
Effects on Leukocytes After Injection of Tumor Necrosis
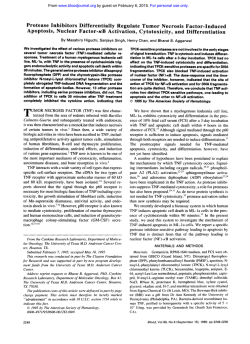
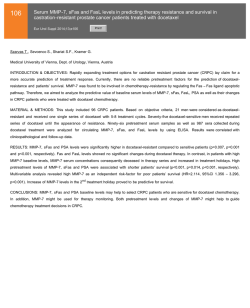
Effects on Leukocytes After Injection of Tumor Necrosis Factor Into Healthy Humans By Tom van der Poll, Sander J.H. van Deventer, C. Erik Hack, Gert J. Wolbink, Lucien A. Aarden, Harry R. Buller, and Jan W. ten Cate Tumor necrosis factor (TNF) has been implicated as a proximal mediator of the septic syndrome. To evaluate the possible role of TNF in leukocyte activation in septicemia, we performed a cross-over saline-controlled study in six healthy men who were intravenously injected with recombinant human TNF (50 pg/m*), and analyzed changes in circulating white blood cells and parameters for neutrophil and monocyte activation. TNF elicited a very rapid neutropenia, reaching a nadir after 15 minutes, followed by a neutrophilia. Lymphocytes showed a sustained decrease, whereas monocytes declined transiently. TNF injection was also associated with neutrophil activation, as reflected by a mean fivefold increase in the plasma concentrations of elastase-q-antitryp- sin complexes and a mean sevenfold increase in plasma lactoferrin levels. Serum neopterin, a marker of monocyte activation, was significantly increased 24 hours after the administration of TNF. These changes occurred in the absence of detectable complement activation, as indicated by unchanged C3a-desarg plasma values. Serum interleukin-6 showed a nearly 40-fold increase after TNF injection, whereas interleukin-1 remained undetectable throughout. We conclude that the systemic release of TNF, triggered early after invasive infection, may be involved in the alterations in circulating leukocyte numbers and in the activation of leukocytes, during the development of the septic syndrome. o 1992 by The American Society of Hematology. I TNF in these inflammatory reactions. For this purpose we NVASIVE BACTERIAL infection may give rise to the clinical syndrome of septicemia characterized by fever, hypotension, vascular leakage, and ultimately multiple organ failure.’ Several physiologically operative host defense mechanisms have been implicated in the development of this syndrome, including leukocytes, which may cause tissue injury by releasing toxic substances from their granules and reactive oxygen metabolites.’ The extent of neutrophil activation in septicemia has been shown to have a prognostic ~ignificance.’.~ In the past years it has become clear that invading bacteria trigger the production of small polypeptides, collectively termed cytokines, mainly by mononuclear and endothelial cells. Among these cytokines, tumor necrosis factor (TNF), interleukin-1 (IL-1), and IL-6 play an important role in the pathophysiology of septicemia? Several lines of evidence indicate that TNF is a critical factor in the initiation of the septic syndrome. Systemic TNF release is observed early after infusion of live bacteria in animals6and endotoxin in humans? and high serum levels of TNF are found in patients with sepsis.8Administration of recombinant TNF induces the septic syndrome in animals,” while monoclonal antibodies (MoAbs) directed against TNF prevent mortality in lethal sepsis models, concurrently attenuating the elaboration of IL-lp and IL-6 into the circulation.”’ Recent in vitro studies have shown interactions between the cytokine network and leukocytes, ie, cytokines are capable of activating a variety of leukocyte functions,” granulocytes can produce cytokine~,’~~’’ and cytokines can enhance the expression of complement receptors on leukoc y t e ~This . ~ ~ suggests that organ damage in septicemia may result from an interplay between these components of the immune system. We recently studied the kinetics of leukocyte activation after an intravenous injection of endotoxin into healthy Endotoxin induced a biphasic change in leukocyte counts involving initial neutropenia and subsequent neutrophilia, associated with degranulation of neutrophils as reflected by increases in the plasma concentrations of elastase-ai-antitrypsin complexes and la~toferrin.’~’~ Interestingly, these responses occurred in the absence of detectable complement activation.’ In the present Blood, Vol79, No 3 (February I ) , 1992: pp 693-698 investigation, we aimed to assess the role of circulating studied six healthy men in a saline-controlled cross-over fashion after a bolus intravenous injection of recombinant human TNF. MATERIALS AND METHODS The study was approved by the institutional research and ethics committees of the Academic Medical Center, University of Amsterdam, and written informed consent was obtained from all volunteers. All subjects were admitted to the Metabolic Research Ward and confined to bed during the 12-hour study period. Study design. The present study was performed simultaneously with investigations on the coagulative and endocrine effects of TNF, results of which have been published previ~usly.’~.’~ The outcomes of clinical parameters, ie, increases in body temperature, occurrence of chills, and the absence of hemodynamic changes were also reported in Six healthy male volunteers (age 27 to 33 years) participated in the study. Medical history, physical examination, and routine laboratory investigation were completely normal in all subjects. They did not use medication and had no febrile disease in the month before the study. Each study period started at 7:30 AM. The volunteers fasted overnight until the end of the study. Each subject was studied twice with an interval of at least 3 weeks. On one occasion a bolus From the Department of lnternal Medicine and the Center for Hemostasis, Thrombosis,Atherosclerosis and Inflammation Research, Academic Medical Center, University of Amsterdam; and the Central Laboratoiy of the Netherlands Red Cross Blood Transfusion Service and the Laboratoiy for Experimental and Clinical Immunology, University of Amsterdam, Amsterdam, The Netherlands. Submitted April 1,1991; accepted September 23, 1991. S.J.H.V.D.and H.R.B. are fellows of the Royal Netherlands Academy of Arts and Sciences. Address reprint requests to T. van der Poll, MD, Department of Internal Medicine, Academic Medical Center, F4-222, Meibergdreef 9, 1105 A 2 Amsterdam, The Netherlands. The publication costs of this article were defiayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C.section 1734 solely to indicate this fact. 0 1992 by The American Society of Hematology. 0006-497119217903-0014$3.00/0 693 VAN DER POLL ET AL 694 intravenous injection of recombinant human TNF of 50 pg/m2 dissolved in 10 mL of isotonic saline was administered; on the other occasion an equivalent volume of isotonic saline was administered. The order in which recombinant TNF and isotonic saline was given was determined by balanced assignment. Venous blood samples were obtained by separate venipunctures, with the use of 19-gauge butterfly needles, directly before the injection of recombinant TNF or isotonic saline and 15,30, and 45 minutes and 1, 2, 3, 4, 5, 6, 8, 10, and 12 hours thereafter. Additional samples were obtained 24 hours postinjection. Blood for the measurement of serum TNF concentrations was obtained immediately before the injection of recombinant TNF or saline and 5,10, 15,30,60, 120,180, and 240 minutes thereafter. Recombinant human TNF was kindly provided by Boehringer Ingelheim (Ingelheim am Rhein, Germany). It was more than 99% pure as determined by sodium dodecyl sulphate-polyacrylamide gel electrophoresis analysis and contained less than 10 ng of endotoxin per milligram of protein as tested by the limulus amoebocyte lysate assay. Assays. Leukocyte counts were determined in blood anticoagulated with K,-EDTA with the use of a flow cytometer (Technicon H1 system; Technicon Instruments, Tarrytown, NY). Leukocyte count differentials were determined both by flow cytometry and hand counting of peripheral blood smears, which showed identical results. Blood for the determination of elastase-a,-antitrypsin complexes, lactoferrin, and C3a-desarg was collected in siliconized Vacutainer tubes (Becton Dickinson, Plymouth, UK) to which EDTA (10 mmol/L) and Polybrene (Aldrich, Milwaukee, WI) (0.05%, wt/vol) were added to prevent any in vitro complex formation. Blood samples were centrifuged at 4°C for 20 minutes at 1,600g. The plasma concentrations of elastase-a,-antitrypsin complexes and lactoferrin were measured with a radioimmunoassay (RIA) that has been described in detail? Briefly, sepharose beads, to which polyclonal antibodies against human elastase or an MoAb against lactoferrin were coupled, were incubated with the samples to be tested. Elastase-a,-antitrypsin or lactoferrin bound to the beads was quantitated by incubation with '"I-MoAb against complexed a,-antitrypsin (RIA for elastase-a,-antitrypsin) or polyclonal I-antilactoferrin (RIA for lactoferrin). The plasma levels of elastase-a,-antitrypsin complexes and lactoferrin are expressed as nanograms per milliliter using preformed complexes and purified lactoferrin as standards, respectively. Complement activation was assessed by measuring the plasma concentrations of C3adesarg by an RIA as reported previously.18To prevent interference with native C3 in the assay, samples were incubated with polyethylene glycol before being tested. The results are expressed as nanomoles per liter. Serum for the determination of neopterin, TNF, IL-6, and IL-1 was prepared by centrifugation of clotted blood for 20 minutes at 1,600g (room temperature). The serum concentrations of neopterin were measured with an RIA (IMMUtest Neopterin; Henning, Berlin, Germany) and expressed as nanomoles per liter. The serum levels of TNF were determined by IRMA (Medgenix, Fleurus, Belgium) as described previously.16 Polypropylene tubes were coated with a combination of MoAbs to recombinant TNF that recognize distinct epitopes of TNF. The tubes were incubated overnight with a mixture of the sample to be tested and anti-TNF antibody labeled with '"I. After decantation, the bound fraction was counted in a gamma counter, and the level of TNF was expressed in picograms per milliliter in relation to a standard binding curve for recombinant TNF. The serum concentrations of IL-6 were measured using the B9 assay as described previously." Briefly, serum was heated for 30 minutes at 56°C and a titration of each serum was added to 5,000 B9 cells and compared with a standard IL-6 preparation. Serum IL-6 levels are expressed as units per milliliter, where 1 U/mL is the concentration that leads to half-maximal proliferation. One unit equals about 1pg of IL-6. The identity of IL-6 in positive sera was confirmed with a neutralizing antiserum to recombinant IL-6. The limit of detection of the B9 assay is 7 U/mL. Samples with values below the limit of detection were assigned a value of 7 U/mL. The serum concentrations of IL-1 were measured using the D10 assay as reported previously.*" D10 cells were incubated with serum in the presence of IL-2 (50 U/mL). Under these conditions 1 pg of IL-1 per milliliter causes half-maximal proliferation. Standard curves were generated by incubation with recombinant IL-la. The limit of detection of the D10 assay is 30 pg/mL. Statistical analysis. Values are given as means f SEM. Differences in results between the TNF and saline experiments were tested by analysis of variance and Newman-Keul's test for multiple comparison, as indicated. A P value <.05 was considered to represent a significant difference. RESULTS Leukocyte counts. Baseline leukocyte counts were similar and within normal limits in both study periods (Fig 1). TNF injection was associated with a biphasic change in total leukocyte counts, which largely reflected the change in the number of circulating neutrophils (both P < .0001 by analysis of variance). Marked initial decreases in total leukocytes and neutrophils were observed, reaching a nadir after 15 minutes. Total leukocytes dropped from 5.2 f 0.4 x 10y/Lat baseline to 1.2 2 0.1 x 10y/L;neutrophils from 2.6 f 0.3 X 10y/L to 0.2 & 0.04 X 10y/L. Early blood sampling in three subjects showed that the decrease in circulating neutrophils was already apparent as early as 5 minutes after TNF injection. The initial neutropenia was followed by a neutrophilia becoming significant after 1 hour. From this timepoint and onward band cells appeared in the circulation, with a maximum of 18% to 26% of circulating white blood cells after 2 to 4 hours. Total leukocyte and neutrophil counts peaked after 6 hours (12.9 f 1.3 x 10y/L and 11.9 ? 1.3 x 10y/L, respectively) and were still significantly elevated after 12 hours. Total leukocyte and neutrophil counts had returned to control values in samples obtained after 24 hours (data not shown). TNF administration also elicited a rapid and sustained lymphopenia (P < .0001 by analysis of variance), which reached a nadir after 5 hours (from 2.0 f 0.2 X 10y/Lat baseline to 0.3 ? 0.1 x 109/L).Lymphocytes remained decreased until the end of the 12-hour study period; 24 hours after TNF or saline injection lymphocyte counts were similar (data not shown). TNF induced a transient monopenia lasting 2 hours postinjection (P < .005 by analysis of variance). Minimal monocyte counts were observed after 15 minutes, when monocytes had almost completely disappeared from the peripheral blood (from 0.3 f 0.1 X 10y/L at baseline to 0.02 f 0.01 x 109/L). Neutrophil activation. Activation of neutrophils was assessed by measurements of the plasma concentrations of elastase-a,-antitrypsin complexes and lactoferrin. Preinjection values were similar in both study periods (Fig 2). TNF elicited sharp increases in the plasma levels of elastaseqantitrypsin complexes and lactoferrin, both becoming significant after 30 minutes and peaking after 3 hours. Elastase- TNF AND LEUKOCYTES 695 At baseline, neopterin levels were not different in both study periods (6.0 & 1.3 nmol/L before TNF; 5.3 f 0.4 nmol/L before saline), and they remained unchanged until 8 hours after the initial injections. Twelve hours after TNF injection a modest nonsignificant increase in serum neopterin was found compared with the control period (7.8 f 1.4 nmol/L v 5.8 f 1.2 nmol/L), which became significant 24 hours postinjection (8.7 & 0.8 nmol/L v 4.5 f 0.8 nmol/L). Complement activation. Activation of the complement system was monitored by measuring the plasma concentrations of C3a-desarg. As compared with saline, TNF did not affect C3a-desarg levels throughout the entire observation period (data not shown). Cytokines. The serum levels of TNF have been reported previously.’6 Briefly, TNF was not detectable in serum obtained at baseline or during the saline control period (Fig 3). After injection of recombinant TNF, the highest serum level was measured after 5 minutes (4,261 f 785 pg/mL). Thereafter, serum TNF concentrations decreased rapidly. Leukocytes (xlOO/l) 128- 40- Neutrophils (XIOO/l) 12- 84- - 0. Elastase -a,antltrypsin (ng/ml) Lymphocytes (xlOa/I) ‘1 - * * * * * * l5OI 0 Monocytes (XIOg/l) 0 0.6 J*I I 1 Lactoferrin (ng/ml) *T 0 2 4 6 8 1 0 1 *T 2 Tlme (hrs) Fig 1. Mean (kSEM) leukocyte counts after intravenous bolus injections of recombinant human TNF (50 pg/mZ; solid circles) or an equivalent volume of isotonic saline (open circles). Asterisks indicate statistical significance for the comparison of TNF with saline (P < .05 by Newman-Keul‘s test). a,-antitrypsin increased from 43 f 6 ng/mL at baseline to 223 f 28 ng/mL ( P < .0001 by analysis of variance); lactoferrin from 212 f 41 ng/mL to 1526 f 227 ng/mL (P < .0001 by analysis of variance). From 3 hours and onward gradual decreases in elastase-a,-antitrypsin and lactoferrin were observed, whereby the former remained elevated until the end of our 12-hour observation period. Monocyte activation. The serum concentrations of neopterin were determined as a measure of monocyte activation. , 0 2 4 6 a I . . 12 Time (hrs) Fig 2. Mean (+SEM) plasma concentrations of elastase-a,antitrypsin complexes and lactoferrin after intravenous bolus injections of recombinant human TNF (50 pglm’; solid circles) or an equivalent volume of isotonic saline (open circles). Asterisks indicate statistical significance for the comparison of TNF with saline (P < .05 by Newman-Keul’s test). VAN DER POLL ET AL 696 - 300 - 200 - 100 ‘I 0 2 4 8 . . -0 , 8 12 Tbne (Ius) Fig 3. Mean (+SEM) serum concentrations of IL-6 after intravenous bolus injection of recombinant human TNF (50 pg/mz; solid circles); IL-6 remained below the limit of detection (7 U/mL) in the saline control period. Asterisks indicatestatistical significancefor the comparison of TNF with saline (P < .05 by Newman-Keul‘s test). In addition, mean (+SEM) serum levels of TNF are shown (solid triangles) after injection of recombinant TNF. TNF was not detectable during the control period. Serum IL-6 concentrations were below the limit of detection (7 U/mL) in the saline control period. TNF induced an increase of serum IL-6 concentrations that became significant after 30 minutes (Fig 3). Serum IL-6 peaked after 2 hours (265 4 56 U/mL; P < .OW1 by analysis of variance). IL-1 activity was not detectable in serum during either study period (data not shown). DISCUSSION TNF is a pleiotropic protein that occupies a pivotal early role in the pathogenesis of the septic syndrome. In the course of septicemia, initiation of the cytokine network is followed by activation of other mediator systems, which is considered to importantly contribute to the development of the septic syndrome. Among these mediator systems, leukocytes are of particular interest. The objective of the present study was to evaluate the effects of circulating TNF on white blood cells. It was shown that intravenous injection of TNF induced marked changes in peripheral blood leukocyte counts, and activation of neutrophils as reflected by up to sevenfold increases in the plasma concentrations of elastase-a,-antitrypsin complexes and lactoferrin. An increase in neopterin serum levels after 24 hours indicated monocyte activation. TNF elicited an early decrease in circulating neutrophils that was already apparent after 5 minutes and reached a nadir after 15 minutes. Thereafter, neutrophil counts rapidly increased and a neutrophilia with immature forms developed. The initial neutropenia was most likely caused by adhesion of neutrophils to the vascular endothelium. In vitro TNF almost instantly enhances the adherence of neutrophils to cultured endothelial cells by increasing the expression of the CD 11/18 complex on the surface of neutrophils.” The neutrophilia from 1 hour and onward was probably due mainly to recruitment of marrow neutrophils, because in rats TNF-induced neutrophilia is associated with decreased neutrophil counts in the bone marrow.22Additionally, in cancer patients, labeled autologous leukocytes reinfused 15 minutes before TNF infusion rapidly disappeared from the circulation and did not return when leukocytosis developed.23 TNF injection also provoked a sustained lymphopenia, which may have been caused by enhanced lymphocyte adhesion to vascular endothelium secondary to expression of intercellular adhesion molecule 1 (ICAM-1) and vascular adhesion molecule 1 (VCAM-1) on the surface of endothelial cells by a direct action of TNF.24,25 Although IL-1 remained undetectable in the circulation after TNF injection, confirming previous findings in cancer patients infused with TNF in higher doses,26 cell-bound IL-1 may have been involved as a secondary mediator in the TNF-induced changes in circulating white blood cells as it shares many effects with TNF on the interaction between leukocytes and e n d o t h e l i ~ m . ~ ~ ~ ~ IL-6 does not affect the adhesive capacity of endothelial cells,x but has been shown to induce neutrophilia and a mild lymphopenia in rats in vivo.*’ Since, in the present study, serum IL-6 showed a nearly 40-fold increase after TNF injection, this cytokine may have contributed to altered neutrophil and lymphocyte counts observed several hours after the administration of TNF. Activation of neutrophils likely plays a pivotal part in the development of organ damage in septicemia. The capability of neutrophils to disrupt the normal architecture of tissues is derived from the combined cooperative action of released chlorinated oxidants and proteinases2 Elastase is a very potent proteinase, degrading almost all components of the extracellular matrix, as well as a variety of plasma proteins.28 Moreover, elastase is an important mediator of endothelial cell injury, resulting in vascular leakage.2yThe host’s primary defense against uncontrolled action of elastase is the proteinase inhibitor a,-antitrypsin, which rapidly and irreversibly binds to elastase, forming elastase-a,antitrypsin complexes. Lactoferrin is a glycoprotein from neutrophil specific granules. Several proinflammatory functions have been postulated for lactoferrin, including antimicrobicidal activity and regulation of neutrophil adhesiveness. Neutrophils secrete elastase and lactoferrin on stimulation with various agonists in vitro. As neutrophils are the predominant source of circulating and the exclusive source of circulating la~toferrin,~’ the plasma concentrations of these proteins are commonly used as a measure of neutrophil activation in vivo. In patients with sepsis, elevated plasma levels of elastase-a,-antitrpsin complexes and lactoferrin have been consistently f o ~ n d . 3 , ~ TNF induced marked increases in the plasma concentrations of both neutrophil markers, reaching significance after 30 minutes and peaking after 3 hours. TNF may have provoked this neutrophil degranulation directly,””’ at later stages possibly in concert with IL-6.33In addition, granulocyte-macrophage colony-stimulating factor (GM-CSF), an important stimulator of the proliferation and maturation of leukocytes, may have been involved because TNF induces the production of this protein by several cell types in vitro?4 697 TNF AND LEUKOCYTES We did not measure GM-CSF in serum because, to our knowledge, release of GM-CSF to the circulation has never been found in infectious or other diseases. Intravenous endotoxin has also been shown to induce increases in the plasma levels of elastaseq-antitrypsin and 1a~toferrin.l~’~ However, in these experiments the increase in elastase-a,-antitrypsin occurred only after 2 to 3 whereas lactoferrin started to increase after 90 minutes.15 The differential time courses of the increases in neutrophil markers after endotoxin and TNF injection indicate that degranulation of neutrophils in endotoxemia may proceed via endotoxin-induced TNF. These results, taken together with previous studies reporting that TNF stimulates respiratory burst activity of neutrophils in vitro36 and primes neutrophils for hypochlorous acid production in vivo? implicate this cytokine as an important factor in the activation of neutrophils in septicemia. Neopterin is exclusively released by activated monocytes and macrophages. Patients with septic shock have very high levels of neopterin in the circulation, which is interpreted to reflect monocyte activation?8 Our study establishes that TNF may play a role in this process. TNF induced an increase in neopterin serum concentrations, becoming significant after 24 hours, which contrasted with the rapid activation of neutrophils. It is likely that TNF stimulated neopterin release indirectly, as it does not affect the production of neopterin by monocytes in Severe septicemia is commonly associated with activation of the complement ~ystem.~’ Intravenous injection of TNF did not elicit complement activation, as indicated by unchanged plasma levels of C3a-desarg. This finding confirms our previous observation after injection of endotoxin into healthy subjects, that activation of granulocytes can occur in the absence of complement activati~n.’~’~ It is unlikely that our inability to detect complement activation was due to inappropriate sensitivity of the assay for C3a-desarg. Using the same assay we could readily detect activation of the complement system in several disease states, including sepsis3’ and after treatment with recombinant IL-2 in cancer patients:’ However, these patients were severely ill and showed signs of shock and multiple organ failure, which contrasts with the relatively mild clinical response to intravenous endotoxin and TNF in healthy subjects. Conceivably, complement activation only occurs in more severe clinical conditions. It remains to be established whether repeated and/or prolonged exposure to higher amounts of TNF does stimulate the complement cascade. In conclusion, this study shows that a single intravenous injection of TNF induces marked alterations in the peripheral blood counts and functional properties of leukocytes. These data substantiate the proximal role of TNF in the initiation of leukocyte activation in septicemia. ACKNOWLEDGMENT We are indebted to Dr Auguste Sturk and the other members of the staff of the coagulation laboratory for their excellent technical support; to Dr Frans J. Hoek for the determinations of the serum concentrations of TNF; to Dr Fanny Berends for analyzing peripheral blood smears; to Gerdie Wentink and Lida Stuiver for preparing the illustrations; and to Marieke Kat for secretarial assistance. REFERENCES 1. Harris RL, Musher DM, Bloom K, Gathe J, Rice L, Sugarman B, Williams TW, Young EJ: Manifestations of sepsis. Arch Intern Med 147:1895,1987 2. Weiss SJ: Tissue destruction by neutrophils. N Engl J Med 320:365,1989 3. Duswald K-H, Jochum M, Schramm W, Fritz H: Released granulocytic elastase: An indicator of pathobiochemical alterations in septicemia after abdominal surgery. Surgery 98:892, 1985 4. Nuijens JH, Abbink JJ, Wachtfogel YT, Colman RW, Eerenberg AJM, Dors D, Kamp AM, Strack van Schijndel RJM, Thijs LG, Hack CE: Plasma elastase-a,-antitrypsin and lactoferrin in sepsis: Evidence for neutrophils as mediators in fatal sepsis. J Lab Clin Med (in press) 5. Fong Y, Lowry S F Tumor necrosis factor in the pathophysiology of infection and sepsis. Clin Immunol Immunopathol 55:157, 1990 6. Hesse DG, Tracey KJ, Fong Y, Manogue KR, Palladino MA Jr, Cerami A, Shires GT, Lowry SF: Cytokine appearance in human endotoxemia and primate bacteremia. Surg Gynecol Obstet 166:147, 1988 7. van Deventer SJH, Bdller HR, ten Cate JW, Aarden LA, Hack CE, Sturk A Experimental endotoxemia in humans: Analysis of cytokine release and coagulation, fibrinolytic and complement pathways. Blood 76:2520,1990 8. Waage A, Halstensen A, Espevik T Association between tumour necrosis factor in serum and fatal outcome in patients with meningococcal disease. Lancet 1:355,1987 9. Tracey KJ, Beutler B, Lowry SF, Merryweather J, Wolpe S, Milsark IW, Harir RJ, Fahey TJ 111, Zentella A, Albert JD, Shires GT, Cerami A: Shock and tissue injury induced by recombinant human cachectin. Science 234:470,1986 10. Fong Y, Tracey KJ, Moldawer LL, Hesse DG, Manogue KR, Kenney JS, Lee AT, Kuo GC, Allison AC, Lowry SF, Cerami A: Antibodies to cachectin/tumor necrosis factor reduce interleukin l p and interleukin 6 appearance during lethal bacteremia. J Exp Med 170:1627,1989 11. Steinbeck MJ, Roth J A Neutrophil activation by recombinant cytokines. Rev Infect Dis 11549,1989 12. Dubravec DB, Spriggs DR, Mannick JA, Rodrick M L Circulating human peripheral blood granulocytes synthesize and secrete tumor necrosis factor a.Proc Natl Acad Sci USA 87:6758, 1990 13. Cicco NA, Lindemann A, Content J, Vandenbussche P, Lubbert M, Gauss J, Mertelsmann R, Herrmann F: Inducible production of interleukin-6 by human polymorphonuclear neutrophils: Role of granulocyte-macrophage colony-stimulating factor and tumor necrosis factor-alpha. Blood 75:2049,1990 14. Berger M, Wetzler EM, Wallis RS: Tumor necrosis factor is the major monocyte product that increases complement receptor expression on mature human neutrophils. Blood 71:151, 1988 15. van Deventer SJH, Hack CE, Wolbink GJ, Voermans HJ, Strack van Schijndel RJM, ten Cate JW, Thijs LG: Endotoxininduced neutrophil activation. The role of complement revisited. Prog Clin Bioi Res 367:101, 1991 16. van der Poll T, Buller HR, ten Cate H, Wortel CH, Bauer KA, van Deventer SJH, Hack CE, Sauenvein HP, Rosenberg RD, 698 ten Cate JW: Activation of coagulation after administration of tumor necrosis factor to normal subjects. N Engl J Med 3221622, 1990 17. van der Poll T, Romijn JA, Wiersinga WM, Sauerwein HP: Tumor necrosis factor: A putative mediator of the sick euthyroid syndrome in man. J Clin Endocrinol Metabol71:1567,1990 18. Hack CE, Paardekoper J, Eerenberg AJM, Navis GO, Nijsten MWN, Thijs LG, Nuijens JH: A modified competitive inhibition radioimmunoassay for the detection of C3a. Use of '=I-C3 instead of '"I-C3a. J Immunol Methods 107:77,1988 19. Aarden LA, de Groot ER, Schaap OL, Lansdorp PM: Production of hybridoma growth factor by human monocytes. Eur J Immunoll7:1411,1987 20. Helle M, Boeije L, Aarden LA: Functional discrimination between interleukin 6 and interleukin 1. Eur J Immunol 18:1535, 1988 21. Gamble JR, Harlan JM, Klebanoff SJ, Vadas MA: Stimulation of the adherence of neutrophils to umbilical vein endothelium by recombinant human tumor necrosis factor. Proc Natl Acad Sci USA 828667,1985 22. Ulich TR, del Castillo J, Keys M, Granger GA, Ni R-X: Kinetics and mechanisms of recombinant human interleukin 1 and tumor necrosis factor-a-induced changes in circulating numbers of neutrophils and lymphocytes. J Immunoll393406,1987 23. Schell-Frederick E, Tepass T, Lorscheidt G, Pfreundschuh M, Schaadt M, Diehl V: Effects of recombinant tumor necrosis factor (rHuTNFa) on human neutrophils and monocytes: In vitro, exvivo and in vivo. Eur J Hematol43:286,1989 24. Bevilacqua MP, Pober JS, Mendrick DL, Cotran RS, Gimbrone MA Jr: Identification of an inducible endothelial-leukocyte adhesion molecule. Proc Natl Acad Sci USA 84:9238,1987 25. Carlos TM, Schwartz BR, Kovach NL, Yee E, Rosso M, Osborn L, Chi-Rosso G, Newman B, Lobb R, Harlan JM: Vascular cell adhesion molecule-1 mediates lymphocyte adherence to cytokine-activated cultured human endothelial cells. Blood 76:965, 1990 26. Starnes H F Jr, Warren RA, Jeevanandam M, Gabrilove JL, Larchian W, Oettgen HF, Brennan M F Tumor necrosis factor and the acute metabolic response to tissue injury in man. J Clin Invest 82:1321,1988 27. Ulich TR, del Castillo J, Guo K In vivo hematologic effects of recombinant interleukin-6 on hematopoiesis and circulating numbers of RBCs and WBCs. Blood 73:108,1989 28. Janoff A Elastase in tissue injury. Annu Rev Med 36:207, 1985 VAN DER POLL ET AL 29. Smedley LA, Tonnesen MG, Sandhaus RA, Haslett C, Guthrie LA, Johnston RB Jr, Henson PM, Worthen GS: Neutrophil-mediated injury to endothelial cells. Enhancement by endotoxin and essential role of neutrophil elastase. J Clin Invest 77:1233,1986 30. Bennet RM, Kokocinski T Lactoferrin turnover in man. Clin Sci 57:453,1979 31. Koivuranta-Vaara P, Banda D, Goldstein IM: Bacteriallipopolysaccharide-induced release of lactoferrin from human polymorphonuclear leukocytes: Role of monocytes-derived tumor necrosis factor a.Infect Immun 55:2956, 1987 32. Burnett D, Chamba A, Hill SL, Stockley R A Effects of plasma, tumour necrosis factor, endotoxin and dexamethason on extracellular proteolysis by neutrophils from healthy subjects and patients with emphysema. Clin Sci 77:35,1989 33. Borish L, Rosenbaum R, Albury L, Clark S: Activation of neutrophils by recombinant interleukin 6. Cell Immunol 121:280, 1989 34. Gasson JC: Molecular physiology of granulocyte-macrophage colony-stimulating factor. Blood 77:1131, 1991 35. Suffredini AF, Harpel PC, Parillo JE: Promotion and subsequent inhibition of plasminogen activation after administration of intravenous endotoxin to normal subjects. N Engl J Med 3201165, 1989 36. Larrick JW, Graham D, Toy K, Lin LS, Senyk G, Fendly BM: Recombinant tumor necrosis factor causes activation of human granulocytes. Blood 69:640,1987 37. Wewers MD, Rinehart JJ, She 2-W, Herzyk DJ, Hummel MM, Kinney PA, Davis WB: Tumor necrosis factor infusions in humans prime neutrophils for hypochlorous acid production. Am J Physiol259L276,1990 38. Troppmair J, Nachbaur K, Herold M, Aulitzky W, Tilg H, Gastl G, Bieling P, Kotlan B, Flener R, Mull B, Aulitzky WO, Rokos H, Huher C: In-vitro and in-vivo studies on the induction of neopterin biosynthesis by cytokines, alloantigens and lipopolysaccharide (LPS). Clin Exp Immunol74:392,1988 39. Hack CE, Nuijens JH, Felt-Bersma RJF, Schreuder WO, Eerenberg-Belmer AJM, Paardekooper J, Bronsveld W, Thijs LG: Elevated plasma levels of the anaphylatoxins C3a en C5a are associated with a fatal outcome in sepsis. Am J Med 86:20,1989 40. Thijs LG, Hack CE, Strack van Schijndel RJM, Nuijens JH, Wolbink GJ, Eerenberg-Belmer AJM, van der Val1 H, Wagstaff J: Activation of the complement system during immunotherapy with recombinant IL-2. Relation to the development of side effects. J Immunol144:2419,1990








© Copyright 2026