
PDF (721 kB) - Lung Cancer
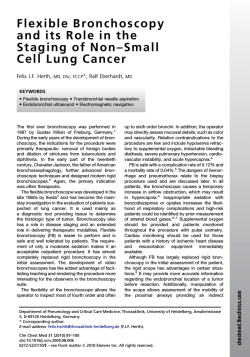
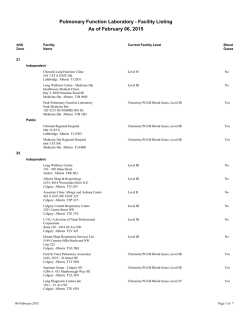
Lung Cancer 80 (2013) 249–255 Contents lists available at SciVerse ScienceDirect Lung Cancer journal homepage: www.elsevier.com/locate/lungcan Review Personalized therapy on the horizon for squamous cell carcinoma of the lung Han Sang Kim a , Tetsuya Mitsudomi b , Ross A. Soo c , Byoung Chul Cho a,∗ a Division of Medical Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Republic of Korea Department of Surgery, Kinki University Faculty of Medicine, Japan c Department of Haematology-Oncology, National University Cancer Institute, National University Health System, Singapore b a r t i c l e i n f o Article history: Received 29 November 2012 Received in revised form 15 February 2013 Accepted 16 February 2013 Keywords: Squamous cell carcinoma Non-small cell lung cancer Targeted therapy Driver mutation Biomarker a b s t r a c t Squamous cell carcinoma (SQCC) of the lung is the second-largest subtype of non-small cell lung cancer (NSCLC), causing an estimated 400,000 deaths per year worldwide. Recent developments in cancer genome sequencing technology expanded our knowledge of driver mutations, which were identified as novel candidates for targeted therapy in various cancers. Successful targeted treatments for lung adenocarcinoma, NSCLC’s primary subtype, with EGFR mutation or ALK fusion are clinically available, and a clinical trial of personalized targeted therapy in patients with lung adenocarcinoma is underway by the Lung Cancer Mutation Consortium. Although there are targeted treatments for lung adenocarcinoma, no personalized therapies currently exist for SQCC. Recently, comprehensive genomic characterization of lung SQCC using massively parallel sequencing has enabled us to identify several potential driver mutations/signaling pathways. These are FGFR1 amplifications, PI3KCA mutations, PTEN mutations/deletions, PDGFRA amplifications/mutations, and DDR2 mutations. The march toward personalized therapy may have taken a step forward with the discovery of these potential biomarkers for the treatment of SQCC of the lung. This article reviewed the current knowledge of genomic landscape of lung SQCC and summarized ongoing clinical trials of targeted agents for lung SQCC. Also, we will suggest several other actionable mutations with matching drugs that should be investigated in future clinical trials for the personalized treatment of lung SQCC. Crown Copyright © 2013 Published by Elsevier Ireland Ltd. All rights reserved. 1. Introduction Lung cancer is the leading cause of cancer-related death worldwide, causing ∼1.5 million deaths per year [1]. Non-small cell lung cancer (NSCLC) comprises about 85% of newly diagnosed lung cancers, which can be classified into two major histological subtypes: adenocarcinoma (∼50%) and squamous cell carcinoma (∼30%). Squamous cell carcinoma of the lung (SQCC) is closely associated with tobacco smoking. The discovery of so-called ‘driver mutations’ such as the epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) has led to the remarkable improvement in personalized therapy for lung adenocarcinoma [2–4]. However, no such available molecular target exists in squamous histology. Patients with SQCC are treated with ‘one-size-fits-all’ platinum-based chemotherapy, and therapies developed for lung adenocarcinoma such as bevacizumab, pemetrexed and EGFR tyrosine kinase inhibitors are contraindicated or largely ineffective ∗ Corresponding author at: Division of Medical Oncology, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Republic of Korea. Tel.: +82 2 2228 8126; fax: +82 2 393 3652. E-mail address: [email protected] (B.C. Cho). in lung SQCC [5–7]. For this reason, the identification of novel druggable molecular targets in SQCC is a top research priority. Recent developments in genomics using next-generation sequencing (NGS) technology allow us to capture information on genetic alterations of the tumor including single nucleotide variation, copy number alterations, and chromosomal rearrangements in whole-genome level [8]. Application of NGS in lung cancer research has produced a comprehensive profile of genetic alteration and has led to the identification of potential targets for personalized treatments [9–14]. In this review, we highlight the current knowledge of molecular targets, ongoing clinical trials of targeted agents, and actionable mutations with matching drugs in lung SQCCs. 2. Genomic landscape of lung SQCC using NGS technology Whilst comprehensive genome-scale characterization has been reported in lung adenocarcinoma [11,13,14], genetic alteration in SQCC is less understood. Single platform studies have identified several genetic changes related to SQCC, such as amplification of p63, PI3KCA, PDGFRA, SOX2, or FGFR1 and mutation in p53, EGFRvIII, PI3KCA, NRF2, PTEN, and DDR2 (Table 1) [15]. In 2012, the cancer genome atlas (TCGA) researchers produced a comprehensive genomic landscape of SQCC using whole exome/genome 0169-5002/$ – see front matter. Crown Copyright © 2013 Published by Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.lungcan.2013.02.015 250 H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 Table 1 Previously-identified genetic alterations in squamous cell carcinoma of the lung. Genetic alteration Chromosomal region Year reported in SQCC Reference p53 Mutation p63 Amplification EGFRvIII mutation PI3KCA mutation/amplification NRF2 mutation PDGFRA amplification SOX2 amplification PTEN mutation FGFR1 amplification DDR2 mutation 17p13.1 3q28 7p12 3q26.3 2q31 4q12 3q26.3–q27 10q23.3 8p12 1q23.3 1992 2000 2006 2007 2008 2009 2009 2010 2010 2011 [72] [73,74] [75] [54] [76] [64] [77] [58] [49] [67] Abbreviations: SQCC, squamous cell carcinoma of the lung. sequencing, mRNA sequencing, mRNA expression and promoter methylation for 178 lung SQCCs [12]. The major findings were as follows: (i) lung SQCC is characterized by complex genomic alterations, with a mean of 360 exonic mutations, 165 genomic rearrangements, and 323 segments of copy number alterations per tumor. They identified statistically recurrent mutations in 11 genes (TP53, CDKN2A, PTEN, PIK3CA, KEAP1, MLL2, HLA-A, NRF2, NOTCH1, RB1 and HLA-A) and somatic copy number alterations of chromosomal segments containing SOX2, PDGFRA and/or KIT, EGFR, FGFR1 and/or WHSC1L1, CCND1, CDKN2A, NFE2L2, MYC, CDK6, MDM2, BCL2L1, EYS, FOXP1, PTEN, and NF1. Of note, compared with lung adenocarcinoma, almost all lung SQCCs display somatic mutation of TP53 (81%) and selective amplification of chromosome 3q. (ii) There were frequent alterations in the cell cycle control (CDKN2A/RB1, 72%), response to oxidative stress (NFE2L2/KEAP1/CUL3, 34%), apoptotic signaling (PI3K/AKT, 69%) and squamous differentiation (SOX2/TP63/NOTCH1, 44%). (iii) Most importantly, they identified a potentially targetable gene or pathway alteration in most lung SQCC samples studied (Fig. 1). Although EGFR and KRAS mutations, the two most common oncogenic aberrations in lung adenocarcinoma, are extremely rare, there are frequent alterations in PI3K/AKT pathway and receptor tyrosine kinase (RTK) signaling, including EGFR amplification, BRAF mutation or FGFR amplification or mutation, in 69% of samples. Interestingly, loss-of-function mutations in HLA-A class I major histocompatibility gene were found in 3% of the tumors, suggesting a potential role of genotypic selection of patients for immunotherapies, such as anti-programmed death 1 (PD1) and anti-cytotoxic T-lymphocyte antigen 4 (CTLA4) antibodies. In a study by Paik et al. [16], the incidence of known targetable driver mutations in SQCC was examined using multiplex PCR sequencing. The driver mutations included PIK3CA mutations, PTEN mutations/deletions, FGFR1 amplifications, and DDR2 mutations. Overall, 60% of patients were found to have druggable targets, and the frequency of these mutations was similar to those in TCGA genetic profiles (Fig. 1). Although functional dependence of lung SQCC on these newly identified genetic mutations or pathway alterations should be validated, these data can help to facilitate effective personalized treatment for lung SQCC. 3. Currently ongoing clinical trials in lung SQCC Several agents are expected to be effective for the treatment of SQCC, and therefore currently are being tested in clinical trials (Table 2). These are cytotoxic nab-paclitaxel, novel targeted agents, and immunotherapies Table 3. 3.1. New cytotoxic agents Next-generation taxane (nab-paclitaxel, abraxane) is currently being evaluated in late phase trials. Nab-paclitaxel, composed of paclitaxel nanoparticle and human albumin, utilizes albumin receptor 60-kDa glycoprotein (gp60) and intracellular caveolin-1 and achieves higher intratumoral concentration compared with previous taxanes [17]. In addition, SPARC (secreted protein, acidic and rich in cysteine) increases nab-paclitaxel accumulation in the tumor area [17]. In patients with stage IIIB/IV NSCLC, nab-paclitaxel showed higher objective response rate (ORR) and less neuropathy and neutropenia than solvent-based paclitaxel (ORR, 33% vs. 25%; P = 0.005) [18]. In subgroup analysis, nab-paclitaxel had better efficacy in squamous histology (ORR, 41% vs. 24%, P < 0.001) than non-squamous histology (ORR, 26% vs. 25%, P = 0.808). One possible explanation for the better efficacy of nab-paclitaxel in squamous histology may be aberrant caveolin-1 expression in SQCC [19]. A study using SPARC, ceveolin-1, and miroRNAs as predictive biomarkers in patients with advanced stage NSCLC treated with carboplatin and nab-paclitaxel is ongoing (NCT00729612). 3.2. Targeted agents 3.2.1. Anti-EGFR therapy The currently approved EGFR-targeted agents in lung SQCC are small molecule tyrosine kinase inhibitors (TKIs), erlotinib and gefitinib [20,21]. Although treatment with EGFR-TKIs has afforded tremendous clinical benefits in lung adenocarcinomas with EGFR Fig. 1. Frequency of potential actionable drug targets in squamous cell carcinoma of the lung. H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 251 Fig. 2. Alterations in actionable oncogenic signaling pathways in squamous cell carcinoma of the lung. mutations, the same is not true for lung SQCCs, in which the ORR to EGFR-TKIs is typically less than 10%. In a recent TCGA data, EGFR mutations associated with the sensitivity to EGFR-TKIs was not found in lung SQCCs [12]. This was also confirmed by Rekhtman et al. [22], which reported that EGFR mutation does not occur in pure lung SQCCs from which adenosquamous carcinoma and poorly differentiated adenocarcinoma were excluded [22]. Cetuximab, the monoclonal antibody targeting EGFR protein, in combination with cisplatin/vinorelbine had a minimal survival benefit compared with chemotherapy alone in patients with stage IIIB/IV NSCLC in the FLEX study (overall survival [OS], 11.3 vs. 10.1 months; P = 0.044) [23]. In a preplanned subset analysis, a survival benefit was seen in squamous histology, albeit minimal (OS, 9.0 vs. 8.2 months). High tumor EGFR expression (immunohistochemistry score ≥200), which was more common in SQCC than in non-SQCC histology, may serve as a predictive biomarker for the selection of patients who would be most likely to derive a clinical benefit from treatment with chemotherapy plus cetuximab [24]. Other anti-EGFR agents, such as the second-generation EGFRTKI (afatinib) or the monoclonal antibody (necitumumab), are currently being studied in lung SQCC patients (Table 2). 3.2.2. Anti-MET therapy MET, a proto-oncogene located on 7q21-31, encodes a tyrosine kinase receptor for hepatocyte growth factor (HGF). MET protein expression, positivity defined as more than grade 1+ staining by immunohistochemistry, was observed in about 40% of lung SQCCs, and was associated with poor prognosis [25]. MET gene amplification, albeit not reported in TCGA data, was reported to be more frequent in patients with lung SQCC than in those with adenocarcinoma [26]. Furthermore, MET gene amplification has been shown to play a role in primary or acquired resistance to EGFR-TKI [27,28]. Onartuzumab, the monoclonal antibody against MET, in combination with erlotinib showed improvements in overall survival (OS) and progression-free survival (PFS) compared with erlotinib alone in a MET-overexpressed (Met Dx+) subgroup of advanced NSCLC patients in a randomized phase II study [29]. A randomized phase II study to test activity of onartuzumab in combination with a platinum doublet in lung SQCC is currently ongoing (NCT01519804). 3.2.3. Anti-insulin-like growth factor 1 (IGF-1) therapy Insulin-like growth factor-1 receptor (IGF-1R, located in 15q26.3) is a cell surface receptor with tyrosine kinase activity Table 2 Ongoing clinical trials exclusively for squamous cell carcinoma of the lung. Regimen Newer cytotoxic agents Albumin-bound paclitaxel/carboplatin vs. Gemcitabine/carboplatin Targeted agents Afatinib (EGFR) vs. Erlotinib Necitumumab (EGFR)/gemcitabine/cisplatin vs. Gemcitabine/cisplatin Onartuzumab (MET)/paclitaxel/platinum vs. Paclitaxel/platinum AXL1717 (IGF-1R) vs. docetaxel Gemcitabine/carboplatin/Iniparib (PARP-1) vs. Gemcitabine/carboplatin Immunotherapeutic agents Reolysin/paclitaxel/carboplatin Ipilimumab/paclitaxel/carboplatin vs. Paclitaxel/carboplatin BMS-936558 vs. docetaxel Phase Line of therapy II 1st III III II II III 2nd 1st 1st 2nd 1st 800 1097 110 140 780 II III III 1st 1st 2nd 55 920 264 Abbreviations: ORR, objective response rate; PFS, progression-free survival; OS, overall survival. Planned N 120 Primary endpoint ClinicalTrials.gov identifier ORR NCT01236716 PFS OS PFS PFS OS NCT01523587 NCT00981058 NCT01519804 NCT01561456 NCT01082549 ORR OS ORR NCT00998192 NCT01285609 NCT01642004 252 H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 Table 3 Selected potential actionable genetic alterations with matched targeted agents in squamous cell carcinoma of the lung. Molecular alteration/drug Target FGFR amplification FGFR1-3 AZD4547 BGJ398 FGFR1-3 LY2874455 FGFR1-4 FGFR1-2, VEGFR2 Brivanib FGFR, VEGFR, PDGFR, FLT3, c-KIT Dovitinib PI3KCA mutation PI3K, mTOR BEG235 BKM120 PI3KC-A,B,D,G GDC0941 PI3KC-A,B,D,G PX-866 PI3KC-A,D,G PTEN mutation/deletion PI3KC-B GSK2636771 PDGFRA amplification/mutation PDGFRA Crenolanib PDFGR, VEGFR, FGFR BIBF1120 PDFGR, VEGFR, FGFR, c-KIT Pazopanib DDR2 mutation DDR2, BCR/ABL, SRC, c-KIT Dasatinib BRAF mutation MEK1, MEK2 Trametinib MEK1, MEK2 MEK162 ERBB2 amplification EGFR, ERBB2, ERBB4 Afatinib EGFR, ERBB2 Lapatinib T-DM1 ERBB2, cytotoxic Sponsor Study phase (cancer type) ClinicalTrials.gov identifier AstraZeneca Novartis Eli Lilly Bristol Myers Squibb Novartis II (breast, stomach) I (solid tumors) I (solid tumors) III (liver, colon) III (kidney), II (lung) NCT01202591, NCT01457846 NCT01004224 NCT01212107 NCT00858871, NCT01367275 NCT01223027, NCT01676714 Novartis Novartis Genentech Oncothyreon II (breast) II (lung), I (breast) II (lung), I (breast) II (prostate) I (solid tumors) NCT00620594 NCT01297491, NCT01339442 NCT01493843, NCT00960960 NCT01331083, NCT01204099 Glaxo Smith Kline I (solid tumors) NCT01458067 Arog Pharmaceuticals Boehringer Ingelheim Glaxo Smith Kline II (glioma, GIST) III (lung, ovary) III (kidney, sarcoma) II (lung) NCT01229644, NCT01243346 NCT00805194, NCT01015118 NCT00720941, NCT00753688 NCT01027598 Bristol-Myers Squibb II (lung) II (breast) NCT01491633 NCT00371345 Glaxo Smith Kline Norvatis III (melanoma) II (lung) II (melanoma) NCT01245062 NCT01362296 NCT01320085 Boehringer Ingelheim Glaxo Smith Kline Roche III (lung, breast) III (breast), I (lung) III (breast, stomach) NCT01523587, NCT01125566 NCT00078572, NCT00528281 NCT00829166, NCT01641939 that activates the PI3K/Akt/mTOR and RAS/RAF/MAPK signaling pathways by binding IGF-1 or IGF-2 ligand [30]. The protein or mRNA expression of IGF-1R, but not IGF-1R gene copy number, was reported to be higher in lung SQCC than in other histologic subtypes [31]. In a phase II study with NSCLC, CP-751871 (figitumumab) with paclitaxel and carboplatin showed a response rate of 78% in patients with advanced SQCC [32]. However, two subsequent phase III studies of figitumumab with paclitaxel/carboplatin or erlotinib were discontinued due to non-significant survival benefit and increased toxicity [33,34]. A phase II study is ongoing to compare anti-tumor activity of AXL1717, a small-molecule IGF-1R inhibitor, with docetaxel as a second-line treatment of advanced lung SQCC (NCT01561456). 3.2.4. PARP-1 inhibitor Poly (ADP-ribose) polymerase-1 (PARP-1) is an important DNA repair enzyme, which is implicated in base excision repair and single-strand break (SSB) repair. When PARP-1 is inhibited, accumulated unrepaired SSBs are converted to double-strand breaks (DSB), inducing cell death [35]. PARP-1 is significantly upregulated at the mRNA level in multiple cancer types, including lung SQCC [36]. Iniparib is a novel PARP-1 inhibitor and has demonstrated synergistic activity with gemcitabine and carboplatin in preclinical studies [37]. A phase III trial of iniparib in combination with gemcitabine/carboplatin versus chemotherapy alone in SQCC is currently ongoing (NCT01082549) with the primary endpoint being OS [38]. 3.3. Immunotherapeutic agents Immunotherapy utilizes antibodies, vaccines, or viruses to modulate T-cell activity. Tumor infiltration of CD4+ /CD8+ T-cell was associated with better prognosis while higher expression of immunosuppressive regulatory T-cell was related to disease recurrence in operable NSCLC patients [39]. Two immunologic targets of current interest are cytotoxic T-lymphocyte antigen-4 (CTLA-4) and programmed death-1 (PD-1), which are negative regulators of T-cell activation [40,41] The preliminary efficacy of ipilimumab, the fully human monoclonal antibody against CTLA-4, has recently been reported in NSCLC [40]. In a randomized phase II study, a phased ipilimumab regimen (two doses of placebo plus paclitaxel and carboplatin followed by four doses of ipilimumab plus paclitaxel and carboplatin) showed better immune-related PFS (irPFS) compared to paclitaxel/carboplatin alone in patients with stage IIIB/IV NSCLC (5.7 vs. 4.6 months; P = 0.05), though statistically not significant [40]. The improvement in irPFS with the addition of ipilimumab to chemotherapy was greater in SQCC (HR, 0.55 [95% CI, 0.27–1.12]) than in non-squamous histology (HR, 0.82 [95% CI, 0.52–1.28]). Although caution is warranted in interpreting these subset data, it is notable that tumor-infiltrating T cells are more abundant in lung SQCC [42]. The aberrant increase in the expression of ligands for PD-1 was observed in SQCC including B7-H1, also known as PD-L1, and B7H3 [43]. Blockade of PD-1, a co-inhibitory receptor expressed by activated T cells, can overcome immune resistance and mediate tumor regression [44]. In a phase I study in patients with advanced solid tumors including NSCLC patients (n = 76), BMS-936558, the fully human monoclocal antibody against PD-1, showed a response rate of 18% and a PFS rate at 24 weeks of 26% [41]. The expression of PD-1 ligand on tumor was suggested as a potential biomarker for response. Oncolytic viruses have been investigated for use in cancer treatment. The Reoviruses are double-stranded RNA viruses targeting RAS-activated cells [45]. Preliminary results from a single-arm phase II trial of Reolysin, an isolated Reovirus, in combination with carboplatin and paclitaxel, showed a response rate of 26% and a disease control rate of 83% in lung SQCC (NCT00998192). 4. Promising druggable targets in SQCC Based on the recent findings on comprehensive genomic characterization of lung SQCC [12,16], promising druggable mutations on the horizon for targeted therapy will be reviewed (Fig. 2). 4.1. FGFR1 amplification The fibroblast growth factor receptor (FGFR) tyrosine kinase family is comprised of four kinases, FGFR 1–4, and plays a crucial H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 role in cancer cell growth, survival, and resistance to chemotherapy. Furthermore, an elevated concentration of FGF in serum is an independent adverse prognostic factor in NSCLC [46,47]. FGFR1 has been shown to be a target for deregulation by amplification, point mutation, or translocation [48]. Weiss et al. [49] examined high-resolution genomic profiles of 77 lung adenocarcinomas and 155 SQCCs and identified amplifications of FGFR1 exclusively in lung SQCC. Examination of an independent series by fluorescent in situ hybridization (FISH) revealed FGFR1 amplification of 22% in SQCC samples. FGFR1 amplification drives downstream activation of mitogen-activated protein kinase (MAPK) signaling in cancer cells. Treatment with FGFR inhibitor showed downstream inhibition and induction of apoptosis in FGFR1-amplified cell lines as well as strong antitumor activity in xenograft model, strongly supporting the utility of FGFR1 amplification as a relevant therapeutic target in lung SQCC. Recently, Cho et al. [50] observed FGFR1 amplification in 13% and found that FGFR1 amplification is a negative prognostic factor in patients with resected SQCC (disease-free survival, 26.9 vs. 94.6 months, P < 0.0001). The incidence of FGFR1 amplification was also associated with smoking status (current smoker, 28.9% vs. former smoker, 2.5% vs. non-smoker, 0%; P < 0.0001). This finding suggests that FGFR1 amplification is an oncogenic aberration caused by cigarette smoking in SQCC, while Heist et al. reported that there was no significant difference in overall survival stratified by FGFR amplification status [51]. 4.2. Phosphoinositide 3-kinase (PI3K) pathway The PI3K pathway is a major oncogenic signaling pathway which functions in cell survival and proliferation [52]. Somatic mutation or amplification of PIK3CA, encoding the p110␣ catalytic subunit, is known to be more prevalent in lung SQCCs than lung adenocarcinomas [53–55]. The incidence of PIK3CA mutation and amplification in lung SQCCs was reported to be 8–16% and 33–43%, respectively [12,16,53]. In phase I trials, response rate was significantly higher for patients with PIK3CA mutations treated with PI3K/AKT/mTOR pathway inhibitors than for those without documented mutations (35% vs. 5%, P < 0.001) [56]. Because lung SQCC patients were not included in these trials, further studies are needed to determine whether PIK3CA is a predictive marker to PIK3CA inhibition or not, in lung SQCC. The tumor suppressor PTEN confers phosphatase activity, which inhibits the PI3K/AKT/mTOR signaling pathway. Loss of PTEN expression has been reported in 74% of NSCLC [57]. Several mechanisms are associated with loss of PTEN expression, including PTEN point mutation/deletion/hypermethylation. The incidence of PTEN mutation/deletion was reported to be 15–28% in lung SQCC [12,16,58]. PTEN loss is associated with a poorer response to erlotinib in EGFR-mutant NSCLC [59]. Drugs targeting the PI3K/AKT/mTOR signaling pathway may be effective in PTEN-deficient tumors. In particular, a crucial role of PIK3CB has been reported in PTEN-deficient tumors [60,61]. In a prostate cancer model, the inhibition of PIK3CB reduced Akt phosphorylation and prevented tumorigenesis [60]. While PIK3CA depletion did not affect PI3K signaling in colorectal cancer cells, downregulation of PIK3CB is required for PI3K pathway inhibition in PTEN-deficient tumors [61]. These data supports the selective inhibition of PIK3CB may be effective in the treatment of PTEN-deficient tumors. 4.3. PDGFRA amplification/mutation Platelet-derived growth factor receptor (PDGFR) tyrosine kinase, which is classified as PDGFRA and PDGFRB, plays a crucial role in cell proliferation and angiogenesis [62,63]. The 253 amplification of the chromosomal segment of 4q12 harboring PDGFR-␣ has been reported in ∼9% of lung SQCCs [12,64]. Several multi-targeted TKIs targeting PDGFRA, such as sorafenib, sunitinib, and imatinib, are currently available. Despite initial enthusiasm for the anti-PDGFRA therapy, the addition of sorafenib to platinum-based chemotherapy disappointingly failed to improve survival in a randomized phase III study [65]. Notably, the addition of sorafenib increased mortality in a subset of lung SQCCs. A selective anti-PDGFRA agent, crenolanib, is now tested in a phase II study in patients with glioma and gastrointestinal stromal tumor (NCT01229644, NCT01243346). 4.4. Anti-DDR2 therapy Discoidin domain receptor 2 (DDR2) tyrosine kinase has been known to promote cell proliferation and survival when activated by its collagen ligand [66]. Mutation in the kinase domain of DDR2 was identified in 3.8% of lung SQCC samples (11/290) [67]. DDR2 mutation promotes malignant transformation and is associated with sensitivity to shRNA-mediated depletion of DDR2 or dasatinib, which was approved for the treatment of Bcr-Abl-positive chronic myelogenous leukemia. It also promotes malignant transformation, suggesting that gain-of-function mutations in DDR2 may be a promising therapeutic target in lung SQCCs [67]. A phase II trial to confirm the efficacy of dasatinib in lung SQCC with DDR2 mutation is currently underway (NCT01491633). 4.5. BRAF mutation BRAF mutation leads to the development of cancer through constitutional serine/threonine kinase activity [68]. BRAF mutation is present in ∼4% of SQCC, all of which are not canonical V600E mutation [69]. As mitogen-activated protein kinase (MEK) dependency was observed in BRAF mutant tumor, MEK inhibitor may benefit from non-V600E BRAF mutant SQCC [70]. 4.6. ERBB2 amplification Amplification of ERBB2, an EGFR family receptor tyrosine kinase, was found to be present in ∼4% of lung SQCC [12,71]. Further research needs to be done to confirm the efficacy of ERBB2-directed therapy in ERBB2-amplified lung SQCC. 5. Perspectives The recent expansion of our knowledge on the genomic landscape of lung SQCC leads to the identification of potential driver mutations, including FGFR1 amplification, PIK3CA mutation, PTEN mutation/deletion, PDGFRA amplification/mutation, DDR2 mutation, and BRAF mutation. The impact of these mutations on the response to the matching targeted therapy should be validated in future clinical trials. Similar to routine EGFR mutation testing in lung adenocarcinoma at diagnosis, better understanding of driver mutations and molecular pathways may lead to the development of mutation panels for the selection of patients with lung SQCC for a specific targeted therapy at the time of diagnosis or even disease progression. Furthermore, as the acquired resistance to targeted therapy is common and inevitable, identification of driver oncogene leading to drug resistance should be a research priority to achieve future personalized therapies for lung SQCC. 254 H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 Conflict of interest statement The authors have no conflicts of interest to declare. [24] Acknowledgements [25] This work was supported by the National Research Foundation of Korea (NRF) grants funded by the Korea government (MEST) (2012R1A2A2A01046927). [26] [27] References [28] [1] Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011;61:69–90. [2] Sandler AB, Johnson DH, Herbst RS. Anti-vascular endothelial growth factor monoclonals in non-small cell lung cancer. Clin Cancer Res 2004;10:4258s–62s. [3] Giaccone G. Epidermal growth factor receptor inhibitors in the treatment of non-small-cell lung cancer. J Clin Oncol 2005;23:3235–42. [4] Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med 2010;363:1693–703. [5] Johnson DH, Fehrenbacher L, Novotny WF, Herbst RS, Nemunaitis JJ, Jablons DM, et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol 2004;22:2184–91. [6] Hanna N, Shepherd FA, Fossella FV, Pereira JR, De Marinis F, von Pawel J, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol 2004;22:1589–97. [7] Scagliotti GV, Parikh P, von Pawel J, Biesma B, Vansteenkiste J, Manegold C, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-smallcell lung cancer. J Clin Oncol 2008;26:3543–51. [8] Meyerson M, Gabriel S, Getz G. Advances in understanding cancer genomes through second-generation sequencing. Nat Rev Genet 2010;11:685–96. [9] Campbell PJ, Stephens PJ, Pleasance ED, O’Meara S, Li H, Santarius T, et al. Identification of somatically acquired rearrangements in cancer using genome-wide massively parallel paired-end sequencing. Nat Genet 2008;40:722–9. [10] Pleasance ED, Stephens PJ, O’Meara S, McBride DJ, Meynert A, Jones D, et al. A small-cell lung cancer genome with complex signatures of tobacco exposure. Nature 2010;463:184–90. [11] Lee W, Jiang Z, Liu J, Haverty PM, Guan Y, Stinson J, et al. The mutation spectrum revealed by paired genome sequences from a lung cancer patient. Nature 2010;465:473–7. [12] The Cancer Genome Atlas Research N, Genome sequencing centres: Broad I, Hammerman PS, Lawrence MS, Voet D, Jing R, et al. Comprehensive genomic characterization of squamous cell lung cancers. Nature 2012;489:519–25. [13] Imielinski M, Berger AH, Hammerman PS, Hernandez B, Pugh TJ, Hodis E, et al. Mapping the hallmarks of lung adenocarcinoma with massively parallel sequencing. Cell 2012;150:1107–20. [14] Govindan R, Ding L, Griffith M, Subramanian J, Dees ND, Kanchi KL, et al. Genomic landscape of non-small cell lung cancer in smokers and neversmokers. Cell 2012;150:1121–34. [15] Weir BA, Woo MS, Getz G, Perner S, Ding L, Beroukhim R, et al. Characterizing the cancer genome in lung adenocarcinoma. Nature 2007;450:893–8. [16] Paul Paik AH, Lu Wang, Natasha Rekhtman, Marc Ladanyi, Kris Mark G. Multiplex testing for driver mutations in squamous cell carcinomas of the lung. J Clin Oncol 2012;30 (suppl; abstr 7505). [17] Gradishar WJ. Albumin-bound paclitaxel: a next-generation taxane. Expert Opin Pharmacother 2006;7:1041–53. [18] Socinski MA, Bondarenko I, Karaseva NA, Makhson AM, Vynnychenko I, Okamoto I, et al. Weekly nab-paclitaxel in combination with carboplatin versus solvent-based paclitaxel plus carboplatin as first-line therapy in patients with advanced non-small-cell lung cancer: final results of a phase III trial. J Clin Oncol 2012;30:2055–62. [19] Yoo SH, Park YS, Kim HR, Sung SW, Kim JH, Shim YS, et al. Expression of caveolin1 is associated with poor prognosis of patients with squamous cell carcinoma of the lung. Lung Cancer 2003;42:195–202. [20] Shepherd FA, Rodrigues Pereira J, Ciuleanu T, Tan EH, Hirsh V, Thongprasert S, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 2005;353:123–32. [21] Kim ES, Hirsh V, Mok T, Socinski MA, Gervais R, Wu YL, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trial. Lancet 2008;372:1809–18. [22] Rekhtman N, Paik PK, Arcila ME, Tafe LJ, Oxnard GR, Moreira AL, et al. Clarifying the spectrum of driver oncogene mutations in biomarker-verified squamous carcinoma of lung: lack of EGFR/KRAS and presence of PIK3CA/AKT1 mutations. Clin Cancer Res 2012;18:1167–76. [23] Pirker R, Pereira JR, Szczesna A, von Pawel J, Krzakowski M, Ramlau R, et al. Cetuximab plus chemotherapy in patients with advanced [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] [41] [42] [43] [44] [45] [46] [47] non-small-cell lung cancer (FLEX): an open-label randomised phase III trial. Lancet 2009;373:1525–31. Pirker R, Pereira JR, von Pawel J, Krzakowski M, Ramlau R, Park K, et al. EGFR expression as a predictor of survival for first-line chemotherapy plus cetuximab in patients with advanced non-small-cell lung cancer: analysis of data from the phase 3 FLEX study. Lancet Oncol 2012;13:33–42. Masuya D, Huang C, Liu D, Nakashima T, Kameyama K, Haba R, et al. The tumourstromal interaction between intratumoral c-Met and stromal hepatocyte growth factor associated with tumour growth and prognosis in non-small-cell lung cancer patients. Br J Cancer 2004;90:1555–62. Go H, Jeon YK, Park HJ, Sung SW, Seo JW, Chung DH. High MET gene copy number leads to shorter survival in patients with non-small cell lung cancer. J Thorac Oncol 2010;5:305–13. Engelman JA, Zejnullahu K, Mitsudomi T, Song Y, Hyland C, Park JO, et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science 2007;316:1039–43. Tanizaki J, Okamoto I, Sakai K, Nakagawa K. Differential roles of transphosphorylated EGFR, HER2, HER3, and RET as heterodimerisation partners of MET in lung cancer with MET amplification. Br J Cancer 2011;105: 807–13. Spigel DRTJE, Ramlau R, Daniel DB, Goldschmidt JH, Blumenschein GR, Krzakowski MJ, et al. Final efficacy results from OAM4558g, a randomized phase II study evaluating MetMAb or placebo in combination with erlotinib in advanced NSCLC. J Clin Oncol 2011;29 (suppl; abstr 7505). Pollak MN, Schernhammer ES, Hankinson SE. Insulin-like growth factors and neoplasia. Nat Rev Cancer 2004;4:505–18. Dziadziuszko R, Merrick DT, Witta SE, Mendoza AD, Szostakiewicz B, Szymanowska A, et al. Insulin-like growth factor receptor 1 (IGF1R) gene copy number is associated with survival in operable non-small-cell lung cancer: a comparison between IGF1R fluorescent in situ hybridization, protein expression, and mRNA expression. J Clin Oncol 2010;28:2174–80. Karp DD, Paz-Ares LG, Novello S, Haluska P, Garland L, Cardenal F, et al. Phase II study of the anti-insulin-like growth factor type 1 receptor antibody CP-751,871 in combination with paclitaxel and carboplatin in previously untreated, locally advanced, or metastatic non-small-cell lung cancer. J Clin Oncol 2009;27:2516–22. Jassem JCJL, Karp DD, Mok T, Benner RJ, Green SJ, Park K, et al. Randomized, open label, phase III trial of figitumumab in combination with paclitaxel and carboplatin versus paclitaxel and carboplatin in patients with non-small cell lung cancer (NSCLC). J Clin Oncol 2010;28:15s (suppl; abstr 7500) 2010. Yee D. Insulin-like growth factor receptor inhibitors: baby or the bathwater? J Natl Cancer Inst 2012;104:975–81. Krishnakumar R, Kraus WL. The PARP side of the nucleus: molecular actions, physiological outcomes, and clinical targets. Mol Cell 2010;39:8–24. Ossovskaya V, Koo IC, Kaldjian EP, Alvares C, Sherman BM. Upregulation of poly (ADP-ribose) polymerase-1 (PARP1) in triple-negative breast cancer and other primary human tumor types. Genes Cancer 2010;1:812–21. Davar D, Beumer JH, Hamieh L, Tawbi H. Role of PARP inhibitors in cancer biology and therapy. Curr Med Chem 2012;19:3907–21. Spigel DRPGH, Hainsworth JD, De Marinis F, Kabbinavar FF, Kim ES, Lynch TJ, et al. Sarah Cannon Research Institute and Tennessee Oncology, Nashville, TN. Randomized phase III trial of gemcitabine/carboplatin with or without iniparib (BSI-201) in patients with previously untreated stage IV squamous non-small cell lung cancer (NSCLC). J Clin Oncol 2011;29 (suppl; abstr TPS220). Petersen RP, Campa MJ, Sperlazza J, Conlon D, Joshi MB, Harpole Jr DH, et al. Tumor infiltrating Foxp3+ regulatory T-cells are associated with recurrence in pathologic stage I NSCLC patients. Cancer 2006;107:2866–72. Lynch TJ, Bondarenko I, Luft A, Serwatowski P, Barlesi F, Chacko R, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, doubleblind, multicenter phase II study. J Clin Oncol 2012;30:2046–54. Suzanne Louise Topalian JRB, Stephen Hodi F, David F McDermott, David C Smith, Scott N Gettinger, Janis M Taube, et al. Anti-PD-1 (BMS-936558, MDX1106) in patients with advanced solid tumors: Clinical activity, safety, and a potential biomarker for response. 2012 ASCO Annual Meeting. J Clin Oncol 2012;30 (suppl; abstr CRA2509). Hiraoka K, Miyamoto M, Cho Y, Suzuoki M, Oshikiri T, Nakakubo Y, et al. Concurrent infiltration by CD8+ T cells and CD4+ T cells is a favourable prognostic factor in non-small-cell lung carcinoma. Br J Cancer 2006;94: 275–80. Boland JM, Kwon ED, Harrington SM, Wampfler JA, Tang H, Yang P, et al. Tumor B7-H1 and B7-H3 expression in squamous cell carcinoma of the lung. Clin Lung Cancer 2012;14:157–63. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer 2012;12:252–64. Strong JE, Coffey MC, Tang D, Sabinin P, Lee PW. The molecular basis of viral oncolysis: usurpation of the Ras signaling pathway by reovirus. EMBO J 1998;17:3351–62. Joensuu H, Anttonen A, Eriksson M, Makitaro R, Alfthan H, Kinnula V, et al. Soluble syndecan-1 and serum basic fibroblast growth factor are new prognostic factors in lung cancer. Cancer Res 2002;62:5210–7. Fischer H, Taylor N, Allerstorfer S, Grusch M, Sonvilla G, Holzmann K, et al. Fibroblast growth factor receptor-mediated signals contribute to the malignant phenotype of non-small cell lung cancer cells: therapeutic implications and synergism with epidermal growth factor receptor inhibition. Mol Cancer Ther 2008;7:3408–19. H.S. Kim et al. / Lung Cancer 80 (2013) 249–255 [48] Turner N, Grose R. Fibroblast growth factor signalling: from development to cancer. Nat Rev Cancer 2010;10:116–29. [49] Weiss J, Sos ML, Seidel D, Peifer M, Zander T, Heuckmann JM, et al. Frequent and focal FGFR1 amplification associates with therapeutically tractable FGFR1 dependency in squamous cell lung cancer. Sci Transl Med 2010;2, 62ra93. [50] Hye Ryun Kim DJK, Dae Ryong Kang, Jin Gu Lee, Sun Min Lim, Chang Young Lee, Sun Young Rha, et al. Fibroblast growth factor receptor 1 gene amplification is associated with poor survival and cigarette smoking dosage in resected squamous cell lung cancer patients. J Clin Oncol 2012;31:731–7. [51] Heist RS, Mino-Kenudson M, Sequist LV, Tammireddy S, Morrissey L, Christiani DC, et al. FGFR1 amplification in squamous cell carcinoma of the lung. J Thorac Oncol 2012;7:1775–80. [52] Liu P, Cheng H, Roberts TM, Zhao JJ. Targeting the phosphoinositide 3-kinase pathway in cancer. Nat Rev Drug Discov 2009;8:627–44. [53] Kawano O, Sasaki H, Endo K, Suzuki E, Haneda H, Yukiue H, et al. PIK3CA mutation status in Japanese lung cancer patients. Lung Cancer 2006;54:209–15. [54] Okudela K, Suzuki M, Kageyama S, Bunai T, Nagura K, Igarashi H, et al. PIK3CA mutation and amplification in human lung cancer. Pathol Int 2007;57: 664–71. [55] Yamamoto H, Shigematsu H, Nomura M, Lockwood WW, Sato M, Okumura N, et al. PIK3CA mutations and copy number gains in human lung cancers. Cancer Res 2008;68:6913–21. [56] Janku F, Tsimberidou AM, Garrido-Laguna I, Wang X, Luthra R, Hong DS, et al. PIK3CA mutations in patients with advanced cancers treated with PI3K/AKT/mTOR axis inhibitors. Mol Cancer Ther 2011;10:558–65. [57] Marsit CJ, Zheng S, Aldape K, Hinds PW, Nelson HH, Wiencke JK, et al. PTEN expression in non-small-cell lung cancer: evaluating its relation to tumor characteristics, allelic loss, and epigenetic alteration. Hum Pathol 2005;36: 768–76. [58] Jin G, Kim MJ, Jeon HS, Choi JE, Kim DS, Lee EB, et al. PTEN mutations and relationship to EGFR, ERBB2, KRAS, and TP53 mutations in non-small cell lung cancers. Lung Cancer 2010;69:279–83. [59] Sos ML, Koker M, Weir BA, Heynck S, Rabinovsky R, Zander T, et al. PTEN loss contributes to erlotinib resistance in EGFR-mutant lung cancer by activation of Akt and EGFR. Cancer Res 2009;69:3256–61. [60] Jia S, Liu Z, Zhang S, Liu P, Zhang L, Lee SH, et al. Essential roles of PI(3)K-p110beta in cell growth, metabolism and tumorigenesis. Nature 2008;454:776–9. [61] Wee S, Wiederschain D, Maira SM, Loo A, Miller C, deBeaumont R, et al. PTEN-deficient cancers depend on PIK3CB. Proc Natl Acad Sci USA 2008;105:13057–62. [62] Zhang H, Bajraszewski N, Wu E, Wang H, Moseman AP, Dabora SL, et al. PDGFRs are critical for PI3K/Akt activation and negatively regulated by mTOR. J Clin Invest 2007;117:730–8. 255 [63] Williams LT. Signal transduction by the platelet-derived growth factor receptor. Science 1989;243:1564–70. [64] Ramos AH, Dutt A, Mermel C, Perner S, Cho J, Lafargue CJ, et al. Amplification of chromosomal segment 4q12 in non-small cell lung cancer. Cancer Biol Ther 2009;8:2042–50. [65] Scagliotti G, Novello S, von Pawel J, Reck M, Pereira JR, Thomas M, et al. Phase III study of carboplatin and paclitaxel alone or with sorafenib in advanced nonsmall-cell lung cancer. J Clin Oncol 2010;28:1835–42. [66] Day E, Waters B, Spiegel K, Alnadaf T, Manley PW, Buchdunger E, et al. Inhibition of collagen-induced discoidin domain receptor 1 and 2 activation by imatinib, nilotinib and dasatinib. Eur J Pharmacol 2008;599:44–53. [67] Hammerman PS, Sos ML, Ramos AH, Xu C, Dutt A, Zhou W, et al. Mutations in the DDR2 kinase gene identify a novel therapeutic target in squamous cell lung cancer. Cancer Discov 2011;1:78–89. [68] Wan PT, Garnett MJ, Roe SM, Lee S, Niculescu-Duvaz D, Good VM, et al. Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF. Cell 2004;116:855–67. [69] Paik PK, Arcila ME, Fara M, Sima CS, Miller VA, Kris MG, et al. Clinical characteristics of patients with lung adenocarcinomas harboring BRAF mutations. J Clin Oncol 2011;29:2046–51. [70] Solit DB, Garraway LA, Pratilas CA, Sawai A, Getz G, Basso A, et al. BRAF mutation predicts sensitivity to MEK inhibition. Nature 2006;439:358–62. [71] Grob TJ, Kannengiesser I, Tsourlakis MC, Atanackovic D, Koenig AM, Vashist YK, et al. Heterogeneity of ERBB2 amplification in adenocarcinoma, squamous cell carcinoma and large cell undifferentiated carcinoma of the lung. Mod Pathol 2012;25:1566–73. [72] Kishimoto Y, Murakami Y, Shiraishi M, Hayashi K, Sekiya T. Aberrations of the p53 tumor suppressor gene in human non-small cell carcinomas of the lung. Cancer Res 1992;52:4799–804. [73] Yamaguchi K, Wu L, Caballero OL, Hibi K, Trink B, Resto V, et al. Frequent gain of the p40/p51/p63 gene locus in primary head and neck squamous cell carcinoma. Int J Cancer 2000;86:684–9. [74] Hibi K, Trink B, Patturajan M, Westra WH, Caballero OL, Hill DE, et al. AIS is an oncogene amplified in squamous cell carcinoma. Proc Natl Acad Sci USA 2000;97:5462–7. [75] Ji H, Zhao X, Yuza Y, Shimamura T, Li D, Protopopov A, et al. Epidermal growth factor receptor variant III mutations in lung tumorigenesis and sensitivity to tyrosine kinase inhibitors. Proc Natl Acad Sci USA 2006;103:7817–22. [76] Shibata T, Ohta T, Tong KI, Kokubu A, Odogawa R, Tsuta K, et al. Cancer related mutations in NRF2 impair its recognition by Keap1-Cul3 E3 ligase and promote malignancy. Proc Natl Acad Sci USA 2008;105:13568–73. [77] Bass AJ, Watanabe H, Mermel CH, Yu S, Perner S, Verhaak RG, et al. SOX2 is an amplified lineage-survival oncogene in lung and esophageal squamous cell carcinomas. Nat Genet 2009;41:1238–42.




© Copyright 2026