
CBO Lowers ACA Net Cost Projections Drop By $101M Congress
Vol. 3, No. 5 — February 4, 2015 Exchange Round-Up House Votes Full ACA Repeal, Tax Season Kicks Off, Enrolling Winds Down House Republicans Tuesday easily passed legislation that would repeal the Affordable Care Act and require the committees of jurisdiction to present a replacement bill in six months. The president’s budget, meanwhile, requests $629 million in budgetary authority to support exchange functions as the administration expects to collect about $1.56 billion in user fees. HHS has also included $380 million under the establish grant funding line to help support state decisions and potential transitions from one exchange type to another. The $2.2 billion total includes $1.56 billion in user fees and $629 million in requested budget authority that would continued on page 10 Insurers, Hospitals, More Unite With Dem Lawmakers Against King Plaintiffs Insurance advocates, hospital groups, unions, public health experts and others on Wednesday (Jan. 28) filed friendof-court briefs defending premium tax credits in the federally-operated marketplace, joining consumer advocates and lawmakers who crafted versions of the Affordable Care Act in opposition to the plaintiffs in King v. Burwell ahead of oral arguments at the U.S. Supreme Court in March. Amicus briefs supporting the Obama administration were due this week, while those in favor of the plaintiffs were due Dec. 29. Families USA Executive Director Ron Pollack told Inside Health Policy Tuesday (Jan. 27) that he expected around two dozen friend-of-court briefs to be filed in support of the administration Wednesday (Jan. 28). continued on page 6 Obama’s Budget Outlines $2.2B Needed To Fully Fund ACA Implementation Health insurance exchanges are estimated to cost the federal government $2.2 billion in fiscal 2016, according to President Obama’s fiscal 2016 budget request that fully funds Affordable Care Act implementation. Across all accounts, the administration is requesting $639 million for marketplace operations, $808 million for consumer information and outreach, $657 million for marketplace information technology and $85 million for federal administration. The $2.2 billion total includes $1.56 billion in user fees and $629 million in requested budget authority that would fund CMS activities and administrative expenses toward the exchanges as well as cover $544 million to support the growth and operations of exchange activities like eligibility, plan management and quality improvement. continued on page 8 HHS Has $380M In Grant Funds That May Support Exchange Transitions The Obama administration lists $380 million in left-over health insurance exchange grants in its fiscal 2016 budget and signals states may put some of that money toward a move from one type of marketplace to another, while being unclear about how exactly those funds may be used. “CMS will continue to support transitions that may occur over the next year and the support needed thereafter” in changing from a state partnership marketplace to a state-based exchange, or from using the federally-operated marketplace to a partnership, according to the CMS budget justification released Monday night (Feb. 2). The funds would come at a crucial time for states that may need to scramble to create their own marketplace if the continued on next page IN THIS ISSUE . . . Boustany Bill Would Let Employers Help With Premiums .......................................................................... p3 Administration Holds Off On SEP, Says 6M Could Save Penalties .......................................................... p13 Finance Dems, GOP Propose ACA Fixes In ‘Heroes’ Markup ................................................................... p14 IRS Waives Penalties For Those Who Don’t Rectify Tax Credits by April 15 .......................................... p16 U.S. Supreme Court rules against the administration in King v. Burwell, effectively disallowing premium tax credits from being distributed to low-income Americans in states that offer health care plans through the federal exchange. Though the justification adds that grants will not be awarded after Dec. 31, 2014, the document adds that CMS requires “administrative resources for continued activities” in fiscal 2016. Some states will still be in the development stage of establishment and will need further technical assistance, the document says, as well as improving functions of renewals, privacy and security, and calculating and reporting advance payments for premium tax credits. “Funding will also be used for contracts to provide States with instruction on establishment of Marketplace business functions (e.g., eligibility, plan management) and to help States use their grant funding to implement programmatic components that are in line with Federal policy,” the budget justification says. The ACA appropriated funding as needed to help states stand up their exchanges, but required the marketplaces to be self-sustaining as of Jan.1, 2015. However, CMS has said states can continue using the grant money for certain functions. “States may use Establishment grants to fund their start-up costs, whether for State-based or State Partnership Marketplace function, or to support the Federally-facilitated Marketplaces, but ongoing operations are self-funded through user fees or other funding,” the HHS budget brief said. It is unclear whether the description referred to those grants paid out before the end of 2014 or the money that may be available in fiscal 2016. The money will also support an estimated 66 full-time equivalent staff members who work as project officers, grants management staff, technical help teams and managers to oversee state progress in their cooperative agreements. More than $5.5 billion was allocated to 37 states and Washington, DC to establish and build their own exchanges since 2011, including $2.1 billion in fiscal 2015. States may continue to spend grant money in 2015 and beyond, CMS said. — Rachel S. Karas Pelosi Disputes GOP’s Piecemeal Approach To Dismantling ACA House Minority Leader Nancy Pelosi (D-CA) said Tuesday (Feb. 3) she is confident the U.S. Supreme Court will rule in favor of the Obama Administration in King v. Burwell, for which oral arguments begin next month. Plaintiffs in that suit say the Affordable Care Act does not allow the federal government to pay premium subsidies to residents in states that receive help from the federal government running exchanges. “I don’t see how that’s a constitutional issue,” she said during an appearance at the Brookings Institution. Pelosi said earlier in a speech that affordable health care is a pillar of President Obama’s budget and a stable economy. Even if all Americans had health insurance, Congress would have needed to pass the Affordable Care Act to drive down unsustainably high health care costs. She said Republicans are wrong to think they can remove some parts but retain a functional whole. They support banning insurance companies from denying coverage to people with pre-existing conditions, but to do that the government must impose an individual mandate so that people don’t wait until they’re sick to buy insurance, which would drive up health care costs. If the government makes people buy insurance, it must help those with low incomes to afford it, she said. “You can’t take pieces of it,” she told Inside Health Policy. Pelosi also said that ACA supporters didn’t move quickly enough to deter arguments against health care reform that had “absolutely nothing to do with the bill” when it passed in 2010. “That really poisoned the well and we didn’t have an antidote out there early enough,” she said. “Public sentiment is everything. You can’t assume the public will understand this is in their interest.” She also said Democrats are willing to improve the bill, but they’re not willing to kill the law. “Any bill we pass can be subjected to scrutiny to say how can we do this better or that better in the implementation and of course we’re always, always open to that but not something that totally takes the heart of it and undermines it. It’s too important,”she said. — Rachel S. Karas SUBSCRIPTIONS: 703-416-8500 or 800-424-9068 [email protected] NEWS OFFICE: 703-416-8572 Fax: 703-416-8543 [email protected] 2 Health Group Publisher: Senior Editor: Associate Editor: Donna Haseley ([email protected]) Amy Lotven ([email protected]) Rachel Karas ([email protected]) Production Manager: Production Specialists: Lori Nicholson ([email protected]) Daniel Arrieta, Michelle Moodhe Health Exchange Alert is published every Wednesday by Inside Washington Publishers, P.O. Box 7167, Ben Franklin Station, Washington, DC 20044. Subscription rates: $705 per year in U.S. and Canada; $755 per year elsewhere (air mail). © Inside Washington Publishers, 2015. All rights reserved. Contents of Health Exchange Alert are protected by U.S. copyright laws. No part of this publication may be reproduced, transmitted, transcribed, stored in a retrieval system, or translated into any language in any form or by any means, electronic or mechanical, without written permission of Inside Washington Publishers. Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 Study Offers Ways To Boost Brokers’ Role In Marketplace Enrollment Despite facing certain obstacles at the beginning of the open enrollment process, insurance agents and brokers were instrumental in driving enrollment in many states and will continue to be as funding for other assisters falls, according to a brief by Georgetown University and the Urban Institute. The report, based on interviews with brokers in 21 states and the District of Columbia, pinpoints several changes that would help agents and brokers enroll more people in the coming years. “As the federal government and states direct less funding to navigators, a real opportunity exists for brokers to play a major role in enrollment in marketplaces,” said Kathy Hempstead, who directs coverage issues at the Robert Wood Johnson Foundation. “Brokers have a unique skill set, and the non-group market is a growing opportunity. With better supports and incentives, brokers could be even more effective in enrolling low-income consumers.” Lack of experience with the low-income community was one of the many challenges faced by brokers, the report says. Brokers and agents also had issues with the exchange site technology and overburdened marketplace calls centers that were staffed by people who did not have the proper expertise, according to several people interviewed in the survey. The report offers six changes that would help brokers with enrollment nationwide. These include: easy-to-use directories to help people identify a nearby broker for enrollment assistance; improved, hands-on broker training; improved IT systems that speed marketplace enrollment; compensation for enrolling low-income individuals and families in Medicaid; marketplace customer support tailored for the broker community; and ongoing monitoring of broker-assisted enrollment to identify problems or barriers more quickly. Jessica Waltman of the National Association Health Underwriters, which represents brokers and agents, in response to the report stressed that licensed, professionally trained health insurance brokers “have been an important source of coverage help for individual health insurance consumers in both state exchanges and the federal exchange from day one.” “Despite many challenges with the exchanges last year, they helped millions of people obtain coverage and have serviced their clients’ exchange-based coverage throughout the coverage year and this current open enrollment season,” she said. She also notes that NAHU has called for many of the changes in the report for more than a year. “Increased tools for brokers to help people get covered and stay covered are particularly important since a broker works with their client year-round to ensure that the client has coverage that fits their specific needs and can utilize it effectively,” she says. — Amy Lotven Boustany Bill Would Let Employers Help With Premiums Rep. Charles Boustany (R-LA), chairman of House Ways and Means oversight subcommittee, aims to introduce a tweaked version of his bill amending the Internal Revenue Code to treat employer payments for employee health care premiums and amounts paid to health reimbursement arrangements for their employees as medical expenses under accident or health plans, excluding them from gross income for tax purposes. Boustany’s senior health adviser, Melissa Gierach, said she is reviewing the bill introduced in December to potentially tweak details that could make the legislation more functional and targeted to achieve its goal, but nothing that would change its overall intent. The congressman hopes to get the bill reintroduced as quickly as possible this Congress, hopefully in the next two weeks before recess begins Feb. 16, she said. A potential Senate partner on the bill might be Sen. Chuck Grassley (R-IA), who on Jan. 28 offered an amendment to the Hire More Heroes bill that would allow small business owners to offer their employees financial help to buy health insurance on a pre-tax basis. He based his amendment on the Boustany bill, Gierach said. Grassley did not ask for a vote on the amendment while the Finance Committee marked up the “Heroes” bill, which would exempt veterans from the employer mandate’s employee count caps. He said he hopes to work with Finance Chairman Sen. Orrin Hatch (R-UT) to later address the issue. Katie Mahoney, executive director of health policy at the U.S. Chamber of Commerce, said the business lobby had a few concerns with the first iteration of Boustany’s bill but declined to elaborate on what future fixes might be. She said the ACA’s provisions that block employers from providing HRAs to their employees are problematic, and the Chamber would like to see more flexibility for employers. “We look forward to working with Boustany to achieve this goal and view it as an important tool for employers … as a defined contribution system emerges,” she said Thursday (Jan. 29). The Chamber has not formally come out in support of the bill but does view it as tackling a significant issue. In the meantime, Mahoney said, employers are exploring ways to move to a defined contribution system like using private exchanges, while being mindful of competing tax implications due to possible “double-dipping” with premium tax credits. Boustany’s proposal last year had a few pieces that the Chamber sought to revise, but Mahoney would not elaborate on what changes might be made. She was unaware of Grassley’s amendment last week but called it very interesting and Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 3 said she would look into it. Last week, Boustany also introduced a bill to repeal part of the ACA and amend the Public Health Service Act to allow cooperative governing of individual health insurance coverage offered in multi-state businesses. Neither bill has been scheduled for a vote. — Rachel S. Karas Congressional CHIP Advisers Weigh Program Extension Alternatives Congressional Medicaid and CHIP advisers late last week looked at a handful of potential alternatives to extending the Children’s Health Insurance Program, which expires in 2016. The advisers discussed the following options without formally weighing in on them: augmenting existing exchange subsidies, which currently help with the cost of premiums for those earning up to 400 percent of the federal poverty level and help cover cost sharing for those earning up to 250 percent of the federal poverty level; providing wrap-around coverage for things that exchange and work plans may not cover, like dental plans; and increasing Medicaid coverage. The Medicaid and CHIP Payment and Access Commission met Thursday (Jan. 21) to discuss the potential end of the CHIP program and how to address the needs of the 1.1 million children who would lose coverage, as children’s advocates step up pressure on Congress to act by March to extend the program for four years. The commission is looking both at what effects the expiration of CHIP would have on current enrollees as well as possible ways to cover those children through other methods. A study by the Urban Institute showed families that lose coverage may face significant financial barriers in securing coverage for their children. Of the 1.1 million projected to become uninsured if CHIP expires, about 40 percent would be eligible for subsidized exchange coverage. The other 60 percent could move to their parents’ employer plans, though this would likely cost over $5,500 in out-of-pocket premiums, or 13.2 percent of their likely income, the Urban Institute study concludes. Noting CHIP’s very low cost-sharing, several commissioners expressed concern over the new payments families would be taking on if the program expires. Of the projected 1.1 million that would go uninsured, only 600,000 are ineligible for exchange subsidies. Families with parents already enrolled in the exchange would have little change in premium costs, but those not already enrolled in the exchange would be faced with enrolling in plans that would be six to 11 times more expensive than CHIP. And while premiums would not change much for those families that are already part of the exchange, the families’ out-of-pocket costs would be seven to 15 times greater, according to information presented to MACPAC. Commissioner Mark Hoyt said there may be sticker shock, with many families unable or unwilling to spend more. “That strikes me as a pretty significant hurdle to join one of those two pools,” he said of exchange and work coverage. Commissioner Sharon Carte was also concerned about future cost-sharing for families currently enrolled in CHIP, many whom have little disposable income or even tend to spend more on basics than they earn, according to a report included in the chapter presented to MACPAC commissioners. “Cost-sharing can be designed in a way that presents an access barrier,” she said. “You can have coverage, but if there’s not access what’s it really worth?” Several commissioners also said they were concerned about the idea of bringing all the CHIP kids into existing insurance pools as that would increase insurers’ risk. In addition to the risk issue, commissioners questioned the financial aspects of funding subsidies, the financial burden states would take on if Medicaid was expanded to cover the CHIP population, and whether the costs of adding kids to exchange or work plans would incentivize parents to cut hours at work in order to have children, especially particularly sick ones, qualify for Medicaid. The commission also discussed the recently expired primary care pay bump for Medicaid and the program’s coverage of mental health issues. — Rebecca Beitsch HHS OIG Seeks Additional Funding To Expand ACA Oversight The HHS Office of Inspector General requested $417 million for fiscal 2016, including an $83 million increase and 38 additional full-time employees for oversight and investigations related to the health insurance marketplaces. OIG also seeks an increases of $70 million and 192 employees for Medicaid and Medicare oversight. OIG says that it will initiate at least five to 10 ACA-related reviews in addition to the ones outlined in its 2015 work plan released in November. “These reviews could focus on emerging Marketplace issues, including, for example, vulnerabilities that may arise in connection with the second open enrollment period; implementation of additional Marketplace functionality, such as the redetermination process; or the premium stabilization programs. They could also focus on other ACA areas, including Medicaid expansion, new Medicare payment and delivery models, or new grant programs. The ACA marketplaces add a substantial new dimension to HHS’ landscape, OIG says in its budget justification, 4 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 noting the exchanges must implement and successfully operate complex program requirements. OIG’s oversight of the marketplaces focuses on payments, eligibility, management and administration, and security. By focusing on these key areas, OIG hopes to ensure that taxpayer dollars are spent for their intended purposes in a system that operates efficiently and is secure, the department says. OIG’s budget justification document also responds to several requests Congress had included in the omnibus spending bill enacted in December. The omnibus agreement provided an additional $24 million to OIG for ACA oversight activities. OIG says an advisory team has already met and the department is on schedule to provide Congress with a plan in mid-February for how it will use that funding. Congress also expected OIG to ensure that full oversight of ACA activities are in the 2015 work plan. The plan was released in November, and OIG says it is planning a mid-year update to keep Congress informed. OIG is prioritizing three areas: health insurance marketplaces, including the payments for financial assistance, Medicare and Medicaid reforms, and grant expenditures. The department is also preparing a report to the HHS secretary and congressional appropriators with the top 25 unimplemented recommendations that the OIG believes should be prioritized and has committed to make the report “more targeted” than in prior years. That report is slated to be out prior to 90 days after the enactment of the spending bill signed Dec. 16. OIG had been asked to provide no later than June 1 a report to Congress assessing the IRS procedures to reconcile the tax credits and to look at how HHS uses IRS information to reduce fraud and overpayments. OIG says it is working closely with the Treasury Inspector General for Tax Administration (TIGTA) on that report, and also says it expects that between itself and the TIGTA “a range” of reports related to the APTCs will be issued. — Amy Lotven House GOP Creates ACA Task Force, CBO Can’t Score Repeal Bill The chairs of the House committees of jurisdiction have launched a working group tasked with developing a replacement plan for the ACA as well as a contingency plan should the high court invalidate the federal exchange subsidies, House Majority Leader Kevin McCarthy (R-CA) announced Friday (Jan. 30). Also on Friday, the Congressional Budget Office told House Rules Committee Chair Pete Sessions (R-TX) that the agency would be unable to provide a score for a full ACA repeal bill (HR 596) that the House is slated to take up on Tuesday (Feb. 3). The task force, which consists of Energy and Commerce Chair Fred Upton (R-MI), Ways and Means Chair Paul Ryan (R-WI), and Education and Workforce Chair John Kline (R-MN), “recognizes that full repeal requires a thoughtful replacement strategy,” McCarthy said in his announcement. “Each of these chairmen and their committee members have been working on patient-centered solutions to help people with the problems created by Obamacare for many years. The group will also develop a contingency plan — consistent with an ultimate full replacement plan — to enact in case the Supreme Court rules in King v. Burwell that Obamacare subsidies offered on the federal exchange are illegal,” the announcement said. “This law is fundamentally flawed: It takes power away from the patient and hands it to bureaucrats. Instead of making people’s health care decisions easier, in many cases it makes those decisions for them,” the three Chairs said in a joint statement on the task force. “That’s why the American people need patient-centered solutions to replace Obamacare. Ours will put individuals and families in the driver’s seat and use the principles of choice and competition to make highquality health care more affordable and accessible for all.” “At the same time,” they add, “this latest court case against Obamacare is yet another sign that the law was a costly mistake. If the Supreme Court rules as we expect—that the law clearly doesn’t allow subsidies to be offered on the federal exchange—then millions more families will have their coverage in danger because Obamacare is fundamentally flawed.” The Supreme Court is slated to hear oral arguments in the case on March 4. Various House committees have pressed both HHS and IRS to reveal the administration’s contingency plans if the the Court rules in favor of King. The administration has been — and is expected to remain — tight-lipped about any planning, and has continued to express confidence that the justices will rule in its favor. McCarthy also announced Friday that the House will vote on Rep. Bradley Bryne’s (R-AL) full ACA repeal bill on Tuesday. It’s unclear how the bill would impact the budget, however, because CBO says it cannot be scored prior to the vote. “Preparing an estimate of the budgetary impact of that legislation would take CBO and the staff of the Joint Committee on Taxation at least several weeks because there are hundreds of provisions in the law that would be repealed and those provisions are in various stages of implementation. Therefore, we are unable to provide such an estimate at this time,” CBO writes. — Amy Lotven Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 5 Amicus Brief Filed In King . . . begins on page one The case threatens to pull health insurance subsidies from nearly 10 million Americans who enrolled in coverage through the federal exchange and partnership marketplaces. America’s Health Insurance Plans (AHIP), the American Hospital Association and others argued that offering tax credits to low-income people who qualify for assistance only in states that run their own exchanges would not only be a disaster for families and individuals who cannot otherwise afford coverage, but would also destroy the health care system as it now stands under the ACA. “We will not mince words: Petitioners’ position, if accepted, would be a disaster for millions of lower and middleincome Americans. The ACA’s subsidies have made it possible for more than 9 million men, women, and children to have health care coverage — some for the first time in years; some, no doubt, for the first time in their lives. That coverage allows them to go to the doctor when they are sick, and to do so without fear that the resulting bill could leave them in financial distress,” the American Hospital Association, Federation of American Hospitals, Association of American Medical Colleges and America’s Essential Hospitals wrote in their brief filed Wednesday. “If Petitioners’ interpretation is accepted, however, that salutary development will be reversed. The ranks of the uninsured will swell again, with all that portends in the way of untreated illness and overwhelming debt.” An ACA without subsidies would leave hospitals unable to make up funds that were cut when the law was passed — with the expectation that new patients using their new tax credits would replenish the deficit, the AHA wrote. “That could imperil some hospitals, and will make it more difficult for others to carry out their missions, including effectively serving their communities.” AHIP said in its own brief filed this week that pulling subsidies would create substantially dysfunctional insurance markets and far higher costs than if the ACA had not been enacted. Premium tax credits and shared responsibility payments are essential to an actuarially viable marketplace because they are key to ACA market reforms, the insurers said. “There is no practical reason to distinguish between State- and federally-operated exchanges in this regard,” AHIP wrote. “The ACA’s shared responsibility obligation and eligibility for premium assistance tax credits are governed by nationally established standards with payment from the federal treasury, regardless of which sovereign administers the particular exchange. It makes no difference to the market reforms whether the exchange is State- or federally-operated. Likewise from the perspective of consumers, State- and federally-operated exchanges perform the same basic functions — facilitating the comparison of plan choices, the determination of eligibility, and the enrollment process.” A brief filed by 131 current and former members of Congress and state legislators, including the House and Senate leaders who crafted the bill, said that limiting subsidies to state-based exchanges was never their intent and doing so would contradict their longtime goal of providing universal health care. “If, as Petitioners argue, the threat of cutting off access to insurance for upwards of 80% of the individuals expected to gain access through the Exchanges was a ‘stick’ to encourage state officials to establish state Exchanges, Congress surely would have communicated to the States that the availability of the tax credit turned on the establishment of a state Exchange, and the States would have understood that message. Neither event happened,” the lawmakers wrote. The hospitals agreed that creating such a narrow definition was not what Congress meant to do and not what lawmakers wrote. “One clause of Section 36B might support Petitioners’ position when read in total isolation. But when read in light of the ACA’s definitions of the word “Exchange” and the rest of the Act’s text and structure — as it must be — the clause does not. It instead extends subsidies to residents across the country. This Court should so hold. And it should reject Petitioners’ contrary interpretation, which creates absurdities across the statute that Petitioners cannot explain.” But friends of the petitioners did try to explain their position, in 21 briefs filed last month. Fifteen Republican Congressional leaders wrote a brief alleging that the plain text of the law is indeed grounds for conditionality and that the IRS should not be allowed to give subsidies for health plans through its faulty decision-making that violates separation of powers. Similarly, the libertarian Cato Institute and constitutional law professor Josh Blackman pushed back against Obama for what they view as circumventing Congress’ power to make law. “In what has become a troubling pattern of abuse, the executive branch has modified, delayed, and suspended these three pillars of the ACA,” the writers said of the individual and employer mandates and the insurance subsidies. “None of these provisions have gone into effect as Congress designed because they conflicted with the president’s policy preferences. Through a series of memoranda, regulations, and even blog posts, executive officials have disregarded statutory text, ignored legislative history, and remade the law on their own terms.” “Executive lawmaking—which has alas become commonplace—poses a severe threat to the separation-of-powers principles that undergird the Constitution and ultimately the rule of law itself. Accordingly, this Court should vacate the IRS rule that provides subsidies in states that did not establish exchanges. This rule violates Congress’s limitation of such subsidies to insurance bought through exchanges ‘established by the State,’” the Cato brief says. Another brief filed on behalf of Oklahoma, Alabama, Georgia, Nebraska, South Carolina and West Virginia said that 6 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 a move by Congress to make the availability of tax credits conditional is consistent with its longstanding practice of conditioning federal funds on state implementation of federal programs. “The bottom line is that there is no merit to the argument that the IRS Rule must be upheld in order to prevent unfair surprise to the States. States are constantly aware of their options under federal programs and how participation, or non-participation, in federal programs will affect their residents.” — Rachel S. Karas HHS Asked To Include Exchange Costs, Oversight Details In Fiscal 2016 Request When President Obama’s fiscal 2016 budget request debuts on Monday (Feb. 2), congressional appropriators hope to see an update on how CMS works to prevent improper payments and correctly pay claims the first time, according to language in last year’s Labor/HHS spending bill. The request was one of many listed in a 2015 appropriations agreement that heavily focused on oversight and responsible spending by HHS. CMS was told to list all insurance marketplace-related cost data for each fiscal year since the Affordable Care Act was enacted in 2010, as well as estimate those costs for fiscal 2016. That includes federal payroll and other administrative costs; marketplace-related information technology and non-IT program costs like health plan benefit and rate review, marketplace oversight, payment and financial management, and eligibility and enrollment data; and costs of consumer information and outreach costs including the call centers, navigator grants and consumer education and outreach; exchange quality review, the Small Business Health Options Program and employer activities; and other exchange activities. When the appropriations bill passed last year, the agreement modified the provision related to ACA exchange funding transparency and added new bill language to prevent CMS from supporting risk corridor payments through its Program Management appropriations account. Congress agreed to support health reform oversight and told the HHS Inspector General’s Office to provide lawmakers a plan of how it would run those activities no more than 60 days after enactment. The HHS inspector general was also told to consult with his counterpart at Treasury and report on IRS procedures to reconcile advance premium tax credits that low-income Americans received to help cover the cost of their health care plans in the federal and state-run health insurance exchanges. HHS should also detail how it uses IRS information to curb fraud and overpayments, lawmakers said. CMS did not update congressional committees on key topics like ACA innovation grants and exchange enrollment numbers, appropriators wrote. “These notifications often are provided to organizations and the media prior to notification to the House and Senate Committees on Appropriations, and in some cases without any notification,” the act said. CMS was told to notify the appropriations committees “not less than one full business day” before HHS releases ACA-related data and grant opportunities. The act also called for new methods of tracking and reporting fraud, waste and abuse: Congress asked CMS to propose prevention measures that would replace its usual “pay and chase” process. CMS was then directed to collaborate more with the HHS OIG on overseeing ACA-related contracts, making sure all contractors meet performance benchmarks and are held accountable for any actions that violate the contract. That report was due no later than 90 days after the appropriations act was approved, the act said. It was expected to detail current oversight measures for CMS contracts and how the agency can penalize a contractor if they do not follow through on their obligations. Congress also told HHS in its fiscal 2014 omnibus to correct a frequently asked questions page from 2013 on the provider nondiscrimination section of the ACA, which states that a “group health plan and a health insurance issuer offering group or individual health insurance coverage shall not discriminate with respect to participation under the plan or coverage against any health care provider who is acting within the scope of that provider’s license or certification under applicable state law.” Lawmakers want the department to change the FAQ to “reflect the law and Congressional intent,” but said CMS has not complied. “CMS is directed to provide a corrected FAQ by March 3, 2016 or an explanation for ignoring congressional intent.” The agreement later gave $71 million to the HHS OIG and told it to improve its annual budget request to include more details and performance measures of discretionary oversight. Congress expects the OIG to ensure that full oversight of ACA activities were added to its fiscal 2015 work plan and told the office to be substantially active in tracking all HHS operations. The fiscal 2016 request should also include an explanation of how the policy driving physicians to hold faceto-face certifications for home health care has prevented fraud, grown health care access and affected Medicare and Medicaid costs, the 2015 appropriations agreement said. CMS needs to specify how to simplify provider documentation for in-person work in this request, after an analysis of rebasing Medicare home health agencies was due within 90 days of enactment. CMS was told to describe its fiscal management processes in its fiscal 2016 budget request, including detailed plans Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 7 for mandatory and discretionary resources and tables of requested and actual funding for the previous and current years. The agreement asked for another update in the fiscal 2016 request on how CMS is making users aware of IT solution test space, as well as one on demonstrations of Medicare Parts C and D. That description should list pros and cons of plan service areas that could impact senior housing options in a particular geographic area, lawmakers said. Congress also expects CMS to update lawmakers on progress in changing the Medicare star quality rating system methodology as part of the new budget request. Finally, CMS was told to include a timeline, milestones and measurable goals to address their concerns about recovery audit contractor efficiency to reduce the backlog of Medicare claim appeals. The fiscal 2016 request should actuarially estimate the amount of improper payments, actual and estimated recoveries by year, and the percentage of recovered payments compared to the total. President Obama is expected to unveil a budget request on Monday that would reverse automatic across-the-board cuts of sequestration and add about $74 billion in “discretionary investments” above sequestration caps next year. HHS Secretary Sylvia Burwell will present the department’s fiscal 2016 budget on Monday. — Rachel S. Karas HHS Wants $30M To Examine Benefits . . . begins on page one HHS Secretary Sylvia Burwell said at a press briefing Monday (Feb. 2) that when this budget request is combined with proposed legislation, the United States would save a net estimate of $250 billion in the next decade, slow Medicare spending growth, and generate $223 billion in net savings through building a better health delivery system. Ellen Murray, HHS assistant secretary for financial resources, said that as in most years, the CMS Program Management account would be used to fund the exchanges. HHS expects to bring in more income from user fees in 2016 than in 2015, and other funding options include secretary transfer and the non-recurring expense fund. As time goes on, the exchanges will be almost exclusively funded by the fees, Murray said. The user fee is currently 3.5 percent of premiums for issuers selling products through the federal exchange. CMS Acting Administrator Andy Slavitt said the agency’s requests for major expense items like information technology are lower than in past years and should continue to drop. He reiterated that user fees will create a sustainable path for exchange funding going forward. The HHS appropriations agreement last year included bill language “to prevent the CMS Program Management appropriation account from being used to support risk corridors payments,” yet risk corridor funding was still listed under that account in the fiscal 2016 request. The Program Management account also lists $340 million for non-marketplace information technology systems and other support to allow CMS staff and stakeholders to access secure data through the IT shared services initiative. This year’s request cuts $1.76 billion in insurance exchange grants from $2.1 billion to $380 million, after the final round of grants to plan and establish their own marketplaces ended in December. HHS has provided $5.5 billion to states to build and establish exchanges since 2011, the budget says. The administration further says that states can use establishment grants to fund start-up costs of state-based or partnership marketplaces, or to support the Federally Facilitated Marketplace. Daily operations, however, are funded through local user fees or other revenue sources, the budget says. The budget request also expects to bring in nearly $4 billion less in transitional reinsurance program receipts than it did in fiscal 2015 at around $6 billion in 2016. The budget proposal lists a nearly $2 billion increase in risk adjustment receipts, up to $5.6 billion in fiscal 2016, and $940 million more through the risk corridor program for a total of nearly $6.4 billion. The administration also proposes spending $30 million on a new project that would examine how changes to health insurance benefit packages would affect health care use, costs and outcomes. Its findings would shape the creation of health care models that better serve families and providers. The project would use the “gold standard” randomized controlled trial study design along with the Health Insurance Experiment that began in the 1970s, the HHS budget-in-brief said. “A new effort is needed to rigorously examine how modern health insurance plans can be redesigned to maximize health status and quality, and minimize unnecessary costs,” the brief said. “The requested funds will enable HHS to plan and initiate the study using state-of-the-art evaluation methods to answer critical research questions that cannot be directly addressed through other means.” The Obama administration estimates that it will find $38.4 billion in savings to insurance marketplace subsidies in the next 10 years, budget documents said. In total, the fiscal 2016 budget proposal asks for $83.8 billion in discretionary budget authority for HHS, $4.8 billion more than the agency received last fiscal year. — Rachel S. Karas 8 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 News in Brief Medicaid, CHIP Enrollment Now 10.1M Above Baseline Senators Push Bill Stripping Employer Mandate, House To Vote On Full ACA Repeal Nearly 69 million Americans were enrolled in Medicaid or CHIP in November 2014 — a 17.5 percent increase, or about 10.1 million people, over the July-September 2013 baseline, CMS announced Monday (Feb. 2). The data also show a 25.5 percent increase in enrollment in states that expanded Medicaid and a 7 percent increase in those that did not, CMS acting Medicaid and CHIP director Vikki Wachino wrote in a blog post. Wachino also touted the recent news that Indiana will be expand access to Medicaid, becoming the 28th state — plus the District of Columbia — to do so. “We are encouraged by interest from governors from all across the country who understand both the economic benefits of Medicaid expansion and the health and financial security it brings to many individuals. We remain committed in working together toward the larger goals of high quality, affordable health coverage for all Americans,” Wachino said. Under the ACA, the federal government pays 10 percent of the costs for states to expand Medicaid to all people earning up to 138 percent of the federal poverty level through 2016, after which federal funding dips to 90 percent. HHS recently released data showing that 3.2 million adults had enrolled in Medicaid by March 2014, the first quarter following the expansion. — Amy Lotven Senate Finance Chair Orrin Hatch (R-UT) and health committee Chair Lamar Alexander (R-TN) introduced legislation Thursday (Jan. 29) that would fully repeal the health law’s employer mandate, which requires firms with 50 or more full-time employees to provide minimum coverage or pay a fine. Meanwhile, Rep. Bradley Byrne (R-AL) announced that the House will vote next week on his bill to fully repeal the law and require the committees of jurisdiction to come up with “an alternative, patient-centered solution.” “This vote is notable because it will be the first time since Republicans have taken control of the Senate that the House will act on a bill to repeal ObamaCare. “Senator Harry Reid can no longer stand in the way of allowing a vote on repealing this law once and for all,” Byrne said in a press release. While the GOP holds the Senate, Republicans do not have the votes to override a presidential veto, and so senators have been focusing on piecemeal change, many of which will also face a veto. “Until we have a Republican president and can repeal Obamacare, the responsible thing to do is repeal the employer mandate—one of several steps we can take to repair the damage Obamacare has done,” Alexander said upon introducing the American Jobs Protection Act. The bill has 26 original co-sponsors. Last week, Hatch and Alexander introduced a bill (S. 203) that would repeal the individual mandate. — Amy Lotven Oversight Republicans Seek ACA Implementation, King Contingency Details From IRS A trio of House oversight Republicans on Thursday (Jan. 29) asked the IRS to provide details on ACA implementation and its expected impact on taxpayers, and also inquired how the agency intends to respond should the Supreme Court rule that credits cannot flow through the federally facilitated exchanges in the highly watched King. v. Burwell case. The Republican members say they are concerned IRS has not informed taxpayers of possible consequences of the case. “The IRS could prevent confusion and uncertainty by preparing revisions to the Healthcare Premium Tax rule, providing taxpayer guidance on the implications of a ruling adverse to the IRS, and informing Congress of possible contingency plans,” wrote committee chair Jason Chaffetz (R-UT) along with Reps. Mark Meadows (R-NC) and Jim Jordan (R-OH). The lawmakers say in their Jan. 29 letter that many Americans will be facing additional paperwork during this year’s tax filing season, and many are also expected to see lower tax refunds or will owe the IRS following the premium tax credit reconciliation process. Additionally, they note, the administration has said up to 6 million people would be subject to fines for not having coverage. The House Republicans ask IRS to provide data on the number of people whose tax bills may increase or decrease due to the reconciliation process, and all documents and communications related to taxpayer messaging on responsibilities related to the ACA. They also request all documents and communications regarding any contingency planning on King v. Burwell. — Amy Lotven CA Renewals Show Consumers Mainly Sticking With Original Plan California health plans are touting a new report from Covered California that shows consumers are generally choosing to stick with exchange plans purchased during the first enrollment period, with the state’s issuers retaining about 90 percent of their consumers. “With 90 percent of enrollees sticking with their existing health plan, it is clear that there is stability in the market and people are pleased with their coverage,” Charles Bacchi, president and CEO of the California Association of Health Plans (CAHP), said of the news. California had about 1.1 million exchange enrollees eligible for renewal, according to the exchange. However, during the renewal process, the exchange found that about 85,000 of those were eligible for Medi-Cal. The exchange forwarded the names of the 944,000 of the remaining consumers to their chosen health plans, and is still working to renew another 80,000 enrollees who were unable to be auto-enrolled or did not select another plan. More than 60 percent of the 944,000 — about 576,000 individuals — took no action and were therefore automatically renewed into their existing plan. Another 368,000 explored other options and of those about 54,000 opted to switch plans. The exchange also released a table breaking down each issuer’s enrollment gains and losses and rates of retention. While every plan retained at least 90 percent of its consumers, one plan — Kaiser Permanente — had a 99 percent retention rate. Of the other large California exchange carriers, Anthem Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 9 had a 93.6 percent rate while Blue Shield held onto 94.7 percent of its consumers. — Amy Lotven Senators Introduce Companion Bill Recognizing Pharmacists As Providers A bipartisan group of senators introduced a bill to recognize pharmacists in medically underserved areas as Medicare providers under Part B who can be reimbursed for certain services a day after House lawmakers introduced companion legislation. Pharmacists are pleased both houses have introduced such a bill. Sens. Chuck Grassley (R-IA), Sherrod Brown (D-OH), Mark Kirk (R-IL) and Bob Casey (D-PA) introduced the bill Thursday (Jan. 29) to the delight of pharmacists. “Through the introduction of this legislation, Senators Grassley, Brown, Kirk and Casey have demonstrated tremendous commitment to improved healthcare access and outcomes for underserved Medicare patients,” National Association of Chain Drug Stores President and CEO Steven Anderson says in a statement. — Michelle M. Stein HHS: Nearly 7.3M Enrollees In FFM Through Jan. 23 Almost 7.3 million people chose a health insurance plan or were automatically re-enrolled in their existing plan through Healthcare.gov from Nov. 15 through Jan. 23, HHS announced in its weekly snapshot Wednesday (Jan. 28). That number in- cludes enrollees in the federally facilitated marketplace, statefederal partnership marketplaces and supported state-based marketplaces. Week nine saw 137,298 plan selections, bringing the total to 7,293,989 since 2015 open enrollment began. That also marks a drop of nearly 300,000 sign-ups from the previous week, though officials expect to see a large uptick in enrollments as the period closes next month. More than 9.7 million applications were submitted as of Jan. 23, the report said. For the second week, HHS also released a breakdown of enrollment numbers by state: Alabama: 137,941; Alaska: 17,051; Arizona: 171,723; Arkansas: 55,853; Delaware: 20,776; Florida: 1,301,745; Georgia: 435,523; Illinois: 290,791; Indiana: 189,220; Iowa: 37,338; Kansas: 81,205; Louisiana: 142,192; Maine: 62,983; Michigan: 301,646; Mississippi: 84,101; Missouri: 213,514; Montana: 47,701; Nebraska: 62,458; Nevada: 54,101; New Hampshire: 47,042; New Jersey: 213,573; New Mexico: 43,651; North Carolina: 467,560; North Dakota: 15,756; Ohio: 198,608; Oklahoma: 103,001; Oregon: 92,059; Pennsylvania: 425,854; South Carolina: 166,159; South Dakota: 18,248; Tennessee: 188,276; Texas: 940,707; Utah: 118,064; Virginia: 321,982; West Virginia: 27,849; Wisconsin: 179,626; and Wyoming: 18,112. Numbers included in the snapshot do not reflect effectuated enrollments, or those for which the first month’s premium has been paid. Open enrollment closes Feb. 15, by which many believe the administration will hit its target of 9.1 million FFM enrollees. — Rachel S. Karas Exchange Round-Up . . . begins on page one fund CMS activities and administrative expenses toward the exchanges as well as cover $544 million to support the growth and operations of exchange activities like eligibility, plan management and quality improvement. CMS says that the exchange establishment funding line is to support extensions of previously allocated funding for start up and other exchange costs. Under the ACA, exchanges are supposed to be fully self-sustaining as of Jan. 1, 2015, but CMS did say that states could use the money for certain functions not related to operations through 2016. CMS announced the final grants in December. The HHS Office of Inspector General requested $417 million for fiscal 2016, including an $83 million increase and 38 additional full-time employees for oversight and investigations related to the health insurance marketplaces. OIG also seeks an increase of $70 million and 192 employees for Medicaid and Medicare oversight. Three Republicans joined Democrats in opposing the repeal bill, which for the first time may see a vote in the Senate, yet will face a certain veto. Republicans meanwhile are working to develop ACA replacement legislation. House Majority Leader Kevin McCarthy (R-CA) announced that the chairs of the House committees of jurisdiction — Ways and Means Chair Paul Ryan (R-IS), Energy and Commerce Chair Fred Upton (R-MI) and Education and the Workforce Chair John Kline (R-MN) — would make up a task force that will focus on replacing the ACA and potentially a task force to develop legislation to replace the ACA as a contingency plan should the high court side with the plaintiffs in King v. Burwell and invalidate the federal exchange subsidies. In other King v. Burwell news, the Center for American Progress (CAP) on Thursday (Jan. 29) threw cold water on the idea that Congress would take quick legislative action if the Supreme Court rules against the administration, noting that the Congressional Budget Office would have to score the impact of a decision invalidating federal subsides accessed through Healthcare.gov. The Urban Institute has already run an estimate and found that it would cost $340 billion over 10 years, which CAP views as an insurmountable cost in this economic and political environment, to reinstate the subsidies to the federally facilitated states. Also last week, dozens of ACA supporters submitted their “friend of the court” briefs to the Supreme Court backing up the administration’s stance in the King v. Burwell case. “We will not mince words: Petitioners’ position, if accepted, would be a disaster for millions of lower and middle-income Americans,” the American Hospital Association, Federation of American Hospitals, Association of American Medical Colleges and America’s Essential Hospitals wrote in their brief 10 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 filed Wednesday. An ACA without subsidies would leave hospitals unable to make up funds that were cut when the law was passed — with the expectation that new patients using their new tax credits would replenish the deficit, the hospitals wrote. “That could imperil some hospitals, and will make it more difficult for others to carry out their missions, including effectively serving their communities.” America’s Health Insurance Plans (AHIP) said in its own brief filed this week that pulling subsidies would create substantially dysfunctional insurance markets and far higher costs than if the ACA had not been enacted. Premium tax credits and shared responsibility payments are essential to an actuarially viable marketplace because they are key to ACA market reforms, the insurers said. Many insurers released their earnings reports over the past few weeks and also discussed progress with the exchange enrollment and related policies. On Tuesday (Feb. 4) Aetna said that it was pleased with the first year of the exchange, particularly in light of the initial problems with the exchanges, and ended 2014 with about 560,000 enrollees. Aetna says it is on track to exceed projections for the current enrollment period, and also says it has successfully transitioned the vast majority of its “offexchange” membership to ACA compliant plans. “As we look at our total individual business, we now project that we will end the first quarter with approximately 1.1 million members, including up to 800,000 on exchange members. As we enter the second year of this emerging marketplace, we are cautiously optimistic on the potential for public exchanges to develop into an attractive growth opportunity, where we continue to offer value to our customers and generate a reasonable return for our shareholders,” Aetna Chairman and CEO Mark Bertolini said in prepared remarks. Also on Tuesday, Centene reported that it had 75,000 exchange lives as of Dec. 31. The demographics remain in line with pricing, and the financial performance of exchange business was slightly ahead of projections for 2014, Centene officials said. Early enrollment indicates we were tracking to meet our 2015 membership projection across our original nine states and two new states — Illinois and Wisconsin — the company entered for 2014. Anthem President and CEO Joe Swedish reported last week that the company had ended last year with 707,00 exchange enrollees in its 14 states. Anthem officials noted that the Blue Cross Blue Shield brand was an asset to the company, because along with pricing and network configuration, it is a core factor in consumer decision-making, he said, according to a Seeking Alpha transcript. And finally, tax season has officially kicked in and the majority of exchange enrollees should have access to their 1095-A forms that HHS said were to arrive by Feb. 2. Administration officials last week announced a partnership with several companies to help people navigate the new rules. Administration officials Wednesday (Jan. 28) stopped short of saying they would be willing to create a special enrollment period (SEP) for those who find out too late that they may be on the hook for penalties next year, instead saying that staff is completely focused on the Feb. 15 deadline for open enrollment. Officials did say, however, that they believe about 2 to 4 percent of the 150 million taxpayers, or up to 6 million people, could owe fines for failing to purchase coverage, and another 10 to 20 percent will claim a hardship exemption. In the states: Hawaii state auditors found that “improper planning and procurement procedures” created an unsustainable health insurance exchange, Pacific Business News reported Jan. 29. They also said that the Hawaii Health Connector board of directors could not agree on a strategic plan but nonetheless continued to do business, and possibly jeopardized $204.4 million in federal grant money by not following procurement policies and procedures when hiring consultants. The Connector’s market was limited because only about 8 percent of state residents are uninsured, thanks to a previous state health care act, and the Connector’s IT development faltered because of little communication between former exchange director Coral Andrews, the staff and board of directors. It sometimes took up to four months for the board to get a response to their questions, Pacific Business News reported. “‘The board’s ability to monitor its massive IT system’s development progress was impaired by an uncooperative executive director who withheld information,’” PBN said the auditor wrote. “‘Throughout the website development process, the board was largely unaware of the Connector’s myriad problems.’” Jeff Kissel, the Connector’s director since October, said many changes have been made in response to the audit completed last year. The exchange aims to become self-sustaining by 2022, seven years later than the federal goal for state marketplaces. A state bill under consideration would revise that requirement to 2023. As part of that bill, Hawaii’s state legislature is debating whether to let the Connector use state bonds to borrow up to $28 million over the next 10 years until it can support itself. In Nevada, Shawna DeRousse, chief operating officer of the Silver State Health Insurance Exchange, is leaving this month — making her the third top official to depart in the past year. She said she looks to start a career in the private sector. Nevada’s health exchange was riddled with glitches as a state-run marketplace in the first year of open enrollment before joining Healthcare.gov and improving in its second year. Washington Health Benefits Exchange staff told the state marketplace’s board that Wahealthplanfinder had “significantly improved” its account invoice processing and insurance carrier payments, the Seattle Times reported Jan. Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 11 22. Exchange CEO Richard Onizuka said that of the accounts processed in December, 1.7 percent had carrier payment problems and 1.5 percent had invoice problems. He added that too many people are still being affected, while board members noted that actual error rates are higher when including problems that have not yet been caught. Staff then said re-enrollment numbers were not meeting expectations. As of Dec. 31, 79,000 of around 130,000 customers had reenrolled for 2015, chief of staff Pam MacEwan said. “Exchange staff also said that some consumers may have been confused by messages that went out from carriers mistakenly indicating that if consumers wanted to keep their current account they didn’t need to take any action,” the Seattle Times wrote. Florida’s Republican House speaker Steve Crisafulli said last week that “we’re not going to be doing anything on the issue,” when talking to reporters about Medicaid expansion prospects in the state. Meanwhile, the Senate has offered several plans to expand health care to around 1 million low-income residents in the past few years, giving supporters hope that Florida will follow in Indiana’s footsteps of expansion after long opposition. Florida currently leads the nation in enrollment at 1.27 million residents, partially because those people who would otherwise qualify for the Medicaid expansion are forced into buying a private plan on the exchange. New York Democratic Gov. Andrew Cuomo’s new budget includes a nearly $69 million tax on health insurance policies to pay for administrative costs of the state’s New York State of Health insurance exchange after federal grant funds dry up, the New York Post reported Monday (Feb. 2). Upset Republicans say that had Cuomo not started a state-run exchange through executive order, there would be no need for new taxes to support it now. Cuomo’s administration called it a “modest” tax, while state insurance plan officials believe it will make health coverage less affordable for residents. Polls in Kentucky and Iowa that took the pulse of voters’ thoughts on Obamacare found that 41 percent of Kentuckians had an unfavorable view of the law, while 39 percent had a favorable opinion. Twenty percent said they don’t know. And though 60 percent said the law hasn’t affected their families, more than half said they didn’t have enough information about it, at 51 percent, The Courier-Journal reported Sunday (Feb. 1). Iowans were much more emphatic: more than 80 percent were in favor of repealing the Affordable Care Act, and 45 percent said getting rid of the law was in their top two issues — compared to 43 percent who wanted more aggressive pursuit of terrorists, Bloomberg News wrote Monday (Feb. 2). The latest enrollment figures: • Oregon: 85,912 on-exchange; 92,872 off-exchange; 178,784 total as of Jan. 25 • Colorado: 125,378 QHPs; 58,235 Medicaid; 2,884 CHIP; 186,497 total as of Jan. 31 • Massachusetts: 70,490 eligible for unsubsidized QHPs; 21,334 eligible for subsidized QHPs; 118,834 eligible for ConnectorCare (second lowest-cost); 220,998 eligible for MassHealth (Medicaid and CHIP); 431,656 total as of Monday (Feb. 2). • Vermont: 21,407 in effectuated QHPs; 9,101 in effectuated Medicaid or Dr. Dynasaur plan; 30,508 total effectuated plans as of Jan. 26. • Washington: more than 127,000 in QHPs as of Jan. 25 • Rhode Island: 19,189 paid QHP renewals; 6,539 new paid QHPs; 25,728 total paid QHPs as of Jan. 24. Rhode Island’s numbers now reflect those individuals whose insurance was canceled because they chose a plan but did not pay by their coverage effective date. • Michigan: 533,110 in Medicaid as of Jan. 26. — Amy Lotven SUBSCRIPTION ORDER FORM Sign me up to receive Health Exchange Alert at $705 per year in the U.S. and Canada; $755 per year elsewhere (air mail). Name __________________________________________________ Affiliation _______________________________________________ Address _________________________________________________ City/State/Zip ____________________________________________ Phone __________________________________________________ E-mail __________________________________________________ To order by mail: Send this coupon to Health Exchange Alert, P.O. Box 7167, Ben Franklin Station, Washington, DC 20044. To order by phone, fax or e-mail: Call 800-424-9068 (in the Washington, DC area, 703-416-8500). Fax to 703-416-8543. E-mail at [email protected] Please check one: Visa MasterCard Bill me Check enclosed (DC subscribers add 6% sales tax) Card number _________________________________________ Name on the card _____________________________________ Signature _______________________________________________ 12 Exp. date ____________________________________________ Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 CAP: $340 Billion Cost Would Limit Congressional Response To King The Center for American Progress (CAP) on Thursday (Jan. 29) threw cold water on the idea that Congress would take legislative action if the Supreme Court rules against the administration in King v. Burwell, noting that the Congressional Budget Office would have to score the impact of a decision invalidating federal subsides accessed through Healthcare.gov. The Urban Institute has already run an estimate and found that it would cost $340 billion over 10 years, which CAP views as an insurmountable cost in this economic and political environment, to reinstate the subsidies to the federally facilitated states, CAP’s Topher Spiro writes in the brief. Therefore, the report concludes, “the Supreme Court cannot rely on congressional Republicans who have voted many times to repeal the Affordable Care Act’s coverage to save it from the consequences of a ruling that would unravel that expansion.” The brief illustrates the difficulty Congress would face following a ruling for the plaintiffs, noting that Congress has long been unable to pay for a permanent reform of Medicare payments to physicians—which would cost $144 billion over 10 years—despite strong bipartisan support. “If Congress cannot come up with even that amount of money for a bipartisan reform, it would be a miracle for it to find more than two times that amount for a contentious reform,” Spiro writes. Since the Court decided to take up the case Nov. 7, health experts have debating how easily or difficult it would be for various contingencies. Initially many believed that states would be pressured to act or that the administration could make it easier for states to set up their own exchanges. However, since then, many experts have backtracked and acknowledged that various factors — including ideological opposition, prohibitive costs and timing — would likely make it difficult for most states to take action. The CAP brief notes that CBO would take all of those factors into account for its assumption. “Putting together all of these legal, practical, and political constraints, CBO would likely assume that not many—if any—additional states would set up their own marketplace to qualify for tax credits or otherwise be able to access equivalent funding. As a result, the Urban Institute’s estimate of a $340 billion reduction in federal spending is a reasonable approximation of how CBO would update its baseline,” Spiro says. CAP also argues that the state innovation waivers, which allow states to get exemptions from certain ACA policies in order to examine alternative reforms, are not a feasible solution to a ruling in favor of King. “The Affordable Care Act does not authorize state innovation waivers until 2017,” the brief argues. “More importantly, state innovation waivers only provide states with federal funding equal to the amount of tax credits that they would otherwise receive.” “Because a Supreme Court decision against the Affordable Care Act would eliminate tax credits in states that do not run their own marketplace, such states would not be entitled to any federal funding under a state innovation waiver,” Spiro says. — Amy Lotven Administration Holds Off On SEP, Says 6M Could Save Penalties Administration officials Wednesday (Jan. 28) stopped short of saying they would be willing to create a special enrollment period (SEP) for those who find out too late that they may be on the hook for penalties next year, instead saying that staff is completely focused on the Feb. 15 deadline for open enrollment. Officials did say, however, that they believe about 2 to 4 percent of the 150 million taxpayers, or up to 6 million people, could owe fines for failing to purchase coverage, and another 10 to 20 percent will claim a hardship exemption. HHS official also said that the department is in the process of sending out out 4 million 1095-A forms to consumers who received coverage through the exchange. Those forms will be used by consumers to report information on the amount of tax credits received. At filing time, the income a consumer initially estimated on his or her application will be reconciled with actual income, and those who received more credits than they were eligible for for must re-pay the government. However, officials say that most consumers’ repayments will not exceed any tax refund that they would have been eligible for, so few people will have to pay out. Instead, their refund would be reduced. The vast majority of Healthcare.gov consumers will have their forms by Feb. 2, and the forms are also available through their website accounts, officials said. State-based exchanges are also in the process of sending out the forms. The administration officials were speaking on a conference call with reporters that also highlighted HHS’ partnership with wide-ranging non-profits and other groups to help consumers understand the new tax process. “Every year, non-profit organizations and tax preparers provide millions of Americans the assistance they need to file their returns and we are pleased to collaborate with them,” said HHS Secretary Sylvia Burwell. “When it comes to health care and taxes, the only change the vast majority of people will notice is the requirement to check a box to indicate that they had health insurance all year through their job, Medicare, Medicaid, Tricare or the Veterans Affairs. A smaller number of people, including those who purchased coverage through the Health Insurance Marketplaces or those who Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 13 were uninsured for some or all of the year, will need to take additional steps when filing their taxes. We are working to provide taxpayers with the tools and information they need to file their returns and answer their questions,” she said. Partners include: AARP Foundation Tax Aide, Center for Budget Policy and Priorities, H &R Block, Jackson Hewitt, TaxACT, National Women’s Law Center, Community Action Partnership, Corporation for Enterprise Development, and TurboTax Advocates and other stakeholders have been pushing HHS to created the special enrollment period for people who file taxes after Feb. 15 and find out that they will owe the government next year because they did not purchase coverage. Healthcare.gov CEO Kevin Counihan said last week that HHS is aware of the issue. On Wednesday’s call, an official said that HHS was more focused on encouraging people to enroll by the deadline and added, “We will deal with special considerations after Feb. 15.” Officials also said that IRS had decided to waive penalties for those failing to fully re-pay excess credits by the April 15 deadline because it is the first year of the new filing rules. In order to be eligible for the waiver a person must be up to date in tax payments, owe the IRS due to the tax credits and have reported the payments in a timely fashion, the agency said in a notice issued this week. Rachel Klein of Families USA says that the group appreciates the IRS’ move and believes it makes sense for the IRS to do whatever possible to help out consumers. Klein adds that while advocates would hope that the IRS would treat all taxpayers equitably — as opposed to narrowing the eligibility for the waiver — in generally she is very pleased. Klein says she hopes the IRS will continue to take action to make things as easier for consumers. Sen. Orrin Hatch (R-UT), however, is questioning the decision. In a letter sent Wednesday, he asks the IRS to explain what led to the decision to offer a waiver, how many taxpayers are expected to owe tax debt based on excess insurance subsidies, if the Internal Revenue Service communicated with other agencies in creating the waiver program, and if there are plans for future waiver programs. — Amy Lotven Finance Dems, GOP Propose ACA Fixes In ‘Heroes’ Markup Senators on both sides of the aisle discussed amendments that would modify provisions of the Affordable Care Act during a Finance Committee markup of the Hire More Heroes Act on Wednesday (Jan. 28), though none were formally added. While some were filed, others were not relevant to the markup and others were never offered by the sponsoring member. The bill was reported non-amended out-of-committee by a roll call vote of 26 to 0. The “Hire More Heroes Act” aims to provide incentives for companies to hire more veterans by exempting them from the ACA’s 50-employee threshold, which requires an employer offer job-based health insurance, if the veteran already has medical coverage through the TRICARE program or the VA. Suggested amendments to the bill — many of which seek to change parts of the employer mandate — included: • Chuck Grassley (R-IA): Grassley’s amendment would allow small employers to continue to financially help their employees buy health insurance on the individual market on a pre-tax basis. Standalone health reimbursement arrangements and employer payment plan arrangements would not be included as group health plans under the ACA and therefore not subject to the penalty for failing to meet certain group health plan requirements. The amendment would also clarify that employees who receive employer assistance are ineligible to receive premium tax credits or cost-sharing subsidies for on-exchange insurance. • John Thune (R-SD): The “Helping Individuals Regain Employment Act” would permanently exempt long-term unemployed individuals who are hired for work from the ACA’s full-time employee count for as long as they are working for that same employer. A similar Thune amendment would extend that exemption to long-term unemployed veterans, including reservists, who are currently seeking employment. The U.S. Labor and Treasury Departments would be asked to study how the ACA impacts job opportunities available to those veterans. To offset the amendment, HHS would withhold payments “to any Medicaid provider or supplier under a State plan under title XIX of the Social Security Act to individuals with a tax lien.” Thune also seeks to amend the ACA to exempt public schools, universities and colleges from the employer mandate. The U.S. Department of Education would be required to submit a study to Congress on the mandate’s effects on a school’s ability to fulfill its mission and maintain academic programs, before and after repeal. • Pat Toomey (R-PA) and Mark Warner (D-VA): The senators look to exempt volunteers who work with emergency services, government and tax-exempt organizations from counting as employees under the ACA’s shared responsibility requirements. “Bona fide volunteer” services are those for which people are repaid or given reasonable benefits and nominal fees for reasonable expenses incurred while volunteering. • Dan Coats (R-IN): The amendment would exempt certain categories of people with disabilities from counting toward the limit of full-time employees that determines if an employer is large enough to be subject to the employer mandate. • Debbie Stabenow (D-MI): She would amend the bill so any full-time hourly worker who is a military veteran covered by TRICARE or the VHA health care program must be paid, at minimum, $10.10 per hour indexed for inflation, 14 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 for the employer to exclude the employee from their full-time worker count. • Bob Menendez (D-NJ): He furthered Thune’s suggestion by specifying that veterans with VA or TRICARE benefits would be exempt, and that the Labor Department and VA would have to create rules prohibiting employers from discriminating against veterans without those military benefits. Menendez also discussed an amendment stopping employers from using the veteran exemption to stop providing job-based health coverage unless at least 95 percent of their employees have access to or are enrolled in an alternative qualified health insurance plan. • Sherrod Brown (D-OH): One amendment would retroactively extend the health coverage tax credit, ended by the ACA in 2013, from Jan. 1, 2014 through Dec. 31, 2016. The tax credit was available to laid-off employees who receive trade adjustment assistance benefits, as well as retirees whose pension payments come through the Pension Benefit Guaranty Corporation. The HCTC helps displaced workers make health coverage more affordable and gives them time to move to other insurance plans, and “serves as a critical bridge to Medicare for retirees who have lost much of their pensions through no fault of their own,” a description of the amendment reads. Brown would also amend U.S. Code to extend children’s health coverage through age 26 for those under the VA’s Civilian Health and Medical Program, making it consistent with the ACA provision that covers children on their parents’ insurance through age 26. The bill would also ensure that eligibility would not be limited for those who were permanently incapable of supporting themselves before age 18. • Bob Casey (D-PA): Casey brought up an amendment that would change the way the Internal Revenue Service interprets part of the ACA, allowing an employee’s dependents to access premium tax credits if the cost of an employer’s family coverage is higher than 9.5 percent of household income. “In interpreting this part of the law, IRS defined ‘affordable’ based on the cost of insurance for the employee alone, without taking into account the added cost of insuring an entire family … (it) is a commonsense bill that would strengthen the ACA and help millions of Americans gain access to meaningful health insurance coverage.” Casey also aims to clarify Congress’ intent on states’ obligation to give Medicaid coverage to former foster children. He would change the law to ensure all former foster children who enrolled in Medicaid upon turning 18 can keep that coverage until age 26. Sen. Tom Carper (D-DE) discussed amendments to modify several areas of Medicaid and Medicare, and Brown listed a popular amendment that would extend the Children’s Health Insurance Program through 2019. — Rachel S. Karas Congressmen, Families USA Defend ACA Subsidies Amid New Amicus Briefs Two current and former congressmen said Wednesday (Jan. 28) that a U.S. Supreme Court ruling to make subsidies unavailable through the federal health insurance exchange in King v. Burwell would go against the way they wrote the law and their intent to provide health insurance to all Americans. The idea that congressmen who had spent their careers in public service campaigning for universal health care would then draft a law narrowing the pool based on where people live rather than their health status is a fallacy, former Rep. George Miller (D-CA), who retired last year, said. He added that no one thought the text of the law, which says subsidies are available in exchanges “established by the State,” was inconsistent with the idea of universally available tax credits. “It was never debated … that somehow this is the wrong thing to do,” Miller said at a Families USA press conference to debut consumer advocates’ amicus brief filed Wednesday in support of the administration. Rep. Sandy Levin (D-MI) called the plaintiff’s interpretation that subsidies can only be received by consumers whose states run their own exchanges, rather than using the Healthcare.gov platform, a figment of their imaginations. “We don’t think there’s anything to be fixed,” he said, adding that making premium tax credits unavailable to states on the federal exchange was never part of a discussion about differences between the two bills before passage. “There’s no problem,” he said. “They’re now dredging this up and the court should not be a party to dredging.” The law’s writers “didn’t have to be a legislative genius” to know many of the states would not create their own exchanges, Levin said. He added that there is “zero evidence” that subsidy conditionality was intended in the law’s drafting. “This is not a legitimate case,” Levin said. “The petitioners are out to destroy the ACA.” Families USA Executive Director Ron Pollack said advocates never thought King v. Burwell was a serious legal challenge. But because the court did not follow its traditional guidelines for choosing to hear a case, he said, they have to take it seriously. Pollack believes there is no constitutional issue at hand and no conflict between the circuit courts of appeals that have heard the case and similar lawsuits. Pollack and the congressmen agreed that there was no discussion at a state level to indicate that states saw any threat to the subsidies if they opted to join the federal exchange. Not a single governor understood that the law’s language had implications in terms of receiving subsidies, Pollack said. Families’ amicus brief contends that affordable health coverage was intended for legal residents in all states, regardless of whether that state runs its own marketplace or the federal government facilitates it for the state. The plaintiffs are Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015 15 quarantining six words from a subsection that deals with the formula for calculating subsidy amounts rather than eligibility for those tax credits, the brief said. “Petitioners now seek to interpret it to death,” Families wrote of the ACA. “In so doing, they proffer a reading of the law so artificial that no one mentioned it during debates on the bill, or in the political uproar following its passage, or even in the suit challenging its constitutionality.”— Rachel S. Karas House E&C Asks HHS For Details On Post-King Contingency Plans House Energy and Commerce Republicans on Wednesday (Jan. 28) asked HHS to hand over any communications and documents related to potential contingency plans should the Supreme Court rule against the administration in King v. Burwell, a decision that would eliminate subsidies for those who enrolled via Healthcare.gov. The letter comes the same day that those supporting the administration’s position must file their friend-of-court briefs with the high court. “While the Supreme Court has yet to rule, it is clear that the court’s decision could have a profound impact on the operation of the (Affordable Care Act), says the Jan. 28 letter. “Given HHS’ responsibilities, we believe it is prudent that the department plan for the full range of potential outcomes and consequences of the court’s decision,” adds the letter, which was signed by Energy and Commerce Chairman Fred Upton (R-MI), Vice Chairman Marsha Blackburn (R-TN), Chairman Emeritus Joe Barton (R-TX), Oversight and Investigations Subcommittee Chairman Tim Murphy (R-PA), and Health Subcommittee Chairman Joe Pitts (R-PA). The members ask HHS to describe all scenarios that have been considered and any options that have been rejected, approved or are under discussion, and to provide the federal authority related to those potential contingencies. HHS revealed Tuesday (Jan. 27) that 7.1 million out of the 9.5 million total people who have selected plans came in through the federally-facilitated insurance marketplace, and that 87 percent of those consumers were eligible for subsidies. The high court is slated to hear oral arguments in King on March 4, and a decision is expected in late June. The administration has consistently expressed confidence that the court will rule in its favor and that no contingencies are needed. Sources believe that the administration is eying plans but will not reveal them prior to the ruling. — Amy Lotven IRS Waives Penalties For Those Who Don’t Rectify Tax Credits by April 15 Individuals who were overpaid advanced payment tax credits (APTCs) to purchase exchange coverage will not receive additional penalties if they are unable to pay back in full by April 15 under a new waiver the IRS quietly announced Monday. Typically, individuals must pay in full by the due date or be subject to a penalty for failure to pay or underpaying. “This is the first year Americans will take some additional steps related to the Affordable Care Act when they file their taxes, and the Administration is committed to making the process as smooth as possible.,” says a Treasury spokesperson. “We are providing tools and information necessary for individuals to understand the new system. Starting this year, just like taxpayers reconcile their tax withholding with their actual tax liability and get refunds or make an additional payment accordingly, individuals benefiting from tax credits for Health Insurance Marketplace coverage will follow the same process,” the spokesperson adds. The staffer continues: “Normally, taxpayers may owe certain penalties for late payments or underpayment of estimated tax. However, to help smooth the process for the first year of the Affordable Care Act, the IRS will waive these penalties for eligible taxpayers if they resulted from repayment of excess advance payments of the premium tax credit for Marketplace coverage. Taxpayers who receive a waiver for this late payment penalty are still required to pay their full tax liability, including any interest. They will also have access to the available repayment options, such as a payment plan or an installment agreement,” the aide said. In order to receive the waiver, a taxpayer must be up to date on payments and must have reported the excess payments to the IRS in a timely fashion. The exchange provided tax credits based on estimated income which could differ from the actual income and create a discrepancy. This difference is reconciled via the IRS form. “The IRS has discretionary authority to grant relief from both of these penalties. It obviously decided to exercise this discretion with respect to premium tax credit overpayments for 2014 because the reconciliation process is new and individuals have no prior experience with it,” health expert Tim Jost wrote in a Health Affairs blog. “There are no assurances that the IRS will waive the penalties again for 2015, however. Enrollees receiving tax credits should be careful to ensure that their eligibility information is kept up to date with the marketplace to avoid an overpayment. Under the law, individuals who received excess payments must re-pay the federal government. Congress had originally limited the subsidy recapture amount to $400 per family, but later increased the cap to $2,500 per family as a way to offset the 2010 Medicare physician payment fix, and later to help cover the costs of repealing the ACA’s unpopular 1099 reporting provision. — Amy Lotven 16 Health Exchange Alert - www.InsideHealthPolicy.com - February 4, 2015
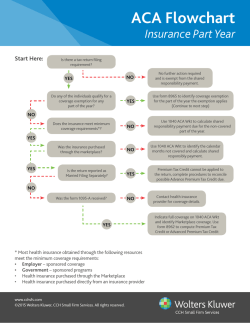



© Copyright 2026