 lo00 8 0 Q 8 750 Serial Determinations of SICAM-I 8 0 500 250 0 0 sionmolecules and their soluble counterparts, we studied splenomegalyhepatomegaly and therelationshipbetween SICAM-l (n = 39, of which only 4 had hepatomegaly, excluding splenectomized cases). Patients with organomegaly had significantly ( P = ,0006)higher levels of SICAM- 1 (707 i 317 v 430 5 240 ng/mL), as shown in Fig 4B. A correlation existed between the lymphocyte counts and serum levelsof sICAM-l ( r = .32, P = .0009) but data were widely distributed (not shown). Excluding patients on therapy or off treatment with cytostatics, the same pattern was seen (not shown). I 0 (n=23) 8 0 I 1-11 (n=61) In 10 B-CLL patients, sera were obtained prospectively at 2 to 8 occasions and analyzed for SICAM-l. According to the original Rai classification, 8 of 10 patients exhibited a change in clinical stage (7 progressions and l regression on therapy). As shown in Fig 5 , a switch in Rai stage was consistently paralleled by a corresponding change in serum SICAM-l level in all individuals studied. The same results were registered using the Binet (9/10 changes in stage) and IIIh lo00 (n=29) I *** l 0 0 Fig 2. Serum SICAM-l in relation to the corrected Rai classification. B-CLL patients in high-riskstages have significantlyhigher (P< .OOOl) levels of SICAM-l than patients in low- and intermediaterisk stages. Horizontal bars indicate mean values. 0 0 750 and low-risk (380 -C 185) patients. There was a trend toward higher sICAM-l levels in the intermediate-risk versus lowrisk group, but the difference wasnot statistically significant. Using the Binet staging system, we likewise found that the SICAM-l levels in stage C (739 t- 335 ng/mL) were significantly elevated (P < .0001) compared with stages B and A (481 t- 245 and 448 t- 233, respectively). Again, no difference was found between stages A and B (data not shown). Among B-CLL patientsin Binet stage A,a survival advantage has been reported for patients with Hb values greater than 120 g/L compared with cases having Hb values 120 g/ L or less." Therefore, we compared circulating SICAM-l levels with Hb levels in 48 stage-A patients. Patients with Hb values 5 1 2 0 g/L had significantly higher ( P = ,001) serum SICAM-l levels compared with patients havinghigher Hb values (S83 t- 241 v 366 t- 163 ng/mL) (Fig 3). 0 0 0 0 504 250 B 0 0 0 8 0 e SICAM-I Versus Lymphocyte Doubling Time, Lymphocyte Count, and Organomegaly Patients having an LDT less than 1 year had significantly higher levelsof serum SICAM-l comparedwith cases having longer LDT's (640 t- 331 v 434 t 213 ng/mL, P = .01) (Fig 4A). Neither the modified Rai nor the Binet classification accounts for hepatomegaly andor splenomegaly as single factor. Because this might be relevant when considering adhe- 0 a Hb > 120 gh (n=38) Hb I 120 g/l (n=10) Fig 3. Serum SICAM-l in Binet stage A patients related to Hb levels ( P = .001). The horizontal bars indicate mean values. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3013 IS ELEVATED IN B-CLL SICAM-l B A I yY1 l 1" l " I I 1250 0 0 8 0 0 8 0 Q8 8 0 B 8 0 0 1000 t 750 e 0 i 8 8 Fig 4. (A) Serum SICAM-l levels are correlated with the lymphocyte doubling time (LDT; P= .01). (B) Patientswith splenomegaly andlor hepatomegaly have hiaher serum levels of slCAM-l than patients without organomegaly ( P = .0006). Horizontal bars indicate mean values. (n=60) I 0 0 0 0 0 1250 1000 I l " " 1500 0 0 0 0 8 Ie I 8 8 0 - LDT 2 1 year LDT < 1 year (n=53) IWCLL 1992 (10/10 changes in stage) classifications (data not shown). One patient was treated with peroral 2-chlorodeoxyadenosine (CdA) X 8 according to a recent protocol. A good partial remission was recorded, the patient changing in stage from C(IV) to A(0) at the end of therapy. The serum SICAM-l levels rapidly dropped to normal levels and stayed low during therapy (from 724 to 325 ng/mL). One B-CLL patient was monitored before and after splenectomy. Serum SICAM-1 rapidly dropped from 8 18 to 470 ng/mL after the operation (data not shown). 1"' I /4 Organomeg. No Organomeg. (n=64) (n=39) SICAM-I Compared With Other Serum Markers Among serum markers claimed to be associated with clinical stage and disease activity in B-CLL, we chose to consider sCD23, TK, P2m, andLDH and compared these with SICAM-1 (Tables 1 through 3). The correlation between each individual serum marker and the corrected Rai classification is shown in Table 1. SICAM-lwas equal or superior to sCD23, TK, and LDH. No significant correlation between P2m and corrected Rai stage was registered. Table 2 shows the correlation between each individual serum marker and the LDT. With the exception of LDH, the other serum markers (SICAM-l, sCD23, TK, and P2m) were correlated to LDT,with marginal significance for P2m. Table 3 shows the criss-cross correlations between serum levels of the five markers and the lymphocyte count. SICAM-l wasmost strongly correlated to TK and sCD23, followed by P2m and the lymphocyte count. No correlation was seen with LDH. SICAM-I and Prognosis 0 0 I n 1 I11 IV Fig 5. Serialanalysis of serum SICAM-l in eight patients changing in Rai stage (seven progressing and one regressing on therapy). Table 4 shows the prognostic value (survival) of SICAM1 and the four other serum markers in univariate and multivariate Cox regression analysis. A significant ( P < .002) survival advantage was registered in patients with lower serum SICAM-l levels. However, no cutoff value was found. With the exception of LDH, the other markers sCD23, TK, and P2m also showed significant correlation to survival. Mul- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. CHRISTIANSEN ET AL 301 Table 1. Rai Staging System Correlated With Different Serum Markers Rai Stage I + II 0 SICAM-l (ng/mL) sCD 23 (pglmL) O m (pg/mL) TK (U/L) LDH(pkat!L) PValues 380 -t 185' (n = 22) 339 2 283 (n = 22) 5.23 2 9.24 (n = 22) 2.60 5 0.99 (n = 13) 6.04 t 1.39 (n = 20) 443 724 4.92 7.50 6.34 111 2 217 (n = 62) t 688 (n = 61) 2 6.45 (n = 61) 2 5.84 (n = 43) 5 1.63 (n = 54) 711 1,796 7.97 25.5 9.88 + IV 0 5 336 (n = 29) 2 1,466 (n = 291 f 6.08 (n = 29) 2 29.89 (n = 18) f 5.29 (n = 21) VI + II 0 VIII NS NS NS NS NS + IV 1.0001 <.0001 NS ,0001 1.0001 I t II V I I I i- IV ,0001 .ooo 1 NS 1.0001 1.0001 Abbreviation: NS, not significant. * Mean 5 standard deviation. Table 2. Lymphocyte Doubling Time Correlated With Serum Markers Lymphocyte Doubling Time <lyr SICAM-l 575 sCD23 (pg/mL) 1,216 732 P2m (pg/mL) 17 TK (U/L) 7.8 LDH (pkaVL) P Values 2 1 yr 2 297* (n = 48) 444 2 248 (n = 65).01 f 1,158 (n = 48)709 2 910 (n = 64).01 2 793 (n = 47) 464 2 615 (n ? 23 (n = 34)5.8 f 5.6 (n = 40) 6.6 2 2.5 (n = 55) 2 3.9 (n = 40) = 65).05 .004 NS Abbreviation: NS, not significant. * Mean 2 SD. tivariate analysis was performed with two, three, or four prognostic factors against each serum marker. The results were identical, and therefore, only the analyses testing the corrected Rai staging plus LDT versus each serum marker are shown (Table 4).The highest P value was obtained for SICAM-l, although this did not reach significance ( P = .08) in the present patient material. DISCUSSION The most commonly used methods for predicting prognosis in B-CLL are clinical staging systems that estimate the static tumor mass:7,L5,37 whereas additional information is obtained by studying the kinetics of leukemic cell expansion, ie, lymphocyte doubling time," the lymphocyte and marrow morphol~gy,'~ and ~ ' ~cytogenetic aberration^.'^ The prediction of prognosis is particularly difficult in patients representing early clinical stages," and serial monitoring of different serum marker~l~.~' and activated lymphocyte phenotypes3' reflecting disease activity have been proposed. The present investigation is, to our knowledge, the first to show that serum levels of 82-kD SICAM-l are elevated in B-CLL and correlate with survival in univariate analysis. However, elevated serum levels of SICAM-l have recently been described in patients with other hematopoietic tumors such as HD34-36a and childhood ALL,36and also in malignant melanoma3333y. In HD patients, serum SICAM-l levels were related to tumor mass, B symptoms, circulating interleukin2 (IL-2) receptor (CD25) levels, and disease-free survival. In melanoma, increased SICAM-l serum levels" and tumor cell ICAM-l expression4"were typical for metastatic disease. In the case of HD, it was shown by histochemistry that the malignant cells overexpress ICAM-1,35and that HDcell lines release SICAM-l when exposed to various c y t o k i n e ~ . ~ ~ In the present study, the serum SICAM-l levels inBCLL patients were positively correlated to the tumor mass as reflected by the modified Rai and Binet stagings, lymphocyte counts and isolated splenomegaly/hepatomegaly.In patients repeatedly monitored during disease progression or regression on cytoreductive therapy, the circulating SICAM-l levels changed accordingly. SICAM-l was also correlated to a kinetic parameter represented by the lymphocyte doubling time. This indicates that SICAM-l maynot simply reflect the static tumor mass in B-CLL. Further, the serum SICAM1 levels were inversely correlated to Hb levels in patients with early clinical stage, and this may turn out to have prognostic significance." We also compared SICAM-l with other serum markers said to reflect disease activity in B-CLL, ie, sCD23, TK, LDH, and P2m.L6"9SICAM-l was equally well or better correlated with clinical stage and LDT.In univariate regression analysis, all serum markers but LDH correlated with survival, andin multivariate analysis, SICAM-I was the only markerapproaching significance ( P = .08) for prognostic information when included after clinical stage and lymphocyte doubling time. Based on all the present observa- Table 3. Correlation of SICAM-l With Other Serum Markers and Lymphocyte Count Lymphocyte Count SICAM-l sCD 23 &m TK SICAM-1 sCD 23 0.32' ( P = ,0009) 0.41 ( P < .0001) 0.47 - 0.47 ( P < ,0001) 0.45 ( P < ,0001) 0.42 ( P < .0001) P m 0.06 (NS) 0.21 (NS) 0.06 (NS) 0.52 ( P < ,0001) 0.47 ( P < ,0001) 0.45 ( P = ,0001) TK LDH ( P i ,0001) 0.45 ( P < ,0001) 0.52 ( P < .0001) 0.47 0.18 (NS) Abbreviation: NS, not significant. Spearman's correlation coefficient. 0.42 ( P < ,0001) ( P < ,0001) 0.45 0.24 ( P0.12 = .02) - ( P = .0001) (NS) LDH 0.18 (NS) 0.24 ( P = .02) 0.12 (NS) - 0.50 ( P < ,0001) 0.50 ( P < ,0001) - From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3015 SICAM-l IS ELEVATED IN B-CLL Table 4. Prognostic Value of dCAM-1 and Other Serum Markers Teated in the Cox Proportional Hazard Regression Model ~~ SICAM-l sCD23 D2m TK LDH Univariate Analysis ( P value) Multivariate Analysis ( P value) ,002 <.002 .08 ,006 ,002 .068 .23 .30 .27 .95 tions, we think that a prospective study repeatedly monitoring serum SICAM-l in B-CLL is justified. The cellular origin of SICAM-l in B-CLL is presently unknown. Soluble ICAM-l is thought to be released from the cell surface through proteolytic cleavage:'"' Some 40% of B-CLL patients were reported to have surface ICAM-lI leukemic cells in the blood.43 However, in our experience the surface expression of ICAM-1 on circulating B-CLL cells is low and poorly correlated with serum SICAM-l levels (unpublished observations). Further, circulating B-CLL cells are arrested in the GO phase of the cell cycle," and the proliferative tumor cell compartment is likely represented by the bone marrow, lymph nodes, and spleen. Several inflammatory mediators including IL-1, tumor necrosis factor a (TNFa),interferon 7 , and IL-4 enhance cell surface expression of ICAM-1,'" 45-48 and B-CLL cells have been reported to releaseatleast TNFa, E-1, andpossibly IL-2."-5' Furthermore, T-cells and NK-cells in these patients are phenotypically a~tivated.~' Thus, circulating SICAM-l in B-CLL may originate from either tumor cells, regulatory cell types, or both, and this is presently under investigation. ACKNOWLEDGMENT We are grateful to Dr J. Bring and A. Taube at the Department of Statistics, Uppsala University, for their expert help with the statistical analysis. REFERENCES 1. Montserrat E, Rozman C: Chronic lymphocytic leukemia: Prognostic factors and natural history, in Rozman C (ed): Bailliere's Clinical Hematology, v01 6. London, UK, BalliBre Tindall, 1993, p 849 2. Rai KR: Progress in chronic lymphocytic leukemia: A historical perspective, in Rozman C (ed): BailliBre's Clinical Hematology, v01 6. London, UK, Ballikre Tindall, 1993, p 757 3. Dighiero G, Travade P, Chevret S, Fenaux P, Chastang C, Binet JL, the French Cooperative group on CLL: B-cell chronic lymphocytic leukemia: Present status and future directions. Blood 78:1901, 1991 4. Foon K A , Rai KR, Gale R P Chronic lymphocytic leukemia: New insights into biology and therapy. Ann Int Med 113: 525, 1990 5. Montserrat E, Rozman C: Prognostic factors in chronic lymphocytic leukemia, in Polliack A, Catovsky D (eds): Chronic Lymphocytic Leukemia. Chur, Switzerland, Harwood, 1988, p 111 6. Rai K, Sawitsky A, Cronkite E, Chanana AB, Levy RN, Pasternack BS: Clinical staging of chronic lymphocytic leukemia. Blood 46:219, 1975 7. Binet JL, Auguier A, Dighiero G, Chastang C, Piquet H, Goasguen J, Vaugier G, Potron G, Colona P, Thomas M, Tchernia G, Jacqiullat C, Boivin P, Lesty C, Duault MT, Monconduit M: A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate analysis. Cancer 48:198, 1981 8. Rai KR: A critical analysis of staging in CLL, in Gale RP, Rai KR(eds): Chronic Lymphocytic Leukemia: Recent Progress and Future Directions. New York, NY, Liss, 1987, p 253 9. Chronic lymphocytic leukemia: Proposals for a revised prognostic staging system. Report From The International Workshop on CLL. Br J Haematol 48:365, 1981 10. Montserrat E, Sanchez-Bison0 J, Vifiolas N,Rozman C: Lymphocyte doubling time in chronic lymphocytic leukemia: Analysis of its prognostic significance. Br J Haematol 62567, 1986 11. French Cooperative Group on Chronic Lymphocytic Leukemia: Natural history of stage A chronic lymphocytic leukemia untreated patients. Br J Haematol 76:45, 1990 12. Rozman C, Hernandez-Nieto L, Montserrat E, Brugues R: Prognostic significance of bone marrow patterns in chronic lymphocytic leukemia. Br J Haematol 47529, 1981 13. Melo JV, Catovsky D, Galton DAG: The relationship between chronic lymphocytic leukaemia and prolymphocytic leukaemia. Analysis of survival and prognostic features. Br J Haematol 65:23, 1987 14. Juliusson G, Gahrton G: Chromosomal aberrations in B-cell chronic lymphocytic leukemia. Pathogenetic and clinical implications. Cancer Genet Cytogenet 45:143, 1990 15. Vallespi T, Montserrat E, Sancz MA: Chronic lymphocytic leukemia: Prognostic value of lymphocyte morphological subtypes. A multivariate analysis in 146 patients. Br J Haemtol 77:478, 1991 16. Lee J, Dixon D, Kantarjian H, Keating M, Talpaz M: Prognosis of chronic lymhocytic leukemia: A multivariate regression analysis of 325 untreated patients. Blood 69:929, 1987 17. Simonsson B, Wibell L, Nilsson K: µglobulin in chronic lymphocytic leukemia. Scand J Haematol 24 174, 1980 18. Kallander CFR, Simonsson B, Hagberg H, Gronowitz JS: Serum deoxythymidine kinase gives prognostic information in CLL. Cancer 54:2450, 1984 19. Sarfati M,Bron D, Lagneaux L, Fonteyn C, Frost H, Delaspesse G: Elevations of IgE-binding factors in theserum of patients with B-cell derived chronic lymphocytic leukemia. Blood 71:94, 1988 20. Van Oer's MHJ, Pals ST, Evers LM, Van der Schoot CE, Koopman G, Bonfrer JMG, Hintzen RQ, Von der Borne AEG, Van Lier RAW: Expression and release of CD27 in human B-cell malignancies. Blood 82:3430, 1993 21. Marlin SD, Springer TA: Purified intercellular adhesion molecule-l (ICAM-I) is a ligand for lymphocyte function associated antigen 1 (LFA-I). Cell 512313, 1987 22. Makgoba MW, Sanders ME, Ginther Luce EG, Dustin ML, Springer TA, Clark EA, Mannoni P, Shaw S: ICAM-I a ligand for LFA-l dependent adhesion of B, T and myeloid cells. Nature 33 1:86, 1988 23. Larson, RS, Springer TA: Structure and function of leucocyte integrins. Immunol Rev 114: 181, 1990 24. Pardi R, Inverrardi L, Bender JR: Regulatory mechanisms in leukocyte adhesion: Flexible receptors for sophisticated travellers. Immunol Today 13:224, 1992 25. Dougherty GJ, Murdock S, Hogg N: The function of human intercellular adhesion molecule-l (ICAM-1) in the generation of an immune response. Eur J Immunol 18:35, 1988 26. Dustin ML, Springer TA: Lymphocyte function associated antigen-] (LFA-I) interaction with intercellular adhesion molecule1 (ICAM-l) is one of at least three mechanisms for lymphocyte adhesion to cultured endothelial cells. J Cell Biol 107:321, 1988 27. Smith CN, Martin SD, Rothlein R, Toman C, Anderson DC: Cooperative interactions of LFA-I and Mac-l with intercellular ad- From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 3016 hesion molecule-l in facilitating adherence and transendothelial migration of human neutrophils in vitro. J Clin Invest 83:2008, 1989 28. Rothlein R, Mainolti EA, Czaikowski M, Marlin SD: A form of circulating ICAM-I in human serum. J Immunol 147:3788, 1991 29. Adams DH, Mainolti E, Elias E, Neuberger JM, Rothlein R: Detection of circulating intercellular adhesin molecule- 1 after liver transplantation-Evidence of local release within the liver during graft rejection. Transplantation 55:83, 1993 30. Kling E, Bieg S, Boehme M, Scherbaum WA: Circulating intercellular adhesion molecule-l as anew disease marker in patients with systemic lupus erytromatosis. Clin Invest 71:299, 1993 3 1. Cush JJ, Rothlein R, Lindsley HB, Mainolfi EA, Lipsky PE: Increased levels of circulating intercellular adhesion molecule 1 in the sera of patients with rheumatoid arthritis. Arthritis Rheum 36: 1098, I993 32. Hauschild S, Scmitt WH, Kekow J, Szymkowiak C, Gross WL: Elevated serum levels of ICAM-1 in Wegener’s Granulomatosis. lmmun Infekt 20:84, 1992 33. Harning R, Mainolti E, Bystryn JC, Henn M, Meluzzi VJ, Rothlein R: Serum levels of circulating intercellular adhesion molecule 1 in human malignant melanoma. Cancer Res 51:5003, 1991 34. GNSS HJ, Dolken G, Brach M, Mertelsmann R, Herrman F Serum levels of circulating ICAM-l are increased in Hodgkin’s disease. Leukemia 7: 1245, 1993 35. Pizzolo G, Vinante F, Nadali G, Ricetti MM, Morosato L, Marrocchela R, Vincenzi C: ICAM- I tissue overexpression associated with increased serum levels of its soluble form in Hodgkin’s disease. Br J Haematol 84:161, 1993 36. Pui CH, Luo X, Evans W, Martin S, Rugg A, Wilimus J, Crist WM, Hudson M: Serum intercellular adhesion molecule-l in childhood malignancy. Blood 82:895, 1993 36a. Christiansen I, Kalkner KM, Enblad G, Gildhof C, Glimelius B, Totterman TH: Soluble ICAM-I in Hodgkin’s disease: A promising independent predictive marker for relapse. (submitted) 37. Chronic lymphocytic leukemia: Recommendations for diagnosis, staging and response criteria. International Workshop on CLL. AnnIntMed 110:236, 1989. 38. Totterman TH, Carlsson M, Simonsson B, Bengtsson M, Nilsson K: T-cell activation and subset patterns are altered in B-CLL and correlate with the stage of the disease. Blood 74:786, 1989 39. Altomonte A, Colizzi F, Esposito G, Maio M: Circulating intercellular adhesion molecule 1 as a marker of disease progression in cutaneous melanoma. N Engl J Med 327:959, 1992 40. Johnson JP, Stade BG, Holzmann B, Schwable W, Riethmuller G: De novo expression of intercellular adhesion molecule- 1 CHRISTIANSENET AL in melanoma correlates with increased risk for metastasis. Proc Natl Acad Sci USA 86:641, 1989 41. Rothlein R, Czajkowski M, O’Neill MM, Marlin SD. Mainolti E, Merluzzi VJ: Induction of intercellular adhesion molecule I 011 primary and continuos cell lines by pro-inflammatory cytokines. Regulation by pharmacological agents and neutralizing antibodies. J Immunol I41 :1665, 1988 42. Seth R, Raymond FD, Makgoba MW: Circulating ICAM-I isoforms: Diagnostic prospects for inflammatory and immune disorders. Lancet 338:83, 1991 43. Maio M, Pinto A, Carbone A, Zagonel V, Gloghini A, Marotta G, Cirillo D, Colombatti A, Ferrara F, Del Vecchio L, Ferrone S: Differential expression of CDS4/intercellular adhesion molecule- l in myeloid leukemias and in lymphoproliferative disorders. Blood 76:783, 1990 44. Andreeff M, Darzynkiewicz Z, Sharpless TK, Clarkson BD. Melamed MR: Discrimination of human leukemia subtypes by flow cytometric analysis of cellular DNA and RNA. Blood 55:282, 1980 45. Dustin ML, Rothlein R, Bhan AK, Dinarello CA, Springer TA: Induction by IL-I and interferon-y: Tissue distribution, biochemistry and function of natural adherence molecule (ICAM-I). J lmmunol 137:245, 1986 46. Pober JS, Gimbrone MA, Lapiene LA, Mendrick DL, Fiers W, Rothlein R, Springer TA: Overlapping patterns of activation of human endothelial cells by interleukin-l, tumor necrosis factor and immune interferon. J Immunol 137:1893, 1986 47. Olive D, Lopez M, Blaise D, Viens P, Stoppa AM, Brandely M, Mawas C, Mannoni P, Maraninchi D: Cell surface expression of ICAM-I (CD54) and LFA-3 (CD%), two adhesion molecules, is upregulated on bone marrow leukemic blasts after in vivo administration of high-dose recombinant interleukin-2. J Immunother 10:412, 1991 48. Carlsson M, Soderberg 0, Nilsson K: Interleukin-4 enhances homotypic adhesion of activated B-chronic lymphocytic leukemia (B-CLL) cells via a selective up-regulation of CD54. Scand J Immuno1 37515, 1993 40. Cordingley I T , Hoffbrand AV, Heslop HE, Turner M, Bianchi A, Reittie JE, Vyakarnam A, Brenner MK: Tumor necrosis factor as an autocrine tumour growth factor for chronic B-cell malignancies. Lancet 8592:969, 1988 50. Pistoia V, Cozzolino F, Rubartelli A, Toraia M, Roncella S, Ferranini M:In vitro production of interleukin 1 by normal and malignant human B lymphocytes. J Immunol 136:1688, 1986 S I. Rossi JF, Commes T, Jourdan M: Interleukin-2 production i n B-cell chronic lymphocytic leukemia. Blood 66:840, 1985 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1994 84: 3010-3016 Serum levels of soluble intercellular adhesion molecule 1 are increased in chronic B-lymphocytic leukemia and correlate with clinical stage and prognostic markers [see comments] I Christiansen, C Gidlof, AC Wallgren, B Simonsson and TH Totterman Updated information and services can be found at: http://www.bloodjournal.org/content/84/9/3010.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.














© Copyright 2026