
HIC refractaria
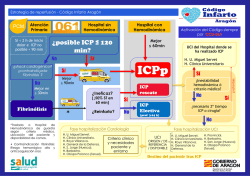
HIC Refractaria Posgrado de Medicina Intensiva Cátedra de Medicina Intensiva Semestre NeuroRReanimación Set 2016 Grupo de Neurointensivismo TRATAMIENTO DE LA HIC OBJETIVOS DE LA PRIMERA SEMANA HEMODINAMIA INTRACRANEANA • PIC < 20-25 mmHg (15) DESCOMPRESIVA LESIÓN TEMPORAL(única o bilateral) COMPRESIÓN CISTERNAS DE LA BASE DLM Rosner y col. (1996) Robertson y col.(1999) Steiner, Czosnyka y col. (2002) • PPC entre 50-70 mmHg (60-80) TRATAMIENTO DE LA HIC SIN DESCONOCER LA IMPORTANCIA DE LOS UMBRALES DE PIC PUEDE EXISTIR NEURODETERIORO AÚN CON VALORES SUBUMBRAL (Marshall y col, J Neurosurg 1983. Alteraciones pupilares) TOLERAR NIVELES SUPRAUMBRAL PUEDE SER ADECUADO EN PACIENTES CON BUENA EVOLUCIÓN CLÍNICA Y TOMOGRÁFICA (Chambers IR y col, J Neurosurg 2001) TRATAMIENTO DE LA HIC 1- MEDIDAS INESPECIFÍCAS • APLICABLES A TODOS • EFECTIVAS TRATAMIENTO DE LA HIC ESTRATEGIA PROGRESIVA • ESCALONADA: NIVELES TERAPÉUTICOS • BALANCE RIESGO / BENEFICIO (mayor complejidad e invasividad) • ADITIVA RETIRADA LENTA E INVERSA TRATAMIENTO DE LA HIC EBIC GUÍAS DEL SUR REVISIONES COCHRANE COINCIDENCIAS Y DISCREPANCIAS TRATAMIENTO DE LA HIC PRIMER NIVEL PRIMER NIVEL SEGUNDO NIVEL: BBT (Pentobarbital) SEGUNDO NIVEL (Intermedias) OPCIONES TERCER NIVEL TRATAMIENTO DE LA HIC GUÍAS DEL SUR • PRIMER NIVEL • SEGUNDO NIVEL • TERCER NIVEL •PASO 1 DRENAJE LCR •PASO 2 OSMOTERAPIA •PASO 3 HV MODERADA •PASO 4 BNM •INDOMETACINA •THAM •HV INTENSA •PPC TARGET •BBT •DESCOMPRESIVA •HIPOTERMIA MODERADA •DRENAJE LUMBAR HIC REFRACTARIA DEFINICIÓN • AUSENCIA DE RESPUESTA A MEDIDAS DE PRIMER NIVEL (A TOPE) • PIC PERSISTENTEMENTE >20-25mmHg HIC REFRACTARIA INCIDENCIA 15-30% HIC REFRACTARIA FISIOPATOLOGÍA • VASORREACTIVIDAD CEREBRAL • COMPLIANCE INTRACRANEANA HIC REFRACTARIA IMPACTO PRONÓSTICO MORTALIDAD 60-70% HIC REFRACTARIA HERALDOS 1. HIPOXIA - HIPOTENSIÓN 2. SINDROME HERNIARIO PREVIO 3. SWELLING INTRAOPERATORIO 4. “OPEN PRESSURE” > 18 mm Hg 5. TRASTORNO DE CRASIS 6. HIPERLEUCOCITOSIS MANTENIDA TRATAMIENTO DE LA HIC GUÍAS DEL SUR • PRIMER NIVEL •PASO 1 DRENAJE LCR •PASO 2 OSMOTERAPIA •PASO 3 HV MODERADA •PASO 4 BNM “ALTERNATIVAS TERAPEÚTICAS MÁS ALLÁ DE LAS GUÍAS” • SEGUNDO NIVEL •INDOMETACINA •THAM •(HV INTENSA) •PPC TARGET • TERCER NIVEL •BBT •DESCOMPRESIVA •HIPOTERMIA MODERADA •DRENAJE LUMBAR TRATAMIENTO DE LA HIC REFRACTARIA MEDIDAS DE SEGUNDO NIVEL O INTERMEDIAS • SENCILLAS DE IMPLEMENTAR (menos invasivas que TERCER NIVEL) • BAJO COSTO • ADECUADO BALANCE RIESGO/BENEFICIO TRATAMIENTO DE LA HIC REFRACTARIA INDOMETACINA • AINE (EICOSANOIDES) • ESPECIAL ACCIÓN CEREBRAL • VASOMODULADOR EFECTO DEL BOLO DE INDOMETACINA SOBRE PIC 47,5 n= 11 45 34,4 PIC 35 25 23,6 21,3 16,4 15 9,2 5 ANTES DESPUES t P = 0.0001 BIESTRO Y COL J NEUROSURG; 83:627-630, 199 INDOMETACINA FSC-CMRO2 35% SN 10% NS CYTOCHROME C OXIDASE AFFINITY ? INDOMETACINA AUTORREGULACIÓN CEREBRAL INDOMETACINA FUERTE DESCENSO DE LA PIC MANTENIMIENTO DE LA PPC REDUCCIÓN DEL FSC MANTENIENDO CMRO2 AFINIDAD CYTOCHROME C OXIDASE MEJORA ACOPLAMIENTO (DEMANDA/CONSUMO) MEJORÍA DE AUTORREGULACIÓN (Otras medidas resultan más efectivas) INDOMETACINA DOSIS • BOLO 50 mg 15-20 min • INFUSIÓN 30 mg/h CONTROL CON SJO2 ? JAMÁS SUSPENDER BRUSCAMENTE!! EFECTO REBOTE PUEDE SER GRAVE Indomethacin for control of ICP. Sader N1, Zeiler FA, Gillman LM, West M, Kazina CJ. Abstract Our goal was to perform a systematic review of the literature on the use of indomethacin and its effects on intracranial pressure (ICP) in patients with neurological illness. All articles from MEDLINE, BIOSIS, EMBASE, Global Health, Scopus, Cochrane Library, the International Clinical Trials Registry Platform (inception to July 2014), reference lists of relevant articles, and gray literature were searched. Two reviewers independently identified all manuscripts utilizing the following inclusion and exclusion criteria. INCLUSION CRITERIA: Humans, prospective studies (five or more patients), documented ICP response to indomethacin, and English. EXCLUSION CRITERIA: non-English, retrospective studies, no documentation of ICP response to indomethacin, and animal studies. A two-tier filter of references was conducted. First, we screened manuscripts by title and abstract. Second, those references passing the first filter were pulled, and the full manuscript was checked to see if it matched the criteria for inclusion. Two reviewers independently extracted data including population characteristics and treatment characteristics. The strength of evidence was adjudicated using both the Oxford and GRADE methodology. Our search strategy produced a total of 208 citations. Twelve original articles, 10 manuscripts, and 2 meeting proceeding, were considered for the review with all utilizing indomethacin, while documenting ICP in neurological patients. All studies were prospective. Across all studies, there were a total of 177 patients studied, with 152 receiving indomethacin and 25 serving as controls in a variety of heterogeneous studies. All but one study documented a decrease in ICP with indomethacin administration, with both bolus and continuous infusions. No significant complications were described. There currently exists Oxford level 2b, GRADE C evidence to support that indomethacin reduces ICP in the severe TBI population. Similar conclusions in other populations cannot be made at this time. Comments on its impact, on patient outcome, and side effects cannot be made given the available data. At this time, indomethacin for ICP control remains experimental and further prospective study is warranted. Neurocritical Care, Junio 2015 CSIC Grupos - INDOPET TRATAMIENTO DE LA HIC REFRACTARIA TROMETAMINA (THAM) 0,3 M ACETATO • pH 8,6 • pk 7,82 (Bic. Na pK 6,1) • 380 mOsmol/L THAM PROPIEDADES FARMACOLÓGICAS • BASE DÉBIL • CAPACIDAD AMORTIGUADORA THAM CAPACIDAD AMORTIGUADORA • R-NH2 + H+ + La- R-NH3+ + LaH2CO3 H+ + HCO3 - • R-NH2 + H2O + CO2 R-NH3+ +HCO3- THAM PROPIEDADES FARMACOLÓGICAS • PENETRACIÓN CELULAR • PASAJE A TRAVÉS DE LA BHE THAM PROPIEDADES FARMACOLÓGICAS • ELIMINACIÓN RENAL • CONTRAINDICADO EN LA I. RENAL THAM MECANISMO DE ACCIÓN • SE POSTULA: 1) REGULACIÓN DEL VSC 2) REGULACIÓN DEL EDEMA CELULAR-VOLUMEN CELULAR 3) AUTORREGULACION CEREBRAL? “BOMBA ASPIRADORA DE PROTONES” ACIDOSIS INTERSTICIAL Y CELULAR POST-INJURIA ACCIÓN A DISTANCIA THAM INDICACIONES NEUROINJURIA 1- PIC REFRACTARIA 2- CORRECCIÓN DE HV ACCIDENTAL 3- IPA/DISTRESS THAM y PIC Experiencia CTI-HC 45 40 40,6 n=7 35 30 25 31,7 22,8 20 18,4 15 12,1 10 5,8 5 0 p = 0.005 Dr. Codina Dr. A Biestro THAM INDICACIONES • MODO DE USO • DOSIS 1- PIC REFRACTARIA (SjO2) SINERGIA HIPERVENTILACIÓN HIPOTERMIA SSH? THAM INDICACIONES 2- CORRECCIÓN HV ACCIDENTAL 200-300 mL 3-6 hs (repetir) THAM INDICACIONES 3- IPA/DISTRES THAM for control of ICP Zeiler FA1, Teitelbaum J, Gillman LM, West M. Abstract Our goal was to perform a systematic review of the literature on the use of tromethamine (THAM) and its effects on intracranial pressure (ICP) in patients with neurological illness. All articles from MEDLINE, BIOSIS, EMBASE, Global Health, HealthStar, Scopus, Cochrane Library, the International Clinical Trials Registry Platform (inception to February 2014), reference lists of relevant articles, and gray literature were searched. Two reviewers independently identified all manuscripts pertaining to the administration of THAM in human patients that recorded effects on ICP. Secondary outcomes of effect on cerebral perfusion pressure, mean arterial pressure, patient outcome, and adverse effects were recorded. Two reviewers independently extracted data including population characteristics and treatment characteristics. The strength of evidence was adjudicated using both the Oxford and GRADE methodology. Our search strategy produced a total 2,268 citations. Twelve articles, 9 manuscripts, and 3 meeting proceedings were considered for the review with all utilizing THAM while documenting ICP in neurosurgical patients. All studies were prospective. Across all studies, there were a total of 488 patients studied, with 263 receiving THAM and 225 serving as controls in a variety of heterogeneous studies. All but one study documented a decrease in ICP with THAM administration, with both bolus and continuous infusions. One study documented a reduction in cerebral perfusion pressure. No significant renal dysfunction, hepatocellular injury, or hypoglycemia were reported. Three prospective randomized control trials displayed trends to improved outcome in severe traumatic brain injury (TBI) patients with THAM administration. There currently exists Oxford level 2b, GRADE B evidence to support that THAM reduces ICP in the TBI and malignant ischemic infarct population, with minimal side effects. The literature suggests THAM may be useful for ICP reduction in certain cases, though the safety of the compound in these circumstances is still unclear. Further prospective study is warranted. Neurocritical Care, Octubre 2014 TRATAMIENTO DE LA HIC ESTRATEGIA “TARGET” • “PPC ÓPTIMA” : MEJOR Mx o PRx PPC>60(70)mmHg ES SUFICIENTE? TRATAMIENTO DE LA HIC REFRACTARIA HV INTENSA 25-30 mmHg • POTENTE MEDIDA TRANSITORIA • OPTIMIZADA: SJO2 ≥ 50-55% • ASOCIAR THAM (TRABAJO de WOLF y col.) TRATAMIENTO DE LA HIC REFRACTARIA MEDIDAS DE TERCER NIVEL • LA CORRECTA SELECCIÓN DEL PACIENTE ES CRUCIAL • DESICIÓN DIFÍCIL (NQ) • FACTOR TIEMPO TRATAMIENTO DE LA HIC GUÍAS DEL SUR • PRIMER NIVEL •PASO 1 DRENAJE LCR •PASO 2 OSMOTERAPIA •PASO 3 HV MODERADA •PASO 4 BNM “ALTERNATIVAS TERAPEÚTICAS MÁS ALLÁ DE LAS GUÍAS” • SEGUNDO NIVEL • TERCER NIVEL •INDOMETACINA •THAM •(HV INTENSA) •PPC TARGET •BBT •DESCOMPRESIVA •HIPOTERMIA MODERADA •DRENAJE LUMBAR TRATAMIENTO DE LA HIC REFRACTARIA BARBITÚRICOS (BBT) BBT POTENCIALES EFECTOS BENEFICIOSOS • • METABOLISMO CEREBRAL (funcional) VSC EFECTO NEUROPROTECTOR POBRE, POR LO QUE NO ESTÁ INDICADO SU USO PROFILÁCTICO (Estudios Richmond y Toronto, 80s) TIOPENTAL (URU) • • • • ACCIÓN CORTA DEPRESOR MIOCÁRDICO DEPRESOR INMUNIDAD EFECTO DIRECTO VASOCONSTRICTOR • • CLÍNICA MUERTE ENCEFÁLICA VENTANA CLÍNICA BBT THE MYTHICAL EISENBERG´s STUDY BBT C 37 patients R F 32% 68% M 8% M 83% 36 patients R 17% F 83% Outcome at month: p<0.05 Eisenberg HM et al.:J Neurosurg. 1988 Jul;69(1):15-23 BBT EN LA PRÁCTICA: TEST DEL BOLO TIOPENTAL 5 a 10 mg/k en 15´ 1. EEG (salva supresión) COMPLETO < 20mmHg INFUSIÓN 2. MONITOREO HEMODINAMICO 1-6 mg /K / h RESPONDEDORES INVASIVO PIC INCOMPLETO > 20mmHg 3. HIDROCORTISONA APROX. 25% NO RESPONDEDORES PIC o INFUSIÓN (Juicio Clínico) xx INFUSIÓN BBT 62% 53% BBT BBT EFICACIA Thio Pento ICP CONTROL 36% 13% ICU MORTALITY 50% 0.16 ESTUDIOS EXPERIMENTALES SEÑALAN DIFERENCIAS Y MEJORES RESULTADOS CON PENTOBARBITAL (OXI) vs THIOPENTAL (THIO) 73% 0.19 ESTUDIOS CLÍNICOS NO LO CONFIRMAN Perez Barcena J et al: Neurocirugía2005, 16:5-13 Critical Care 2008, 12 (4):R112 BBT UNA ALTERNATIVA : PROPOFOL • EXCELENTE VENTANA CLÍNICA • REPERCUSIÓN HEMODINÁMICA • DOSIS <5 mg /K /h • 3 - 4DÍAS TRATAMIENTO DE LA HIC REFRACTARIA HIPOTERMIA MODERADA 32-34 TRATAMIENTO DE LA HIC REFRACTARIA HIPOTERMIA TERAPÉUTICA INTRAVASCULAR POTENCIALES EFECTOS BENEFICIOSOS • METABOLISMO CEREBRAL (BASAL) EDEMA CEREBRAL •REDUCCIÓN METABOLISMO GLUCOSA (ACOPLE FSC) • CASCADAS INFLAMATORIAS DESCENSO PIC • AA EXCITATORIOS • FLUJOS IÓNICOS TRANSMEMBRANA MUERTE CELULAR TRATAMIENTO DE LA HIC REFRACTARIA HIPOTERMIA TERAPÉUTICA INTRAVASCULAR • SOFTWARE INTELIGENTE (AJUSTES DÉCIMA GRADO) • CATETERES ENDOVASC. CON INTERCAMBIO TÉRMICO EN CIRCUITO CERRADO Consolas con software inteligente ENFRIAMIENTO INTRAVASULAR “CERRADO” TRATAMIENTO DE LA HIC REFRACTARIA HIPOTERMIA TERAPÉUTICA INTRAVASCULAR 4 FASES • PRE-ENFRIAMIENTO (B SF 30ml/K 4º 30’) • ENFRIAMIENTO Consolas (2-3hs) con software • MANTENIMIENTO (32-33ºC) • RECALENTAMIENTO (1º/día) inteligente TRATAMIENTO DE LA HIC REFRACTARIA POBLACIÓN BIEN SELECCIONADA EDAD < 45 AÑOS SIN COMPROMISO SISTÉMICO CORTA EVOLUCIÓN DE LA LESIÓN (4-5 DÍAS) Hypothermia for traumatic head injury. Sydenham E, Roberts I, Alderson P Cochrane Database Syst Rev. 2009;(1):CD001048. AUTHORS' CONCLUSIONS: • There is no evidence that hypothermia is beneficial in the treatment of head injury. • Hypothermia may be effective in reducing death and unfavourable outcomes, but significant benefit was only found in low quality trials (tendency to overestimate the treatment effect). • The high quality trials found no decrease in the likelihood of death with hypothermia, but this finding was not statistically significant and could be due to the play of chance. • Hypothermia should not be used except in the context of a high quality randomised controlled trial with good allocation concealment. Hypothermia treatment for traumatic brain injury: a systematic review and meta-analysis. Peterson K, Carson S, Carney N. J Neurotrauma. 2008 Jan;25(1):62-71. • Reductions in risk of mortality were greatest and favorable neurologic outcomes much more common when hypothermia was maintained for more than 48 h. • Potential benefits of hypothermia may likely be offset by a significant increase in risk of pneumonia. • In sum, the present study's updated meta-analysis supports previous findings that hypothermic therapy constitutes a beneficial treatment of TBI in specific circumstances. HIPOTERMIA TERAPÉUTICA ¨CLAVES PARA EL ÉXITO¨ 1.NIVEL o GRADO 2.DURACIÓN (48hs o PIC) 3.RECALIENTAMIENTO PASIVO 4.NO asociar BBT HIPOTERMIA TERAPÉUTICA PROBLEMAS ¨VITALES¨ 1.MANEJO MEDIO INTERNO y Eq. A-B 2.MANEJO HEMODINAMIA / VOLEMIA 3.INMUNODEPRESIÓN / INFECCIÓN 4.CRASIS Indicaciones • HIPOTERMIA PROFILÁCTICA: NO esta recomendado en el TEC • HIPOTERMIA TERAPÉUTICA: Opción en HIC refractaria • < 45 años • manteniendo otras medidas • sólo en centros con entrenamiento Hipotermia Profiláctica Neurosurg Clin N Am. 2016 Oct;27(4):489-97. Hipotermia - PCR TRATAMIENTO DE LA HIC REFRACTARIA DESCOMPRESIVA (1900) DESCOMPRESIVA DEFINICIÓN: procedimiento BIFÁSICO • RESECCIÓN ÓSEA + DUROPLASTIA (Yoo 1999, PIVOT) • CRANIECTOMÍA (1) CRANIOPLASTIA (2) DIMENSIONES • PUNTO CLAVE PARA QUE REALMENTE CUMPLA SU ROL AUMENTO CAPACIDAD ≥12 cm INTRACRANEANA FOSA TEMPORAL DECOMPRESIVA TÉRMICA 37º ? <36º 36.5º DESCOMPRESIVA CLASIFICACIÓN • PRIMARIA • SECUNDARIA TIPOS • BIFRONTAL • TEMPORAL • FOSA POSTERIOR DESCOMPRESIVA LATERAL DESCOMPRESIVA • TRABAJO de TAYLOR A. y col. (Childs Nervus System. FEB 2001) • HIC REFRACTARIA ¨…….ICP will be reduced, fewer episodes of intracranial hypertension will occur, and functional outcome and quality of life may be better than in children treated with medical management alone¨. DESCOMPRESIVA CANDIDATOS • < 60 AÑOS • LESIÓN III- IV • COMPROMISO SISTÉMICO Y/O POLITRAUMA TIMING • < 48 horas • HIC refractaria: >25 • En el contexto de manejo progresivo DESCOMPRESIVA COMPLICACIONES EN MAS o EXPANSIVAS • PIC ELEVADA EN MENOS o EXCAVADAS • PIC BAJA 1. AGUDAS • HEMATOMAS • LESIONES DE REPERFUSIÓN 1. Presentación ALEJADA 2. Agravados por PL y el Ortostatismo 3. Mejoran con CRANIOPLASTIA 2. SUBAGUDA o CRÓNICA • HIDROCEFALIA Precedida por FÍSTULA LCR y/o HIGROMA lateral/interhemisférico DESCOMPRESIVA SEMIOLOGÍA DE LA DESCOMPRESIVA • HERIDA • LATIDO • TENSIÓN (MODIF. CON LA POSICIÓN) • COLGAJO ÓSEO (ABDOMINAL) • VERIFICAR POSICIÓN DE CATETER DE PIC (TC) INFARTO VENOSO HIPOTERMIA + DECOMPRESIVA REDUCCIÓN DE PIC REDUCCIÓN PIC ++ +++ CONTROL DE LA CASCADA INJRIANTE ROTURA DEL AISLAMIENTO TÉRMICO MENOR REPERFUSIÓN AMORTIGUACIÓN DEL REWARMING SINERGIA + HIPOTERMIA + BARBITÚRICOS INMUNODEPRESIÓN INMUNODEPRESIÓN ++ ++ COMPROMISO HEMODINÁMICO COMPROMISO HEMODINÁMICO ++ ++ ANTAGONISMO TÉRMICO TEMPERATURA CEREBRAL SINERGIA - Descompresiva Lesiones del DECRA No realizar esta técnica en pacientes con aumento transitorio (10-15min) de PIC>20 Los pacientes deberán tener HIC refractaria > 25-30? mantenida (1 hora o mas?) Descompresiva Secundaria Decompressive Craniectomy in Patients with Traumatic Brain Injury: Are the Usual Indications Congruent with Those Evaluated in Clinical Trials? Kramer AH1,2,3, Deis N4,5, Ruddell S4, Couillard P4,5,6, Zygun DA7, Doig CJ4,8, Gallagher C4,5,6. BACKGROUND: In patients with traumatic brain injury (TBI), multicenter randomized controlled trials have assessed decompressive craniectomy (DC) exclusively as treatment for refractory elevation of intracranial pressure (ICP). DC reliably lowers ICP but does not necessarily improve outcomes. However, some patients undergo DC as treatment for impending or established transtentorial herniation, irrespective of ICP. METHODS: We performed a population-based cohort study assessing consecutive patients with moderate-severe TBI. Indications for DC were compared with enrollment criteria for the DECRA and RESCUE-ICP trials. RESULTS: Of 644 consecutive patients, 51 (8 %) were treated with DC. All patients undergoing DC had compressed basal cisterns, 82 % had at least temporary preoperative loss of ≥1 pupillary light reflex (PLR), and 80 % had >5 mm of midline shift. Most DC procedures (67 %) were "primary," having been performed concomitantly with evacuation of a space-occupying lesion. ICP measurements influenced the decision to perform DC in 18 % of patients. Only 10 and 16 % of patients, respectively, would have been eligible for the DECRA and RESCUE-ICP trials. DC improved basal cistern compression in 76 %, and midline shift in 94 % of patients. Among patients with ≥1 absent PLR at admission, DC was associated with lower mortality (46 vs. 68 %, p = 0.03), especially when the admission Marshall CT score was 3-4 (p = 0.0005). No patients treated with DC progressed to brain death. Variables predictive of poor outcome following DC included loss of PLR(s), poor motor score, midline shift ≥11 mm, and development of perioperative cerebral infarcts. CONCLUSIONS: DC is most often performed for clinical and radiographic evidence of herniation, rather than for refractory ICP elevation. Results of previously completed randomized trials do not directly apply to a large proportion of patients undergoing DC in practice. Neurocritical Care, Agosto 2016 TRATAMIENTO DE LA HIC REFRACTARIA DRENAJE LUMBAR CONTROLADO (DLC) DRENAJE LUMBAR CONTROLADO • PL, edema de papila e HIC • RESURGIMIENTO 1.Pseudotumor Cerebral 2.Meningitis Criptocóccica OPCIÓN REQUISITOS 1. VENTRICULOSTOMÍA 2. CISTERNAS PRESENTES 3. AUSENCIA LESION MASA y/o DLM DRENAJE LUMBAR FUNDAMENTOS • ESPACIO ESPINAL : > 50 % DE LCR >30% DE LA COMPLIANCE CRANIOSPINAL • NO COMPRESIÓN POR EDEMA • MENOR RIESGO DE INFECCIÓN Y HEMORRAGIA Clinical evaluation of the safety and efficacy of lumbar cerebrospinal fluid drainage for the treatment of refractory increased intracranial pressure. Tuettenberg J, Czabanka M, Horn P, Woitzik J, Barth M, Thomé C, Vajkoczy P, Schmiedek P, Muench E. J Neurosurg. 2009 Jun;110(6):1200-8. J Neurosurg. 2009 Dec;111(6):1295; author reply 1295-6. Neurologic outcome of posttraumatic refractory intracranial hypertension treated with external lumbar drainage. Abadal-Centellas JM, Llompart-Pou JA, Homar-Ramírez J, Pérez-Bárcena J, Rosselló-Ferrer A, IbáñezJuvé J. J Trauma. 2007 Feb;62(2):282-6; discussion 286. J Trauma. 2007 Sep;63(3):720-1; author reply 721. Therapy of malignant intracranial hypertension by controlled lumbar cerebrospinal fluid drainage. Münch EC, Bauhuf C, Horn P, Roth HR, Schmiedek P, Vajkoczy P. Crit Care Med. 2001 May;29(5):976-81. External lumbar drainage in uncontrollable intracranial pressure in adults with severe head injury: a report of 7 cases. Willemse RB, Egeler-Peerdeman SM. Acta Neurochir Suppl. 1998;71:37-9. Lumbar drainage for the treatment of severe bacterial meningitis. Abulhasan YB, Al-Jehani H, Valiquette MA, McManus A, Dolan-Cake M, Ayoub O, Angle M, Teitelbaum J. Neurocrit Care. 2013 Oct;19(2):199-205. Meningitis aguda grave Neuro-intensive treatment targeting intracranial hypertension improves outcome in severe bacterial meningitis: an intervention-control study. Glimåker M, Johansson B, Halldorsdottir H, Wanecek M, Elmi-Terander A, Ghatan PH, Lindquist L, Bellander BM. PLoS One. 2014; 9(3):e91976. Epub 2014 Mar 25. DRENAJE LUMBAR CONTROLADO EN LA PRÁCTICA 1. DRENAJE CERRADO CON APERTURA SOLAMENTE CUANDO LA PIC SUPERA 25 mmHg DURANTE 10-20 min 2. DRENAJE CONTRA PRESIÓN DE 15 mmHg 3. MONITOREO RIGUROSO DEL RIESGO DE DESCENSO CEREBRAL: TENTORIAL (foramen de Pacchioni) y TONSILAR (foramen Magno) DRENAJE LUMBAR CONTROLADO TOMOGRAFÍA CRANEO IDEAL CONTAR CON ESTUDIO PREVIO A LA MEDIDA TERAPEÚTICA CORTES FINOS A NIVEL DEL TENTORIO Y FOSA POSTERIOR • ¨sag ratio¨(Tentorio 0.91; 1 desplasamiento) • Compresión Cisternal • Compresión III y IV ventrículo DRENAJE LUMBAR CONTRAINDICACIONES • LESIÓN MASA Y DESVÍO DE LA LÍNEA MEDIA • CISTERNAS BASALES BORRADAS APROX. 10% RIESGO HERNIACIÓN NO CONFIARSE EN AUSENCIA DE CONTRAINDICACIONES DRENAJE LUMBAR CONTROLADO MEDIDAS CORRECTIVAS 1.CIERRE INMEDIATO 2.POSICIÓN DE TRENDELENBURG URGENTE DRENAJE LUMBAR ? Sindrome Levy-Rekate EDEMA CEREBRAL F. CENTRÍPETA SUMA ARITMÉTICA Hipertensión Intracraneana HIDROCEFALIA F. CENTRÍFUGA RESTA GIOMÉTRICA ¨Cisternas Presentes¨ PATRÓN SEUDONORMAL HSA, MENINGITIS, TRAUMA Caída GCS + anisocoria (Chequear respuesta después de cada medida) Elevar Cabecera Cama Asegurar PAM 80-90 Corregir Hipoxemia Normoventilación 35 Iniciar SAC Chequear y Solucionar A-B-C Rechequear en forma seriada Osmoterapia carga iv SSH/Manitol HV 25-30 TC Urgente Convocar NQ urgente Evacuación Derivación Ext. Decompresiva Primaria BBT bolo iv Lesión pasible de Neurocirugía BQ Independientemente de la respuesta clínica la TC debe realizarse siempre Unidad Neurointensivismo Lesión no pasible de Neurocirugía Neuromonitoreo Multimodal Si se realizó Dsc. PIC usualmente controlada Descompresiva Secundaria Si disponemos DVE y continuamos con HIC abrirla dado que es altamente efectiva No contamos DVE THAM Indometacina BBT infusión Hipotermia Terapéutica Si persiste HIC: 1-Chequear topes terapéuticos de otras medidas de 1 Nivel utilizadas 2- Si están al máximo, pasar al 2 y/o 3 N 3- Rechequear topes en la evolución y mantener medidas al máximo mientra continúe con HIC refractaria Drenaje Lumbar

© Copyright 2026