
Plasma Crosslinked Fibrin Polymers: Quantitation
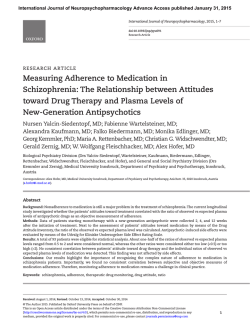
From www.bloodjournal.org by guest on February 6, 2015. For personal use only. Plasma Crosslinked Fibrin Polymers: Quantitation Based on Tissue Plasminogen Activator Conversion to D-Dimer and Measurement in Normals and Patients With Acute Thrombotic Disorders By Abraham Kornberg, Charles W. Francis, and Victor J. Marder Plasma crosslinked fibrin polymers (XLFP) are formed as a result of in vivo hemostatic activation and are elevated in thrombotic disease. We have investigated the plasmic degradation of plasma XLFP in vitro t o provide information regarding the pattern of crosslinking and the composition of degradation products. Plasma XLFP were identified by sodium dodecyl sulfate (SDS)-agarose electrophoresis and Western blotting and quantitated by gel scanning. D-dimer was measured by enzyme-linked immunosorbent assay and the results were verified by SDS-polyacrylamide gel electrophoresis and Western blotting of the digests. Complete degradation of XLFP occurred only after supplementation of plasma with plasminogen (5 U/mL) and incubation with recombinant tissue plasminogen activator (rt-PA), indicating that the normal plasma plasminogen concentration limits plasmic degradation in vitro. Gel electrophoresis showed that the principal terminal degradation products of XLDP were fragments D, DD, and E, indicating that crosslinking occurred primarily through y chain dimers. After adding a low concentration of thrombin t o plasma in vitro, XLFP increased progressively before clotting, and the concentration correlated with the increase in the D-dimer concentration after degradation (r = .98). Plasma XLFP and D-dimer concentrations in plasmic digests were significantly elevated in patients with stroke (150 f 83 pg/mL and 88 f 32 pg/mL), myocardial infarction (217 f 110 pg/mL and 84 f 30 pg/ mL), and venous thrombosis (187 f 80 pg/mL and 86 f 19 pg/mL) compared with normals (28 f 12 pg/mL and 25 7 pg/mL). There was a strong correlation between the plasma concentration of XLFP and the D-dimer immunoreactivity of plasma after plasmic degradation (r = .87). The results indicate that XLFP in plasma are crosslinked primarily through y chains and degrade t o fragment DD with plasminogen activation. Also, the immunoreactivity of in vitro plasmic digests of plasma reflects the concentration of XLFP and may provide a useful indirect measure of in vivo hemostatic activation in patients with thrombotic disease. 0 1992by The American Society of Hematology. H results indicate that D-dimer is the primary plasmic derivative of XLFP and that the D-dimer concentration in plasmic digests of plasma provides an indirect measure of the content of XLFP. Also, the plasma concentration of XLFP in normals and patients is measured, showing an increase in patients with thrombosis. EMOSTATIC activatian is primarily a localized process resulting in fibrin formation at sites of vessel injury, inflammation, or thrombus formation. However, the thrombin that is formed results in systemic effects, including release of fibrinopeptide A from fibrinogen and circulation of “soluble fibrin.” The latter is heterogeneous in composition and reflects a variable extent of polymerization and crosslinking. Low concentrations of soluble fibrin are found in normal plasma and increased concentrations are found in patients with thrombotic disease using several methods, including gel filtration chromatography,14 affinity chromatography,5p6high performance liquid chromatography? sodium dodecyl sulfate (SDS)-agarose gel electrophoresis?-1° potentiation of tissue plasminogen activator (t-PA) activity,” ethanol gelation,’* and protamine sulfate precipitation.l3 An alternative approach to the evaluation of plasma soluble fibrin is based on the identification of covalently crosslinked fibrin polymers (XLFP) resulting from the action of factor XIII, to crosslink fibrin into dimers and p01ymers.l~Using electrophoretic techniques, we9 and othe r ~ ~have ~ identified , ~ ~ - low ~ ~concentrations of XLFP in normal plasma and elevated concentrations in patients with thrombotic disease, including acute myocardial infarction (MI). Crosslinked fibrin polymers contain the yy chain c r o ~ s l i n k , ~ J ~which J ~ - ~ is~ resistant to plasmin,zO,21 and plasmic degradation yields derivatives containing crosslinked yy chain remnants, including fragment DD.21-z4In plasma of patients undergoing fibrinolytic therapy, plasma XLFP are degraded in vivo, contributing to elevated plasma concentrations of fibrin degradation products.5 In this study, we have investigated the plasmic degradation of XLFP in vitro. Conditions required for complete degradation of plasma XLFP are identified and relations between the concentration of XLFP and the D-dimer immunoreactivity after degradation are characterized. The Blood, VOI 80,NO3 (August 1). 1992: pp 709-717 * MATERIALS AND METHODS Patients and blood samples. Blood was obtained by antecubital venipuncture from normals and patients, anticoagulated with sodium citrate (0.4% final concentration), immediately placed on ice, centrifuged within 1hour of collection at 2,300g for 15 minutes at 4”C, aliquoted, and stored at -70°C. Samples were thawed within 7 days and prepared for electrophoresis or plasmic digestion. Acute MI was diagnosed in patiests with persistent chest pain, an elevated MB fraction of creatine kinase, and electrocardiographic changes of ST segment elevation with subsequent development of significantQ waves (transmural) or ST segment depression (subendocardial). Stroke was a clinical diagnosis based on the development of irreversible neurologic signs and symptomsand the exclusion of other disorders, such as tumors, infections, demyelinating diseases, and trauma, with confirmation by appropriate radio- From the Hematology Unit, Depaninent of Medicine, University of Rochester School of Medicine and Dentisty, Rochester, Ny. Submitted October 25 1991; accepted March 31,1992. Suppried in pari by Grant No. HL-30616from the National Heart, Lung and Blood Instihrte, National Institutes of Health, Bethesda, MD. Address reprint requests to Charles W. Francis, MD, Hematology Unit, PO Box 610, University of Rochester Medical Center, 601 Elmwood Ave, Rochester, NY14642. The publication costs of this article were defrayed in part by page charge payment. T%is article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section I734 solely to indicate this fact. 0 1992 by The American Society of Hematology. 0006-4971I92 /8003-OO18$3.OO10 709 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 710 KORNBERG, FRANCIS, AND MARDER streptavidin-horseradish peroxidase conjugate (Bethesda Research Laboratories) diluted l:l,OOO in TTBS. The blot waswashed in TTBS after each step and was developed by submerging it in a solution of 20 mmol/L. 3.3'-diaminobenzadine tetrahydrochloride (Sigma) in 'ITBS containing 3.4 mmol/L nickel chloride and 0.009% hydrogen peroxide. The reaction was terminated after color development ( 5 to 10 minutes) by washingwith water, and the blot was dried and photographed. For quantitation. gels were scanned, and protein in bands quantitated by comparison with a standard curve as described previously.y graphic or magnetic resonance imaging. Deep vein thrombosis was diagnosed by venography in patients with compatible clinical findings. Fihrinogen and fihrin digests. Fibrinogen (grade L) was purchased from Helena Laboratories (Beaumont, TX) and reconstituted at a concentration of 5 mg/mL in 50 mmol/L Tris, 100 mmollL sodium chloride, pH 7.6. Plasmic digests were prepared by incubation with plasmin (kindly provided by the Bureau of Biologics Standards, Bethesda, MD) at a concentration of 0.15 Committee on Thrombolytic Agents (CTA) UlmL, at 37°C for 90 minutes. Digestion was terminated by the addition of aprotinin (Mobay Chemical Co, New York, NY) to a final concentration of 300 kallikrein inhibitory units (KIU)/mL to inhibit plasmin. Fragment DD was isolated from a plasmic digest of crosslinked fibrin prepared as described elsewhere.2hLyophilized finely ground fibrin was digested by suspending in 50 mmol/L Tris, 100 mmol/L sodium chloride, 5 mmol/L calcium chloride, pH 7.6, and incubation with 3.4 CTA UlmL plasmin with gentle magnetic stirring at 37°C for 24 hours. Digestion was terminated by the addition of aprotinin (100 KIUlmL) to inhibit plasmin, and fragment DD was purified by gel filtration on a column (2.5 x 140 cm) of Sephaclyl S-300(Pharmacia LKB Biotechnology, Inc, Piscataway, NJ) in 50 mmol/L Tris, 150 mmol/L sodium chloride, 40 mmollL sodium ethylenediaminetetraceticacid (EDTA), pH 7.6, at a flow rate of 35 mLlh. The protein peak containing fragment DD was identified by SDS-polyacrylamidegel electrophoresis (SDS-PAGE) of aliquots, p l e d , and stored. Preparation ofplasma digests. Aliquots of 50 p.L of plasma were incubated with recombinant t-PA (rt-PA) purchased from Genentech, Inc (South San Francisco, CA) alone or with human gluplasminogen obtained from Sigma Chemical Co (St Louis, MO) at 37°C. and 500 KlUlmL aprotinin was added at intervals to inhibit plasmin. Normal plasma contains 1 UlmL plasminogen (2.4 FmollL). Electrophoretic analysis. SDS 2% agarose electrophoresis and SDS 4% to 10% gradient PAGE were performed as described e l ~ e w h e r e .Western ~ . ~ ~ blotting was performed using a modification of the method of Towbin et a12"as described previously.B Immunostainingwas performed by incubating the nitrocellulose paper for 30 minutes at 25°C with the following sequence of antibodies and reagents: rabbit antihuman fibrinogen antiserum (Cappel Laboratories, Westchester, PA) diluted 1:2,000 in Tween tris-buffered saline (TTBS); biotinylated goat-antirabbit IgG (Bethesda Research Laboratories, Gaithersburg, MD) diluted 1:1,OOO in TTBS; 1 Trimer Dimer -- Monomer- 2 3 4 5 6 D-dimer enzyme-linked immunosorhent assay (ELISA). Crosslinked fibrin degradation products were measured with an ELSA (Dimertest; American Diagnostica, Greenwich, CT)using a monospecific antibody (DDl3B6) reactive with a site associated with the factor XII1.-mediated yy crosslink and a panspecific tag antibody (4D2) reactive with fibrin and fibrinogen degradation Precoated plates were used, and the results were calculated with a standard curve from 78 to 5,OOO nglmL of purified fragment DD provided by the manufacturer. Statistical anulysis. Comparison of means was performed using the two-tailed t-test. Variance is described as 2SD. RESULTS To determine the conditions for in vitro degradation of XLFP, plasma samples containing varying amounts of XLFP were incubated in vitro with rt-PA or rt-PA plus plasminogen and then analyzed by SDS-agarose electrophoresis and Western blotting (Fig 1). Incubation of plasma with a high concentration of rt-PA (200 pg/mL) resulted in incomplete degradation of fibrinogen and XLFP (lanes 2,s. and 8). Bands consistent with fibrinogen degradation products X and Y in addition to fragment D were present after 1 hour of incubation with 200 pg/mL rt-PA in all samples, and less degraded derivatives larger than fibrinogen were evident in the digest in lane 5. Supplementation with 1 or 2 U/mL plasminogen resulted in greater, but still incomplete, degradation with rt-PA (data not shown). However, complete degradation of fibrinogen and XLFP occurred in all plasma samples after incubation for 1 hour with 25 Fg/mL rt-PA plus 5 U/mL plasminogen (Fig 1, lanes 3,6, and 9). After digestion under these conditions, electrophoresis 7 8 9 -w w cJ @ # 'b - -l) rt-PA (pg/ml) plasminogen (U/ml) so - - m -D 0 200 25 0 200 25 0 200 25 0 0 5 0 0 5 0 0 5 'E + DD Fig 1. Plasmic degradation of plasma XLFP at varying concentrations of rt-PA and plasminogen. Three separate stored, citrated plasma samples were incubated at 3PC with varying concentrationsof rt-PA and plasminogen, and the reaction was terminated after 1 hour by the additionof aprotinin (500 U/mL). subjected An aliquot from to SDS each2% sample agarose was electrophoresis, followed by Western blotting with antifibrinogen antiserum. The locations of the fibrinogen/fibrin monomer and crosslinked fibrin dimer and trimer are indicated. Fibrinogen fragments X, D, and E can be identified, but fragments DD and Y overlap with this gel system. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. QUANTITATION OF CROSSLINKED FIBRIN POLYMERS 711 II- )c -Monomer -0 Pentamer - Quadramer - Trimer - Dimer .14 .28 .43 .57 .71 .86 1.O A Time/ Clotting Time Fig 2. Formation and degradation of plasma XLFP. (A) Imreaslng XLFP in plasma after addition of thrombin. Stored, pooled cltrated plasma was incubated with 0.01 U/mLthrombin (0.9 pmol/L) and 10 mmol/L calcium chloride at 37°C. Aliquots were withdrawn at lntervals and subjected to SDS 2% agarose electrophoresis followed by Western blotting with antifibrinogen antiserum. The "TimelClotting Time" value reflects the incubationtime of each sample divided by the time of first visible fibrin formation at 35 minutes. (B) Plasmic digestion of plasma containing increasingamounts of XLFP formed by addition of thrombin. Aliquots of plasma were withdrawn from plasma samples shown in (A) and incubated with 25 pg/mL rt-PA and 5 U/mL plasminogen for 1 hour at 37°C. Aprotinin (500 U/mL) was added to each digest, and an aliquot was subjected to SDS 4% to 10% gradient PAGE, followed by Western blotting with antifibrinogen antiserum. The .57 time/clotting time value was not analyzed in this experiment. - -DD -D showed no bands larger than fragment DD, a heavy band with the migration of fragment D, and a fainter band consistent with fragment DD. Because incubation of plasma with 25 pg/mL rt-PA plus 5 U/mL plasminogen resulted in apparently complete degradation, all digests in subsequent experiments were prepared using these conditions. To determine whether a correlation existed between the D-dimer immunoreactivityof plasmic digests and the plasma concentration of XLFP, we prepared plasma containing varying concentrations of XLFP. A low concentration of thrombin (0.01 U/mL, 0.9 pmol/L) was added to stored citrated pooled plasma, resulting in a progressive increase in XLFP before visible clot formation occurred (Fig 2A). Whereas the monomer band did not change in intensity after addition of thrombin, the dimer band increased slightly at .14 and .28 of the clotting time, and was more prominent at .43 and .57 of the clotting time. At .71 and .86 of the clotting time, the dimer band was most prominent, with six to nine polymeric forms. The intensity of all bands decreased at 1.0 of the clotting time (35 minutes), when 1E 0 .14 .28.43 .71 -86 1.o TimeXlotting Time B fa..it fibrin strands were first visible -.I the plasma and before solid clot formation occurred. Incubation of aliquots of the same plasma samples with rt-PA and plasminogen yielded digests that contained predominantly fragments D, E, and DD by SDS-PAGE (Fig 2B). Whereas bands corresponding to fragments D and E did not change up to .86 of the clotting time, the D-dimer band increased progressively from .28 to .43 and was most From www.bloodjournal.org by guest on February 6, 2015. For personal use only. KORNBERG, FRANCIS, AND MARDER 712 prominent at .71 and .86 of the clotting time, corresponding to the increase in XLFP (Fig 2A). The intensity of the E, D, and D-dimer bands decreased at the time of visible fiber formation (1.0 of the clotting time), in parallel with the decrease in the monomer and polymeric forms on the SDS-agarose gel. This correspondence was examined more closely by comparison of the plasma concentration (pg/ mL) of XLFP as determined by SDS-agarose gel electrophoresis and scanning densitometry and as the ratio of polymer to monomer bands, with D-dimer concentration in plasmic digests assayed by ELISA (Fig 3A). Before addition of thrombin to the plasma, XLFP concentration, the ratio of polymer to monomer, and the digest DD concentration were 180 f 52 pg/mL, .17 f .02, and 44 f 7 pg/mL, respectively. These values increased 1.3-, 1.2-, and 1.9-fold at .28 of the clotting time, 2.7-, 2-, and 3.1-fold at .57 of the clotting time, and to 7.4-, 5.8-, and 7-fold at .86 of the clotting time. Regression analysis indicated a high correlation between D-dimer immunoreactivity in the plasmic digests and XLFP expressed as concentration (r = .98) (Fig 3B) or as the ratio of polymer/monomer (r = .80). D-dimer concentrations in the plasmic digests were also determined from densitometric scanning of Western blots of SDSpolyacrylamide gels (Fig 2B) and quantitated by comparison with a standard curve of purified fragment DD. Similar amounts of immunoreactive D-dimer were found in the digest by ELISA and by densitometric analysis of the gels (r = .87) (Fig 4). The D-dimer immunoreactivity in plasmic digests of 1.2 plasma from 12 normals was distributed over a narrow range, with a mean f SD of 25 2 7 pg/mL (Fig 5). After collection, maintenance of the blood sample at 4°C for up to 8 hours or at room temperature for up to 4 hours before centrifugation and preparation of plasmic digests did not alter the results (data not shown). Similarly, storage of citrated plasma at -70°C for up to 2 weeks before digestion did not alter the results obtained by ELISA. The addition of hirudin (20 U/mL), a specific thrombin inhibitor, or iodoacetamide (10 mmol/L), an inhibitor of factor XI& to plasma before digestion did not affect results, indicating a negligible effect of hemostatic activation during plasmic digestion. The interassay and intraassay coefficients of variance were both 13% with normal plasma. The concentration of XLFP in plasma from normal individuals was lower than that in pooled plasma after prolonged storage (Figs 2 and 3), reflecting storage-induced changes in the latter. Increased D-dimer immunoreactivity was found in plasmic digests of plasma from patients with thrombotic disorders (Fig 5). The mean f SD values for 10 patients with stroke was 88 2 32 pg/mL, for 14 patients with myocardial infarction 84 2 30 pg/mL, and for six patients with venous thrombosis 86 f 19 pg/mL. The values were distributed over a wide range of 32 to 144 pg/mL, but only 4 of the 30 samples from patients were within the range of normals, and the mean D-dimer concentration of the digested plasmas in each patient group was significantly higher than in normal plasma (P < .005). 1200 1.0 1000 .8 800 .6 600 .4 400 , .2 0 04 0 .2 .4 .6 TimeIClotting Time .8 1.0 A 0 200 400 600 800 1000 Fibrin Polymer (pglml) 1200 1400 6 Fig 3. Measurementof XLFP in thrombin-treatedplasma samples and D-dimer immunoreactivity of plasmic digests. (A) Thrombin (0.01 U/mL) and calcium chloride (10 mmol/L) were added to stored, pooled normal plasma, incubated at 37"C, and aliquots withdrawn at the indicated intervals as in Fig 2A. Samples were subjected to SDS 2% agarose electrophoresis and Western blotting with antifibrinogenantiserum, and the concentration of plasma fibrin polymer (0-0) was determined by gel scanning and comparison with a standard curve of purified fibrinogen at known concentrations. The ratio of polymer/monomer (x-x) was determined directly from the gel scan tracing. Plasmic digests of the same plasma aliquots were preparedand D-dimer immunoreactivity (0-0) of the digests was measured by ELISA. The values representmean -c SD of three experiments. (B) Correlation between plasma Concentration of XLFP and D-dimer immunoreactivity in plasmic digests. As determined by linear regression, the equationfor the line is y = .23X 23 (r = .98). + From www.bloodjournal.org by guest on February 6, 2015. For personal use only. QUANTITATION OF CROSSLINKED FIBRIN POLYMERS 500 713 normals (P < .005) (Table 1).Similarly, the D-dimer immunoreactivity in plasmic digests of plasma from each of the three patient groups was significantly higher than in normals (P < .005). Just as was found for XLFP prepared in vitro (Fig 3), linear regression analysis showed a good correlation (r = .87) between the plasma concentration of XLFP and the D-dimer immunoreactivity of plasmic digests (Fig 7), with a best-fit equation of y = .28X + 28. D-dimer immunoreactivity in the digests measured by ELISA was closely correlated with D-dimer concentration determined by band intensity after SDS-PAGE (Fig 6B). 1 400 \ P, 3. L DISCUSSION 0 100 200 300 400 DD by ELSA (pg/ml) Fig 4. Comparison of D-dimer concentration in plasmic digests of thrombin-treated plasma as measured by ELSA and gel analysis. Plasma was incubated with 0.01 U/mL thrombin and 10 mmol/L calcium chloride and aliquots were withdrawn at intervals up to the time of clot formation as in Fig 1. Digests were prepared and subjected to SDS 4% to 10% gradient PAGE and Western blotting with antifibrinogen antiserum. D-dimer concentration in plasmic digests was measured by ELISA and by gel scanning in comparison with a standard curve of purifiedfragment DD. The values are derived from three experiments. The equation of the line as determined by linear regression is y = .98X 47 (r = .87). In the present study, we have shown that the D-dimer immunoreactivity of plasmic digests of plasma reflects the concentration of plasma XLFP. To obtain this result, complete degradation to fragment DD was necessary because less complete digests contain heterogeneous mixtures of larger crosslinked fibrin degradation products with lower imm~noreactivity.~~ Incubation of plasma with rt-PA at a high concentration (200 p,g/mL) degraded XLFP incompletely, but the addition of supplemental plasminogen (5 U/mL) to plasma containing rt-PA at a lower concentration (25 pg/mL) resulted in complete degradation. This is consistent with a prior report showing incomplete degradation of fibrinogen and XLFP after incubation of plasma in vitro with plasminogen and also with the demon- 140 + The plasma samples from normals and patients that were used to prepare plasmic digests were also evaluated by SDS-agarose electrophoresis and Western blotting (Fig 6A). Bands corresponding to XLFP were faint in normals, but were clearly visible, although to a variable extent, in the three patient groups. After plasmic degradation, prominent bands corresponding to fragments D and E were present by SDS-PAGE and were approximately the same in all samples (Fig 6B). A band corresponding to fragment D-dimer could not be clearly identified in plasma from normals, indicating that its concentration was less than 100 p,g/mL, which is the limit of sensitivity of the electrophoretic method. The prominence of the fragment DD band by SDS-PAGE in patient samples corresponded to the intensity of XLFP in the same sample by SDS-agarose electrophoresis. For example, fibrin polymer bands were faint on the SDS-agarose gel in the patient with stroke in lane 4 of Fig 6A, and no clearly identifiable D-dimer band was present in the corresponding SDS-PAGE. In contrast, XLFP bands were prominent in the samples from a patient with stroke in lane 7 and with acute MI in lane 10, and the fragment DD band was easily identified in the corresponding digest samples (Fig 6B). The concentration of XLFP and the polymer/monomer ratio in patient samples were significantly higher than in 120 ? 100 \ 0 a L Q Q 80 60 $ 8 20 0 I I I I Normals Stroke I I t Myocardial Deep Vein Infarction Thrombosis Fig 5. DD concentration in plasmic digests of plasma from normals and patients with thrombotic disease. Plasma from normals and patients was incubated with 25 pg/mL rt-PA and 5 U/mL plasminogen. D-dimer immunoreactivityin the plasmic digests was measured by ELISA. From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 714 KORNBERG, FRANCIS, AND MARDER Normals Trimer Myocardial Infarction Stroke 1 2 3 4 5 6 7 16 22 28 80 160 150 280 8 9 Deep Vein Thrombosis 10 11 - 120 170 220 320 2 3 Myocardial Infarction Stroke Normals 4 5 6 7 8 - 9 10 11 220 260 310 A Fibrin Polymer (pglml) 1 12 13 14 Deep Vein Thrombosis 12 13 14 I '"* - DD - I =- & I ' : ._I I I 20 14 31 40 96 102140 DD 88 98140100 97 106106 by ELISA (pg/ml) stration that plasminogen depletion limits in vitro degradation of plasma clots incubated in plasma with rt-PA.'* Incomplete degradation of fibrinogen also occurs in vivo, with a predominance of fragment X during thrombolytic therapy with streptokinase or t-PA.J3 Table 1. Content of plasma XLFP and of D-Dimer in Plastic Digests of Plasma From Normals and Patients With Thrombotic Disorders Normals In = 12) Acute MI In = 14) Venous Stroke Thrombosis In = 101 In = 6 ) Plasma XLFP concentration (m/mL) 28 f 12 217 f 110 150 f 83 187 f 80 Plasma ratio of polymer/ monomer .16 f .02 .30 t .1 .28 f .13 .32 f .06 D-dimer concentration in plasmic digests (rrg/mL) 25 t 7 84 t 30 88 t 32 86 f 19 All values are mean t SD. B ]E Flg6. Electrophoretkanalysis of fibrinogenderivin plasma from normals and patients with thrombotic disease M o m and after degradation. (A) Untreatedplasma. Plasma from normals and patients was subjected to SDS 2% agarose electrophoresis followed bv Western blotting - with antifibrinwen antiserum. The plasma concentration of XLFP was determined by densitometric scanning using a standard curve derived from purified fibrinogen at known concentrations. (B) Plasma digests. Plasmic digests of the same plasma samples from normals and patients were prepared and aliquots subjected to SDS 4% to 10% gradient PAGE followed by Western blotting with antifibrinogen antiserum to determine D-dimer concentration. The locations of fragments DD, D, and E are indicated. Bands migrating between DD and D are not identified but may represent fragment Y or heterogeneity of DD resulting from additional proteolytic changes. Ddimer immunoreactivity in the plasmic digests was measured by ELISA. Using the combination of rt-PA (25 pg/mL) and plasminogen (5 U/mL) to prepare plasmic digests of plasma, we explored the relationship between plasma XLFP content and D-dimer immunoreactivity of the digests. Plasma containing varying concentrations of XLFP was prepared by the addition of a low concentration of thrombin in vitro. A strong correlation was found between the concentration of plasma XLFP as determined by SDS-agarose gel electrophoresis and the D-dimer concentration of the plasma digest as measured by ELISA (r = .98) (Fig 3B). The reliability of measuring digest D-dimer by ELISA was confirmedby its significant correlation with D-dimer concentration estimated from Western blots after SDS-PAGE (r = .87) (Fig 4). A similar approach was used to evaluate XLFP in plasma from normals and patients with thrombotic disorders. The amounts of XLFP and of plasma digest DD were increased From www.bloodjournal.org by guest on February 6, 2015. For personal use only. QUANTITATION OF CROSSLINKED FIBRIN POLYMERS 715 I' " I I 0 100 I I 200 300 I 400 Fibrin Polymer (pg/ml) Fig 7. Correlation between the plasma concentration of XLFP and DD immunoreactivityin plasmic digests of plasma from normals and patients with thrombotic disease. Plasma from normals ( 0 )and patients with myocardial infarction (0). stroke (X), and deep vein thrombosis (A)was subjected to SDS-agarose electrophoresis followed by Western blotting with antifibrinogen antiserum, and the concentration of XLFP was determined by densitometric scanning of Western blots using standard curves of purified fibrinogen at known concentrations. Plasmic digests of the same plasma samples were preparedand D-dimer immunoreactivitywas measured by ELISA. The equation for the line is y = .28X 28 (I = .87), as determined by linear regression. + in patients compared with normals (Table l), with a good correlation between XLFP determined by gel electrophoresis and plasmic digest DD measured by ELISA (Fig 7). The amount of fragment D D detected by Western blotting of plasma digests (Fig 6B) corresponded to the amount of XLFP on SDS-agarose gels (Fig 6A) and to digest DD measured by ELISA, confirming that the measurement reflected the D-dimer concentration in the digest derived from XLFP. Although there was little overlap between the plasma digest DD values in normals and patients (Fig 5 ) , the small number of patients in each group limits conclusions about the diagnostic value of this approach in patients with thrombotic disease. The results indicate that D-dimer is the primary crosslinked plasmic degradation product of XLFP and thereby provide additional evidence that the yy isopeptide bond is the principal crosslink in soluble fibrin in plasma. This view is consistent with prior reports of the pattern of factor XIIIa crosslinking of fibrin in vitro using purified p r o t e i n ~ l ~in , ~ which ~ , ~ ~ y chains are crosslinked more rapidly than a chains. It is also consistent with several reports7J5J7Jssuggesting that soluble fibrin contains mainly yy crosslinks. Shainoff et aP6 have also found crosslinked fibrin polymers in the plasma of normals and elevated levels in patients with thrombotic disease similar to those in this report. However, using direct immunoprobing of gels with monoclonal antibodies against individual fibrin chains, they detected both a-Aa and yy crosslinks in the polymers. Formation of Aa-a and Aa-y crosslinks has been attributed to tissue transglutaminase activity, whereas yy crosslinks are a product of factor XIII,.37 Our findings do not exclude the presence of some fibrin polymers crosslinked through a or A a chains. However, electrophoretic analysis of digests (Figs 2B and 6B) and the correlation between the plasma concentration of XLFP and D-dimer immunoreactivity (Figs 3 and 7) suggests that D-dimer is the predominant plasmic degradation product, and indicates that circulating XLFP are crosslinked primarily through y chains, both in the in vitro model and in normals and patients with thrombotic disease. Consistent with our prior report? we found a mean plasma concentration of XLFP of 28 p,g/mL in normal plasma by SDS-agarose electrophoresis. This is associated with D-dimer immunoreactivity after plasmic digestion of 25 kg/mL (Table 1). Linear regression of the correlation between plasma XLFP concentration and D-dimer immunoreactivity (Fig 7) derived the equation y = .28X + 28. An XLFP concentration of 28 pg/mL in normals predicts a digest D-dimer continuation of 36 kg/mL, close to the observed mean in normals of 25 pg/mL (Table 1). The slope of .28 indicates an increase of D-dimer iqmunoreactivity of 280 kg/mL for an increase of 1,000 kg/mL in plasma XLFP, and is close to the value of .29 predicted on the relative mass of the D-dimer portion of a fibrin dimer, which is the predominant polymeric species present before degradation. This analysis, together with the highly significant correlation between digest DD concentrations measured by ELISA and by SDS-PAGE densitometry, suggest that increases in D-dimer immunoreactivity in plasma digests accurately reflect elevated levels of XLFP and prove that the measurements by the 3B6/4D2 ELISA reflect the actual concentrations of D-dimer in the plasmic digests of plasma. It has been s ~ g g e s t e d ~that ~ 9the ~ D-dimer immunoreactivity using the 3B6/4D2 assay can be falsely elevated in the presence of high concentrations of fragment D because the secondary antibody (4D2) reacts with both fibrin and fibrinogen degradation products. However, prior reports have found no reaction with the assay at fragment D concentration of up to 200 ~ g / m L , 3which ~ , ~ ~far exceeds the concentration of fragment D in the sample after dilution. Further, a concentration of fibrinogen degradation products of 2,200 pg/mL gave a reaction using the assay of only 1,300 ng/mL.39 Therefore, even if there is some level of crossreactivity or any other effect of fibrinogen degradation products on the 3B6/4D2 ELISA, the contribution to the total would be small but could contribute to the positive Y intercept of the linear regression analysis. The correlation between plasma XLFP and D-dimer immunoreactivity both in the in vitro model (Figs 2 and 3) and in normals and patients (Fig 7) indicates that the D-dimer level measured by ELISA after plasmic digestion may be a useful measure of the amount of XLFP in plasma from normals and patients with thrombotic disorders. Plasma soluble fibrin has been measured previously by several techniques, based on its unique physical and chemical properties. Musumeci et a1,2 using gel filtration chromatography, and Edgar et al: using affinity chromatography, reported levels of 25 p,g/mL and 27 kg/mL, respectively, in normals, values similar to our findings. Others have reported higher levels in normals of 120 to 184 kg/mL using gel filtration c h r o m a t ~ g r a p h y ~and . ~ ,lower ~ levels of 3 to 7 kg/mL using affinity chromatography6 and chromogenic From www.bloodjournal.org by guest on February 6, 2015. For personal use only. KORNBERG, FRANCIS, AND MARDER 716 assay." The different concentrations may be attributed to different molecular species of soluble fibrin measured using the various methods. Despite these differences, all methods identify an increase of between 3- and 10-fold in soluble fibrin in patients with thrombotic disea~e,l-~.~Jl similar to our findings (Table 1).However, most nf these techniques are difficult to perform and impractical for routine clinical use. Our approach is based on the specificity of D-dimer as a marker for XLFP20,21,23,29 and the significant correlation between plasma XLFP and D-dimer immunoreactivity of plasmic digests. The results indicate that measurement of D-dimer immunoreactivity in plasmic digests may be useful in evaluation of hypercoagulable states by providing a simple and accurate measure of the plasma content of XLFP. ACKNOWLEDGMENT The authors acknowledge the technical assistance of Kristina Klingbeil and the help of Carol Weed in preparation of the manuscript. REFERENCES 1. Fletcher AP, Alkjaersig N, Davies A, Lewis M, Brooks J, Hardin W, Landau W, Raichle ME: Blood coagulation and plasma fibrinolytic enzyme system pathophysiology in stroke. Stroke 7:337, 1976 2. Musumeci V, Culasso D, Boni P: A rapid chromatographic method for quantitation of high molecular weight fibrinogen derivatives in plasma. Thromb Haemost 39555,1978 3. Neri Serneri GG, Gemini GF, Abbate R, Favilla S: Occurrence of soluble very high molecular weight fibrinogen complexes in hypercoagulable states. An in v i m and in vivo study on their features. Thromb Haemost 42:1561,1979 4. Fletcher AP,Alkjaersig NK, Ghani FM, Tulevski V, Owens 0: Blood coagulation system pathophysiology in acute myocardial infarction: The influence of anticoagulant treatment on laboratory findings. J Lab Clin Med 93:1054,1979 5. Edgar W, Mckillop C, Howie PW, Prentice CRM: Composition of soluble fibrin complexes in pre-eclampsia. Thromb Res 10567,1977 6. Matthias FR, Reinicke R, Heene DL: Affinity chromatography and quantitation of soluble fibrin from plasma. Thromb Res 10:365,1977 7. Ishikawa A, Iwasaki Y Rapid estimation of soluble fibrin monomer complexes by high performance liquid chromatography for the purpose of early detection of DIC. Thromb Res 30:521, 1983 8. Connaghan DG, Francis CW, Lane DA, Marder VJ: Specific identification of fibrin polymers, fibrinogen degradation products, and crosslinked fibrin degradation products in plasma and serum with a new sensitive technique. Blood 65:589,1985 9. Francis CW, Connaghan DG, Scott WL, Marder VJ: Increased plasma concentration of cross-linked fibrin polymers in acute myocardial infarction. Circulation 75:1170,1987 10. Proietti AB, McGuire M, Bell W: Specific identification of fibrin(ogen) degradation products in plasma and serum using blotting and peroxidase labeled antiserum. Am J Hematol34:270, 1990 11. Wiman B, Ranby M: Determination of soluble fibrin in plasma by a rapid and quantitative spectorphotometric assay. Thromb Haemost 55:189,1986 12. Kierulf P, Godal HC: Fibrinemia in medical patients screened by the ethanol test. Acta Med Scand 190185,1971 13. Gurewich V, Hutchinson E Detection of intravascular coagulation by serial-dilution protamine sulfate test. Ann Int Med 75:895, 1971 14. Chen R, Doolittle R F y-y Crosslinking sites in human bovine fibrin. Biochemistry 10:4686, 1971 15. Kierulf P: Studies on soluble fibrin in plasma. V. Isolation and characterization of the clottable proteins obtained from plasmas upon gelation with ethanol. Thromb Res 4:183,1974 16. Ly B, Jakobsen E: Some aspects of the bonds interlinking soluble fibrin complexes in human plasma. Thromb Res 6:65, 1975 17. Selmayer E, Muller-Berghaus G: Soluble crosslinked fibrin(ogen) polymers. Thromb Haemost 542304,1985 18. Graeff H, Hafter R, Bachmann L Subunit and macromolecular structure of circulating fibrin from obstetric patients with intravascular coagulation. Thromb Res 16:313, 1979 19. Ittyerah R, Alkjaersig N, Fletcher A, Chaplin H: Coagulation factor XI11 concentrates in sickle-cell disease. J Lab Clin Med 88546,1976 20. Pizzo SV, Schwartz ML, Hill RL, McKee P A The effect of plasmin on the subunit structure of human fibrin. J Biol Chem 248:4574,1973 21. Pizzo SV, Taylor LM Jr, Schwartz ML, Hill RL, McKee P A Subunit structure of fragment D from fibrinogen and cross-linked fibrin. J Biol Chem 248:4584,1973 22. Francis CW, Marder VJ, Barlow GH: Plasmic degradation of crosslinked fibrin. Characterization of new macromolecular soluble complexes and a model of their structure. J Clin Invest 66:1033,1980 23. Gaffney PJ, Brasher M: Subunit structure of the plasmininduced degradation products of crosslinked fibrin. Biochem Biophys Acta 295:308,1973 24. Brenner B, Francis CW, Marder VJ: The role of soluble crosslinked fibrin in D dimer immunoreactivity of plasmic digests. J Lab Clin Med 113:682,1989 25. Brenner B, Francis CW, Totterman S, Kessler CM, Rao AK, Rubin R, Kwaan HC, Gabriel KR, Marder VJ: Quantitation of venous clot lysis with the D-dimer immunoassay during fibrinolytic therapy requires correction for soluble fibrin degradation. Circulation 81:1818, 1990 26. Olexa SA, Budzynski Az: Primary soluble plasmic degradation product of human cross-linked fibrin. Isolation and stoichiometry of the (DD)E complex. Biochemistry 18:991,1979 27. Neville DM Jr: Molecular weight determination of proteindodecyl sulfate complexes by gel electrophoresis in a discontinuous buffer. J Biol Chem 246:6328,1971 28. Towbin H, Staehelin T, Gordon J: Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: Procedure and some applications. Proc Natl Acad Sci USA 76:4350,1979 29. Francis CW, Doughney K, Brenner B, Klingbiel K, Marder VJ: Increased immunoreactivity of plasma after fibrinolytic activation in an anti-DD ELISA system. Role of soluble crosslinked fibrin polymers. Circulation 79:666, 1989 30. R latt DB, Blake AS, Cottis LE, Massingham DA, Fletcher WA, Masci PP, Whitaker AN, Elms M, Bunce I, Webber AJ, Wyatt D, Bundesen PG: An immunoassay for human D dimer using monoclonal antibodies. Thromb Res 31:767,1983 31. Elms MJ, Bunce IH, Bundesen PG, Rylatt DB, Webber AJ, Masci PP, Whitaker AN: Measurement of crosslinked fibrin degradation products-An immunoassay using monoclonal antibodies. Thromb Haemost 50:591,1983 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. QUANTITATION OF CROSSLINKED FIBRIN POLYMERS 32. Onundarson FT, Francis CW,Marder VJ: Depletion of plasminogen in vitro or during thrombolytic therapy limits fibrinolytic potential. J Lab Clin Med (in press) 33. Owen J, Friedman KD, Grossman BA, Wilkins C, Berke AD, Powers ER: Quantitation of fragment X formation during thrombolytic therapy with streptokinase and tissue plasminogen activator. J Clin Invest 791642,1987 34. Pissano JJ, Finlayson JS, Peyton MP: Cross-link in fibrin polymerized by factor XIII: e(y-glutamyl) lysine. Science 1602392, 1968 35. Doolittle RF, Chen R, Lau F Hybrid fibrin: Proof of the intermolecular nature of y-y crosslinking units. Biochem Biophys Res Commun 44:94,1971 36. Shainoff JR, Valenzuela R, Urbanic DA, DiBello PM, Lucas 717 FV, Graor R: Fibrinogen Aa and y-chain dimers as potential differential indicators of atherosclerosis and thrombotic vascular disease. Blood Coag Fibrinol1:499,1990 37. Murthy SNP, Lorand L Cross-linked Aa-y chain hybrids serve as unique markers for fibrinogen polymerized by tissue transglutaminase.Proc Natl Acad Sci USA 87:9679,1990 38. Eisenberg PR, Jaffe AS, Stump DC, Collen D, Bovill EG: Validity of enzyme-linked immunosorbent assays of cross-linked fibrin degradation products as a measure of clot lysis. Circulation 82:1159,1990 39. Lawler CM, Bovill EG, Stump DC, Collen DJ, Mann KG, Tracy RP: Fibrin fragment D-dimer and fibrinogen Bp peptides in plasma as markers of clot lysis during thrombolytic therapy in acute myocardial infarction. Blood 76:1341,1990 From www.bloodjournal.org by guest on February 6, 2015. For personal use only. 1992 80: 709-717 Plasma crosslinked fibrin polymers: quantitation based on tissue plasminogen activator conversion to D-dimer and measurement in normal and patients with acute thrombotic disorders A Kornberg, CW Francis and VJ Marder Updated information and services can be found at: http://www.bloodjournal.org/content/80/3/709.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.






© Copyright 2026