
HEART-REACTIVE ANTIBODY, VIRAL ILLNESS, AND THE
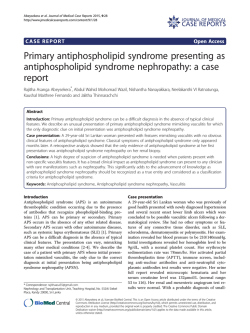
HEART-REACTIVE ANTIBODY, VIRAL ILLNESS, AND THE POSTPERICARDIOTOMY SYNDROME Correlates of a Triple-Blind, Prospective Study By MARY ALLEN ENGLE, M.D.* AND (BY INVITATION) JOHN B. ZABRISKIE, M.D.** AND LAURENCE B. SENTERFIT, D.Sc.*** NEW YORK The postpericardiotomy syndrome (PPS) is a common postoperative event that occurs in 20-30% of patients following cardiac surgery in which the pericardium is entered. '3 The syndrome is recognized by the presence, or by the persistence, beyond the first postoperative week of f'ever and signs of pericardial and often pleural reaction, sometimes with effusions. Rarely it recurs late postoperatively. Aside from the discomfort and prolongation ot' postoperative morbidity that it causes, its significance lies in the confusion with other causes of postoperative fever (such as endocarditis, the postperfusion syndrome of lymphocytosis and hepatosplenomegaly,45 atelectasis, or pneumonia) or of cardiomegaly (such as cardiac failure). Diagnosis is made by excluding these conditions as well as by identifying signs of the syndrome.6 Presently, management of this self'-limited but sometimes prolonged illness is entirely empiric since the cause is not known. In mild instances rest in bed is ef'fective management. In the sick patient, with large pericardial eff'usion, pericardiocentesis may be required for cardiac tamponade. Therapy with salicylates or with steroids has been employed with varying results. A similar syndrome occurs following myocardial infarction7 and after penetrating8' 9 or blunt10 pericardial trauma. Features common to these three settings for the syndrome (intrapericardial surgery or trauma or myocardial infarction) include damage to heart muscle and the opportunity for intrapericardial bleeding. Two theories proposed for etiology of the syndrome are that it represents i!n autoimmune reaction or that it is a viral illness.2 3 10 11 Possibly both factors are involved: an inapparent virus in the host may * Department of Pediatrics, The New York Hospital-Cornell University Medical College. New York New York 10021 ** Rockefeller University, New York, New York 10021 *Department of Microbiology, The New York Hospital-Cornell University Medical College, New York, New York 10021 This work was supported by NHLI Research Grant #1 ROI HL 16246 147 148 ENGLE, ZABRISKIE AND SENTERFIT be activated by the trauma of surgery and an organ-antibody reaction may result. We have had an opportunity to test these hypotheses. PLAN OF STUDY Subjects for the investigation were consecutive, longterm survivors of intrapericardial surgery in the pediatric age group. Concurrent analyses were made on a triple-blind basis preoperatively and postoperatively at prescribed intervals in the hospital and after discharge, for circulating antiheart and antiviral antibody and of clinical signs of the syndrome. The samples of blood were obtained the day before surgery and postoperatively on the seventh and tenth days, in the third and fifth weeks and additionally as indicated. The antiheart antibody was determined from serum by an immunofluorescent technique and was ranked 0 to 4+, based on intensity of staining. On the same sample of serum in which heart-reactive antibody was determined, complementfixation studies were performed to a battery of eight viruses (adenovirus, Coxsackie B 1-6, cytomegalovirus) and to Mycoplasma pneumoniae. Clinical course of the patients was evaluated by at least two pediatric cardiologists, one of whom was the principal investigator, and presence or absence of the syndrome was noted. When present, as judged by strict criteria, it was rated mild, moderate, or severe, depending on duration and intensity of manifestations. Physical examination was performed daily in the hospital and on visits for postoperative followup. Electrocardiogram and teleoroentgenogram of' the chest were obtained according to the schedule for blood sampling. Echocardiogram was recorded when pericardial effusion was suspected. All parameters of postoperative care were maintained as standard as possible. Antibiotics were administered for the f'irst five days and not thereafter, unless in a rare circumstance there was clear evidence of' a bacterial infection. In the first 100 patients, ambulation was delayed until the patient was afebrile for 48 hours; earlier ambulation as tolerated was permitted in subsequent patients. Diuretics (furosemide) were used in most patients with effusions. Neither salicylates nor steroids were employed except in twelve subjects with severe syndrome, to be mentioned later. Patients were discharged when they were afebrile for two days on ambulation and effusions were subsiding. In a pilot study prior to undertaking this investigation we looked for the development of' antiheart antibody in a control group of' patients undergoing surgery that was intrathoracic but not intrapericardial, or that involved extensive muscle injury or that required large volumes of transfused blood. In addition, during the course of' this study, we performed immunologic studies on approximately 40 patients with POSTPERICARDIOTOMY SYNDROME 149 pericarditis of other etiology (uremia, rheumatoid arthritis, or of unknown origin), and with miscellaneous conditions such as collagen disorder, cardiomyopathy, bacterial endocarditis, and rheumatic fever. Included were four with postmyocardial infarction syndrome and one with postpericardial trauma syndrome. RESULTS Clinical Evaluation.-Of 300 consecutive survivors of intrapericardial surgery, 83 patients had the postpericardiotomy syndrome (PPS). It was judged to be mild in one third, moderate in slightly more and severe in slightly less than one third of the patients. The last abnormality to disappear was electrocardiographic evidence of pericarditis. Four patients were readmitted within a month of discharge because of exacerbation of the syndrome. Three of these presented as severely ill children with cardiac tamponade. Immunologic Studies.-Preoperative sera and control sera were negative for heart-reactive antibody. However, in 191 subjects an antibody appeared toward the end of the first week. In 89, the staining was greater than 2+ and the antibody could ')e detected into the second month or beyond. This response was called positive. In 102 patients, the antibody rise began at the same time but the staining was less intense, and the antibody disappeared after one month (intermediate group). In the sera of the other nonoperated patients studied, heart-reactive antibody in high titer developed during the course of the illness only in the few patients with postmyocardial infarction syndrome and in the one child with postpericardial trauma syndrome. The antiheart antibody (AHA) was specific for cardiac and for skeletal muscle but it was not species specific for human cardiac muscle. There was little binding to smooth muscle and none to other organs such as lung, liver, thymus, spleen, or kidney. Unlike the heart-reactive antibody demonstrated in patients with rheumatic fever which binds to Group A streptococcal membrane, this antiheart antibody did not. Virologic Studies.-In 180 patients studied, an elevation of viral titer to one or more viruses was measured in 76 subjects. Twenty-five had a high titer on admission that did not change during the course, whereas 51 had a four-fold or greater rise in titer and then decline during the period of observation. Correlation of Triple-Blind Data.-Results of clinical evaluation of PPS and determination of antiheart antibody were compared in each patient, as in Figure 1. When the comparisons for all subjects were analyzed, it was found that none of the patients with negative antiheart antibody had the syndrome 150 ENGLE, ZABRISKIE AND SENTERFIT MODERATE P. P.S - S. V., T, TEMPERIATURLDG. U 37L us X / ++++++ FRICTION fr PLE L IFFU 4.moo ,0O-c o + + a.O PtER1CAIAUFUI.II . .. .. F.. +a+ + . o O + .( 51:iI I ANTAIERT 2 1 r . * .' ..X. AI 25 'A ,AXe, F.& *.r:: FIG. 1. Graph of hospital course and the month after discharge of a child operated upon f'or tetralogy of' Fallot. Postoperative fever persisted for four weeks, while pericardial friction rub was present in the second postoperative week and signs of pericardial effusion appeared on the fifth postoperative day and disappeared after three weeks. Pleural effusion was present from the tenth to sixteenth days. The elevated white blood cell count dropped below 10,000 at the end of three weeks. Heart-reactive antibody, negative preoperatively and on the fourth postoperative day rose to 2+ or higher by the eighth day, declined in the third week and disappeared by one month postoperatively. whereas all of' those with positive antibody had PPS (Figure 2). There does indeed appear in the serum of certain postoperative subjects a heart-reactive antibody that correlates closely with clinical evidence of the PPS. A striking difference was noticed in incidence of syndrome and in antiheart antibody between the inf'ants one year of age or less and those two years of' age and older (Figure 3). Only one baby out of 74 had the syndrome and positive antibody, an incidence of' 1.3%. Beyond two years, the incidence was comparable at all ages, ranging from 29 to 40%. One difference between the babies and those older than two years is the relatively brief' opportunity for exposure to viral illness in the infants. POSTPERICARDIOTOMY SYNDROME 151 Among the 180 patients tested for antibody to viruses were 25 patients who had antibody to one or more viruses prior to surgery but no change throughout the period of study. They were evenly distributed among the three types of responses to antiheart antibody. They constituted 17-19% of those with negative, intermediate, and positive response. In contrast were 51 children in whom a significant rise, four-f'old or greater, and then a drop in titer occurred. This rise was observed in 5% of patients with negative antiheart antibody and no syndrome; in 16% of those with intermediate antiheart antibody and no syndrome; but in 80% of subjects with positive AHA and with the syndrome (Figure 4). The numbers of patients with a significant rise in titer to each viral agent and the percentage who had postpericardiotomy syndrome are shown in Figure 5. Most had no detectable antiviral antibody prior to surgery. In six subjects there was demonstrable titer to Mycoplasma pneumoniae but no rise in titer. Among the 51 patients with a significant rise in viral titer, this elevation was to one agent only in 24 but to 2 agents in five children, to 3 viruses in another 3 patients, and to 4 agents 257 PATIENTS 4 Severe (16) PPS SYNDROME Moderate (28)* Mild (22)E None (191) 100 L LU 80 a cD - & 60 E Z 40 20 n 11, Negaulve iniermeaiate Positive ANTIHEART ANTIBODY FIG. 2. In the first 257 consecutive survivors, none of the subjects with negative antiheart antibody had clinical syndrome, whereas all with positive antiheart antibody had the syndrome. It was severe in 16 and moderately so in 28. Among those with intermediate rise of antibody were two with mild syndrome. These same results now extend to 300 consecutive survivors. AGE DISTRIBUTION OF 257 OPERATED PATIENTS M-1 out syndrome (191) syndrome (66) 80 , 60 0 a 9O E 40 z 20 - ...... nv 0-1 2-5 6-10 11-15 16 &> Age in years FIG. 3. The relationship of age to the occurrence of the postpericardiotomy syndrome is such that babies aged less than two years have a low incidence of only 1.6% of the postoperative complication, whereas the incidence in the pediatric age groups beyond two years is about the same, 30-40%. ANTIHEART ANTIBODY AND RISE IN VIRAL TITER IN 137 PATIENTS bu a. 50 5% | No rise in titer (106) Rise in titer (31: 15% t1 _ 40 L- o * E 30 M 20 10 n v Negative Intermediate rositive FIG. 4. In 137 patients with concurrent measurement of antiheart and antiviral antibody, only 5%, of those with negative antiheart antibody (AHA) and no postpericardiotomy syndrome had a significant rise in titer to one or more viral agents, whereas 68% of those with positive AHA and with postpericardiotomy syndrome had a fourfold or greater rise in titer. In those with intermediate AHA, 15% had a rise in antiviral antibody (AVA). 152 153 POSTPERICARDIOTOMY SYNDROME RISE IN TITER, VIRAL AGENTS IN 137 PATIENTS n1'1 without syndrome (10) A?O PPS syndrome (2 71% 7_ 71-To 67% El LA r_6 .T I a 'a a. z 0 /aoenuvirus A J I £ 4 Coxsackie B A :2 0 r, Cytomegalo- virus FIG. 5. In 137 patients with concurrently measured AHA and AVA in figure 4, the numbers of patients with postpericardiotomy syndrome and with a significant rise in titer to specific viral agents tested are approximately the same. Though none of the first 137 tested had a measurable rise to Coxsackie B4, several of the more recently studied subjects did have. (cytomegolovirus or adenovirus and several of the Coxsackie B group) in two subjects. No patient in the first 137 studied showed a rise to Coxsackie B 4, but 11 of the next 43 patients studied this spring and summer showed a four-f'old or greater rise to this agent. The data obtained suggested the possibility of' viral invasion, or reactivation of latent virus, of cardiac muscle at the time of surgery. Types of Surgery Performed.-We questioned whether the type of operation and the amount of' myocardial trauma incident to the repair bore any relation to incidence of' the syndrome. The same types of operation were performed in all age groups (Figure 6). The most frequent anomaly operated upon was tetralogy of Fallot, in which a right ventriculotomy was performed for excision of infundibular pulmonic stenosis and f'or closure of' the ventricular septal defect with a patch of tef'lon f'elt. Next most common was atrial septal defect. There appeared to be no difference in the response of patients with a simple secundumtype defect and those with an ostium primum who had a cleft in the mitral valve sutured at the same time; so these two types of atrial septal defect were combined for the analysis. Surgical repair was through a right atriotomy. A teflon felt patch was used to close all the primum defects and for the large secundum defects. Simple ventricular septal defect (VSD), closed with a teflon f'elt patch and usually through a small right ventriculotomy, was the next most common anomaly; while repair of' a VSD plus some other lesion such as transposition and/or pulmonic stenosis was the fourth most common surgical procedure. In the patients with immunologic and with virologic studies (Figure 6), those with repair 154 ENGLE, ZABRISKIE AND SENTERFIT OPERATION & POSITIVE ANTI HEART ANTIBODY 257 PATIENTS 60 144%) Without sydrome *17%) m0 PPS syndrome 40 12% 39% 30 0% 20 18% EL10 E 0 40 31% OPERATION & VIRAL RISE 137 PATIENTS II 6%39 ~~9% 30 20 ~~$0% 10 10 Tetralogy ASD VSD only VSD plus TGA only Valvar PS FIG. 6. The types of operations most frequently performed are shown in order of decreasing frequency at the bottom of the figure. The percentage with postpericardiotomy syndrome is indicated at the bottom of each bar for the 257 measured AHA (at top of figure) and for the 137 with concurrently measured AVA (bottom portion of figure). The syndrome occurred with higher frequency in those with tetralogy of Fallot and with ventricular septal defect plus some other anomaly than it did in those wherein there was less damage to cardiac muscle (ASD=atrial septal defect; VSD only=ventricular septal defect; TGA=transposition of great arteries undergoing emplacement of intrapericardial baffle; valvar PS = valvar pulmonic stenosis undergoing pulmonary valvotomy via a pulmonary arteriotomy). of tetralogy of Fallot and of VSD plus another lesion (the two conditions with the greatest potential for myocardial trauma) had the highest incidence of the syndrome, while none of those with only transposition of the great arteries repaired by use of an intra-atrial pericardial baffle had the PPS. Management.-In a self-limited condition of' uncertain etiology, it is difficult to judge the effect of treatment, such as rest and diuretics and the two modalities often recommended: salicylates or steroids. Early ambulation as tolerated, in contrast to that which was delayed until the child was afebrile for 48 hours, did not increase the incidence of the syndrome in the last 190 patients as compared with the first 110 POSTPERICARDIOTOMY SYNDROME 155 individuals in the study. However, when they were febrile or did not feel well with the syndrome, some of the children permitted early ambulation voluntarily limited their activity. We do not think it advisable for patients with moderate or large effusion to be active; three patients discharged with decreasing pericardial effusion returned critically ill with pericardial tamponade. Effect of salicylates and steroids.-It is the group of patients with severe illness who are of particular concern for optimal management. We studied the clinical response and the effect on antiheart antibody in 12 such patients. Six patients who received salicylates for several weeks soon became afebrile and began to improve gradually. The heart-reactive antibody did not drop immediately but instead, followed the usual curve of decline. Six other patients who received steroids in the form of prednisone in a dose of 2 mgm./kg. the first week, half that for the second week, and a quarter of that for the third week before the medication was discontinued, had a more impressive response. Promptly the clinical manifestations subsided, and the antiheart antibody dropped to intermediate levels and disappeared earlier than expected. Prevention.-We know of no means as yet of prevention of the syndrome in an individual patient undergoing intrapericardial surgery. In one boy with vascular hemophilia, steroids in therapeutic dosage were administered for one week prior to repair of his tetralogy of Fallot and in diminishing doses for the first postoperative week. Nonetheless in the second and third weeks he developed moderately severe syndrome with high titer of antiheart antibody. Avoidance of the complication, with reduction in overall incidence of the condition, has come about recently with the trend to early open repair of severe congenital cardiovascular anomalies in infancy, the period when there is the least likelihood of developing postpericardiotomy syndrome. DISCUSSION Antibodies which react to nonhuman myocardium were detected in patients with the PPS by Robinson and Brigden12 and by van der Geld13 in a manner similar to the finding by Kaplan14 and by Zabriskie et a 15 of heart-reactive antibody associated with rheumatic fever. Kaplan and Frengley16, Fowler"7, Kirsh and associates"8, Roberts and Lessof19, Das et al20, as well as Roses, Rose and Rappaport2I have presented thoughtful reviews on the topic of autoimmunity of the heart and the possible connection to the postpericardiotomy syndrome. Our early studies on antiheart antibody confirm an association.22 Concerning the question of the role of viruses, Kahn et al thought Parainfluenza virus, strain 3, might be significant in pathogenesis of the 156 ENGLE, ZABRISKIE AND SENTERFIT syndrome.23 In 1970 Burch and Colcolough suggested from their work with cardiotropic viruses that the syndrome might be caused by reactivation of a latent virus infection when there is trauma to myocardium.24 Lerner, Wilson, and Reyes in 1975 reviewed the subject of enteroviruses and the heart and especially emphasized the probably rolc of Coxsackie viruses, Group B, Types 15. 2 They set forth criteria for establishing an association of' a virus infection with an acute or chronic myocardiopathy.26 SUMMARY AND CONCLUSIONS This study has demonstrated that a heart-reactive antibody appears in the serum of' some patients undergoing intrapericardial surgery and that its presence in high titer correlates with clinical evidence of the syndrome. This correlation is sufficiently high that it constitutes a diagnostic test. Furthermore, a rise in viral titer to one or more of the eight viruses tested occurred in 80% of the patients with the syndrome but in only 5% and 16% of those with no syndrome and negative or intermediate levels respectively of heart-reactive antibody. The freedom from the syndrome in infants may be related to their short period of' experience with exposure to viruses and to viral illness; so they do not react immunologically to this new stress by having the postpericardiotomy syndrome. The greater chance of' having the syndrome with elevation of antiheart antibody and rise in titer that patients with tetralogy of Fallot (large VSD and severe pulmonic stenosis) or with VSD plus some other anomaly showed may be due to a greater amount of myocardial injury in those situations than in the other operations, resulting in greater release of potential antigens. It is interesting that the last clinical sign of the syndrome to disappear is the electrocardiographic abnormalities and that the antibody is still present but in diminished amounts at this time. Just as the elevation of temperature and white blood cell count seem to parallel one another, so too do the electrocardiographic abnormalities and elevation of antiheart antibody. The eff'ect of' steroids in apparently shortening the course of illness and depressing the level of' antiheart antibody suggests that prednisone halted antibody production and that we measured the decline of' the antibody that had already been produced. While it is possible that neither the appearance of antiheart antibody nor the rise in viral titer has any connection with the syndrome or with each other; it seems to us that a reasonable working hypothesis at this time is as f'ollows. The postpericardiotomy syndrome is the result of an immunologically determined response of' the epicardial layer of myocar- POSTPERICARDIOTOMY SYNDROME 157 dium, with inf'lammation and effusion and with "neighborhood" involvement of pleura. Heart-reactive antibody in high titer appears in the sera of' a certain number of individuals (25-30%) who because of their age and previous immunologic experience react to epicardial and myocardial injury incurred at pericardiotomy. This reaction may be triggered by a latent or fresh viral illness. REFERENCES 1. JANTON, 0. H., GLOVER, R. P., O'NEIL, T. J. E., AND FROlo, G. F.: Results of the surgical treatment of mitral stenosis. Circulation 6: 321, 1952. 2. ITO, T., ENGLE, M. A. AND GOLDBERG, H. P.: Postpericardiotomy syndrome following surgery for nonrheumatic heart disease. Circulation 17: 549, 1958. 3. ENGLE, M. A. AND ITO, T.: The postpericardiotomy syndrome. American Journal of Cardiology 7: 73, 1961. 4. HOLSWADE, G. R., ENGLE, M. A., REDO, S. F., GOLDSMITH, E. AND BARONDESS, J. A.: Development of viral diseases and viral disease-like syndrome after extracorporeal circulation. Circulation 27: 812, 1963. 5. ENGLE, M. A. AND MARX, N. R.: The postpericardiotomy and postperfusion syndromes. Heart Bulletin 14: 33, 1965. 6. ENGLE, M. A.: PostQperative syndromes. In Moss, A. F. and Adams, F. H.: Heart Disease in Infants and Children, Baltimore, The Williams and Wilkins Co., 1968, pp. 1087-1101. 7. DRESSLER, W.: Post-myocardial-infarction syndrome: preliminary report of complication resembling idiopathic, recurrent, benign pericarditis. Journal of the American Medical Association 160: 1379, 1956. 8. PETER, R. H., WHALEN, R. E., ORGAIN, E. S. AND MCINTOSH, H. D.: Postpericardiotomy syndrome as a complication of percutaneous left ventricular puncture. American Journal of Cardiology 17: 175, 1966. 9. SEGAL, F. AND TABATZNIK, B.: Postpericardiotomy syndrome following penetrating stab wounds in the chest: comparison with the postcommissurotomy syndrome. American Heart Journal 59: 175, 1960. 10. GOODKIND, M. J., BLOOMER, W. E. AND GOODYER, V. N.: Recurrent pericardial effusion after nonpenetrating chest trauma. Report of two cases treated with adrenocortical steroids. New England Journal of Medicine 263: 874, 1960. 11. DRUSIN, L. M., ENGLE, M. A., HAGSTROM, J. W. C. AND SCHWARTZ, M. S.: The postpericardiotomy syndrome. A six-year epidemiologic study. New England Journal of Medicine 272: 597, 1965. 12. ROBINSON, J. F. AND BRIGDEN, W.: Immunological studies in the post-cardiotomy syndrome. British Medical Journal 2: 706, 1963. 13. VAN DER GELD, H.: Anti-heart antibodies in the postpericardiotomy and the postmyocardial-infarction syndromes. Lancet 2: 617, 1964. 14. KAPLAN, M. H.: The cross-reaction of Group A Streptococci with heart tissue and its relation to induced autoimmunity in rheumatic fever. Bulletin of Rheumatic Disease 9: 560, 1969. 15. ZABRISKIE, J. B., Hsu, K. C. AND SEEGAL, B. C.: Heart-reactive antibody associated with rheumatic fever: characterization and diagnostic significance. Clinical and Experimental Immunology 7: 147, 1970. 16. KAPLAN, N. J. AND FRENGLEY, J. D.: Autoimmunity to the heart in cardiac disease, current concepts of the relation of autoimmunity to rheumatic fever, postcardiotomy 158 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. ENGLE, ZABRISKIE AND SENTERFIT and postinfarction syndromes and cardiomyopathies. American Journal of Cardiology 24: 459, 1969. FOWLER, N.: Editorial: Autoimmune heart disease. Circulation 44: 159, 1971. KIRSH, M. M., McINTosH, K., KALM, D. R., AND SLOAN, H.: Postpericardiotomy syndrome. Annals of Thoracic Surgery 9: 158, 1950. ROBERTS, C., AND LESSOF, M. H.: Immunological aspects of cardiovascular disorders. In, Progress in Cardiology II (Yu, P. N., Goodwin, J. F., ed.) Philadelphia, Lea and Febiger, 1973, pp. 31-48. DAS, S. K., CASSIDY, J. T., AND PErrY, R. E.: The significance of heart-reactive antibodies in heart disease. Critical review. Chest 66: 179, 1974. RoSES, D. F., RoSE, M. R., AND RAPPAPORT, F.: Febrile responses associated with cardiac surgery. Relationships to the postpericardiotomy syndrome and to alerted host immunologic reactivity. Journal of Thoracic and Cardiovascular Surgery 67: 251, 1974. ENGLE, M. A., MCCABE, J., EBERT, P. A. AND ZABRISKIE, J. B.: The postpericardiotomy syndrome and antiheart antibodies. Circulation 49: 104, 1974. KAHN, D. R., ERTEL, P. Y., MURPHY, W. H., KIRSH, M. M., VATHAYANON, S., STERN, A. M. AND SLOAN, H.: Pathogenesis of the postpericardiotomy syndrome. Journal of Thoracic and Cardiovascular Surgery 54: 682, 1967. BURCH, G. E., AND COLCOLOUGH, H. L.: Postcardiotomy and postinfarction syndrome-A theory. American Heart Journal 80: 290, 1970. LERNER, M. A., WILSON, F. M. AND REYES, M. P.: Enteroviruses and the heart (with special emphasis on the probable role of Coxsackievirus, Group B, Types 1-5) I. Epidemiological and experimental studies. Modern Concepts of Cardiovascular Disease 44: 7, 1975. IDEM: Enteroviruses and the heart (with special emphasis on the probable role of Coxsackieviruses, Group B, Types 1-5) II. Observations in humans. Modern Concepts of Cardiovascular Disease 44: 11, 1975. DISCUSSION DR. JOHN MERRILL (Boston): Have you attempted to see whether specific viral antibody in any of the viruses you mentioned will block immunofluorescence to your specific heart reactive antibody? DR. ENGLE: That's a very good question. This is an ongoing prospective study, and we do hope to do that. We have not as yet. DR. NOBLE 0. FOWLER (Cincinnati): This is an area that interests us very much. As Dr. Engle knows, there are several types of heart and pericardiol damage that may look rather similar to the post-pericardiotomy syndrome. These include the so-called idiopathic pericarditis syndrome, the Dressler syndrome, and post-radiation syndrome. It is of interest to us that living in an area where people occasionally get a little bit excited, we have observed instances of the same syndrome following both direct and indirect trauma to the heart of a nonsurgical nature. The syndrome may follow for example a stab wound to the precordium, and one instance followed just a needle puncture of the heart. This raises the question again about the relation of intrapericardial bleeding to this syndrome. Are there any common antigens between heart muscle and red cells? This is one question I would raise. The other question is have you looked at the idiopathic pericarditis syndrome with the test mechanism that you used. DR. ENGLE: Thank you Dr. Fowler. I know that Noble has had a long experience and interest in this condition. The situations he mentioned really are clinically identical. They are called by other descriptive terms just because of their settings, post-myocardial infarction syndrome, post-pericardial trauma syndrome. In our few patients studied with POSTPERICARDIOTOMY SYNDROME 159 these conditions we have found elevated heart reactive antibody of just this same level that is indistinguishable from postpericardiotomy syndrome. All these syndromes have the components of myocardial damage and intrapericardial bleeding. I don't know beyond that what the common ingredient is. We're looking for antibody against tropomyosin. Because the anti-heart antibody test is so specific for this condition that it is really helpful in diagnosis, but it is awkward to do, we would like to develop a radioimmunoassay technique that could be read off as so many nanograms and used everywhere, but we need the optimal antigen-antibody to do it. We don't know those answers, yet. DR. JOSEPH JOHNSON, III (Winston-Salem): I'd like to congratulate you upon this very nice paper. You've alluded by implication already to the problem of assigning pathogenicity to this particular antibody. It is always a question as to whether a particular antibody is a cause of disease or an effect. I wonder whether this antibody is cytotoxic or if it fixes complement. Is there any evidence which would support a pathogenic potential for this antibody? DR. ENGLE: We are working on establishing a cell line in which direct cytotoxicity can be tested. The early studies by Dr. Zabriskie were not rewarding. We were not even certain whether it was against pericardium per se or the different components of pericardium that merged with myocardium. Thus far we have answered certain questions by putting little pieces of a jigsaw puzzle together, but the total picture is by no means clear. It's just a little iarther along, and the possibilities are intriguing, as you suggest. DR. THOMAS MATTINGLY (Columbia): My comment relates to the problem of blood in the pericardium in these syndromes. I do not believe that this factor should be ignored in spite of the brilliant work which you have presented here today. In my experience, I know of no instance in these syndromes where the presence of blood in the pericardial sac or in the mediastinum about the pericardium did not exist. My earliest observations go back to the late forties with the beginning of anticoagulant administration in the management of acute myocardial infarctions. Hemopericardium occasionally occurred as a complication, producing tamponade and requiring paracentesis. In such instances, the presence of blood in the pericardium was well established. The clinical features of so-called post-myocardial infarction were observed to follow these instances of hemopericardium. Again, in 1958, I well remember during the presentation of an exhibit on nonpenetrating and penetrating trauma to the heart which included instances of hemopericardium and recurrent pericarditis, pleuritis, effusion and fever similar to the syndromes you have described here today, Dr. Dressler was presenting his first exhibits on his collection of cases which he described as the "post-myocardial infarction" or "Dresslers syndrome" at the same meeting. He came over and reviewed our exhibit and stated "Your patients have my disease." My reply was "I think it's vice-versa, I think your patients have our disease, namely blood in the pericardium." When one reviews all these syndromes, bleeding in the pericardium sac or in the mediastinum around the sac is a common denominator, including the post-operative cardiomyotomies where the pericardium is either closed or left open. Dr. Fowler, in all probability had bleeding in the pericardial sac following his paracentesis from needle injury to the myocardium. What is needed are some well designed experimental studies where blood is placed in the pericardial sac without any of the other factors present and observe for the clinical syndromes and the antibody responses. This may provide the answer to the crucial question of blood in the pericardium as a factor. DR. ENGLE: I certainly agree with you, Dr. Mattingly. We started out believing the reaction was either an autoimmune response or an unusual viral illness. I now think it's both, and one of the reasons why some people respond one time and not another to the same kind of trauma (some people have to undergo cardiac surgery a second time, as you know) is perhaps the role played by the viral illness. If that too is there at a certain time, then the 160 ENGLE, ZABRISKIE AND SENTERFIT syndrome is triggered in 25 percent of the patients. The role of bleeding certainly is possible in all of these and its role isn't clarified yet. DR. LOCKHART MCGUIRE (Charlottesville): Two questions Dr. Engle. In terms of the definition of the clinical syndrome, do you require a quiescent, afebrile latent period in which the direct inflammatory response to immediate trauma and blood has been eliminated, before you will say that this syndrome exists, or do you include an entire continuum from the immediate post-operative period? I think if you include both you are talking about two different diseases. DR. ENGLE: I think I'm not talking about two different diseases, and we do define it as one of two things, persistence or reappearance. It was thought at first that it occurred late and only in those people who were readmitted to the hospital after discharge. But in looking closely, there were evidences of pericardial involvement earlier. We think that they became worse, or relapsed or that the syndrome recurred. We define the postpericardectomy syndrome as the persistence beyond the first post-operative week of fever and signs of pericardial reaction. Within that first week one gets into surgical pericarditis, which is as you say a completely different thing. DR. McGuIRE: I would agree with that. Either persistence or appearance. That's a good phraseology for the definition. The other question was the role of an infectious agent in eliciting in some way this syndrome, I was going to ask you if you see it in epidemics. Does it correlate with other viral syndromes in your hospital population? DR. ENGLE: We are fortunate to have a virologist who works in Long Island who does such studies and keeps records of which viruses are prevalent at certain times, and we are trying to correlate our work with his. For instance, you will notice that there was no rise in titer to Cocksacki B4 with this syndrome in our first 137 patients but concurrent and coincident with the new B4 epidemic in the New York City area, we have several cases with B4 antibody now. This might suggest that it is a fresh illness, at least in some patients.




© Copyright 2026