
Reducing Urinary Tract Infection/Catheter Associated UTI Rates at
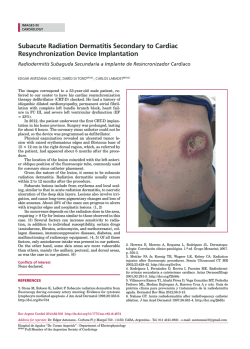
. Reducing Urinary Tract Infection/Catheter Associated UTI Rates at Richmond Hospital Melanie Rydings & Lisa Stewart on behalf of the RH UTI/CAUTI Working Group Aim Statement The Work Qualitative Outcomes Problem: Year to date (2014-15) rates of urinary tract infections among inpatients at Richmond Hospital are 12.6 per 1,000 discharges. Process Map Insert Here! UTIs are the most common Hospital Acquired Infection within Vancouver Coastal Health accounting for 18,900 cases in the past 4 years. The literature suggests that 80% of these are related to urinary catheter placement. Poster: for staff and pts maybe? Pre/ Post Catheter Care & Maintenance Education for Allied Health: Correct Answers are consistently higher post education NSAE: CAUTI - Richmond Quality Urinary Care Allied Health/Porters Quiz Post-Test Results October 2014 NSAE: CAUTI - Richmond Quality Urinary Care Allied Health/Porters Quiz Pre-Test Results October 2014 100 100 83.4 80 60 80 % Goals: All RH patients with catheters have an appropriate and documented indication. 60 59.0 % 40 40 20 20 0 0 Question 1 Question 2 Question 3 Question 4 Question 5 Question 6 Question 7 Question 8 Question 9 Question 10 Question 1 Question 2 Question 3 Question 4 Question 5 Question 6 Question 7 Question 8 Question 9 Question 10 Clinicians and support staff provide appropriate and evidence based Care & Maintenance to catheterized patients. Word on the Units To reduce the Richmond Hospital UTI rate by 25% by September 2015 as measured by Discharge Abstract Database (DAD). Catheters are definitely coming out sooner now that we review them in daily rCARE rounds. Sarah Suozzi, PCC 2 Medicine Telemetry. High Level Strategy I now make sure there is a clear clinical indication before ordering a urinary catheter for a patient. Richard Chan, MD, CCFP (EM), Department Head ED Richmond Hospital Developing a sustainable process by which catheter indication is reviewed daily by interdisciplinary care teams: rCARE and physician rounds. I have many patients all over the hospital and this process is an easy way to track which of my patients have catheters. I wish we had this process for central lines. Dr. Sharadh Sampath, Head, department of surgery, Vancouver Coastal Health – Richmond Provide evidence based care and maintenance education to clinicians and support staff including nursing, allied health, and patient transport. I had no idea that how I was supposed to manage catheters while I was mobilizing patients. I was really glad to see Allied Health included in this Education. Teresa Green, Clinical resource Therapist, VCH. Promote involvement of patients and families in the Care and Maintenance of their indwelling catheter. Next Steps and Sustainability Create Visual tools to: •Provide a method for documenting catheter insertion and indication •Identify patients on the units with indwelling catheters •Track how many day s the catheter has been in •Alert physicians of the presence of an indwelling catheter •Provide physicians with a method for documentation and communication of indication and/or removal. Education to support VCH-U-1030: Intermittent Urinary Catheter, Procedure for Insertion and CPD U-050 Retention Algorithm Introduction of a Daily Care and Maintenance Documentation Tool: Outcome Measures •Discharge Abstract Data and NSQIP UTI Rates •Number of patients with catheters with appropriate indication and documentation. Acknowledgements CAUTI Working Group: Richmond Hospital Kenneth S Poon, MD FRCSC (Urology) Michael McAuley, Director Quality and Patient Safety, VCH Richmond Barb Drake, Clinical Quality & Safety Coordinator Contact: [email protected] and [email protected]







© Copyright 2026